
Abstract
Untargeted metabolomic analysis is a powerful tool used for the discovery of novel biomarkers. Chagas disease (CD), caused by Trypanosoma cruzi, is a neglected tropical disease that affects 6–7 million people with approximately 30% developing cardiac manifestations. The most significant clinical challenge lies in its long latency period after acute infection, and the lack of surrogate markers to predict disease progression or cure. In this cross-sectional study, we analyzed sera from 120 individuals divided into four groups: 31 indeterminate CD, 41 chronic chagasic cardiomyopathy (CCC), 18 Latin Americans with other cardiomyopathies and 30 healthy volunteers. Using a high-throughput panel of 986 metabolites, we identified three distinct profiles among individuals with cardiomyopathy, indeterminate CD and healthy volunteers. After a more stringent analysis, we identified some potential biomarkers. Among peptides, phenylacetylglutamine and fibrinopeptide B (1–13) exhibited an increasing trend from controls to ICD and CCC. Conversely, reduced levels of bilirubin and biliverdin alongside elevated urobilin correlated with disease progression. Finally, elevated levels of cystathionine, phenol glucuronide and vanillactate among amino acids distinguished CCC individuals from ICD and controls. Our novel exploratory study using metabolomics identified potential biomarker candidates, either alone or in combination that if confirmed, can be translated into clinical practice.
Similar content being viewed by others

Introduction
Chagas disease (CD) is a parasitic disease caused by Trypanosoma cruzi, a protozoan endemic to the American continent. CD is considered a neglected tropical disease affecting the global health. According to the World Health Organization (WHO) it affects 6–7 million people1. After an acute phase, often asymptomatic, infected people with CD move to a chronic phase. The indeterminate CD form (ICD) involves a group of infected people who remain asymptomatic with no organ involvement. However, around 30% of the chronically infected individuals will develop an organic impairement, mainly affecting the heart and the digestive tract2. Chronic chagasic cardiomyopathy (CCC) represents the greatest burden of morbidity and mortality among these subjects, accounting to around 12.000 deaths annually3.
CD treatment in the chronic phase is recommended mainly in indeterminate cases and women in childbearing age. In addition, parasitological treatment shows a high rate of adverse events, and there are no reliable surrogate markers for disease progression or cure4,5. Thus, the identification of specific biomarkers for each clinical form is currently needed, as it may have a significant impact on patient management. On one hand, they will allow identifying individuals at a higher risk of progression. On the other hand, they can help monitor treatment response and evaluate drug effectiveness in clinical trials since the only definite criterion of cure is negativization of the serology, which can last more than 20 years6.
Untargeted metabolomics is a powerful tool to search for metabolic variations among pre-established groups. Metabolomic studies have been used for the discovery of novel biomarkers in disease states and report metabolic signatures that can be used for diagnosis, monitoring, and treatment response7. It also has the potential to provide insights into the pathophysiological mechanisms of a disease and, therefore, describe potential targets for new treatments. Previous studies have been conducted with the purpose of identifying metabolic conditions in CD9. However, the only study performed on human samples was performed in heart tissue of end-stage CCC individuals and healthy controls10. Furthermore, neither animal nor human CD metabolome analysis have compared the different stages of the disease.
Therefore, we designed a cross-sectional study with the main objective of describing the metabolomic profile associated with individuals with and without CD, depending on the presence or absence of cardiac involvement, to identify potential prognostic and cure biomarkers.
Subjects and methods
We conducted a cross-sectional study from January 2016 to August 2018. Participants were recruited from three international health centers: 1) Vall d’Hebrón—Drassanes International Health Unit (Barcelona, Spain), 2) National Reference Unit for Tropical Diseases. Infectious Diseases Department. Ramón y Cajal University Hospital (Madrid, Spain) and 3) Institute of Tropical Medicine of São Paulo—USP (São Paulo, Brazil). Biomarker determinations were performed by the enterprise Metabolon, Inc. (617 Davis Drive, Suite 400, Durham, NC 277,133 www.metabolon.com) and analyzed at the Centro de Biología Molecular Severo Ochoa (CBMSO) (Madrid, Spain).
Study population and definitions
The included participants were all from Latin American countries. We defined 4 groups of participants: Group 1 indeterminate Chagas disease (ICD), Group 2 chronic chagasic cardiomyopathy (CCC), Group 3 of healthy volunteers, and Group 4, which comprises individuals with cardiomyopathy other than CCC.
All participants were over 18 years old. Group 1 and 2 included people diagnosed with CD by two different validated serological tests. The organic involvement was studied with a chest radiography, an electrocardiogram (EKG) and heart ultrasound. Those showing abnormalities in at least one of the tests underwent echocardiography to evaluate CCC. We defined CCC as the presence of a conduction alteration related to CD, a left ventricle telediastolic volume (LVEDV) > 55mm3, ejection fraction (EF) < 45% or altered segmental contractility. Participants who had received anti-parasitic treatment before inclusion were also excluded. Group 3 were recruited at international health facilities after a negative ELISA test for CD and normal EKG and echocardiogram. Those participants with arterial hypertension, diabetes mellitus or other comorbidities were excluded from groups 1 to 3. Group 4 were selected from cardiology units and included patients with a LVEDV > 55mm3, EF < 45% or an altered segmental contractility and a negative serologic test.
All included participants underwent a clinical history and physical examination. Chest radiography and 12-lead electrocardiogram were performed at the inclusion visit and echocardiography was performed during the following month. Serum was extracted and aliquots of 100ul were conserved at − 80ºC till the analysis procedure.
Metabolomic analysis
Metabolomic analysis was performed using the Metabolon Global Discovery Panel. Samples were prepared using the automated MicroLab STAR® system from Hamilton Company. A quality assurance (QA)/ quality control (QC) process was performed according to Metabolon procedures. Sample extracts were analyzed by UPLC-MS/MS. Waters ACQUITY ultra-performance liquid chromatography (UPLC) and a Thermo Scientific Q-Exactive high resolution/accurate mass spectrometer interfaced with a heated electrospray ionization (HESI-II) source and Orbitrap mass analyzer operated at 35,000 mass resolution were utilized. Raw data was extracted, peak-identified and QC processed using Metabolon’s hardware and software. Metabolites were identified by comparison to library entries of purified standards.
A variety of curation procedures were carried out to ensure that a high-quality data set was made available for statistical analysis and data interpretation. The QC and curation processes were designed to ensure accurate and consistent identification of true chemical entities, and to remove those representing system artifacts, mis-assignments, and background noise. Proprietary visualization and interpretation software of Metabolon were used to confirm the consistency of peak identification among the samples.
Adobe Illustrator CS5 was used for figure presentation. Volcano plots were done with ggplot2 and ggrepel packages of R programming language (version 4.2.2). Heat map and PCA were computed with the online tool ClustVis, a web tool for visualizing clustering of multivariate data, using a predefined correlation clustering distance method (Pearson correlation subtracted from 1) based on the average distance of all possible pairs37. Bar plots of the most remarkable metabolites were performed in GraphPad Prism (version 8).
Statistics
Statistical analysis of metabolomic study was done according to Metabolon procedures. ANOVA contrasts were used to identify biochemicals that differed significantly between experimental groups, and an estimate of the false discovery rate (FDR) was calculated to consider the multiple comparisons that normally occur in metabolomic-based studies. Statistical analyses were conducted to detect differences in ratios of the mean scaled intensities for a metabolite between two experimental groups. In bar plots representation values are scaled intensity means ± SEMs; and statistical significance respect to healthy controls is displayed by asterisks (*) being **** p < 0.0001, *** p < 0.001, ** p < 0.01 and * p < 0.05; and statistical significance respect to ICD individuals is displayed by hashes (#) being #### p < 0.0001, ### p < 0.001, ## p < 0.01 and # p < 0.05.
Ethics declarations
The study was approved by the institutional review board of the coordinating center located at Vall d'Hebron Hospital in Barcelona, Spain (PR(AG)93/2015), and by the ethics committee of each participant center. There was no commercial sponsorship of the study. Written informed consent for participation was obtained from all the participants. Data on human subjects were analyzed anonymously and clinical investigations have been conducted according to the Declaration of Helsinki.
Results
From January 2016 until August 2018, a total of 120 participants were included in the study: 31 individuals with ICD, 41 individuals with CCC, 30 healthy controls and 18 individuals without CD suffering other cardiomyopathies (referred to as heart disease, HD). The demographics of the participants are presented in Table 1. Sixty-eight (56.7%) participants were male, and the mean age was 50.6 years. Additional information regarding the cardiac involvement of participants in group 2 and 4 can be found in Supplementary material Table S1.
A total of 986 metabolites with known identity from the Metabolon platform were analyzed. Initially, we performed a Principal Component Analysis using the scaled intensities of each metabolite (Fig. 1A). The results showed that the profile of CCC was highly similar to that of HD, while ICD displayed a distinct profile different from both the cardiac individuals and the healthy controls.

Metabolite profile of the different groups. Metabolite profile was performed by Principal Component Analysis (A) and heat map analysis (B). Different groups: individuals with indeterminate Chagas disease (ICD), chronic Chagas cardiomyopathy (CCC) and cardiomyopathy without Chagas disease (HD). Mean scaled intensities of each metabolite were used. A color code was given from high (Red) to low (Blue) values in heat map representation. Cluster analysis for columns and rows was done according to the Pearson correlation.
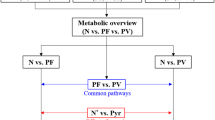
Furthermore, in a heatmap analysis HD and CCC individuals clustered together again, whereas ICD participants formed a separate group (Fig. 1B). Based on these findings, we carried out a deeper analysis to identify potential biomarkers establishing 3 different comparisons: ICD-Control and CCC-Control for the identification of metabolites that changed from a control to a CD individual, and CCC-ICD to identify metabolites that varied with disease progression. Supplementary tables 2–4 compiles all the detected metabolites in each comparison.
In the ICD-control comparison, 96 metabolites were downregulated and 92 were upregulated (Fig. S1). The CCC-control comparison revealed fewer significant changes, with only 7 downregulated and 59 upregulated metabolites (Fig. S2). When comparing CCC and ICD individuals, 68 metabolites were downregulated, while 244 were upregulated (Fig. S3). Supplementary tables 5–7 provides a list of all the downregulated and upregulated metabolites in each comparison.
To further narrow down the potential biomarker candidates, a more stringent analysis was performed by increasing the thresholds of the ratios to > 1 of log2ratio and FDR < 0.01 for significance. The following summary presents the most relevant results based on the subpathways to which the metabolites belong.
Peptides and carbohydrate metabolism
Levels of dipeptide metabolites showed the most significant alterations in all the comparisons. Their expression decreased in almost all individuals with ICD but increased back to control levels in individuals of CCC. However, CCC individuals exhibited higher levels of phenylalanylalanine compared to controls (Fig. 2A,B). Gamma-glutamyl amino acids followed a similar pattern, except for gamma-glutamyl methionine, which showed an opposite behavior (increased in ICD and decreased in CCC). Notably, phenylacetylglutamine (PAG), an acetylated peptide, and fibrinopeptide B (1–13) increasingly changed from controls to ICD and then to CCC individuals. Supplementary table 8 provides a comprehensive list of all the peptide metabolites in each comparison classified by subpathways. Regarding carbohydrate metabolites, our analysis revealed only a few significant changes in the CCC-ICD and ICD-Control studies (Fig. S4 and Supplementary table 9).

Peptide metabolites analysis. (A) Volcano plot of peptide metabolites with log2ratio of mean scaled intensities and -log10FDR of each metabolite. Thresholds of significance are shown by dashed lines: < -1 and > 1 for the log2ratio and > 2 for the -log10FDR. Significant down or upregulated metabolites of ICD-control (green), CCC-ICD (red) and CCC-control (blue) comparisons are displayed. Non-significant metabolites are marked in grey. Subpathways are shown with different symbols. (B) Bar plots of the potential candidates to biomarker of Chagas disease. Values are scaled intensity means ± SEMs. Statistical significance respect to healthy controls is displayed by asterisk (*) being *** p < 0.001, ** p < 0.01 and * p < 0.05. Statistical significance respect to ICD individuals is displayed by hash (#) being #### p < 0.0001, ### p < 0.001, ## p < 0.01 and # p < 0.05.
Lipid metabolism
In ICD participants, we observed reduced levels of primary and secondary bile acids, which returned to control levels in CCC individuals (Fig. S5). However, we did not find many changes in sterols and steroids, although progestin steroids exhibited a substantial increase in ICD individuals (Fig. S6). Eicosanoids and neutral lipids showed only a few significant metabolites, and only some diacylglycerols displayed significance in ICD individuals (Fig. S7). Furthermore, fatty acids and derivatives exhibited minimal changes (Fig. S8).
Regarding glycerolipids, phospholipids and lysophospholipids metabolism, only certain phosphatidylethanolamines and phosphatidylcholines exhibited significant up-regulation in the ICD set (Fig. S9). Supplementary table 10 presents all the lipid metabolites in each comparison, classified by subpathways.
Cofactors and vitamin metabolism
Particularly, within the hemoglobin and porphyrin metabolism subpathway, significant variations were evident. Bilirubin (Z,Z), bilirubin (E,E), and biliverdin exhibited significant increases in ICD participants. Moreover, L-urobilin demonstrated a substantial escalation from ICD to chronic chagasic cardiomyopathy (CCC) participants, indicating a progressive metabolic shift across disease stages. Beta-cryptoxanthin in the vitamin A metabolism showed a similar profile (Fig. 3A,B). Supplementary table 11 lists all the cofactor and vitamin metabolites in each comparison.

Cofactors and vitamins analysis. (A) Volcano plot of cofactor and vitamin metabolites with log2ratio of mean scaled intensities and -log10FDR of each metabolite. Thresholds of significance are shown by dashed lines: < -1 and > 1 for the log2ratio and > 2 for the -log10FDR. Significant down or upregulated metabolites of ICD-control (green) and CCC-ICD (red) comparisons are displayed. Non-significant metabolites are marked in grey. Sub-pathways are shown with different symbols. (B) Bar plots of the potential candidates to biomarker of Chagas disease. Values are scaled intensity means ± SEMs. Statistical significance respect to healthy controls is displayed by asterisk (*) being **** p < 0.0001, *** p < 0.001, ** p < 0.01 and * p < 0.05. Statistical significance respect to ICD individuals is displayed by hash (#) being #### p < 0.0001, ### p < 0.001, ## p < 0.01 and # p < 0.05.
Amino acids metabolism
Significant differences were also found in the urea cycle, arginine, and proline metabolism, and the guanidino and acetamido metabolism. Urea, N2,N5-diacetylornithine and guanidinosuccinate increased in CCC participants compared to the other sets, indicating a progression biomarker pattern (Fig. 4A,B). Supplementary Table 12 lists all these metabolites in each comparison.

Urea and arginine metabolism analysis. (A) Volcano plot of urea and arginine metabolites with log2ratio of mean scaled intensities and -log10FDR of each metabolite. Thresholds of significance are shown by dashed lines: < -1 and > 1 for the log2ratio and > 2 for the -log10FDR. Significant down or upregulated metabolites of ICD-control (green) and CCC-ICD (red) comparisons are displayed. Non-significant metabolites are marked in grey. Sub-pathways are shown with different symbols. (B) Bar plots of the potential candidates to biomarker of Chagas disease. Values are scaled intensity means ± SEMs. Statistical significance respect to healthy controls is displayed by asterisk (*) being **** p < 0.0001, *** p < 0.001, ** p < 0.01 and * p < 0.05. Statistical significance respect to ICD individuals is displayed by hash (#) being #### p < 0.0001, ### p < 0.001, ## p < 0.01 and # p < 0.05.
ICD individuals showed an increase in methionine metabolism, as well as in leucine, isoleucine, and valine metabolism (Fig. 5). In fact, methionine, N-acetylmethionine, N-formylmethionine, 3-methyl-2-oxobutyrate and 4-methyl-2-oxopentanoate exhibited some of the highest ratios for ICD participants (Fig. S10). Furthermore, tyramine O-sulfate and vanillic alcohol sulfate, metabolites of the tyrosine metabolism, showed a significant increase comparing from ICD to CCC subjects.

Amino acids metabolism analysis. (A, B) Volcano plots of amino acids metabolites with log2ratio of mean scaled intensities and -log10FDR of each metabolite. Thresholds of significance are shown by dashed lines: < -1 and > 1 for the log2ratio and > 2 for the -log10FDR. Significant down or upregulated metabolites of ICD-control (green), CCC-control (blue) and CCC-ICD (red) comparisons are displayed. Non-significant metabolites are marked in grey. Sub-pathways are shown with different symbols. (C) Bar plots of the potential candidates to biomarker of Chagas disease. Values are scaled intensity means ± SEMs. Statistical significance respect to healthy controls is displayed by asterisk (*) being *** p < 0.001, ** p < 0.01 and * p < 0.05. Statistical significance respect to ICD individuals is displayed by hash (#) being #### p < 0.0001, ### p < 0.001, ## p < 0.01 and # p < 0.05.
However, the most notable profile as progression biomarkers, with a specific and significant increase in CCC participants, was observed among three metabolites: vanillactate and phenol glucuronide of the tyrosine metabolism, and the cystathionine of the cysteine metabolism. Supplementary Table 13 lists all the amino acids metabolites in each comparison.
Discussion
Despite significant advancements in the study of the immunopathogenesis of CD, there is an urgent need to identify markers for disease progression and cure in clinical practice, particularly for the development of drugs and vaccines. This is the first analysis using a metabolomic approach to provide a more comprehensive description of the various stages of CD, comparing them with healthy individuals and cardiopathies of different etiologies.
One of the major findings from our groundbreaking study is that patients with CD exhibit a distinct metabolic profile depending on the stage of the disease, with notable differences between ICD and the CCC forms. Interestingly, individuals with ICD demonstrated significant variations compared to healthy controls from the same areas11,12.
Another important finding is that CCC subjects share similarities with individuals suffering from other HD. While CCC has a distinctive physiopathology and characteristic presentation, its subsequent clinical manifestations are not specific to the disease13,14. The latter stages of the cardiac form led to heart failure, which likely exhibits common metabolic variations regardless of its origin. This somewhat validates our approach.
Among these findings, we observed variations in peptide metabolites between the different groups, some of which displayed a potential profile as cure biomarkers. Dipeptides were the most significantly altered metabolites in all the comparisons. Almost all of them exhibited decreased expression in ICD individuals, followed by an increase in CCC subjects, eventually returning to control levels15. Of particular significance is phenylalanylalanine, which was detected at higher levels among CCC participants with the lowest levels among ICD participants. Elevated levels of dipeptides typically result from protein degradation and have been identified as pathogenic factors for oxidative stress and cardiovascular disease16.
Interestingly, among the peptide metabolites, two of them, phenylacetylglutamine (PAG) and fibrinopeptide B (1–13), show promising potential as biomarkers for the cure of CD. PAG binds to various platelet receptors leading to platelet aggregation and subsequent atherothrombosis, which have been associated with myocardial infarction, stroke, and death17. PAG has been clinically linked to heart failure and its severity, and it has been proposed as a potential therapeutic agent for cardiovascular diseases18. Furthermore, elevated serum concentrations of PAG have been observed in patients with heart failure or cardiovascular disease and have been associated with increased risk of hospitalization and mortality19,20,21. Moreover, PAG levels increase with the severity of heart failure in subjects with chronic heart failure, suggesting its potential use as an early screening, diagnostic, and treatment indicator for chronic heart failure22. Therefore, our results strongly support the use of PAG as a biomarker not only for the progression of heart disease but also as a cure biomarker for specific CCC disease and ICD individuals, which is a significant finding considering the absence of cardiac symptoms in these individuals.
Fibrinopeptides are products derived from thrombin activation during coagulation23,24. In our study, most fibrinopeptides exhibited a significant increase in CCC patients, but the isomer fibrinopeptide B (1–13) showed the most pronounced increase compared to controls. This peptide displayed the same pattern as PAG, with increasing levels observed from controls to ICD and CCC individuals. The elevated levels of fibrinopeptides in our samples suggest an enhanced coagulation in infected subjects, potentially leading to cardiovascular disease25. Fibrinopeptide B (1–13) isomer has previously been detected in individuals with acute coronary syndrome (ACS) and ischemic heart disease (IHD), while the isomers B (1–11), B (1–12) and B (1–13) have been correlated with hypertension26,27.
Hemoglobin and porphyrin metabolism metabolites were particularly noteworthy. Heme proteins undergo degradation in the liver, resulting in the production of biliverdin, which is further converted to bilirubin through an exclusive pathway in mammals28. In our study, individuals with ICD exhibited significantly increased levels of biliverdin and bilirubin compared to controls and CCC individuals. Interestingly, population studies have demonstrated a negative correlation between serum bilirubin levels and the development of cardiovascular diseases29,30,31. Conversely, urobilin has been found to be increased in incident heart failure, ACS and IHD26,32. In our study, urobilin was also upregulated in CCC individuals. Thus, decreasing levels of bilirubin and biliverdin coupled with an elevated urobilin could potentially serve as biomarkers of disease progression.
In urea and arginine metabolism, three candidates showed promise as biomarkers of progression: urea, N2,N5-diacetylornithine, and guanidinosuccinate. These metabolites were significantly increased in CCC individuals compared to ICD individuals and controls. The enrichment of the urea cycle has been described in the heart tissue of CCC individuals, and its upregulation has also been associated with mutagenesis in tumor cells10,33. However, interpreting plasma levels of urea is challenging as they are influenced by various physiological processes and can be increased by aging34. Among the branched chain amino acids, in the isoleucine, leucine and valine metabolism, 4-methyl-2-oxopentanoate and 3-methyl-2-oxobutyrate showed a significant increase in ICD participants. This, along with the increase in pyruvate, suggests a potential mitochondrial metabolic disorder in ICD individuals.
In the cysteine, histidine and tyrosine metabolism, metabolites displayed remarkable increases in CCC individuals compared to ICD and controls. One of these metabolites was cystathionine, which is transformed into cysteine by the cystathionine-gamma-lyase (CSE). Studies have shown that CSE overexpression protects against heart failure, while its deficiency exacerbates it35. In our study, we observed an accumulation of cystathionine in CCC participants, suggesting lower CSE activity and exacerbation of cardiac pathology. Additionally, two metabolites of tyrosine metabolism, vanillactate and phenol glucuronide, exhibited significant increases in CCC individuals compared to the other groups. Increased levels of vanillactate have been reported in metabolomics analyses of hypertrophic and dilated cardiomyopathies in plasma as well as in individuals with heart failure, ACS, IHD and chronic IHD26,36. Based on our findings, these molecules hold potential as biomarkers of disease progression in CCC subjects, with cystathionine and phenol glucuronide being associated with an infectious or cardiovascular disease for the first time.
In conclusion, our novel exploratory study using metabolomics in human plasma identified potential biomarker candidates, either alone or in combination. Peptide metabolites such as PAG or fibrinopeptide B (1–13), decreasing levels of bilirubin and biliverdin along with elevated urobilin; cystathionine, phenol glucuronide and vanillactate have shown promise patterns. These candidates should be further validated in targeted studies, but if confirmed, they can be easily translated into clinical practice.
Data availability
All metabolomics database are available with the present submission as Supplementary materials. Any further patient information may be made available upon formal request to the corresponding author (israel.molina@vallhebron.cat) and consent from the ethics board of reference.
References
Chagas disease in Latin America: an epidemiological update based on 2010 estimates. Wkly Epidemiol Rec 90, 33–43 (2015).
Pérez-Molina, J. A. & Molina, I. Chagas disease. Lancet 391, 82–94 (2018).
Maron, B. J. et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 113, 1807–1816 (2006).
Sales, P. A. et al. Experimental and clinical treatment of chagas disease: A review. Am. J. Trop Med. Hyg. 97, 1289–1303 (2017).
Crespillo-Andújar, C. et al. Use of benznidazole to treat chronic Chagas disease: An updated systematic review with a meta-analysis. PLoS Negl. Trop Dis. 16, e0010386 (2022).
Sguassero, Y. et al. Course of Chronic Trypanosoma cruzi Infection after Treatment Based on Parasitological and Serological Tests: A systematic review of follow-up Studies. PLoS One https://doi.org/10.1371/journal.pone.0139363 (2015).
Castelli, F. A. et al. Metabolomics for personalized medicine: the input of analytical chemistry from biomarker discovery to point-of-care tests. Anal. Bioanal. Chem. 414, 759–789 (2022).
Di Minno, A., Gelzo, M., Stornaiuolo, M., Ruoppolo, M. & Castaldo, G. The evolving landscape of untargeted metabolomics. Nutr. Metab. Cardiovasc. Dis. 31, 1645–1652 (2021).
Gironès, N. et al. Global metabolomic profiling of acute myocarditis caused by Trypanosoma cruzi infection. PLoS Negl. Trop Dis. https://doi.org/10.1371/journal.pntd.0003337 (2014).
Díaz, M. L. et al. Metabolomic Profiling of End-Stage Heart Failure Secondary to Chronic Chagas Cardiomyopathy. Int. J. Mol. Sci. https://doi.org/10.3390/ijms231810456 (2022).
Echeverría, L. E. et al. Cardiovascular biomarkers as predictors of adverse outcomes in chronic Chagas cardiomyopathy. PLoS One https://doi.org/10.1371/journal.pone.0258622 (2021).
Chow, S. L. et al. Role of biomarkers for the prevention, assessment, and management of heart failure: A scientific statement from the American heart association. Circulation 135, e1054–e1091 (2017).
Shen, L. et al. Contemporary Characteristics and Outcomes in Chagasic Heart Failure Compared With Other Nonischemic and Ischemic Cardiomyopathy. Circ. Heart Fail https://doi.org/10.1161/CIRCHEARTFAILURE.117.004361 (2017).
Saraiva, R. M. et al. Chagas heart disease: An overview of diagnosis, manifestations, treatment, and care. World J. Cardiol. 13, 654–675 (2021).
Linhares-Lacerda, L. et al. Circulating plasma microRNA-208a as potential biomarker of chronic indeterminate phase of chagas disease. Front Microbiol. https://doi.org/10.3389/fmicb.2018.00269 (2018).
Wu, G. Amino acids: metabolism, functions, and nutrition. Amino Acids 37, 1–17 (2009).
Nemet, I. et al. A Cardiovascular Disease-Linked Gut Microbial Metabolite Acts via Adrenergic Receptors. Cell 180, 862-877.e22 (2020).
Romano, K. A. et al. Gut microbiota-generated Phenylacetylglutamine and heart failure. Circ. Heart Fail 16, E009972 (2023).
Tang, H. Y. et al. Characteristic of metabolic status in heart failure and its impact in outcome perspective. Metabolites 10, 1–14 (2020).
Velasquez-Martinez, M. C., Santos-Vera, B., Velez-Hernandez, M. E., Vazquez-Torres, R. & Jimenez-Rivera, C. A. Alpha-1 Adrenergic Receptors Modulate Glutamate and GABA Neurotransmission onto Ventral Tegmental Dopamine Neurons during Cocaine Sensitization. Int. J. Mol. Sci. https://doi.org/10.3390/ijms21030790 (2020).
Fu, H., Kong, B., Zhu, J., Huang, H. & Shuai, W. Phenylacetylglutamine increases the susceptibility of ventricular arrhythmias in heart failure mice by exacerbated activation of the TLR4/AKT/mTOR signaling pathway. Int. Immunopharmacol. 116, 109795 (2023).
Zhang, Z. et al. Alteration of the gut microbiota and metabolite phenylacetylglutamine in patients with severe chronic heart failure. Front. Cardiovasc. Med. https://doi.org/10.3389/fcvm.2022.1076806 (2023).
Riedel, T. et al. Fibrinopeptides A and B release in the process of surface fibrin formation. Blood 117, 1700–1705 (2011).
Coradin, T., Wang, K., Law, T. & Trichet, L. Type I Collagen-Fibrin Mixed Hydrogels: Preparation, Properties and Biomedical Applications. Gels 2020, Vol. 6, Page 36 6, 36 (2020).
Jennewein, C. et al. Novel aspects of fibrin(ogen) fragments during inflammation. Mol. Med. 17, 568–573 (2011).
Fromentin, S. et al. Microbiome and metabolome features of the cardiometabolic disease spectrum. Nature Medicine 2022 28:2 28, 303–314 (2022).
He, W. J. et al. An untargeted metabolomics study of blood pressure: findings from the Bogalusa Heart Study. J. Hypertens 38, 1302–1311 (2020).
Fujiwara, R. et al. Systemic regulation of bilirubin homeostasis: Potential benefits of hyperbilirubinemia. Hepatology 67, 1609–1619 (2018).
Suh, S. et al. Relationship between serum bilirubin levels and cardiovascular disease. PLoS One https://doi.org/10.1371/journal.pone.0193041 (2018).
Marconi, V. C. et al. Bilirubin Is Inversely Associated With Cardiovascular Disease Among HIV-Positive and HIV-Negative Individuals in VACS (Veterans Aging Cohort Study). J. Am. Heart Assoc. https://doi.org/10.1161/JAHA.117.007792 (2018).
Ozeki, M. et al. High serum bilirubin is associated with lower prevalence of peripheral arterial disease among cardiac patients. Clin. Chim. Acta 476, 60–66 (2018).
Stenemo, M. et al. The metabolites urobilin and sphingomyelin (30:1) are associated with incident heart failure in the general population. ESC Heart Fail 6, 764–773 (2019).
Lee, J. S. et al. Urea cycle dysregulation generates clinically relevant genomic and biochemical signatures. Cell 174, 1559-1570.e22 (2018).
Musch, W., Verfaillie, L. & Decaux, G. Age-related increase in plasma urea level and decrease in fractional urea excretion: clinical application in the syndrome of inappropriate secretion of antidiuretic hormone. Clin. J. Am. Soc. Nephrol. 1, 909–914 (2006).
Kondo, K. et al. H2S protects against pressure overload-induced heart failure via upregulation of endothelial nitric oxide synthase. Circulation 127, 1116–1127 (2013).
Ravi, R. et al. Metabolite Signature in the Carriers of Pathogenic Genetic Variants for Cardiomyopathy: A Population-Based METSIM Study. Metabolites https://doi.org/10.3390/metabo12050437 (2022).
Metsalu, T. & Vilo, J. ClustVis: a web tool for visualizing clustering of multivariate data using Principal Component Analysis and heatmap. Nucl. Acids Res. 43, W566–W570 (2015).
Acknowledgements
This project was funded by “Proyectos de investigación en salud” program of the Instituto Carlos III, Ministry of Science, Innovation and Universities of the Spanish Government. Grant number: PI19/01807. Dr Ribeiro is supported in part by CNPq (465518/2014-1 e 310790/2021-2) and FAPEMIG (RED 00192-23). Dr. Sabino is supported in part by NIH grant: 1U01AI168383-01.
Author information
Authors and Affiliations
Contributions
I.M, N.G and M.F conceived the experiment and decided its methodology. P.BN, JA.PM, F.S, B.MM, JF.RP, ALP.R, A.SM, EC.S, F.N and I.M included the participants and collaborated with the study design. A.HC, M.F and N.G performed the analysis of all metabolic data. A.HC and P.BN co-wrote the paper. All the authors have made substantial contributions to the manuscript and have approved the submitted version. All the authors vouch for the accuracy and integrity of the presented work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Herreros-Cabello, A., Bosch-Nicolau, P., Pérez-Molina, J.A. et al. Identification of Chagas disease biomarkers using untargeted metabolomics. Sci Rep 14, 18768 (2024). https://doi.org/10.1038/s41598-024-69205-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-69205-w
- Springer Nature Limited