
Abstract
Hypertension is a very common comorbidity in type 2 diabetes patients, which leads to important health and treatment challenges. The present study was conducted with the aim of determining the prevalence of hypertension and its risk factors in type 2 diabetes patients. This study was conducted using cross-sectional data from 1245 participants aged between 35 and 70 years and diagnosed with type 2 diabetes at baseline in the Fasa cohort study. The prevalence hypertension was determined and multivariate logistic regression was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the association between various risk factors and hypertension prevalence. The average age of the participants was 53.5 ± 8.7 years and 71.7% (n = 893) were female and 28.3% (n = 352) were male. The prevalence of hypertension in people with type 2 diabetes was 45.5% (n = 566). Higher age (AOR, 95% CI: 8.1, 4.6–14.3), female gender (OR, 95% CI: 1.8, 1.2–2.5), Fars (AOR, 95% CI: 1.6, 1.1–2.4) and Turk (AOR, 95% CI: 1.6, 1.1–2.5) vs. other ethnicity, and overweight (AOR, 95% CI: 1.8, 1.38–2.38) and obesity (AOR, 95% CI: 2.7, 2.0–3.8) vs. BMI < 25 was associated with a higher prevalence of hypertension, while higher physical activity (AOR, 95% CI: 0.57, 0.42–0.78) was associated with lower prevalence of hypertension in the multivariable model. The prevalence of hypertension in persons with type 2 diabetes was high and increased with greater age, in some ethnic groups, and with higher BMI and low physical activity. Further prospective studies are needed to investigate these associations in this population.
Similar content being viewed by others


Introduction
Non-communicable diseases (NCDs) are among the main causes of death worldwide1. Type 2 diabetes is one of the most important non-communicable diseases and can cause a wide range of complications, including cardiovascular, renal and neurological complications2. In the last 3 decades, the prevalence of type 2 diabetes has increased dramatically in developed and developing countries, however, most patients live in low and middle income countries (LMICs)2. The highest prevalence of type 2 diabetes is observed in the Middle East and North Africa region. Iran is one of the countries in the Middle East region, where it is predicted that the prevalence of type 2 diabetes will continue to increase until 20453. The prevalence of type 2 diabetes in the capital of Iran is estimated at 16.7%4, and similarly at 15% in other regions of Iran5.
The most common cause of death in diabetic patients is cardiovascular disease (CVD). Hypertension is an important risk factor for CVD, which is often associated with diabetes6. In recent decades, the prevalence of hypertension has been on the rise in LMICs due to an increase in risk factors for hypertension7. In the Eastern Mediterranean region, the prevalence of hypertension varies in different countries8. In Iran, the prevalence of hypertension has been reported as 19.2%9. One of the important health challenges of type 2 diabetes patients is hypertension, the prevalence of which varies from 32 to 82%, considerably higher than in persons without type 2 diabetes10.
High blood pressure is the leading cause of premature death worldwide, and 9% of disability-adjusted life-years and 19% of all deaths globally are due to elevated systolic blood pressure7. High blood pressure is an important risk factor in the occurrence of CVD and kidney diseases11,12, which imposes a heavy economic burden on societies13. The economic benefits of improving treatment programs for high blood pressure are considerable and outweigh the costs by about 18 to 114. Uncontrolled high blood pressure has many complications, including heart attacks, angina, heart failure, atrial fibrillation, aortic dissection and aneurysm, stroke, sudden cardiac death, and kidney failure7,11,15,16,17,18,19. On the other hand, diabetes can also cause a wide range of complications including macro and micro vascular and other complications6,20. Therefore, it is necessary to manage hypertension in patients with type 2 diabetes.
One of the important principles in the clinical management of patients with type 2 diabetes is diagnosis, identification and treatment of hypertension6. Hypertension management is an important health intervention that can lead to the reduction of CVD outcomes and mortality, and can reduce the heavy economic burden caused by CVDs on societies21. Diagnosing, identifying and treating high blood pressure is very important for the prevention of cardiovascular diseases in the population at risk, especially in patients with type 2 diabetes. Because high blood pressure as a modifiable risk factor for CVDs can be lowered through lifestyle changes and low-cost interventions such as eating low-salt foods, fruit and vegetables, having appropriate physical activity, losing weight, and stopping tobacco use7,22. Therefore, the present study was conducted with the aim of determining the prevalence of hypertension and the demographic, socioeconomic factors affecting it in patients with type 2 diabetes in a large Iranian population.
Methods
This cross-sectional study included people aged 35–70 years old with type 2 diabetes who participated in the Fasa cohort study. The Fasa cohort study is a subset of the PERSIAN (Prospective Epidemiological Research Studies in Iran) cohort study. The PERSIAN study was conducted with the aim of evaluating and identifying risk factors of non-communicable diseases and also calculating the risk of contracting non-communicable diseases. Out of the total 41,000 people in the rural population of Sheshda and Qara-Balagh regions, 11,097 people aged 35 to 70 years were considered as the target population of the Fasa cohort study. Of these, 10,138 people participated in the Fasa cohort study. The basic data collection of Fasa cohort study lasted from 2015 to 2016. Subjects participating in the Fasa cohort study were allowed to withdraw from the study at any time.
In the present study, the data of phase one of the Fasa cohort study have been used. More details of Fasa cohort study are described in other publications23,24.
Information on demographic characteristics (age, gender, education level, ethnicity, marital status), socioeconomic status, physical activity, smoking habits and opium use, and medical history (diabetes, hypertension) was collected by face to face interviews. The interviews were conducted by native interviewers which were trained by the national cohort experts. Anthropometric data (height and weight) were measured by trained personnel.
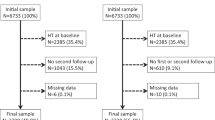
In this study, people with type 2 diabetes were selected and the prevalence of hypertension in them was determined, and then the demographic and socioeconomic factors affecting hypertension were determined. A total of 1245 people who had type 2 diabetes from the population covered by the Fasa cohort were included in this study. Figure 1 shows the flowchart of the participant selection.

Study flowchart.
Measurements
In the Fasa cohort study, information on demographic characteristics including age, sex, marital status, education level, ethnicity, history of diabetes and hypertension, history of smoking and opium use were recorded in the questionnaire during the interviews. In this analysis, people were grouped into four age groups: 35–44 years, 45–54 years, 55–64 years, and 65 years and older. In this survey, the marital status includes two groups: married and others (single, divorced and widowed). People's ethnicity was grouped into three groups: Fars, Turks, and others, and other ethnicities include Arabs, Kurds, Lors, Baluchs, etc. Questions on current smoking status (yes and no) and opium use (yes and no) were asked. The physical activity level of the participants was determined based on Metabolic Equivalent of Task (MET)-hours and was then grouped into three groups: low, medium and high. The wealth index was grouped into 5 groups: very high, high, medium, low and very low. Weight and height was measured by trained personnel and body mass index (BMI) was calculated. BMI was categorized in three groups: underweight or normal weight (< 25), overweight (29.9–25.0) and obese (> = 30). History of type 2 diabetes and hypertension status were categorized as yes or no.
Ethical considerations
This research proposal was approved by the Ethics Committee of Jahrom University of Medical Sciences (IR.JUMS.REC.1402.098). People participated in Fasa Persian cohort study voluntarily and with informed consent. The questionnaire used had no name. All methods have been carried out in accordance with the relevant guidelines and regulations.
Statistical analysis
Means and standard deviations were reported for quantitative variables and frequencies and percentages were reported for qualitative variables. After identifying the participants who had prevalent type 2 diabetes, they were divided into two groups with high blood pressure and without high blood pressure. To determine the cross-sectional association between independent variables such as age, sex, marital status, education, smoking, opium use, physical activity, wealth index and BMI and hypertension, univariate logistic regression analysis was first conducted, and in the next step, the variables included in the univariate analysis with a p < 0.25 were entered into multivariable logistic regression and adjusted ORs (AOR) and 95% CIs were estimated. The significance level was considered to be p < 0.05. Data were analyzed with the Statistical Package for Social Science (IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp) and Stata Statistical Software (Stata 14 for windows, Stata Corp., College Station, TX, USA) software.
Results
A total of 1245 people with type 2 diabetes aged 35–70 years were included. The average age of the participants was 53.5 ± 8.7 years.
Demographic characteristics
In this study, 71.7% of all participants were women. Table 1 shows the demographic and socioeconomic characteristics of the participants separately for men and women.
Prevalence of hypertension
The prevalence of hypertension in people with type 2 diabetes was 45.5%. The prevalence of hypertension in women was higher than in men (49.9% vs. 34.1%). According to the results, 32.6% of smokers and 47.0% of non-smokers had hypertension. The prevalence of hypertension was higher in married people than singles, divorcees and widows (56.9% vs. 43.7%). Also, the prevalence of hypertension was lower in people with high physical activity compared to those with moderate and low physical activity, so that 37.3% of people with high physical activity, 46.6% of people with moderate physical activity, and 52.4% of those with low physical activity had high blood pressure. Hypertension was more common in overweight (46.6%) and obese (57.6%) people than in those who were normal weight or underweight (35.1%) (Table 2).
In the whole population, according to age grouping, the prevalence of hypertension was higher in people aged 65 and older compared to younger age groups. Thus, 63.1% of people aged 65 and over, 55.0% of people aged 55–64, 43.4% of people aged 45–55, and 17.5% of people aged 35–44 had hypertension. In men, the prevalence of hypertension increases with age, so that 6.8% of people aged 35–44, 32% of people aged 45–54, 42.6% of people aged 55–64, and 50% of people aged 65 and over had hypertension. In women, the prevalence of hypertension has increased with age, so that 21.3% of people aged 35–44, 47.4% of people aged 45–54, 61% of people aged 55–64, and 66.7% of people aged 65 and over had hypertension (Fig. 2).

Prevalence of hypertension in age categories in type 2 diabetes patients. (a) Total population, (b) Males, (c) Females.
The results of the univariate analysis and multivariable-adjusted analysis are shown in Table 3. The variables included in the univariate analysis with a p < 0.25 were entered into multivariable logistic regression. According to the multivariable-adjusted analysis, there was a significant association between age and hypertension in diabetic patients, and this association became stronger with increasing age, so that the odds of hypertension for people aged 45–54 years (AOR: 4.0, 95% CI: 2.6–6.1), 55–64 years old (AOR: 6.5, 95% CI: 4.2–10.1) and 65 years and more (AOR: 8.1, 95% CI: 4.6–14.3). Also, a significantly higher prevalence of hypertension was observed in women vs. men (AOR: 1.8, 95% CI: 1.2–2.5). According to the results, being Fars (AOR: 1.6, 95% CI: 1.1–2.4) and being Turkish (AOR: 1.6, 95% CI: 1.1–2.5) also showed a significant association with high blood pressure. Moderate (AOR: 0.69, 95% CI: 0.51–0.94) and high (AOR: 0.57, 95% CI: 0.42–0.78) vs. low levels of physical activity showed inverse associations with hypertension. Overweight (AOR: 1.8, 95% CI: 1.3–3.3) and obesity (AOR: 2.7, 95% CI: 2.0–3.8) were also associated with increased odds of hypertension. However, marital status, smoking, opium use, education level, and wealth index showed no significant association with hypertension prevalence.
Discussion
This study was conducted with the aim of determining the prevalence and risk factors of hypertension in type 2 diabetes patients in the Fasa cohort population. The results showed that the prevalence of hypertension in people with type 2 diabetes was 45.5%. Also, the results of adjusted analysis showed that age, gender, ethnicity, physical activity and BMI were associated with the prevalence of hypertension.
The prevalence of hypertension varies in different regions of the world. But two-thirds of high blood pressure cases are observed in LMICs7. In a recent study conducted in Iran, Rabizadeh et al. reported the prevalence of hypertension in people with type 2 diabetes as 36.1%25, which was lower than the results of the present study.
Increasing age showed a strong positive association with hypertension. The odds of hypertension in the age groups of 45–55, 55–64 and > = 65 years was 4, 6.5 and 8.1 times that of the age group of 35–44 years, respectively. These results are in line with the results of previous studies25,26,27. On the other hand, it should be kept in mind that with the increase in life expectancy and the increase in the aging population, the prevalence of hypertension and type 2 diabetes is continuously increasing in the population28,29.
In this study, the hypertension prevalence in women was 1.8 times that of men. Rabizadeh et al. reported that the prevalence of hypertension in women with type 2 diabetes is significantly higher than in men25. Although in other studies no significant difference was reported in hypertension prevalence between women and men with type 2 diabetes26.
Hypertension prevalence was higher in type 2 diabetes patients who belonged to Fars or Turk ethnic groups than in other ethnic groups. Studies have also shown that the prevalence of type 2 diabetes is different in different ethnic groups5. There is also evidence that the prevalence of hypertension is different in people of different regions of Iran30.
Physical activity was inversely associated with prevalence of hypertension in type 2 diabetes patients, with odds ratios of 0.57 for high and 0.69 for moderate activity when compared to low physical activity, respectively. The results of the present study are consistent with the results of several other studies31,32,33. There is evidence that physical activity has protective effects on both diabetes and hypertension34,35,36,37. Considering the protective role of physical activity on hypertension in type 2 diabetes patients, it is necessary to develop intervention and educational programs and create infrastructures to increase physical activity.
The results showed that increasing BMI was strongly positively associated with prevalence of hypertension in the current study. This is consistent with several other studies26,38. The evidence indicates that obesity, like inactivity and unhealthy diet, is a strong and modifiable risk factor for diabetes and hypertension39. It should be noted that in this study, among the factors related to hypertension, age, gender and ethnicity cannot be modified, but physical activity and BMI can be modified. Therefore, developing interventions and educational strategies to modify lifestyle, including increasing physical activity and improving adherence to healthy diets can be useful and may prevent hypertension in type 2 diabetes patients. Care providers should accurately measure the blood pressure of diabetes patients at each visit. Also, people with type 2 diabetes should be encouraged to perform periodic examinations and regular check-ups, and if diagnosed with hypertension, the complications of hypertension can be prevented with timely and correct treatment.
Study strengths and limitations
Strengths of the current study include the large sample size, with participants included from different ethnic groups, which may increase the generalizability of the results across the Iranian population. In this study, the weight and height of all subjects were measured by trained personnel. The most important limitation of this study was its cross-sectional nature, which cannot determine whether the causal relationship due to the study design. Therefore, further prospective studies are needed in this population to determine in what proportion of people with type 2 diabetes, hypertension occurs.
Conclusion
The prevalence of hypertension in type 2 diabetes patients was 45.5%. We found positive associations between age, female gender, Fars or Turk vs. other ethnicity and BMI and hypertension prevalence, while an inverse association was observed with physical activity. Further prospective studies are needed to investigate these associations in this population.
Data availability
All data generated or analyzed during this study are available from the corresponding author on reasonable request.
References
Zimmet, P. Z., Magliano, D. J., Herman, W. H. & Shaw, J. E. Diabetes: A 21st century challenge. Lancet Diabetes Endocrinol. 2(1), 56–64 (2014).
WHO/Diabetes/https://www.who.int/health-topics/diabetes#tab=tab_1/Date accessed:26 December 2023.
Saeedi, P. et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes Atlas. Diabetes Res. Clin. Pract. 157, 107843 (2019).
Oraii, A. et al. Prevalence, awareness, treatment, and control of type 2 diabetes mellitus among the adult residents of Tehran: Tehran Cohort Study. BMC Endocr. Disord. 22(1), 248 (2022).
Khamseh, M. E. et al. Nationwide prevalence of diabetes and prediabetes and associated risk factors among Iranian adults: Analysis of data from PERSIAN cohort study. Diabetes Ther. 12, 2921–2938 (2021).
Cryer, M. J., Horani, T. & DiPette, D. J. Diabetes and hypertension: a comparative review of current guidelines. J. Clin. Hypertens. 18(2), 95–100 (2016).
WHO, Hypertension. https://www.who.int/news-room/fact-sheets/detail/hypertension. Date accessed:26 December 2023.
Turk-Adawi, K. et al. Cardiovascular disease in the Eastern Mediterranean region: Epidemiology and risk factor burden. Nat. Rev. Cardiol. 15(2), 106–119 (2018).
Najafipour, H. et al. Prevalence and incidence of pre-hypertension and hypertension (awareness/control) in Iran: Findings from Kerman coronary artery diseases risk factors study 2 (KERCADRS). J. Hum. Hypertens. 36(5), 461–472 (2022).
Baskar, V., Kamalakannan, D., Holland, M. & Singh, B. Does ethnic origin have an independent impact on hypertension and diabetic complications?. Diabetes Obes. Metab. 8(2), 214–219 (2006).
Aune, D., Huang, W., Nie, J. & Wang, Y. Hypertension and the risk of all-cause and cause-specific mortality: An outcome-wide association study of 67 causes of death in The National Health Interview Survey. Biomed. Res. Int. 2021(1), 9376134 (2021).
Rapsomaniki, E. et al. Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet. 383(9932), 1899–1911 (2014).
Forouzanfar, M. H. et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. Jama. 317(2), 165–182 (2017).
WHO. Home/News/First WHO report details devastating impact of hypertension and ways to stop it. Available at: https://www.who.int/news/item/19-09-2023-first-who-report-details-devastating-impact-of-hypertension-and-ways-to-stop-it. Date accessed: 19 September 2023.
Baffour, P. K., Jahangiry, L., Jain, S., Sen, A. & Aune, D. Blood pressure, hypertension, and the risk of heart failure: A systematic review and meta-analysis of cohort studies. Eur. J. Prev. Cardiol. 31(5), 529–556 (2024).
Aune, D. et al. Blood pressure, hypertension and the risk of atrial fibrillation: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 38(2), 145–178 (2023).
Hibino, M. et al. Blood pressure, hypertension, and the risk of aortic dissection incidence and mortality: results from the J-SCH study, the UK biobank study, and a meta-analysis of cohort studies. Circulation. 145(9), 633–644 (2022).
Kobeissi, E., Hibino, M., Pan, H. & Aune, D. Blood pressure, hypertension and the risk of abdominal aortic aneurysms: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 34, 547–555 (2019).
Pan, H., Hibino, M., Kobeissi, E. & Aune, D. Blood pressure, hypertension and the risk of sudden cardiac death: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 35(5), 443–454 (2020).
Collaboration, E. R. F. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 364(9), 829–841 (2011).
Fuchs, F. D. & Whelton, P. K. High blood pressure and cardiovascular disease. Hypertension. 75(2), 285–292 (2020).
Madsen, H., Sen, A. & Aune, D. Fruit and vegetable consumption and the risk of hypertension: A systematic review and meta-analysis of prospective studies. Eur. J. Nutr. 62(5), 1941–1955 (2023).
Farjam, M. et al. A cohort study protocol to analyze the predisposing factors to common chronic non-communicable diseases in rural areas: Fasa cohort study. BMC Public Health. 16(1), 1–8 (2016).
Homayounfar, R. et al. Cohort profile: The Fasa adults cohort study (FACS): A prospective study of non-communicable diseases risks. Int. J. Epidemiol. 52(3), e172–e178 (2023).
Rabizadeh, S. et al. Uncontrolled hypertension in patients with type 2 diabetes: What are the correlates?. J. Clin. Hypertens. 23(9), 1776–1785 (2021).
Akalu, Y. & Belsti, Y. Hypertension and its associated factors among type 2 diabetes mellitus patients at Debre Tabor general hospital, northwest Ethiopia. Diabetes, Metab. Syndr. Obes. 1621–1631 (2020).
Choukem, S. P., Kengne, A. P., Dehayem, Y. M., Simo, N. L. & Mbanya, J. C. Hypertension in people with diabetes in sub-Saharan Africa: Revealing the hidden face of the iceberg. Diabetes Res. Clin. Pract. 77(2), 293–299 (2007).
Ekpenyong, C. E., Akpan, U., Ibu, J. O. & Nyebuk, D. E. Gender and age specific prevalence and associated risk factors of type 2 diabetes mellitus in Uyo metropolis, South Eastern Nigeria. Diabetol. Croat. 41(1), 17–29 (2012).
Ogah, O. S. et al. Blood pressure, prevalence of hypertension and hypertension related complications in Nigerian Africans: A review. World J. Cardiol. 4(12), 327 (2012).
Oori, M. J. et al. Prevalence of HTN in Iran: Meta-analysis of published studies in 2004–2018. Curr. Hypertens. Rev. 15(2), 113–122 (2019).
Motuma, A. et al. Co-occurrence of hypertension and type 2 diabetes: Prevalence and associated factors among Haramaya University employees in Eastern Ethiopia. Front. Public Health. 11, 1038694 (2023).
Ambelu, T. & Teferi, G. The impact of exercise modalities on blood glucose, blood pressure and body composition in patients with type 2 diabetes mellitus. BMC Sports Sci., Med. Rehab. 15(1), 153 (2023).
Duclos, M., Dejager, S., Postel-Vinay, N., di Nicola, S., Quéré, S. & Fiquet, B. Physical activity in patients with type 2 diabetes and hypertension–insights into motivations and barriers from the MOBILE study. Vasc. Health Risk Manag. 361–371 (2015).
Colberg, S. R. et al. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care. 39(11), 2065 (2016).
Diaz, K. M. et al. Physical activity and incident hypertension in African Americans: The Jackson heart study. Hypertension. 69(3), 421–427 (2017).
Hayes, P., Ferrara, A., Keating, A., McKnight, K. & O’Regan, A. Physical activity and hypertension. Rev. Cardiovasc. Med. 23(9), 302 (2022).
Aune, D., Norat, T., Leitzmann, M., Tonstad, S. & Vatten, L. J. Physical activity and the risk of type 2 diabetes: A systematic review and dose–response meta-analysis. Eur. J. Epidemiol. 30, 529–542 (2015).
Abougalambou, S. S. I. & Abougalambou, A. S. A study evaluating prevalence of hypertension and risk factors affecting on blood pressure control among type 2 diabetes patients attending teaching hospital in Malaysia. Diabetes Metab. Syndr. Clin. Res. Rev. 7(2), 83–86 (2013).
Jiang, S. Z., Lu, W., Zong, X. F., Ruan, H. Y. & Liu, Y. Obesity and hypertension. Exp. Ther. Med. 12(4), 2395–2399 (2016).
Acknowledgements
We would like to thank Jahrom University of Medical Sciences, Jahrom, Iran and Fasa University of Medical Sciences, Fasa, Iran who cooperated with us in conducting this research.
Funding
Jahrom University of Medical Sciences provided facilities.
Author information
Authors and Affiliations
Contributions
F.R. and A.T. designed the study design. F.R., M.R. and A.D. did the analyses. F.R., A.T., R.K.H., and D.A. were responsible for data interpretation. R.K.H., A.D., M.R., and D.A. drafted the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Taheri, A., Khezri, R., Dehghan, A. et al. Hypertension among persons with type 2 diabetes and its related demographic, socioeconomic and lifestyle factors in the Fasa cohort study. Sci Rep 14, 18892 (2024). https://doi.org/10.1038/s41598-024-69062-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-69062-7
- Springer Nature Limited