
Abstract
The safety of exercise practice by individuals with cardiovascular disease is due to a good clinical evaluation to identify patients with a higher risk of adverse events, thus the study of simple variables capable of predicting the rate of events during exercise is relevant and may provide better screening tools to be applied in the clinical practice. The study aimed to evaluate if clinical and physical parameters can predict the rate of adverse events during exercise-based cardiac rehabilitation. This was a cohort study that followed 73 patients during 24 sessions of exercise. Were registered 217 simple adverse events, at a rate of 2.5 events per hour of exercise. We found that higher adiposity, worse pulmonary function, lower functional capacity, and reduced heart rate variability were significant and acceptable predictors of adverse events during exercise, according to the ROC curve analysis. We state that these simple physical parameters may be useful for cardiac risk stratification in cardiac rehabilitation programs with low resources, contributing to its safety.
Similar content being viewed by others


Introduction
Exercise-based cardiac rehabilitation (CR) is level A of evidence and grade I of recommendation for primary and secondary prevention of cardiovascular diseases (CVD)1. CR enhances physical and emotional aspects, favors functional independence, and reduces hospitalizations and mortality rates2. However, despite the supervised setting, exercise may trigger major adverse events (AE) such as sudden cardiac death and myocardial infarction3. Fortunately, the occurrence of major AE is very low, the higher rates were registered long ago in the early 70s, being one major event per 15 000 h of exercise4. Nowadays, the last measure published in 2020 revealed an average of one sudden cardiac death for every 219 970 h of exercise3. This is also applied when high-intensity interval training is performed in CR, the major events occurrence rate is approximately one event per 2 227 h5. This low occurrence may be associated with the monitorization of minor AE, once the major cardiac events are often preceded by those of minor gravity6. Surprisingly, the occurrence of minor events such as fatigue, muscle pain, angina, and dizziness, is relatively high, ranging from 3.57 to 25.6 h of CR to occur one minor AE8. Thus, identifying patients more susceptible to these events is essential to guide an adequate level of monitoring and exercise intensity prescription.
Most minor AE are signs and symptoms of exercise intolerance. Patients with CVD are more susceptible to triggering these minor AE due to diverse factors, such as cardiac output limitation, altered vascular function, low muscular strength, and its compromised metabolism, altered pulmonary function, high adiposity, sympathetic hyperactivation, and altered electric conductivity of cardiomyocytes9,10,11. Thus, we hypothesize that measures of resting heart rate, cardiac autonomic modulation, muscular strength, pulmonary function, body composition, and functional capacity may be useful in predicting the occurrence of minor AE during exercise.
Based on these aspects this study aimed to evaluate if physical (body composition, pulmonary function, muscular strength, cardiac autonomic modulation, functional capacity, and cardiovascular resting parameters) and clinical (age, clinical diagnosis, and cardiac risk factors) parameters can predict the occurrence of minor AE during exercise-based CR.
Results
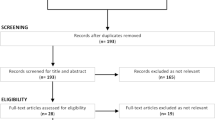
Were recruited 79 participants of a CR program, after the sample losses the number of participants included in the analysis varied among the outcomes as detailed in Fig. 1.

Participants flow chart. N number, HRV heart rate variability, WHR waist-to-hip ratio, rMSSD root square of the mean of the square of the differences between adjacent normal RR intervals of the series, SDNN standard deviation of the mean of all normal RR intervals in the series, LF low-frequency spectral component, HF high-frequency spectral component, LF/HF the ratio between low- and high-frequency components, SD1 dispersion of the points perpendicular to the line with the smallest diameter of the ellipse, SD2 dispersion of the points perpendicular to the line with the largest diameter of the ellipse, SD1/SD2 ratio between the short- and long-term components of RR intervals, ms milliseconds, ms2 milliseconds squared, u.n. standardised units, HR resting heart rate, SBP systolic blood pressure, MEP maximal expiratory pressure, FVC forced vital capacity, FEV1 forced expiratory volume in the 1st second.
The sample was composed predominantly of male participants, over 60 years of age, with the main diagnosis of coronary artery disease and hypertension as the main cardiac risk factors (eTable 1). The physical characteristics are shown in eTable 2, in general, the population was overweight, had high body adiposity, impaired respiratory muscle strength, low functional capacity, and cardiac autonomic modulation within the expected range for the elderly population with CVD.
Occurrence of adverse events (AE)
During the study 217 AE were registered, an average of 2.5 ± 3.0 events occurred per session and only 20 (24.7%) participants did not report any AE.
Figure 2A contains the breakdown of the type of event and the period it occurred during the session. Most of the events occurred during exercise (ergometry and warm-up), and only 15.9% of the events were recorded during the cool-down. The number of events recorded per patient ranged from 1 to 20, but 77.4% of the participants reported 1–3 events (Fig. 2B).

Characteristic of the occurrence of events. Representation of the absolute number of events recorded during exercise and recovery (A) and absolute number of participants stratified by the number of events recorded over the follow-up period (B). N/A not applicable.
Relationship between clinical and physical parameters and AE
To report all data and analysis we created a repository at https://zenodo.org (https://doi.org/10.5281/zenodo.10372903). All data not included in the body of the text is available there.
The relationship between clinical characteristics and AE assessed by binary logistic regression was not statistically significant for any of the models studied (eTable 3).
The significant relationships between physical parameters and AE are reported in the body of the text, however, when the same variable was significant in more than one model, the result presented was the one with the highest odds ratio, the other models are available in the repository.
The variables body mass index (BMI), body adiposity index (BAI), forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), and LF (n.u) are associated with the occurrence of at least three events, while body fat percentage, resting HR, quadriceps muscle strength, and percentage of FVC are associated with the occurrence of at least six events. Finally, the distance covered in the six-minute walk test (6MWT), and LF/HF ratio were associated with the occurrence of at least one event and percentage of maximal expiratory pressure (MEP) with at least two events (Fig. 3).

Univariable logistic regression, cutoff value, and number of events associated with the observed risk of adverse events. OR odds ratio, 95% CI 95% confidence interval, BMI body mass index, Kg/m2 kilogram per square meter, 6MWT 6 min walk test, m meters, HR heart rate, bpm beats per minute, % percentage, bpm beats per minute, N Newton, MEP maximal expiratory pressure, FVC forced vital capacity, FEV1 forced expiratory volume in the 1st second, L liters, LF low-frequency spectral component, LF/HF ratio between low- and high-frequency components, n.u. normalized units. *Cutoff defined by the 3rd quartile, †Cutoff defined by the median, §Cutoff defined by the 33% percentile.
The quality of the predictors identified in the regression was evaluated by the area under the curve (AUC) (Table 1). The variables with acceptable predictive power (AUC > 0.7)12 were BAI, body fat percentage, distance covered in the 6MWT, FEV1 (L), LF (u.n), and LF/HF ratio, and percentage values of MEP and FVC. It was also possible to note that most of the variables showed greater specificity than sensitivity.
The variables with significant and acceptable AUC are illustrated in eFig. 1 and were included in multivariate regression models (Table 2) as follows: A. Body composition (Body fat and BAI); B. Lung capacity (FVC and FEV1); and C: Cardiac autonomic modulation (LF u.n. and LF/HF ratio). Regarding MEP and distance covered in the 6MWT, no multivariate analysis was performed due to the lack of significance in similar variables.
Discussion
The main results of this study reveal that measures of body composition, pulmonary function, functional capacity, and cardiac autonomic modulation are specific tests with acceptable predictive power to identify individuals with higher chances of presenting AE during exercise in CR programs. The most prevalent AE were fatigue, and muscle and chest pain, which are the initial manifestations of exercise intolerance in individuals with CVD, that usually precede events with a worse prognosis6.
The physiological basis for these results may be mainly related to the reduced physical fitness, that favors the early occurrence of signs and symptoms of exercise intolerance13,14. The low physical fitness in these populations may be related to a great range of abnormalities in the main body organic systems, such as reduced pulmonary function15, cardiac output limitation and reduced blood flow to active tissues14, altered uptake and utilization of oxygen by skeletal muscle16, sympathetic nervous system hyperactivity over the heart and vasculature17, and altered lipid profile18. In line with these concepts, our sample had low functional capacity19, high adiposity20, weakened respiratory muscles21, restrictive respiratory disorder22, and reduced HRV23. Thus, the relationship between the distance covered in the 6MWT and AE may reflect the effect of the cluster of alterations inherent to the CVD (eFig. 2).
Specifically for high adiposity, it promotes chronic inflammation, which alters endothelial function and afterload, contributing to cardiac overload and limited flow supply18. As for skeletal muscles, it favors the installation of insulin resistance, reduction of mitochondrial content, and the number of type I fibers, factors that contribute to the reduction of oxidative capacity and the early production of lactate16, favoring muscle fatigue and pain11, two of the most prevalent AE in the study.
The quality and mechanics of the ventilatory response during exercise are other factors that contribute to the development of fatigue and dyspnea in individuals with CVD. These individuals have an exaggerated ventilatory response at low loads, reduced lung compliance, and high airway resistance. The development of these abnormalities may be due to chronic inflammation, once the deterioration of the pulmonary elastic component is related to the presence of pro-inflammatory factors. As for the exaggerated ventilatory response, it is due to excessive stimulation of the respiratory center via chemoreflex, in face of the altered muscle metabolism15,24. Corroborating with this concept, the value of FEV1 predicted the occurrence of AE, and a previous study has shown that there is an inverse relationship between FEV1 values and the concentration of C-reactive protein in the plasma25, strengthening the role of inflammation in the clinical manifestations of exercise intolerance in CVD.
On the other hand, the relationship between MEP and the occurrence of AE is innovative. To this date, the role of expiratory muscles in limiting physical effort has been little studied and the results are controversial. A possible hypothesis that explains the result obtained may be related to the early fatigue of the weakened expiratory muscles, as Taylor & Romer reported that in healthy individuals the exercise performed after the induction of expiratory fatigue resulted in higher subjective perceptions of muscle pain and dyspnea26.
The cardiovascular responses to exercise are modulated by the autonomic nervous system, individuals with CVD have a sympathetic overactivity, which is initially installed as a compensatory mechanism to increase cardiac output, however, in the long term, it is associated with negative outcomes17, and our study reinforces this concept as the lower the HRV the higher the AE occurrence. Specifically, for the LF index, which in our study was the index with the strongest predictive power over AE, evidence has suggested that it is strongly related to the concentration of pro-inflammatory agents in plasma27. Therefore, this autonomic profile contributes to the perpetuation of the chronic inflammatory condition, corroborating our other findings.
The results of our study are innovative and advance the knowledge in the field by demonstrating that simple clinical variables have the potential to be included as a cardiac risk stratification tool to be used in CR programs to provide more individualized treatment, especially in rehabilitation centers with low resources, as the measures used to estimate the risk are cheap and easily obtainable. We highlight the possibility that the cut-off values established here may be used in future research as a means of comparing groups and analyzing the effect of interventions. However, the recruitment carried out by convenience in a single rehabilitation center may represent a selection bias, thus we encourage as future research the replication of our study in larger and more diverse populations to validate the predictive models and ensure their generalization across different settings and demographics. Moreover, future research should also address the long-term predictive value of the identified parameters and their impact on diverse patient outcomes.
We conclude that the occurrence of simple AE during CR can be acceptably predicted by the absolute values of BAI, body fat percentage, 6MWT, FEV1, LF (u.n) and LF/HF ratio, and percentage values of MEP and FVC.
Methods
Study design and ethical aspects
This was a prospective observational longitudinal study (registered at clinicaltrials.com—NCT04790643) and reported according to the “Strengthening the Reporting of Observational Studies in Epidemiology”28. At first, data were collected for all physical and clinical variables, after that the volunteers were followed up by independent researchers for 2 months during 24 routine sessions of CR to register the occurrence of minor AE. The data collection and follow-up were carried out between September 2021 and October 2022.
All procedures were approved by the Ethical Research Committee of São Paulo State University Campus of Presidente Prudente, São Paulo, Brazil (CAAE: 35831220.8.0000.5402), were under the Declaration of Helsinki and were performed according to the current guidelines regulating each physical test. All volunteers were informed about the objectives and procedures of the study and signed a consent form.
Participants
The population was composed of males and females included in the CR program carried out at an outpatient school clinic of physiotherapy located in Presidente Prudente, São Paulo, Brazil. Recruitment was made by convenience and all participants of the program were evaluated for eligibility by an independent researcher. Eligible patients were those with a main diagnosis of any CVD or with at least one cardiac risk factor (obesity, arterial hypertension, dyslipidemia, diabetes mellitus, and family history)29.
The inclusion criteria were not having orthopedics and/or neurologic disorders that could interfere with the physical evaluations, and not having a known lung disease, to minimize potential confounders in the pulmonary evaluations. Were excluded those who didn’t accomplish 24 sessions of exercise in the follow-up period, and those who had any alteration of the medication of daily use during follow-up. It is important to highlight that if the participants weren’t capable of correctly performing the respiratory maneuvers, and/or weren’t allowed to be submitted to bioelectrical impedance and/or presented errors greater than 5% in the RR intervals series were excluded from the analysis of these specific outcomes. Also, we performed an outlier filtering by outcome, thus values detected as outliers were excluded from the final analysis.
For the sample characterization was extracted from the patient’s medical record the presence of associated diseases, age, sex, period of treatment in CR, and medication of daily use. Also, for characterization purposes, the patient was asked the following question for assessment of stress: “Do you consider yourself a stressed person and/or that you suffer too much stress in your daily life?” if the response was affirmative, we considered that the risk factor of stress was present. The level of physical activity was evaluated by self-report according to the World Health Organization recommendation30.
Physical evaluation
Cardiovascular parameters
Resting heart rate (HR) was measured using the Polar RS800CX HR monitor (Polar Electro OY, Finland)31 in the supine position for 20 min. The average obtained between the 5th and 20th min was analyzed.
Blood pressure was measured using a stethoscope (Littmann, Saint Paul, USA) and an aneroid sphygmomanometer (Welch Allyn-Tycos, New York, USA). Three measurements were taken over 15 min in a sitting position. The average of the last two measurements was analyzed32.
Respiratory parameters
The peak expiratory flow (PEF), forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio, were obtained through spirometry33 (MIR-Spirobank II–Mini Spirometer, Italy).
Maximum expiratory (MEP) and inspiratory (MIP) pressures were assessed through a manuvacuometer (GerAr®, Brazil). The average of the 3 values obtained in maneuvers sustained for at least 1 s with no air leak was analyzed34.
All respiratory parameters were analyzed as raw values and the percentage achieved from the predicted, considering formulas validated for the Brazilian population21,35.
Cardiac autonomic modulation
Cardiac autonomic modulation was assessed using HR variability (HRV), recorded through the Polar RS800CX (Polar Electro OY, Finland)31.
Participants were instructed to abstain from stimulant substances and not to perform vigorous physical activities for 24 h. The HRV was assessed in a calm and thermoneutral environment, with the participant in the supine position, absolute rest, and spontaneous breathing for 30 min36. A series of 1000 consecutive RR intervals obtained between the 5th and 30th min were analyzed after digital (Polar ProTrainer 5 software, version 5.40) and visual filtering to eliminate premature beats and artifacts.
The indices analyzed were RMSSD; SDNN; LF (low-frequency spectral component ranging from 0.04 to 0.15 Hz) and HF (high-frequency spectral component ranging from 0.15 to 0.4 Hz) both expressed in milliseconds squared (ms2) and in normalized units (un); LF/HF ratio; SD1; SD2; SD1/SD2 ratio37. These indices were calculated at the Kubios HRV Standard software—version 3.0.038.
Quadriceps muscular strength
It was assessed using a digital dynamometer (Meditec, Brazil). The test consisted of three maximal isometric contractions from a 60º angle of knee flexion, with the body stabilized. The contractions lasted 5 s and had an interval of 30 s between them. The value considered was the highest peak strength measured among them39.
Submaximal functional capacity
Functional capacity was assessed by the 6 min walk test (6MWT). Two tests were performed on the same day with a minimum interval of 30 min, and the test with the longest distance was analyzed40.
Anthropometric measures
Were evaluated body mass index (BMI), waist-hip ratio (WHR)41, conicity index42, abdominal volume index43, and body adiposity index (BAI)44.
To obtain BMI, body mass was measured using a digital scale (Wiso, Digital Scale, W939 Body Analyzer, China) and height was assessed using a stadiometer (Sanny, Personal Caprice, Brazil). For the WHR and the conicity, abdominal volume and body adiposity indices were measured waist circumference at the smallest abdominal circumference; abdominal circumference at the umbilical line; and hip circumference at the greatest circumference in the gluteal region.
Body composition
Using a tetrapolar bioelectrical impedance45 (BIODYNAMICS, 310e, Seattle-USA) were evaluated the percentage of body fat, lean mass, and phase angle. During the exam, participants remained in the supine position with the electrodes positioned in the right hand and foot46.
Participants were instructed not to ingest any food or beverages for 4 h, not to perform physical exercises for 12 h, not to drink alcoholic beverages for 48 h, and to empty the bladder 30 min before the test. As a safety measure, the participants didn’t interrupt the diuretic medication46.
Cardiac rehabilitation program
The CR program was carried out at the Physiotherapy Study and Care Center located at Presidente Prudente, São Paulo, Brazil, an outpatient school clinic. The CR sessions were performed three times a week on alternate days in a room with controlled temperature (22–24 °C).
The sessions consisted of initial rest (5 min), warm-up (15 min), aerobic exercise (30 min) and cool-down (10 min). The initial rest period was dedicated to the evaluation of resting HR and blood pressure. The exercise period started with the warm-up, composed of stretching and varied free active exercises of progressive level of effort. After the warm-up, the participant performed a moderate-intensity continuous aerobic exercise on a treadmill or exercise bike. At the end of the aerobic exercise, the participants walked at a slow pace around the room and seated for cool-down.
The aerobic exercise intensity was set at 40–80% of the HR reserve, according to the ACSM recommendation29. The resting HR was extracted from the previous three sessions of CR before the baseline assessment. As for the maximum HR it was extracted from a stress test performed whiting the last year that was attached to the medical record, however, for those who did not have a recent stress test report, the formula of 220-age was used.
Register of adverse events
The AE were selected based on the study of Vanderlei et al. which identified the most prevalent AE in exercise-based CR8. We considered AE the: abnormal rise of systolic blood pressure during exercise, considering values ≥ 200 mmHg; muscle pain, considered as any discomfort referred in the skeletal muscles in any region of the body; fatigue, considered as a physical unpleasant sensation referred as tiredness that doesn’t ease with strategies to restore energy and accompanied by cognitive and emotional components; dizziness, referred as a sensation of altered body balance and spatial disorientation; and chest pain, considered as pain or discomfort of constrictive, compressive, or burning nature at the substernal or interscapular region, neck, mandible, arms, and fingers8, however, due to logistics was not possible to assess with an electrocardiogram if the report of chest pain was associated with actual ST alteration.
The presence of any of the symptoms tracked was asked by the physician at least one time in each session phase (rest, warm-up, aerobic exercise, and cool-down). Also, to ensure reliability, all participants were instructed regarding the definition of the symptoms and the importance of not omit any discomfort. Therefore, we considered as “adverse event” the report of any symptom during the CR session. Each report was counted as “one event”, however, events reported in the initial rest that were maintained or not during the exercise period were not included in the analyses (eFig. 3). The AE outcome consisted of the absolute value of events recorded throughout the follow-up period per participant, value used to develop the dichotomic models of analysis.
Due to the subjective characteristic of the AE tracked when reported, they were assessed concerning its intensity through a five-point Likert scale, being 1 very low and 5 maximum, to guide the conduct of care to ensure safety. When any symptom was reported the exercise load was reduced and the intensity of the discomfort was assessed again. If the symptom worsened or did not cease the exercise was interrupted and the participant would be referred to a medical center for further investigation. It is worth mentioning that during the study none patients had severe symptoms that required medical interventions.
Statistical analysis
The characterization variables were analyzed using descriptive statistics. The relationship between the dependent (occurrence of events) and independent (physical and clinical characteristics) variables was analyzed using uni and multivariable binary logistic regression.
The accuracy of the univariate models was quantified by the area under the ROC curve (AUC), and for the multivariable models the quality of the model fit was evaluated by the Hosmer–Lemeshow test, and for internal validity, simple bootstrap resampling analysis was performed based on the seed “2000000” for the generation of Mersenne Twister random numbers considering 100 samples with bias-corrected and accelerated 95% confidence interval.
The dependent variable, the occurrence of AE, was categorized into six models considering the occurrence of 1 to 6 AE, to this aim, the occurrence of AE in each model was defined as “positive” or “negative” accordingly to the following: model 1 (0 events = negative/1 or more = positive); model 2 (0 or 1 event = negative/2 or more = positive; model 3 (at most 2 events = negative/3 or more = positive); model 4 (at most 3 = negative/4 or more = positive), model 5 (at most 4 = negative/5 or more = positive) and model 6 (at most 5 = negative/6 or more = positive). After an outlier filtering based on the study of Hoaglin & Iglewicz47, physical variables were categorized into three models based on: (a) the median; (b) the 33% and 66% percentiles to obtain three groups with a similar sample size, and, (c) the first quartile cut-off for those variables in which a low value represents worse performance or third quartile for variables in which a high value represents worse performance. Clinical variables were categorized as “presence” or “absence” of the characteristic.
The analyses were performed using IBM SPSS Statistics—version 22.0 (IBM Corp, Armonk, New York) and MedCalc—version 14.8.1 (MedCalc Software, Ostend, Belgium) considering a statistical significance of less than 5%.
Missing data
There were missing data for the baseline characteristics evaluated. All missing data consisted of participants that for any reason, as described in the previous sections, did not perform some of the evaluations or had the obtained value considered an outlier. In these cases, we applied the deletion method, removing the participant only from the analysis of the specific outcome in which the data is missing. It is important to highlight that from all outcomes six participants were excluded due to a loss of follow-up, as pointed in Fig. 1.
The percentage of missing data per outcome, considering only the losses due to the absence of the evaluation and outlier filtering was: 27.8% for muscle strength, of which 21 participants did not perform the test and 1 was considered an outlier; 17.7% for 6MWT, of which 13 did not perform the test and one was considered an outlier; 21.5% for MIP due to incorrect maneuver and 27.8% for MEP, as additional five participants were considered as outliers; 16.4% for FVC, PEF, and FEV1 due to incorrect maneuver, and 17.7% for FEV1/FVC as one participant was identified as an outlier; 15.2% for the HRV indices of LF and HF in normalized units, SD1, SD2, and SD1/SD2 ratio as 11 participants did not perform the evaluation and one was an outlier; 17.7% for rMSSD, SDNN, and LF in ms2 that had three outliers excluded; 19% for LF/HF ratio due to four outliers; and 21.5% for HF ms2 due to six outliers; 1.3% for WHR and SBP due to one outlier and 2.5% for BAI and HR due to two outliers.
Sample size
The sample power was analyzed considering the analysis of AUC. The expected ratio between negative and positive cases was set at 0.6 estimated based on the previous study from our research group with a different set of participants from the same cardiac rehabilitation program6. The null hypothesis considered was an AUC of 0.5, the expected effect was set at an AUC of 0.79, alpha error at 0.05, and the power at 80%. The resulting sample was 66 participants, and accounting for 10% of sample loss the intended sample size was 73 participants.
Data availability
All anonymized data and analysis results supporting this study's findings are available in Zenodo with the identifier https://doi.org/10.5281/zenodo.10372903.
References
American Association of Cardiovascular & Pulmonary Rehabilitation. Guidelines for Cardiac Rehabilitation Programs. (Human Kinetics, Champaing, 2021).
Dalal, H. M., Doherty, P. & Taylor, R. S. Cardiac rehabilitation. BMJ (Online) 351, (2015).
Thompson, P. D. et al. Exercise and acute cardiovascular events placing the risks into perspective: A scientific statement from the American heart association council on nutrition, physical activity, and metabolism and the council on clinical cardiology. Circulation 115, 2358–2368 (2020).
Fletcher, G. F. & Cantwell, J. D. Ventricular fibrillation in medically supervised cardiac exercise programs: Clinical, angiographic, and surgical correlation. JAMA 238, 2627–2629 (1997).
Wewege, M. A., Ahn, D., Yu, J., Liou, K. & Keech, A. High-intensity interval training for patients with cardiovascular disease—Is it safe? A systematic review. J. Am. Heart. Assoc. https://doi.org/10.1161/JAHA.118.009305 (2018).
Rabinstein, A. A. Sudden cardiac death. In Handbook of Clinical Neurology 19–24 (Elsevier, 2014).
Ribeiro, F. et al. An investigation into whether cardiac risk stratification protocols actually predict complications in cardiac rehabilitation programs?. Clin. Rehabil. 35, 775–784 (2021).
Vanderlei, L. C. M. et al. Analysis of signs and symptoms in ambulatorial programs of physical exercises for cardiac patients. Arq. Ciênc. Saúde 13, 69–74 (2006).
Noakes, T. D. Physiological models to understand exercise fatigue and the adaptations that predict or enhance athletic performance. J. Med. Sci. Sports 10, 123–145 (2000).
Kitzman, D. W. Exercise intolerance. Prog. Cardiovasc. Dis. 47, 367–379 (2005).
Ament, W. & Verkerke, G. J. Exercise and fatigue. Sports Med. 39, 389–422 (2009).
Mandrekar, J. N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 5, 1315–1316 (2010).
Guazzi, M., Bandera, F., Ozemek, C., Systrom, D. & Arena, R. Cardiopulmonary exercise testing: What is its value?. J. Am. Coll. Cardiol. 70, 1618–1636 (2017).
Del Buono, M. G. et al. Exercise intolerance in patients with heart failure: JACC state-of-the-art review. J. Am. Coll. Cardiol. 73, 2209–2225 (2019).
Ramalho, S. H. R. & Shah, A. M. Lung function and cardiovascular disease: A link. Trends Cardiovasc. Med. 31, 93–98 (2021).
Mengeste, A. M., Rustan, A. C. & Lund, J. Skeletal muscle energy metabolism in obesity. Obesity 29, 1582–1595 (2021).
Triposkiadis, F. et al. The sympathetic nervous system in heart failure revisited. Heart Fail. Rev. https://doi.org/10.1007/s10741-023-10345-y (2023).
Koliaki, C., Liatis, S. & Kokkinos, A. Obesity and cardiovascular disease: Revisiting an old relationship. Metab. Clin. Exp. 92, 98–107 (2019).
Dourado, V. Z. et al. Classification of cardiorespiratory fitness using the six-minute walk test in adults: Comparison with cardiopulmonary exercise testing. Pulmonology 27, 500–508 (2021).
Lee, M. M., Jebb, S. A., Oke, J. & Piernas, C. Reference values for skeletal muscle mass and fat mass measured by bioelectrical impedance in 390 565 UK adults. J. Cachexia Sarcopenia Muscle 11, 487–496 (2020).
Pessoa, I. M. B. S. et al. Predictive equations for respiratory muscle strength according to international and Brazilian guidelines. Braz. J. Phys. Ther. 18, 410–418 (2014).
Halpin, D. M. G. et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 203, 24–36 (2021).
Vanderlei, L. C. M., Pastre, C. M., Hoshi, R. A., Carvalho, T. D. & Godoy, M. F. Basic notions of heart rate variability and its clinical applicability. Rev. Bras. Cir. Cardiovasc. 24, 205–217 (2009).
Tumminello, G., Guazzi, M., Lancellotti, P. & Piérard, L. A. Exercise ventilation inefficiency in heart failure: Pathophysiological and clinical significance. Eur. Heart J. 28, 673–678 (2007).
Aronson, D. et al. Inverse association between pulmonary function and C-reactive protein in apparently healthy subjects. Am. J. Respir. Crit. Care Med. 174, 626–632 (2006).
Taylor, B. J. & Romer, L. M. Effect of expiratory muscle fatigue on exercise tolerance and locomotor muscle fatigue in healthy humans. J. Appl. Physiol. 104, 1442–1451 (2008).
Alen, N. V., Parenteau, A. M., Sloan, R. P. & Hostinar, C. E. Heart rate variability and circulating inflammatory markers in midlife. Brain Behav. Immun. Health 15, 100273 (2021).
Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 61, 344–349 (2008).
Pescatello, L., Arena, R., Riebe, D. & Thompson, P. ACSM’S Guidelines for Exercise Testing and Prescription (Lippincott Williams & Wilkins, 2014).
Bull, F. C. et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54, 1451–1462 (2020).
Vanderlei, L. C. M., Silva, R. A., Pastre, C. M., Azevedo, F. M. & Godoy, M. F. Comparison of the polar S810i monitor and the ECG for the analysis of heart rate variability in the time and frequency domains. Braz. J. Med. Biol. 41, 854–859 (2008).
Barroso, W. K. S. et al. Diretrizes Brasileiras de Hipertensão Arterial—2020. Arq. Bras. Cardiol. 116, 516–658 (2021).
Souza, R. B. D. & Pereira, C. A. Diretrizes para testes de função pulmonar. J. Pneumol. 28, 1–238 (2002).
Laveneziana, P. et al. ERS statement on respiratory muscle testing at rest and during exercise. Eur. Respir. J. https://doi.org/10.1183/13993003.01214 (2019).
Alberto, C., Pereira, C., Sato, T. & Rodrigues, S. C. New reference values for forced spirometry in white adults in Brazil. J. Bras. Pneumol. 33, 397–406 (2007).
Catai, A. M. et al. Heart rate variability: Are you using it properly? Standardization checklist of procedures. Braz. J. Phys. Ther. 24, 91–102 (2020).
Shaffer, F. & Ginsberg, J. P. An overview of heart rate variability metrics and norms. Front. Public Health https://doi.org/10.3389/fpubh.2017.00258 (2017).
Tarvainen, M. P., Niskanen, J. P., Lipponen, J. A., Ranta-aho, P. O. & Karjalainen, P. A. Kubios HRV—Heart rate variability analysis software. Comput. Methods Progr. Biomed. 113, 210–220 (2014).
Parr, J. J., Yarrow, J. F., Garbo, C. M. & Borsa, P. A. Symptomatic and functional responses to concentric–eccentric isokinetic versus eccentric-only isotonic exercise. J. Athl. Train. 44, 462–468 (2009).
American Thoracic Society. American thoracic society ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 166, 111–117 (2002).
Mancini, M. C. Diretrizes Brasileiras de Obesidade 2016 (ABESO, 2016).
Valdez, R. & Valdez, D. R. A simple model-based index adiposity. J. Clin. Epidemiol. 44, 955–956 (1991).
Guerrero-Romero, F. & Rodríguez-Morán, M. Abdominal volume index. An anthropometry-based index for estimation of obesity is strongly related to impaired glucose tolerance and type 2 diabetes mellitus. Arch. Med. Res. 34, 428–432 (2003).
Bergman, R. N. et al. A better index of body adiposity. Obesity 19, 1083–1089 (2011).
Lukaski, H. C., Bolonchuk, W. W., Hall, C. B., Siders, W. A. & Widation, W. A. S. Validation of tetrapolar bioelectrical impedance method to assess human body composition. J. Appl. Physiol. 60, 1327–1332 (1986).
Heyward, V. ASEP methods recomendation: Body composition assessment. J. Exerc. Physiol. 4, 1–12 (2001).
Hoaglin, D. C. & Iglewicz, B. Fine-tuning some resistant rules for outlier labeling. J. Am. Stat. Assoc. 82, 1147–1149 (1987).
Acknowledgements
We thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) and the São Paulo Research Foundation (FAPESP) for supporting this work and all personnel of the outpatient cardiac rehabilitation program carried out at Center for Physical Therapy and Rehabilitation Studies and Treatment (CEAFiR), Presidente Prudente, Brazil for allowing and welcoming our research team in their facility.
Funding
This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, Finance code 001, Fundação de Amparo à Pesquisa do Estado de São Paulo, 2020/16551-0.
Author information
Authors and Affiliations
Contributions
MJLL: conceptualization, methodology, formal analysis, writing—original draft, and writing—review & editing. DGP: investigation, and writing—review & editing. JMS: investigation, and writing—review & editing. FR: investigation, data curation, and writing—review & editing. HBV: investigation, data curation, and writing—review & editing. LCMV: conceptualization, methodology, formal analysis, writing—review & editing, supervision, and funding acquisition.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Laurino, M.J.L., Pinheiro, D.G., da Silva, J.M. et al. Predicting the occurrence of minor adverse events in cardiac rehabilitation using physical variables. Sci Rep 14, 17179 (2024). https://doi.org/10.1038/s41598-024-68223-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-68223-y
- Springer Nature Limited