
Abstract
Musculoskeletal disorders (MDs) represent a global health issue, which can lead to disability. Physical activity (PA) reduces pain and increases physical function among patients with MDs. To promote behavioural changes, it seems important to focus on modifiable factors, such as motivation. Thus, this review aims to assess effects of interventions targeting PA on motivation towards PA. Searches used terms referring to “physical activity”, “motivation” and “chronic musculoskeletal disorders” on the databases PubMed, PsychINFO, MEDLINE, EMBASE, PEDro and Web of Science. All types of intervention—including but not limited to RCTs—were eligible for inclusion. Risk of bias was assessed with the Quality Assessment Tool for Studies with Diverse Designs (QATSDD). Among 6 489 abstracts identified, there were 387 eligible studies and 19 were included, reporting in total 34 effect sizes. The meta-analysis concerned 1 869 patients and indicated a small effect of interventions on change in motivation towards PA (d = 0.34; 95% CI [0.15; 0.54]; p < .01; k = 33). Behavioural interventions positively impact PA motivation in patients with MDs. In the literature, most studies focused on intervention’s effect on fear of movement. Future research should assess other explicit motivational constructs, as well as implicit processes.
Similar content being viewed by others


Introduction
Nowadays, people live longer1 but become more prone to non-communicable diseases, including musculoskeletal conditions2. Musculoskeletal disorders (MDs)—osteoarthritis, low back or neck pain—represent a widespread health issue, which can lead to temporary or permanent disability at work, causing high costs for global economy3. In 2021, MDs were the leading cause for years lived with disability worldwide, with a prevalence of 1,690 million3,4, women being more affected than men.
Physical activity (PA) is unequivocally recommended in the management of MDs5,6,7,8, due to its effects in reducing pain, improving physical function and quality of life9,10,11. However, a large majority of patients affected by MDs are not sufficiently active in regard to WHO’s recommendations (i.e., 64%-73%)12,13. Therefore, it seems crucial to implement efficient interventions to promote PA behaviour in this population. Several systematic reviews and meta-analyses examined the effect of interventions aiming at increasing PA level in MDs patients14,15,16,17,18, revealing mixed results. Some articles do not report significant increase17,18, while others do 14,16. Mansi et al.’s systematic review16 showed that interventions using pedometers appear to be effective. Davergne et al.13 found similar results: the use of wearable activity trackers (including pedometers) led to an increase in daily steps (d = 0.83), and in the time spent in moderate-to-vigorous PA (d = 0.41) at the end of the intervention. However, these results are based on a small number of studies—7 and 3, respectively—and there was no evidence of a maintained change in PA at follow-up 2 to 4 months after the end of the interventions. This last result is in line with two previous meta-analyses in which no significant increase in objectively measured PA was reported in the medium and long term (i.e., more than 3 and 6 or twelve months later)16,17,18.
To take up this challenge, it is essential to focus on behaviour determinants19. Among factors that may account for this absence of long term effect, patient’s motivation is considered as a key construct to understand the process of behaviour change20. Motivation is defined as “a driving force or forces responsible for the initiation, persistence, direction, and vigour of goal-directed behaviour”21. In health psychology, socio-cognitive models, which consider the rationality of individuals as the root of behaviours adoption, were predominantly used as theoretical basis in previous studies. With this regard, some authors pointed out the presence of a small set of core concepts that enable understanding the adoption of a behaviour or its absence19. Those concepts include (i) beliefs associated with positive / negative behaviour’s effects, (ii) beliefs in one’s ability to achieve it; and (iii) individual’s intention to achieve it. In patients with MDs, there was a major focus on negative outcomes mentally associated to PA behaviour; this particular type of belief was frequently studied through fear of movement or kinesiophobia22. Kinesiophobia is defined as an excessive, irrational and debilitating fear of physical movement and activity resulting from a feeling of vulnerability to a painful injury or reinjury23. Fear of movement is a specific fear of movement and physical activity that is (wrongfully) assumed to cause reinjury24. Although the definitions are distinct, those two concepts are very similar25 and are sometimes used interchangeably. Finally, PA is perceived as a dangerous behaviour by individuals.
To complement the dominant, socio-cognitive approach, dual models have been proposed in health psychology26. The authors of such models state that two main types of processes govern our behaviours: explicit and implicit. This dichotomy is based on the idea that humans act according not only or always to their reason (explicit), but also to their drives (implicit)27. Over the past decade, there has been a significant increase in the number of studies questioning health-related behaviour adoption through this lens. Regarding PA, most previous studies derived from dual models focused on implicit attitudes (i.e., automatic evaluations of a behaviour, as favourable or unfavourable). Recently, Chevance et al.28 conducted a meta-analysis of 26 studies on this concept, and concluded to the existence of a significant relationship between individual’s implicit attitudes towards PA and their level of PA. Such results were in particular observed among people with chronic conditions (i.e., obese patients29; chronic respiratory disease patients30), but at the time no study was reported among patients with chronic MDs. In sum, past literature suggests that to improve MDs patients’ level of PA, interventions should target PA motivation both at the explicit and implicit level.
Additionally, there were previous attempts to examine the extent to which behavioural interventions actually impact PA motivation is subject to potential moderator effects. Firstly, Knittle and colleagues20 observed that all theoretical constructs may not equally evolve following such an intervention. Larger effects of the intervention were observed in the studies of autonomous motivation (i.e., when people engage in a behaviour for pleasure or fun, when it is congruent with an individual’s sense of self or when it is personally important to the individual) compared to intention. Past literature also examined which characteristics of intervention were associated to PA intervention efficacy. In particular, several features of intervention are associated with more important effects on PA motivation. Interventions targeting groups were more successful than those targeting individuals31. Knittle et al.20 found similar results and also observed that interventions incorporating face-to-face20 components resulted in larger effects compared to those without face-to-face components. However, those meta-analyses did not specifically focus on population concerned by chronic disease, and none concerned MDs patients.
The aims of this systematic review and meta-analysis are thus to (i) assess the effects of intervention targeting PA on motivation towards PA among patients with chronic MDs and (ii) identify potential theoretical and methodological moderators of intervention efficacy.
Methods
Guidelines and registration
The protocol of the current systematic review and meta-analysis was registered at the PROSPERO international database (Number: CRD42021234601). Procedures followed the principles of Preferred Reporting Items for Systematic Reviews and Meta-analysis32. All relevant study material (e.g., pre-registration protocol, pre-print, data and R code) and Supplementary Materials are available on the Open Science Framework (see https://osf.io/tybwz/).
Search strategy
The following electronic databases were used: PubMed, PsycINFO, MEDLINE, EMBASE, PEDro, Web of Science from inception to March 2021. Search terms were referring to “physical activity”, “motivation”, and “chronic musculoskeletal disorders”, using the AND modifier. The keywords used in different databases are listed in Supplementary Material 1. There was no restriction on publication date. Studies published in English, Spanish, French or Italian were considered for inclusion.
Inclusion and exclusion criteria
Studies meeting the following PICOS criteria were considered eligible for inclusion: (1) Population: adults (≥ 18 years) with chronic MDs (≥ 3 months); (2) Intervention: targeting explicitly a change in PA motivation and/or in PA behaviour; (3) Comparison intervention: all conditions, except identical interventions concerning PA and the absence of a control group; (4) Outcomes: a motivational construct assessed pre—and post—intervention; (S) Study design: all experimental design.
For each step of the studies selection, four reviewers established inter-rater reliability, using percentage agreement, working in dyads based on 5% of the articles. If a researcher was not sure about an article inclusion, reviewers discussed until a consensus decision on inclusion/exclusion was reached. They independently screened the titles and abstracts of studies retrieved and then the full-text retained. For studies fulfilling all inclusion criteria but presenting data unsuitable for meta-analysis, corresponding authors were contacted up two times by email to obtain appropriate data.
Coding and data extraction: The same reviewers extracted data. Once the final studies’ inclusion was made, inter-rater reliability in data coding was assessed with a phase in dyads based on 10% of the articles. Then, the articles were divided among reviewers. Data were extracted regarding study population and design (number of participants, sex ratio, mean age, mean BMI, type of musculoskeletal disorder, level of pain), outcomes (motivation variables), and intervention characteristics: duration in weeks, modalities (face-to-face, digital, mix). Data are provided in Supplementary Material 2.
Quality was assessed with the Quality Assessment Tool for Studies with Diverse Designs (QATSDD)33. Scores on the QATSDD can range from 0 to 42. This tool was not proposed to determine which studies should or should not be excluded from a review, but only to get a sense of the variability of methodological quality within the set of studies included. According to Sirriyeh et al.33, any cut-off points to indicate high or low quality would be arbitrary. From its publication to December 2019, it has been used in more than 80 reviews34.
For this step, inter-rater reliability in quality assessment was calculated for a phase in which dyads evaluated 10% of the articles. In the event of ambiguous cases raised by a researcher, consensus was sought through discussion in the team.
Statistical analyses
Based on the mean, standard deviation, and sample size at both points of measurement in each group, Hedges’ g was used as the primary measure of cumulative effect size and 95% CIs and two-sided p-values were calculated. The magnitude of effect sizes was interpreted as small > 0.2, medium > 0.5 or large > 0.835.
A method of Robust Variance Estimation (RVE) was used to account for dependencies of having multiple effect sizes come from each study. A correction for meta-analysis with fewer than 40 studies included were applied36. RVE with small sample correction was used as the main meta-analysis.
Sensitivity analyses
A set of sensitivity analyses were carried out. For outliers’ detection, we performed Baujat and funnel plots. There are two other options recommended to deal with dependencies in effect sizes: aggregating effect sizes within-study and performing a multi-level meta-analysis37. These options (i.e., aggregation and multi-level analyses) were performed as sensitivity analyses. Then, we compared these models to verify the robustness of ours estimated effect sizes.
Heterogeneity was quantified using the I2 indicator.
Moderator analyses
We conducted moderator analyses according to Assink and Wibbelink38. Significant moderator effects were discussed when at least 4 effect sizes were available for all modalities.
All analyses were carried out in R 4.0.339, the code used for this study is available in Supplementary Material 3.
We used the robumeta package40 for the robust variance estimation meta-analysis, the metafor package41 for study aggregation and multi-level meta-analyses.
Results
Eligible studies and assessment tools
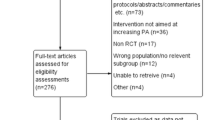
The PRISMA flowchart summarizing the process of study selection and the reasons for study exclusion is shown in Fig. 1. The other items on the PRISMA checklist are presented in Supplementary Material 4. Of the 432 full-text articles assessed for eligibility, 19 were included with 34 effect sizes. In the various stages of selection, we achieved very good interrater reliability, with kappa values ranging from 0.67 to 1.

Flow diagram of incluion process.
Descriptive sample characteristics
The characteristics of studies are shown in Supplementary Material 2. Overall, this study involved 1,869 patients with a mean age of 56.1 (± 9.3) years. They had been experiencing pain for an average of 97.6 (± 58.8) months. Their mean pain was 53.3 (± 14.8) on a visual analog scale of 100. They had a mean BMI of 29.1 (± 3.6). All interventions included both women and men. Eight studies (42%; k = 9) focused on patients with chronic low back pain, seven studies (37%; k = 15) were conducted on patients with arthritis, and only one study (5%) included patients with neck pain (k = 2), ankylosing spondylitis (k = 2), rheumatoid arthritis (k = 2) and axial spondylarthritis (k = 4), respectively.
Descriptive intervention characteristics
On average, the interventions lasted 12.7 weeks. Only three interventions out of 19 (16%) were explicitly based on theoretical models of motivation. Ten interventions (53%) were individual, six (32%) collective and three (16%) mixed. Of the 19 interventions, 14 (78%) were with a face-to-face interventionist only, one (6%) was only phone sessions, and three (17%) were mixed, through smartphone (two, 11%) or phone sessions (one, 6%). Fourteen interventions (74%) out of 19 provided PA, among which 13 (68%) included supervised practice.
Seven studies (37%) combined PA with educational sessions, two (11%) with a booklet, two with both educational sessions and a booklet (11%), and two provided PA practise only (11%). Of the five interventions (26%) without PA practice, four (21%) provided educational sessions and booklet, and one (5%) booklet only.
Regarding control groups, six studies (32%) had no intervention, seven (37%) included PA, four studies (21%) offered booklet but no PA practise, one study (5%) proposed both PA with educational sessions and a booklet, and one study proposed only educational sessions (5%).
Motivational outcomes
The 19 studies yielded effect sizes on 34 motivation scores. Out of those 34 outcomes, fear of movement or kinesiophobia were assessed 13 times (38%); exercise self-efficacy and barriers five times each (15%); PA benefits, four times (12%); and six variables were assessed only once: attitudes, autonomous motivation, barriers, controlled motivation, facilitators, and perceived impact on disease. The scales used to assess each motivational outcomes are presented in Supplementary Material 5.
Risk of bias
The set of included studies had a QATSDD mean score of 31 (± 3.0) on 42. This appears similar to previous investigations using the same tool—in their systematic review of PA intervention among disabled people, Jaarsma and Smith (2018)42 reported an average score of 27. In our meta-analysis, studies’ quality was globally respected for the following items: the presentation of explicit framework, stating their aims clearly in the report, and fitting the research question, and analysis method used. However, studies usually scored poorly on items related to sample size consideration, information on data collection, and involving users or stakeholders in the study design.
Full information on the risk of bias of each study is available in Supplementary Material 6.
Meta-analysis and sensitivity analyses
An outlier was identified and removed43. The RVE corrected for small sample size indicated a small effect of interventions on post-interventions motivation (d = 0.34; 95% CI [0.15; 0.54]; p < 0.01; N = 19; k = 33; see Fig. 2). Between-study heterogeneity was moderate (I2 = 47%).

Forest plot of RVE corrected for small sample size.
The estimate was very comparable to the one observed with other strategies (study aggregation: d = 0.31; 95% CI [0.15; 0.48]; p < 0.01; N = 19; k = 33; multi-level meta-analysis: d = 0.35; 95% CI [0.17; 0.54]; p < 0.01; N = 19; k = 33; see Supplementary Material 7).
Moderator analyses
Various moderator analyses were computed, so as to examine whether motivational constructs (fear vs self-efficacy vs other), modality of intervention (individual vs collective vs mixed), mode of delivery (face to face only vs with smartphone support vs with phone sessions), type of pathology (arthritis vs chronic low back pain vs other), type of intervention (PA only vs PA and additional features), duration of intervention, and study quality, significantly impacted intervention efficacy. There was not significant result. All analyses carried out are available in Supplementary Material 3.
Discussion
This meta-analysis assessed the effects of intervention targeting PA on motivation towards PA among patients with chronic MDs. This work included 19 studies, representing 34 effect sizes and involving 1 869 patients. The studies had a mean QATSDD score of 31 out of 42. In general, studies adequately presented an explicit framework, clearly stated their aims in the report, and aligned the analysis method used and the research question. Our work is the first to examine this research question focusing on this specific population. In view of MDs’ impact on individuals and societies, it is essential to address the issue of regular PA in these populations. The analyses showed a small effect of interventions on motivation.
Overall effect size
The main meta-analysis (i.e., Robust Variance Estimation corrected for small sample sizes) indicated that compared to those in control groups, participants in intervention groups presented a significantly larger change in PA motivation (d = 0.34). There was a low to moderate level of heterogeneity (I2 = 47%)44.
We consider this result as consistent because the two other ways of addressing dependent effect sizes in a meta-analysis (i.e., study aggregation and multi-level meta-analysis) lead to comparable results (respectively, d = 0.31 and d = 0.35).
Our work is in line with previous meta-analyses investigating the impact of interventions aiming at increasing PA levels on motivation towards this behaviour, in which effect sizes ranging from small20,45 to moderate46,47 were reported. However, those results were observed in individuals from the general population20,46, obese individuals47, or elderly individuals45.
Our secondary aim was to discern potential theoretical and methodological moderators that might impact intervention efficacy.
Motivational constructs as moderators
Motivation is a theoretical concept encompassing multiple constructs. We did not find a moderating effect of these constructs. In this work, over a third (13/34) of the effect sizes concerned fear of movement or kinesiophobia. Those variables incorporate beliefs regarding the behaviour’s effects and are specific to patients witch chronic MDs. Self-efficacy and barriers to PA practice were also frequently studied (k = 5 for each); those variables refer to individuals’ perceived ability to engage in PA behaviour. Regarding the effect of interventions aimed at increasing PA on self-efficacy, our results are consistent with previous meta-analyses reporting small effect sizes (d = 0.23 to 0.37)45,47.
Features of interventions as moderators
This study explored several moderators of interventions effects but there were no significant results. Interventions therefore appear to be just as effective in modifying the various motivational constructs, whether they are delivered face-to-face or remotely, in groups or individually, and regardless of the duration of the intervention. These results do not align with the literature. Indeed, previous meta-analyses20,31 observed a favourable effect of group intervention on individuals motivation.
However, these previous works involved a much larger number of interventions (89 and 41, respectively) and predominantly included individuals without chronic pathology. We can hypothesize that the lack of motivation toward PA48 in these patients may make them more responsive to an intervention, regardless of how it is delivered.
Strengths and limitations of the current study
The present study adhered to the protocol previously deposited in the PROSPERO international database (Number: CRD42021234601). Additionally, employed robust and reproducible search, selection and coding procedures, all of which have been made accessible (see https://osf.io/tybwz/). We posit that enhancing motivation for PA among these patients is important; indeed, qualitative studies report that lack of motivation is one of the most commonly reported barriers to physical activity48,49. This work thus provides a synthesis of existing interventions found to be effective in addressing this lack of motivation. Our systematic review showed that most studies in the literature focused on fear of movement and exercise self-efficacy. Specifically, examining fear of movement, assessed using the original Tampa Scale for Kinesiophobia Questionnaire or the PA subscale of the Fear Avoidance Beliefs Questionnaire, we observed that 5 out of 10 studies (50%) reported a difference greater than the minimal clinically important differences for this population (i.e., respectively 4.5 and 4 points)50,51. This is encouraging for clinicians, but it should not discount the interindividual differences that may exist.
Our study has also some limitations. Compared to similar works examining the effect of interventions aimed at increasing PA levels on motivation, we found a relatively limited number of available studies. This smaller sample size may have restricted our ability to detect significant moderators. Furthermore, patients involved in our meta-analyses have different pathologies, with pain experienced for highly heterogeneous periods of time (i.e., ranging from a minimum of 3 months to over ten years).
Moreover, we opted to use a risk of bias assessment tool that does not provide thresholds33. Nonetheless, we tested the moderating effect of study quality scores and found no significant results.
Perspectives
Regarding motivational constructs, only few explicit processes have been studied in MDs patients to date. Fear of movement and self-efficacy are linked to the initiation of intention formation. Intention, while essential, often falls short as a sole determinant when it comes to actualizing behaviour for many individuals52. It is therefore necessary to adopt (i) regulation processes, pertain to the factors that support achieving goals. These processes involve the execution of behaviour in alignment with one's intentions while adjusting them to suit the specific context; and (ii) reflexive or implicit processes, which represent less deliberative elements that impact behavioural actions, primarily via learned associations activated by specific circumstances and stimuli.
To the best of our knowledge, no study has investigated implicit processes in this population. In patients with chronic low back pain, Caneiro et al.53 showed that self-report measures do not always reflect implicit associations between particular movements and threat. Among chronic respiratory patients, implicit attitudes were more favourable to PA at the end of a pulmonary rehabilitation programme. Moreover, they were associated 6 months later with PA30. This stresses the importance of considering such PA predictors in patients with MDs. With regard to interventions, according to Rebar et al.54, PA interventions could potentially enhance their effectiveness by integrating strategies that specifically target non-conscious regulatory, or implicit, processes. Previous research showed that interventions such as evaluative conditioning55 or mental imagery56 may modify implicit processes.
However, patient-reported barriers extend beyond mere motivation. Some of these factors include pain, time restrictions, false recommendations from healthcare professionals, or lack of social support48,49. The authors of these works highlight the diversity of responses from one individual to another. It is therefore important to propose interventions aimed specifically at targeting the needs and expectations of each patient.
Therefore, this systematic review with meta-analysis enabled us to identify some perspectives for interventions aimed at increasing PA in patients with chronic MDs.
For about twenty years, studies aimed at increasing PA in individuals have sought to describe their interventions more precisely. With this goal in mind, Michie et al.57 have proposed a taxonomy of Behaviour Change Techniques (BCTs). BCTs are defined “as an observable, replicable, and irreducible component of an intervention designed to alter or redirect causal processes that regulate behaviour”57. A meta-analysis has identified several BCTs more effective on motivation towards PA (e.g., behavioural goal setting, self-monitoring of behaviour, behavioural practice, or rehearsal)20. Considering the literature specific to this population, we did not find adequate data to test these different BCTs as moderating variables. In patients with chronic MDs population, these BCTs should therefore be included in interventions and well described.
To this end, the Intervention Mapping framework58 appears to be relevant59. This approach, based on theory and evidence, allows interventionists to systematically plan, develop, implement, and evaluate health promotion programs (e.g., increasing levels of PA). It provides a structured 6-step approach to integrating evidence-based techniques and behaviour change theories.
Beyond the components of the interventions, the methodological design employed would benefit from evolving. Indeed, RCTs were well recognized as the “gold standard” for evaluating treatment or intervention outcomes60. However, it seems necessary to adopt another experimental paradigm to understand changes in complex behaviours, including PA61. Firstly, these designs, as in the studies included in this work, present two measurement times. Research that includes multiple evaluations has emphasized how health behaviours are subject to change over time and influenced by various factors, as demonstrated across different temporal contexts62,63,64. As health behaviours are complex, adaptative and continuous tuning interventions should be more effective than “static” interventions and should therefore be adopted. In addition to these two proposals, Chevance et al.61 have also called for a shift from group-only to group- and individual-level statistical inference.
Conclusion
PA is the cornerstone of disease management among patients with chronic MDs. Nevertheless, they often present an insufficient PA level. Therefore, it is essential to set up dedicated interventions. To be efficient, these interventions should act on modifiable factors of PA. In this review, we investigated the efficacy of behavioural interventions targeting PA on PA motivation change in patients with MDs. PA interventions have a small effect on motivation at the end of the interventions. Until now, researchers mainly focused on negative beliefs associated with PA behaviour, especially fear of movement or kinesiophobia. Future studies should (i) have high-resolution behavioural assessments, (ii) precisely describe the content of related to BCT used within the interventions, and (iii) investigate implicit processes.
Data availability
The datasets used and/or analysed during the current study are available on the Open Science Framework (see https://osf.io/tybwz/).
References
Mathers, C. D., Stevens, G. A., Boerma, T., White, R. A. & Tobias, M. I. Causes of international increases in older age life expectancy. The Lancet 385, 540–548 (2015).
Hoy, D. G. et al. The global burden of musculoskeletal conditions for 2010: an overview of methods. Ann. Rheum. Dis. 73, 982–989 (2014).
Vos, T. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet 390, 1211–1259 (2017).
Ferrari, A. J. et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet 403, 2133–2161 (2024).
Hochberg, M. C. et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 64, 465–474 (2012).
Kolasinski, S. L. et al. 2019 American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 72, 220–233 (2020).
Metsios, G. S., Stavropoulos-Kalinoglou, A. & Kitas, G. D. The role of exercise in the management of rheumatoid arthritis. Expert Rev. Clin. Immunol. 11, 1121–1130 (2015).
Qaseem, A., Wilt, T. J., McLean, R. M., Forciea, M. A., & for the Clinical Guidelines Committee of the American College of Physicians. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 166, 514 (2017).
Bennell, K. L. & Hinman, R. S. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J. Sci. Med. Sport 14, 4–9 (2011).
Institut national de la santé et de la recherche médicale (Inserm). Activités physiques : Prévention et traitement des maladies chroniques - Synthèse et recommandations. (EDP Sciences, 2019).
Vanti, C. et al. The effectiveness of walking versus exercise on pain and function in chronic low back pain: A systematic review and meta-analysis of randomized trials. Disabil. Rehabil. 41, 622–632 (2019).
O’Dwyer, T., Rafferty, T., O’Shea, F., Gissane, C. & Wilson, F. Physical activity guidelines: is the message getting through to adults with rheumatic conditions?. Rheumatology 53, 1812–1817 (2014).
Kalın, A. S. & Aytur, Y. K. Physical activity levels of individuals with chronic musculoskeletal disorders: Their relationship with barriers and facilitators. Musculoskeletal Care 21, 797–805 (2023).
Davergne, T., Pallot, A., Dechartres, A., Fautrel, B. & Gossec, L. Use of wearable activity trackers to improve physical activity behavior in patients with rheumatic and musculoskeletal diseases: A systematic review and meta-analysis. Arthritis Care Res. 71, 758–767 (2019).
Eisele, A., Schagg, D., Krämer, L. V., Bengel, J. & Göhner, W. Behaviour change techniques applied in interventions to enhance physical activity adherence in patients with chronic musculoskeletal conditions: A systematic review and meta-analysis. Patient Educ. Couns. 102, 25–36 (2019).
Mansi, S., Milosavljevic, S., Baxter, G. D., Tumilty, S. & Hendrick, P. A systematic review of studies using pedometers as an intervention for musculoskeletal diseases. BMC Musculoskelet. Disord. 15, 231 (2014).
Marley, J. et al. The effectiveness of interventions aimed at increasing physical activity in adults with persistent musculoskeletal pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 18, 482 (2017).
Oliveira, C. B. et al. Physical activity interventions for increasing objectively measured physical activity levels in patients with chronic musculoskeletal pain: A systematic review: review of PA interventions in chronic musculoskeletal pain. Arthritis Care Res. 68, 1832–1842 (2016).
Sheeran, P., Klein, W. M. P. & Rothman, A. J. Health behavior change: moving from observation to intervention. Annu. Rev. Psychol. 68, 573–600 (2017).
Knittle, K. et al. How can interventions increase motivation for physical activity? A systematic review and meta-analysis. Health Psychol. Rev. 12, 211–230 (2018).
Colman, A. M. A Dictionary of Psychology (Oxford University Press, Oxford, 2015).
Luque-Suarez, A., Martinez-Calderon, J. & Falla, D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: A systematic review. Br. J. Sports Med. 53, 554–559 (2019).
Kori, S., Miller, R. & Todd, D. Kinesiophobia: A new view of chronic pain behavior. Pain Manag. 3, 35–43 (1990).
Vlaeyen, J. W. S., KoleSnijders, A. M. J., Rotteveel, A. M., Ruesink, R. & Heuts, P. The role of fear of movement (re)injury in pain disability. J. Occup. Rehabil. 5, 235–252 (1995).
Lundberg, M., Grimby-Ekman, A., Verbunt, J. & Simmonds, M. J. Pain-related fear: A critical review of the related measures. Pain Res. Treat. 2011, 1–26 (2011).
Hagger, M. S. Non-conscious processes and dual-process theories in health psychology. Health Psychol. Rev. 10, 375–380 (2016).
Deutsch, R., Gawronski, B. & Hofmann, W. Reflective and Impulsive Determinants of Human Behavior. (Routledge, London, 2016). https://doi.org/10.4324/9781315523095.
Chevance, G., Bernard, P., Chamberland, P. E. & Rebar, A. The association between implicit attitudes toward physical activity and physical activity behaviour: A systematic review and correlational meta-analysis. Health Psychol. Rev. 13, 248–276 (2019).
Chevance, G. et al. Do implicit attitudes toward physical activity and sedentary behavior prospectively predict objective physical activity among persons with obesity?. J. Behav. Med. 41, 31–42 (2018).
Chevance, G., Héraud, N., Varray, A. & Boiché, J. Change in explicit and implicit motivation toward physical activity and sedentary behavior in pulmonary rehabilitation and associations with postrehabilitation behaviors. Rehabil. Psychol. 62, 119–129 (2017).
Steinmetz, H., Knappstein, M., Ajzen, I., Schmidt, P. & Kabst, R. How effective are behavior change interventions based on the theory of planned behavior? A three-level meta-analysis. Z. Für Psychol. 224, 216–233 (2016).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLOS Med. 6, e1000100 (2009).
Sirriyeh, R., Lawton, R., Gardner, P. & Armitage, G. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pract. 18, 746–752 (2012).
Harrison, R., Jones, B., Gardner, P. & Lawton, R. Quality assessment with diverse studies (QuADS): An appraisal tool for methodological and reporting quality in systematic reviews of mixed- or multi-method studies. BMC Health Serv. Res. 21, 144 (2021).
Cohen, A. J. Statistical Power Analysis for the Behavioural Sciences (Lawrence Erlbaum, 1988).
Tipton, E. Small sample adjustments for robust variance estimation with meta-regression. Psychol. Methods 20, 375–393 (2015).
Moeyaert, M. et al. Methods for dealing with multiple outcomes in meta-analysis: A comparison between averaging effect sizes, robust variance estimation and multilevel meta-analysis. Int. J. Soc. Res. Methodol. 20, 559–572 (2016).
Assink, M. & Wibbelink, C. J. M. Fitting three-level meta-analytic models in R: A step-by-step tutorial. Quant. Methods Psychol. 12, 154–174 (2016).
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing (2020).
Fisher, Z., Tipton, E. & Zhipeng, H. robumeta: Robust Variance Meta-Regression. (2023).
Viechtbauer, W. Meta-Analysis Package for R. (2023).
Jaarsma, E. A. & Smith, B. Promoting physical activity for disabled people who are ready to become physically active: A systematic review. Psychol. Sport Exerc. 37, 205–223 (2018).
Baujat, B., Mahé, C., Pignon, J.-P. & Hill, C. A graphical method for exploring heterogeneity in meta-analyses: Application to a meta-analysis of 65 trials. Stat. Med. 21, 2641–2652 (2002).
Higgins, J. P. T., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560 (2003).
French, D. P., Olander, E. K., Chisholm, A. & Mc Sharry, J. Which behaviour change techniques are most effective at increasing older adults’ self-efficacy and physical activity behaviour? A systematic review. Ann. Behav. Med. 48, 225–234 (2014).
McDermott, M. S., Oliver, M., Iverson, D. & Sharma, R. Effective techniques for changing physical activity and healthy eating intentions and behaviour: A systematic review and meta-analysis. Br. J. Health Psychol. 21, 827–841 (2016).
Olander, E. K. et al. What are the most effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 10, 29 (2013).
Boutevillain, L., Dupeyron, A., Rouch, C., Richard, E. & Coudeyre, E. Facilitators and barriers to physical activity in people with chronic low back pain: A qualitative study. PLOS ONE 12, e0179826 (2017).
McPhail, S. M., Schippers, M., Marshall, A. L., Waite, M. & Kuipers, P. Perceived barriers and facilitators to increasing physical activity among people with musculoskeletal disorders: A qualitative investigation to inform intervention development. Clin. Interv. Aging 9, 2113–2122 (2014).
Pulles, A. N. T. D., Köke, A. J. A., Strackke, R. P. & Smeets, R. J. E. M. The responsiveness and interpretability of psychosocial patient-reported outcome measures in chronic musculoskeletal pain rehabilitation. Eur. J. Pain 24, 134–144 (2020).
Monticone, M. et al. Reliability, responsiveness and minimal clinically important difference of the two Fear Avoidance and Beliefs Questionnaire scales in Italian subjects with chronic low back pain undergoing multidisciplinary rehabilitation. Eur. J. Phys. Rehabil. Med. 56, (2020).
Rhodes, R. E. & Yao, C. A. Models accounting for intention-behavior discordance in the physical activity domain: A user’s guide, content overview, and review of current evidence. Int. J. Behav. Nutr. Phys. Act. 12, (2015).
Caneiro, J. P., O’Sullivan, P., Smith, A., Moseley, G. L. & Lipp, O. V. Implicit evaluations and physiological threat responses in people with persistent low back pain and fear of bending. Scand. J. Pain 17, 355–366 (2017).
Rebar, A. L. et al. A systematic review of the effects of non-conscious regulatory processes in physical activity. Health Psychol. Rev. 10, 395–407 (2016).
Antoniewicz, F. & Brand, R. Learning to like exercising: Evaluative conditioning changes automatic evaluations of exercising and influences subsequent exercising behavior. J. Sport Exerc. Psychol. 38, 138–148 (2016).
Markland, D., Hall, C. R., Duncan, L. R. & Simatovic, J. The effects of an imagery intervention on implicit and explicit exercise attitudes. Psychol. Sport Exerc. 17, 24–31 (2015).
Michie, S. et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 46, 81–95 (2013).
Bartholomew, L. K., Parcel, G. S. & Kok, G. Intervention mapping: A process for developing theory and evidence-based health education programs. Health Educ. Behav. 25, 545–563 (1998).
Latrille, C. et al. An individualized mobile health intervention to promote physical activity in adults with obstructive sleep apnea: An intervention mapping approach. Digit. Health 9, 20552076221150744 (2023).
Saturni, S. et al. Randomized controlled trials and real life studies. Approaches and methodologies: a clinical point of view. Pulm. Pharmacol. Ther. 27, 129–138 (2014).
Chevance, G., Perski, O. & Hekler, E. B. Innovative methods for observing and changing complex health behaviors: Four propositions. Transl. Behav. Med. 11, 676–685 (2021).
Bernard, P. et al. Moderators of theory-based interventions to promote physical activity in 77 randomized controlled trials. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 44, 227–235 (2017).
Voogt, C. V. et al. Using ecological momentary assessment in testing the effectiveness of an alcohol intervention: a two-arm parallel group randomized controlled trial. PloS One 8, e78436 (2013).
Newman, M. A. et al. Monthly variation in physical activity levels in postmenopausal women. Med. Sci. Sports Exerc. 41, 322–327 (2009).
Funding
The study was funded by the Nîmes University Hospital and the University of Montpellier.
Author information
Authors and Affiliations
Contributions
All the authors contributed to the drafting of the current systematic review and meta-analysis’ protocol. M.H., J.B., C.L. and M.B. selected articles and extracted data. M.H. and G.C. conducted the statistical analysis. M.H., J.B. and A.D. contributed to the interpretation of the results. M.H. performed the quality assessment appraisal and wrote the main manuscript text. All authors provided critical feedback on drafts and approved the final manuscript. J.B., A.D. and A.L.C. required study’s funds.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Haas, M., Boiché, J., Chevance, G. et al. Motivation toward physical activity in patients with chronic musculoskeletal disorders: a meta-analysis of the efficacy of behavioural interventions. Sci Rep 14, 18740 (2024). https://doi.org/10.1038/s41598-024-67948-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-67948-0
- Springer Nature Limited