
Abstract
The effect of practice schedule on retention and transfer has been studied since the first publication on contextual interference (CI) in 1966. However, strongly advocated by scientists and practitioners, the CI effect also aroused some doubts. Therefore, our objective was to review the existing literature on CI and to determine how it affects retention in motor learning. We found 1255 articles in the following databases: Scopus, EBSCO, Web of Science, PsycINFO, ScienceDirect, supplemented by the Google Scholar search engine. We screened full texts of 294 studies, of which 54 were included in the meta-analysis. In the meta-analyses, two different models were applied, i.e., a three-level mixed model and random-effects model with averaged effect sizes from single studies. According to both analyses, high CI has a medium beneficial effect on the whole population. These effects were statistically significant. We found that the random practice schedule in laboratory settings effectively improved motor skills retention. On the contrary, in the applied setting, the beneficial effect of random practice on the retention was almost negligible. The random schedule was more beneficial for retention in older adults (large effect size) and in adults (medium effect size). In young participants, the pooled effect size was negligible and statically insignificant.
Similar content being viewed by others
Introduction
One of the variable practice phenomena is that more variability initially hinders learning but, in many cases, subsequently benefits it1. Training schedule is one of the sources of variability1. One of the effects of variability caused by the training schedule is called the contextual interference (CI) effect1.
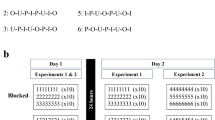
The CI effect has been exhaustively studied since the original Battig’s publication in 19662. Battig reported that immediate performance, retention, and transfer were affected by practice organizations differently, depending on whether they were scheduled in random or blocked order. When the practice was organized in so-called “random order”, it consisted of the training trials arranged randomly with rapidly changing order. It was defined as a high CI. The term random practice is interchangeably used with interleaved practice3,4. On the other hand, the term blocked order was used when trials corresponding to one skill variation were completed before introducing the next skill. The blocked order, sometimes called repetitive practice5, was defined as a low CI.
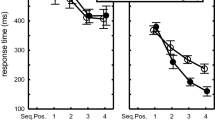
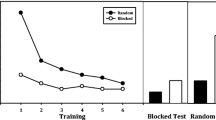
Battig2 noted that random practice condition hinders performance during acquisition, although it facilitates retention and transfer. Participants learning in high CI conditions had better retention and transfer results than the low CI practice groups. Battig focused on verbal learning2; however, specialists in motor learning realized the importance of these findings. The first study using a motor task was conducted by Shea and Morgan6. In their study, now considered classical in motor learning, participants learned three motor barrier knock-down tasks (the purpose of the task was knocking down a specified number of six freely moveable barriers in a prescribed order) in a blocked (low CI) or random (high CI) order. The reaction and movement time (and total time) were measured, evincing that, during acquisition, these times were shorter in the low CI group. Conversely, in retention tests, these times were the longest for the low CI group, tested in a random order, i.e., tested in high CI6. Such discovery, supported by tens of similar findings, had a profound effect in laboratory and field-based studies. Many motor learning books suggest that implementing high CI in practice may enhance learning and transfer7,8,9,10. Despite the fact that there were studies questioning the positive effect of the high CI on retention and transfer or at least showing its relatively small effect size in field studies7,11, most of the reviews and publications focusing on the CI effect in motor learning suggest that this effect is robust across tasks and fields12,13,14,15,16 marginally mentioning the limitations of the CI effect (compared to the emphasized benefits).
Recently, the CI effect aroused interest among researchers focusing on the neurophysiology of motor learning. Their studies reported differences in Central Nervous System (CNS) regions activations while acquiring skills under blocked and random conditions17. These findings sparked an interest in contextual interference topic among more extensive group of researchers.
In 2004, Brady7 formulated first doubts about the CI effect. Considering ES in basic research (Cohen’s d = 0.57) and applied research (Cohen’s d = 0.19), Brady noted that future studies should answer the question asked by Al-Mustafa11 whether CI is a laboratory artifact or sport-skill related.
In 2023, Ammar and colleagues published their meta-analysis18. Unfortunately, it was poorly performed. For example, they searched the Taylor and Francis database, though it is a publisher base, not a scientific one. At the same time, they did not screen the EBSCO database, which consists, among the others, of APA PsycArticles, APA PsychInfo, SPORTDiscus with Full Text, Medline, and Academic Search Complete. Their review was not preregistered, which is a standard procedure these days. Given these methodological flaws, the review of Ammar et al. cannot be considered reliable and valid.
Many of the narrative reviews7,12,13,14,15,16,19,20 did not specify what search terms were used to identify the included studies. The authors did not report the effect sizes of the reviewed studies, either. In a meta-analytic review on CI by Lage21, the authors presented all of the aforementioned components: search terms were specified, and effect sizes of the studies have been reported. Nevertheless, no blocked practice schedule was included, as the study's primary goal was to compare the effect of random and serial practice on transfer and retention.
The meta-analyses on CI conducted by Graser22 and Sattelmayer23 provided the inclusion criteria. However, population criteria were restricted to children with cerebral palsy22 or students in medical and physiotherapy education23.
Given all of the above, it is crucial to update and perform a meta-analysis focusing on the CI effect on retention in general population since retention was the most conspicuous and paradoxical effect reported by Battig2. We hope this meta-analysis may help solve some of the controversies about the CI effect in motor learning.
Therefore, the study's primary objective is to determine the effect of CI on retention in motor learning, as it was initially the main objective of Shea and Morgan study6. In order to be consistent with previous Brady’s meta-analysis7, we formulated secondary objectives based on Brady’s inclusion criteria, i.e.:
-
(1)
To estimate the CI effect in laboratory vs. field-based studies
-
(2)
To estimate the CI effect in young vs. adults vs. elderly adults
-
(3)
To estimate the CI effect in novice vs. experienced participants
Methods
The study was registered in PROSPERO under the number CRD42021228267. The review was conducted according to PICO guidelines24, the PRISMA Statement25 and was supplemented by the Quality Assessment Tool for Quantitative Studies26.
Due to number of included studies, the review has been split into two consecutive papers: retention and transfer meta-analyses. Retention performance was analyzed in the present study.
Inclusion and exclusion criteria
Eligible studies were identified based on PICO (Population, Intervention, Control, Outcome):
Population: young, adult, novice, experienced. Only healthy participants, as classified by authors of the primary studies, were included. We did not include studies on disabled participants. The population criteria were divided into two variables. The first variable was related to the age of the participant. Participants classified as Young were under 18 years old, those between 18 and 60 years old were classified as Adults. Older Adults were participants over 60 years old. The second variable was experience. We recognized Novice and Skilled (Experienced) participants according to the authors’ statement.
Intervention: high CI (random/interleaved schedule); field setting.
Control: low CI (blocked schedule/ repetitive practice); laboratory settings.
The studies utilized a wide variety of motor tasks and experimental procedures. However, only the single-task procedure (as opposed to dual-task procedure, only one task is performed at a time) was considered relevant for this review.
The main category considered for analysis was the contextual interference—studies including groups with different practice order: random schedule (high CI) and blocked schedule (low CI) were compared.
The subgroup analysis was performed. Firstly, the intervention category was related to the nature of research—studies conducted in a field setting using typical sports skills (applied research) were matched up with studies carried out in a controlled laboratory environment (basic research). The second category of subgroup analysis was the age of the participants: young (< 18 y), adults and older Adults (≥ 60 y). The third category was the experience—experienced participants vs. novices.
Outcome: retention test results. The primary outcomes were the standardized effect sizes of CI in retention in motor learning. The outcomes evaluating retention of the learned motor skill were considered selectable. Considering the effect of sleep-induced consolidation of trained skills27,28, meta-analysis consisted of delayed retention results only, i.e., results of the tests performed after 24 h while systematic review consisted of immediate and delayed retention test results. We assumed that most of the analyzed study participants should have slept between acquisition and retention tests during the last 24 h. As Diekelmann and Born27(p.114) noticed, “Sleep has been identified as a state that optimizes the consolidation of newly acquired information in memory, depending on the specific conditions of learning and the timing of sleep.”, hence the CI effect should more conspicuous after memory consolidation. Studies describing immediate retention results were discussed in the systematic review.
Search methods and selection procedure
AW performed the search on the following databases: Scopus (“contextual interference” in Title OR Abstract OR Keywords), EBSCO (“contextual interference” in Title OR Abstract—no Keywords option), Web of Science (“contextual interference” in Topic), ScienceDirect (“contextual interference” in Title OR Abstract OR Keywords), in April 2020 (for the period 1966 to 2020), updated in September 2021 (period 2020 to 2021) and November 2022 (period 2021–2022). Additionally, relevant studies were scrutinized using the Google Scholar search engine (“contextual interference” in Title OR Abstract OR Keywords). PsycINFO (EBSCO) database was searched by SC (“contextual interference” in Title OR Abstract OR Keywords).
For the reliable risk-of-bias assessment, the “grey literature” (i.e., Ph.D. dissertations and conference proceedings) available on-line in the searched databases has been excluded as well as studies in languages other than English.
Given the large number of retrieved citations we applied a method proposed by Dundar and Fleeman29. AW evaluated all the titles, keywords, and abstracts of the studies for inclusion and exclusion criteria and a random sample was cross-checked by senior researcher (SC). Ineligible articles were excluded. Duplicates of identified studies have been removed.
Two co-authors (AW and PS) read the full text of the studies, independently assessing the papers for final eligibility. Any discrepancies between the two authors were discussed with the senior researcher (SC) to reach a consensus.
Data collection and analysis
AW and PS summarized relevant data in developed MS Excel data extraction forms during the screening. Each entry consisted of study characteristics: the authors' names, the title of the study, year of publishing, journal title, and number of experiments (in case of multiple experiments in the same publication). Further details were based on PICO criteria:
- Population (number of participants, age, expertise level, gender),
- Intervention (nature of research, practice schedule, type of motor task, testing procedure, dependent variable),
- Objectives/outcomes (extracted means and standard deviations for all groups and all measures -immediate retention results and delayed retention results). Only the results of the first block in the retention testing procedure were considered for extraction. We assumed that the following blocks may promote further learning. If SEM (standard error of the mean) was available, we converted it into SD. Similarly, if quartiles were available, we converted these with Mean Variance calculator30,31,32,33. Whenever required, the positive/negative effect sizes were transformed to ensure that positive always favors random practice.
We included the results from both, blocked and random scheduled retention tests. If participants were tested in both conditions, both results were included independently. In addition, based on the Quality Assessment Tool for Quantitative Studies (described in the following section), study quality indicators were included (covering: selection bias, study design, confounders, blinding, data collection methods, withdrawals, and dropouts, global rating).
Since the included studies utilized different motor skills (tasks), retention was measured using different scores (numbers, percentages) or units (seconds, meters, number of cycles, etc.), we summarized the analysis using standardized mean difference (SMD) as an effect size measure, i.e. Hedges’ (adjusted) g, very similar to Cohen's d, but it includes an adjustment for small sample bias34,35.
Heterogeneity among the studies was evaluated using I2 statistics. The interpretation of I2, is as follow: 30% to 60% represent moderate heterogeneity; 50% to 90%—substantial heterogeneity; and 75% to 100%—considerable heterogeneity36. However, thresholds for interpretation can be misleading37.
Following guidelines were applied while interpreting the magnitude of the SMD in the social sciences: small, SMD = 0.2; medium, SMD = 0.5; and large, SMD = 0.838.
Given that the studies included in our analyses could yield more than one outcome, we decided to use a model that accounts for various sources of dependence, such as within-study effects and correlations between outcomes. Since there is no universally accepted method for this, we opted to apply two different approaches, each with its own advantages and disadvantages. The first approach is based on a three-level mixed model. The second approach is a classical random-effects model based on averaged outcomes (SMDs) from a single study.
Three-level mixed model
A three-level mixed model which uses (restricted) maximum likelihood procedures39,40 was computed. The model considers the potential dependence among the effect sizes, i.e. when there are multiple outcomes (effect sizes) from one study. The model assumes that the random effects at different levels and the sampling error are independent. The first level of the model refers to variance between effect sizes among participants (level 1). The second level refers to outcomes, i.e. effect sizes extracted from the same study (level 2; within-cluster variance). The third level refers to studies (level 3; between-clusters variance)39. Given the second level in the model accounts for sampling covariation, the benefit of this model is that it is no crucial to know or estimate correlations between outcomes from extracted one study39,41.
Sensitivity analysis was performed using Cook’s D distances. Outcomes further than 4/n (where n was the number of outcomes) were removed to assess how these outliers influence the pooled effect. Meta-analyses were performed with RStudio (version 2023.06.0) and the following packages “metaphor”, “dmetar”, “tidyverse”, “readxl”, and “ggplot”.
Random-effects model with averaged outcomes (effect sizes)
We applied a random effects model which estimates the mean of this distribution of true effect sizes. We applied the model based on averaged outcomes, whenever these outcomes were drawn from the same population (same study). We computed average standard errors using variances and then took the square root, as this approach typically yields the most meaningful results. In this approach, the problem of potential correlations between results is resolved. However, the limitation of this method is that averaging effect sizes from a single study reduces the variances between them, and informative differences between outcomes are lost42,43.
Like in the previous analysis, sensitivity analysis was performed using Cook’s D distances. Meta-analyses were performed with RStudio (version 2023.06.0) and the following packages “tidyverse”, “readxl”, “metaphor”, “dmetar”, and “meta”.
Assessment of risk of bias/quality assessment in included studies
The risk of bias in included studies has been assessed using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies44. The checklist components are as follows: sample selection, study design, identification of confounders, blinding, reliability and validity of data collection methods, as well as withdrawals and dropouts. These elements can be rated strong, moderate, or weak, corresponding to a standardized guide and dictionary. The comprehensive evaluation of the study is determined by assessing six rating aspects. Studies with no weak ratings and at least four strong ratings are regarded as strong. Those with less than four strong ratings and one weak rating are considered moderate, and those with two or more weak ratings are considered weak26.
AW and PS independently assessed the level of evidence and methodological quality of the eligible studies (Appendix 1, https://osf.io/r59zs/?view_only=61397e4508384d13960936a556890962). In case of disagreement, the authors discussed until consensus was reached. If any hesitance arose regarding the quality of the study, the problem was discussed with the senior researcher (SC).
Results
Results of the search
The primary search on electronic databases identified 2119 potential records. After removing duplicates, titles and abstracts of 1255 articles were screened according to PICO criteria, of which 961 records were excluded due to topic reasons, study design issues, and population. The detailed evaluation process is highlighted in the PRISMA Flow Diagram45 (Fig. 1).

PRISMA flow diagram of the search process45. Flowchart of the primary search (time period 1966 to 2020), updated searches (time period 2020 to 2021 and 2021 to 2022), and the inclusion and exclusion process.
The remaining 294 studies were evaluated, and 235 of these were excluded (detailed reasons for exclusion are listed in Appendix 2, https://osf.io/r59zs/?view_only=61397e4508384d13960936a556890962). Four studies did not match population criteria and were excluded (participants with hyperfunctional voice disorders, participants with Parkinson’s disease, children with Developmental Coordination Disorder, individuals with visual impairments). The topics of nine studies were not relevant to the main objectives of our review (related to agility training, chunking process, neural network simulation, the effect of cues, observational learning, feedback, awareness of maximal fluidity). Eighty-two articles were excluded because the study design was not relevant to PICO criteria. Two studies were excluded as the authors either did not provide details on dependent measures or did not inform how the dependent variables were quantified.
Seventy-eight studies were not included due to missing data. In case data were not found in the article, the authors were contacted via e-mail and/or the ResearchGate platform. Ninety-six data requests have been sent, and thirty-eight answers (about 39 articles) were received. Thirteen of theses replays did not report the data, mainly due to a long time since publication. However, data related to twenty-five articles were successfully obtained.
Eighteen articles did not cover retention testing, focusing mainly on transfer. In 40 studies, only abstracts were presented in English. The results of two articles were similar to the same authors’ other articles’ outcomes.
Finally, 59 studies were included in the present systematic review, however the quantitative analysis covered 54 articles. Retention tests up to 24 h after the last acquisition session were defined as immediate retention testing. Accordingly, tests performed after 24 h and more were categorized as delayed. Five studies described immediate retention testing. These results were not included in the meta-analysis. An overview of all included studies is provided in Table 1.
Reasons for exclusion of individual experiments or particular groups of participants
From some studies not all experiments were included, only those that complied with the inclusion criteria. The reasons for exclusion are provided below.
In the study by Schorn and Knowlton4, two experiments were performed. Only the first one was included in the present review. The second experiment examined the transfer. Furthermore, the authors did not provide details regarding a number of participants in each of the four groups. Neither were these details provided in the paper nor by the authors in e-correspondence. Another study consisting of more than one experiment was an article by Ste-Marie and colleagues46, where CI effect on learning handwriting skills in young participants was examined. Only results of (immediate) retention testing were available from the third experiment, as the results available in the text regarding the second experiment mainly focused on transfer. It was not possible to obtain the results from the text in the first experiment.
Of the two experiments conducted in the study by Porter and Magill47, results from the first experiment were possible to obtain. In case of the study by Shea and colleagues48 we were not able to obtain the absolute timing error results (reported as non-significant) from the authors. The second experiment’ results of the mentioned study were not included due to group characteristics (group of ratio-feedback/blocked and random and group of segment-feedback/blocked and random) not compliant with PICO.
Chua and colleagues conducted three experiments, of which two (the second and the third one) were included in the present study. The first experiment was not included as it described constant practice group instead of blocked practice: Constant group participants were divided into three subgroups, and each subgroup threw from one of the distances (4 m, 5 m, or 6 m) for a total of 60 practice trials49. The study of Broadbent and colleagues50 consisted of two experiments. In the first experiment, the authors applied a dual-task procedure. The second one, beside CI effect, involved Stroop procedures which resulted in four groups (blocked-Stroop, blocked, random-Stroop, random). Hence, the results of two groups (random and blocked) were chosen for analysis. Sherwood51 conducted two experiments utilizing a rapid aiming task. However, the results of the second experiment were excluded from the present review, as these were considered to be transfer results.
In an experiment by Beik and colleagues52, participants were randomly assigned to six groups: blocked-similar, algorithm-similar, random-similar, blocked-dissimilar, algorithm dissimilar, or random-dissimilar. According to PICO, retention results of four groups (blocked-similar, random-similar, blocked-dissimilar, random-dissimilar) were considered applicable for the present review. Consistently, out of the four groups (blocked only, random only, blocked-then-random, and random-then-blocked) involved in the study by Wong and colleagues53, two groups were chosen for the purpose of the current review: blocked schedule group and random schedule group.
A study by Porter and colleagues54 described acquisition and retention of participants randomly assigned to three practice groups: high, moderate, and low CI group. For the present review, the retention results of two groups (high CI and low CI) were extracted. The following study of Porter55 consisted of three groups: blocked, random, and increasing-CI practice schedules. Only blocked and random schedule groups were included.
In the study by Del Rey and colleagues56, CI effect was examined in key-pressing task performed by five practice groups. The groups were different in terms of the administered amount of CI and the presence (or absence) of retroactive inhibition. Retention results of two groups (random, blocked-without retroactive inhibition) were chosen for the purpose of the present study.
French and colleagues57 in a study on CI in learning volleyball skills, randomly assigned participants to three acquisition groups: random, random-blocked, or blocked practice. The random and the blocked practice groups were included in the present review. Similarly, in an article by Goodwin and Meeuwsen on CI effect in learning golf skills58, three groups of participants were tested: learning in random, blocked-random, or blocked practice condition. Consistently, only blocked and random practice schedule groups were included in the current review.
Results of quality assessment of included studies
The results of the methodological assessment of the studies included in our systematic review are highlighted in Table 2. Only three articles presented moderate4,46 or high59 methodological quality according to the Quality Assessment Tool for Quantitative Studies44. The primary studies failed mainly on the following criteria: 44 articles scored weak rating in the Selection Bias section, in Withdrawals And Drop-outs section 50 studies scored weak rating. Such relatively strict evaluation records could be explained by the fact that two weak ratings were enough to automatically determine a weak classification of an article in its global rating for all six components of the checklist.
Only studies rated strong and moderate should be included in the meta-analysis26. However, excluding studies rated as weak would make our analysis rather dubious (with only two studies included). Therefore, we have included fifty-four articles in the meta-analysis. Consistently, the impact of this decision on heterogeneity was considered.
Findings
Only delayed retention testing results were included in the present meta-analysis, yielding 194 effect sizes. Outcomes from 54 studies were included in the meta-analysis, resulting in testing of 2068 participants, yielding 6183 measurements in total. A broad range of variables was involved: time (decision time, absolute error time, variable time, reaction time, response time, completion time), distance (accuracy error distance, absolute error distance, median pathway traveled), a number of performed movements, accuracy (accuracy scores, proficiency percentage). Outcome measures evaluating retention of the learned motor skills were presented in various units: meters, seconds, percentages, or scores.
In ten studies, the results of both testing procedures (immediate and delayed) were presented. In a study by Beik60, in addition to immediate testing, participants took part in delayed testing 24 h after their last acquisition session. In Kim's61 article, immediate retention testing was performed 6 h after acquisition, whereas the time interval between acquisition and delayed retention was 24 h. In a study by Porter62, immediate testing results and 7-days delayed testing results were presented. In an experiment by Kaipa et colleagues63, delayed retention testing was performed six days after acquisition. In an article by Parab and colleagues64, young participants took part in the following testing strategy: immediate testing, delayed testing trial (24 h after last acquisition), and finally—testing seven days after the last acquisition session. Wong and colleagues53 applied both testing procedures: immediate and delayed (48 h after the last acquisition session). Porter and Saemi55 described immediate and delayed (48 h) testing results. In an experiment by Li and Lima65, participants were involved in two testing procedures: immediate and delayed—24 h after the last acquisition session. A study by Sherwood51 described two testing strategies: immediate and 24 h delayed; similar procedures could be found in research by Green and Sherwood66.
Motor skills described in primary studies varied in many ways. They were presented in many configurations – gross motor skills or fine motor skills, continuous motor skills and discrete motor skills, open motor skills, and closed motor skills. Motor skills were associated with golf47,49,54,58,67,68, volleyball57,69,70,71, hockey72,73, soccer65,74, tennis75, darts throwing76,77, basketball55,62, dancing78, kicking79, throwing49,77,79,80,81,82,83, jumping80, hopping64, bench pressing59. Some studies described the CI effect in Pawlata roll learning84 and rifle shooting85. Non-sport skills included speech learning53 and laparoscopic skills86,87.
Other motor tasks included: the sequential key pressing task88,89,90,91, serial reaction time task4,92,93, sequential motor task52,60,94, visuomotor task95, motor sequence learning96, rapid aiming task51,66,97, pursuit tracking98,99, discrete sequential production task61,100 and time estimation task101.
Laboratory versus applied setting—comparison characteristics
Fifty-four studies were included in a laboratory vs. applied settings comparison. Five of these studies described results of immediate retention testing, of which two were conducted in laboratory settings56,102 and three in applied settings46,103,104. Thirty studies with reported results of delayed retention testing were carried out in the laboratory (89 effect sizes). In contrast, twenty-four studies describing delayed retention were conducted in applied settings (105 effect sizes).
Experiments conducted in laboratory settings included the following motor skills: sequential key pressing task88,89,90,91, sequential motor task52,60,94, serial reaction time task4,92,93, visuomotor task95, motor sequence learning96, rapid aiming task51,66,97, pursuit tracking98,99, oral motor learning task63 discrete sequential production task61,100 and time estimation task101.
In the study of Broadbent75, acquisition and retention of tennis skills were performed in laboratory settings. Learning and testing of golf skills and throwing were assessed by Chua et al.49. Similarly to Porter et al.54, participants practiced golf skills in the laboratory setting. In the study of Jeon74, the virtual reality-based balance tasks were performed using the Nintendo Wii Fit system. Moreno et al.77, in their study, focused on throwing in the laboratory setting—side throwing, low throwing, and darts throwing skills were learned and tested. Throwing and kicking skills presented in the experiment of Pollatou et al.79 were performed on the two apparatuses specially invented and constructed to measure the selected motor skills.
The study of speech training and testing53 by Wong et al. took place in the laboratory settings. The age of the participants in all the aforementioned laboratory experiments ranged from 11 years75 to 82 years74.
Studies conducted in applied settings were performed in natural environments (game-based or physical education class), examining: volleyball skills57,69,70,71, golf skills47,58,67,68, hockey72,73, soccer65, throwing skills80,81,82,83, basketball55,62, bench-pressing59, distance jumping80 and hopping64, as well as dancing skills78. Riffle shooting motor skills85 acquisition and testing were performed in indoor laboratories; however, all settings, including the position target height, followed the Olympic and International Shooting Sport Federation standards; therefore results of this experiment were included in the applied setting comparison.
Laparoscopic skills acquisition and testing were performed on medical students and post-graduate residents using a virtual reality simulator, mimicking the regular laparoscopic tasks87, using FLS Box trainer, in accordance to the Fundamentals of Laparoscopic Surgery (FLS) program86. The experiment utilizing Pawlata roll skill105 took place in the indoor pool.
The age of the participants in the group of applied studies ranged from 6 years83 to 34 years62. Adult participants were primarily students. An article by Souza and colleagues 106 was the only study describing the retention of motor skills in older adults (65–80 years old) in an applied setting. The motor task performed in the study consisted of throwing a boccia ball to three targets. However, due to missing data, this study was excluded from meta-analytic analysis.
The CI effect in youth vs. adults vs. elderly adults—comparison characteristics
All participants included in the present review were from 6 years83 to 82 years old74. Analyzed age subgroups were: young (up to 18 years old), adults (18 years old to 59 years old), and older adults (60 years and older). The articles covering immediate retention reported results from 68 children and 90 adults. In the delayed retention studies, 418 young participants, 205 older participants, and 1425 adults were included in further analyses. In the article by Tsutsui82, the authors presented results of 20 participants from 15 to 22 years old; therefore, the results of this study were not included in the age subgroups analyses.
The CI effect in novice vs. experienced participants—comparison characteristics
In his meta-analytic study, Brady initially compared the CI effect between skilled and novice participants. He classified their skill levels based on how the studies’ authors labeled them7. We applied the same rule in our review. Consequently, we classified participants of five studies as skilled (n = 202). Participants of these studies were characterized as follows.
In an article by Porter and Saemi, the skill level of participants was characterized in the following way: “participants (…) were considered moderately skilled at passing a basketball, which involved skills they were taught in their respective basketball course. None of the participants played college or professional basketball; however, some participants acknowledged that they did play basketball recreationally from time to time”55 (p. 64–65). Participants in the experiment on CI in learning throwing skills by Tsutsui and colleagues82 were labeled as high-level pitchers (n = 10) or low-level pitchers (n = 10). They were assigned to the aforementioned groups based on pretest scores. In their experiment, Broadbent and colleagues107 described the CI effect on young participants' learning of tennis skills. Based on their skill level, athletes were classified as intermediate. Years of participants’ experience in tennis ranged from 5.3 ± 2.2 in the blocked group to 5.9 ± 3.1 in the random group. In their study, Frömer and colleagues76 investigated the CI effect in learning virtual darts throwing. Based on pretest scores, it was apparent that the participants were familiarized with throwing but were not experts. Participants in the study of Porter and colleagues were classified as unskilled: “(…) had less than two years’ basketball playing experience (1.1 ± 1.3 years) and no representative level basketball playing experience”62(p. 7).
Summarizing, the aforementioned studies described different standards of inclusion to skilled group. Due to this fact, our meta-analytic comparison of skilled versus novice participants was not considered.
Meta-analysis: results
Three-level mixed model
The analysis of contextual interference effect on delayed retention (Fig. 2) covered 54 primary studies and included 2068 participants, yielding 194 effect sizes (descriptions of the studies in Appendix 3 https://osf.io/r59zs/?view_only=61397e4508384d13960936a556890962 ).

The three-level mixed model analysis of retention test results of random vs. blocked practice. The forest plot presents the results obtained by participants aged 6–82, including various motor tasks and different outcome measures. (studies descriptions in Appendix 3 https://osf.io/r59zs/?view_only=61397e4508384d13960936a556890962).
The pooled effect size based on the three-level meta-analytic model was medium SMD = 0.63 (95% CI: 0.33, 0.93; p < 0.001). The estimated variance components (tau squared) were τ32 = 0.93 and τ22 = 0.34 for the level 3 and level 2 components, respectively. This means that I32 = 66% of the total variation can be attributed to between-cluster, and I22 = 24% to within-cluster heterogeneity. Total I2 = 90%.
Sensitivity analysis revealed that there were ten outcomes which were further than 4/n threshold: one outcome from Beik and Fazeli94; one from Beik et al.52; one from Bertollo et al.78; one from Green and Sherwood66; one from Immink et al.96; one from Kaipa and Kaipa63; one from Lin et al.92; one from Pasand et al.70; one from Shea et al.48; and from Wong et al.53.
After having removed the outliers, the pooled effect size was small SMD = 0.43 (95% CI: 0.19, 0.67; p < 0.001). The estimated variance components (tau squared) were τ32 = 0.44 and τ22 = 0.28; I32 = 51% and I22 = 33%; respectively. The outliers had a substantial effect on pooled effect size, i.e. SMD decreased from 0.63 (with outliers included) to 0.43 (without outliers).
Given that 36 outcomes were retrieved from the Parab’s et al. study64 we also performed a sensitivity analysis removing all 36 outcomes. The result was not substantially different from the full analysis: SMD = 0.69 (95% CI: 0.41, 0.97; p < 0.0001).
Random-effects model with averaged SMDs
The analysis based on averaged SMDs (form one study) yielded the following: SMD = 0.71 (95% CI: 0.41, 1.01; p < 0.001) (Fig. 3). The estimated variance components (tau squared) were τ2 = 1.3. Total I2 = 88.5%. The sensitivity analysis without two outcomes66,70 which were further than 4/n threshold, yielded the following SMD = 0.56 (95% CI: 0.32, 0.80; p < 0.001), τ2 = 0.64. Total I2 = 81.69%.

The random-effects model analysis of retention test results of random vs. blocked practice. In columns “Random Total” and “Blocked Total” are provided number of participants.
Laboratory vs. field-based (applied) studies
The included studies were divided into those carried out in a laboratory setting (n = 30), including 1210 participants (89 effect sizes), and the remaining (n = 24) conducted in an applied setting (105 effect sizes), including 858 participants.
Three-level mixed model
A subgroup analysis of the CI effect in laboratory studies was performed (Fig. 4). The test of moderators turned out to be significant F(1, 192) = 4.50, p = 0.03.

The three-level mixed model analysis of retention test results in a random and blocked schedule in a laboratory setting. The forest plot presents the retention test results obtained by participants practicing in a laboratory setting, including various motor tasks and different outcome measures.
The pooled effect size based on the three-level meta-analytic model was large SMD = 0.92 (95% CI: 0.48, 1.36; p < 0.001). The estimated variance components (tau squared) were τ32 = 1.28 and τ22 = 0.11 for the level 3 and level 2 components, respectively. Heterogeneity was high, I32 = 83% and I22 = 7%; total I2 = 90%. Sensitivity analysis revealed that after removing four outcomes, i.e. one from Green and Sherwood66; one from Lin et al.92; one from Shea et al.48; and one from Wong et al.53, the pooled effect size increased SMD = 0.93 (95% CI: 0.59, 1.23; p < 0.001).
Analogously, a subgroup analysis of the CI effect in applied studies was conducted (Fig. 5). The non-significant pooled effect size based on the three-level meta-analytic model was small SMD = 0.23 (95% CI: -0.16, 0.62; p = 0.24). The estimated variance components (tau squared) were τ32 = 0.58 and τ22 = 0.48 for the level 3 and level 2 components, respectively. Heterogeneity was high, I32 = 48% and I22 = 40%; total I2 = 89%.

The three-level mixed model analysis of random and blocked schedule retention test results in an applied setting. The forest plot presents the retention test results in an applied setting, including various motor tasks and different outcome measures.
Sensitivity analysis revealed that after removing three outcomes, i.e. one from Bertollo et al.78; one from Fazeli et al.68, and one from Pasand et al.70, the pooled effect size decreased to negligible and favoring blocked practice SMD = −0.01 (95% CI: −0.35, 0.32; p = 0.94).
Random-effects model with averaged SMDs
The test of moderators was statistically significant QM(1) = 4.11, p = 0.04.
For the studies in laboratory settings (Fig. 6), the model yielded the following: SMD = 0.99 (95% CI: 0.55, 1.43; p < 0.001), τ2 = 1.39. Total I2 = 81.69%. Green and Sherwood’66 results were removed during sensitivity analysis, yielding the following: SMD = 0.82 (95% CI: 0.49, 1.16; p < 0.001); τ2 = 0.70; I2 = 82.35%.

The random-effects model analysis of retention test results of random vs. blocked in an applied setting. In columns “Random Total” and “Blocked Total” are provided number of participants.
The model yielded the following for the studies in applied settings (Fig. 7): SMD = 0.35 (95% CI: −0.04, 0.73; p 0.08), τ2 = 0.75. Total I2 = 84.33%. Two outcomes were removed during sensitivity analysis, i.e. Parab et al.64 and Pasand et al.70. The model changed to SMD = 0.30 (95% CI: 0.04, 0.56; p = 0.02); τ2 = 0.22; I2 = 61.85%.

The random-effects model analysis of retention test results of random vs. blocked in a laboratory setting. In columns “Random Total” and “Blocked Total” are provided number of participants.
The CI effect in young vs. adults vs. elderly adults
Fifty-three studies were included in a meta-analytic comparison of the CI effect in three age groups, resulting in the testing of 205 older adults in total, 1425 adults, and 418 young participants. Participants (aged from 15 to 22 years old) from the study of Tsutsui82 were excluded from this comparison due to difficulty in qualifying them to any of the abovementioned age groups. This analysis yielded 6169 measurements in total and elicited: 49 effect sizes for young participants, 119 effect sizes for adults, and 24 effect sizes for the group of older adults.
Three-level mixed model
The test of moderators was not significant F(2, 189) = 1.69, p = 0.19; however we decided to perform the analysis anyway, because the differences between age groups (SMD) were quite substantial.
The pooled effect size based on the three-level meta-analytic model for the subgroups of young participants was negligible SMD = 0.02 (95% CI: -0.90, 0.94; p = 0.97). The estimated variance components (tau squared) were τ32 = 1.04 and τ22 = 1.05 for the level 3 and level 2 components, respectively. Heterogeneity was high, I32 = 47% and I22 = 47%; total I2 = 94%. (Fig. 8). Sensitivity analysis revealed that after removing two outcomes, i.e. one from Bertollo et al.78; and one outcome from Broadbent et al.75 the pooled effect size decreased to small SMD = −0.39 (95% CI: −1.30, 0.51; p = 0.39).

The three-level mixed model analysis of young participants’ retention tests results: random practice vs. blocked practice. The forest plot presents the retention test results obtained by participants aged 6–18, including a variety of motor tasks and different outcome measures.
The adult’s pooled effect size was medium SMD = 0.63 (95% CI: 0.30, 0.96; p = 0.54) (Fig. 9). The estimated variance components (tau squared) were τ32 = 0.42 and τ22 = 0.53 for the level 3 and level 2 components, respectively. Heterogeneity was high, I23 = 39% and I22 = 48%; total I2 = 86.82%. The estimated variance components (tau squared) were τ32 = 0.99 and τ22 = 0.03 for the level 3 and level 2 components, respectively. Heterogeneity was I32 = 85% and I22 = 2%; total I2 = 87%.

The three-level mixed model analysis of adult participants’ retention tests results: random practice vs. blocked practice. The forest plot presents the retention test results obtained by participants aged 18–59, including various motor tasks and different outcome measures.
Sensitivity analysis revealed that after removing seven outcomes, i.e. Green and Sherwood66; one from Immink et al.96; one from Kaipa and Kaipa63; one from Lin et al.92; one from Pasand et al.70; one from Shea et al.48; and from Wong et al.53, the pooled effect size decreased to small SMD = 0.45 (95% CI: 0.24, 0.66; p < 0.001).
The pooled effect size for older adults was large SMD = 1.45 (95% CI: 0.55, 2.35; p = 0.003) (Fig. 10). The estimated variance components (tau squared) were τ32 = 0.99 and τ22 = 0.10 for the level 3 and level 2 components, respectively. Heterogeneity was high, I23 = 80% and I22 = 8%; total I2 = 88%.

The three-level mixed model analysis of older adults’ retention tests results: random practice vs. blocked practice. The forest plot presents the retention test results obtained by participants aged 60–82, including a variety of motor tasks and different outcome measures.
In sensitivity analysis, one outcome from Beik et al.52 was removed yielding large pooled effect size SMD = 1.64 (95% CI: 0.53, 2.75; p = 0.005).
Random-effects model with averaged SMDs
Test of Moderators turned out to be insignificant: QM(df = 2) = 4.50, p = 0.11.
For the studies with young participants, the model yielded the following: SMD = 0.28 (95% CI: -0.51, 1.08; p = 0.48); τ2 = 1.17; I2 = 91.07% (Fig. 11). During sensitive analysis, Parab’s et al.64 outcomes were removed and, as a result, SMD = 0.58 (95% CI: −0.03, 1.18; p = 0.06); τ2 = 0.53; I2 = 82.83%.

The random-effects model analysis of young participants’ retention tests results: random practice vs. blocked practice. In columns “Random Total” and “Blocked Total” are provided number of participants.
For the studies with adults, the model yielded the following: SMD = 0.66 (95% CI: 0.32, 1.01; p < 0.001), τ2 = 1.06; I2 = 87.84% (Fig. 12). Two studies were removed based on sensitivity analysis, Green and Sherwood66 and Pasand et al.70. The model yielded the following SMD = 0.47 (95% CI: 0.23, 0.70; p = 0.06); τ2 = 0.39; I2 = 73.22%.

The random-effects model analysis of adults’ participants’ retention tests results: random practice vs. blocked practice. In columns “Random Total” and “Blocked Total” are provided number of participants.
For the studies with older adults, the model yielded the following: SMD = 1.58 (95% CI: 0.62, 2.54; p = 0.001), τ2 = 1.15; I2 = 82.63% (Fig. 13). There were no outliers further than 4/n distances from the threshold.

The random-effects model analysis of older adult’s participants’ retention tests results: random practice vs. blocked practice. In columns “Random Total” and “Blocked Total” are provided number of participants.
Risk of publication bias assessment
Substantial heterogeneity (high I2 values) was present in almost every analysis. According to Van Aert and colleagues, none of the publication bias methods has desirable statistical properties under extreme heterogeneity in true effect size108. Therefore, plotting a funnel plot as a visual aid for detecting bias or systematic heterogeneity, in this case, was doubtful. We did not apply other analysis methods, i.e., Egger’s regression test or rank-correlation test.
The possible reasons for high I2 values are elaborated on in the “Discussion”.
Discussion
The study's main objective was to determine the effect size of CI on retention in motor learning. When applying the three-level mixed model, we found that the pooled effect size was statistically significant and medium (SMD = 0.63). Analysis with the random-effects model on averaged outcomes for singles studies yielded similar results, i.e., statistically significant medium effect (SMD = 0.71).
Our secondary objectives were to estimate the CI effect in laboratory versus non-laboratory studies and estimate the CI effect in different age groups. Only analysis of laboratory studies yielded statistically significant results, and the SMD was large (the three-level mixed model SMD = 0.92; the random-effects model SMD = 0.99). Analysis of applied studies turned out to be statistically insignificant, and the effect size was slightly above negligible (SMD = 0.23 in the three-level mixed model and SMD = 0.28 in the random-effects model). In both analyses, random practice was favored.
Lee and White109 suggested that CI effect is more conspicuous in laboratory settings as tasks are less motor demanding, more cognitively loaded, lack intrinsic interest, and quickly reach an asymptote. The robustness of the CI effect in a laboratory setting, on the other hand, might be attributed to its well-controlled specification. Additionally, as Jeon and colleagues74 noticed, the CI effect in laboratory settings was frequently associated with simple tasks. In contrast, CI in more complex tasks was often examined in the field setting. One plausible explanation of this finding may be that the complexity of the sport task, alongside high interference practice, could be too challenging for the information processing system, negatively affecting learning110,111. Therefore, the CI effect in applied setting may not be so conspicuous.
The analyses in age groups yielded significant results in older adults in both analyses. In the first place, CI effect in motor learning of older adults was large (in the three-level mixed model SMD = 1.45 and SMD = 1.58 in the random-effects model), i.e., a random schedule was more beneficial for retention.
The benefits of implementing random practice in motor learning for adult participants were medium (SMD = 0.63 in the three-level mixed model and SMD = 0.66 in the random-effect model). However, the difference between the blocked and random groups of adults was insignificant in the three-level mixed model, whereas it was significant in the random-effect model. The CI effect in young participants was statistically insignificant, and the SMD was negligible in the three-level model (SMD = 0.02) and small in the random-effects model (SMD = 0.28).
The overall results of our review partially corresponded with those reported in the meta-analysis by Brady7. In line with the constantly advancing methodology of conducting meta-analyses, the inclusion criteria implemented in this review were more thoroughly detailed than those presented in Brady’s study7. Consequently, 13 following studies included in Brady’s meta-analysis were considered irrelevant in the present review and, therefore, excluded. The primary studies by Landin and Hebert112, Sekiya and colleagues113,114,115, Wulf and Lee116 described serial practice order instead of random schedule. In the studies by Hebert110, Smith117, Smith and colleagues118, Wrisberg and Liu119 alternating practice instead of random schedule was presented. In the article by Hall and Magill120, experiment described by Lee and colleagues121, and a study by Shea and Titzer122 multiple task learning was implemented. In the article by Bortoli and colleagues123, included in Brady’s meta-analytic study7, constant and variable practice schedules were compared. Unfortunately, data from 19 primary studies, included in his meta-analysis, were not available. Therefore, 12 primary articles included in Brady’s study7 constituted to our meta-analysis, yielding 29 effect sizes.
The remaining 42 primary articles included in our study (yielding 165 effect sizes) were not included in Brady’s study7. Despite this fact, the outcomes of the present review supported previous results of the CI effect described by Brady. In his study, the effect size of the randomized schedule in a laboratory setting was medium (ES = 0.57)—similarly to the outcome obtained in the present meta-analysis. Furthermore, Brady7 reported a different magnitude of randomization for adults and young participants. The CI effect in motor learning of young participants (ES = 0.10) was described as almost trivial, whereas the randomization effect in motor learning of adults was considered roughly moderate (ES = 0.35). Our findings were consistent, showing significant differences of CI effect between age groups. The pooled effect size for young participants was also negligible, the beneficial effect of randomization in adults was medium. The effect size of CI effect in the group of older adults was close to large and this age group is hard to compare since Brady did not recognized older adults as a separate subgroup.
Our results are different from those reported by Ammar and colleagues18. We found that the pooled effect size was medium 0.63 while Ammar et al. reported small. Probably the differences we found may be attributed to the search strategies, number of studies and effects sizes included in both meta-analysis. Ammar et al. omitted EBSCO database (including APA PsycArticles, APA PsychInfo, SPORTDiscus with Full Text, Medline, and Academic Search Complete), searching a publisher database instead (Taylor and Francis). They finally included 28 studies and 84 ES whereas in our meta-analysis 54 studies and 194 ES were included. Similarly, the differences in subgroups analysis can be explained in methods applied.
Age- and settings-related differences
The most interesting trend found in our and Brady’s7 meta-analysis was that the CI effect is more conspicuous in older adults. However, what has to be emphasized is that all included experiments with older adults' participation were performed in a laboratory setting. On the opposite, only one primary study75, including 18 young participants, was conducted in a laboratory setting. The remaining studies, including 400 youth, were performed in an applied setting. Due to this fact, it is difficult to differentiate whether participants' age plays a crucial role in the CI effect. Perhaps it is the setting that is critical when considering the CI effect? To solve this problem, more studies on children in a laboratory and more studies on older adults and elderly in an applied setting could be conducted. Given the disparity between settings in different age groups, the overall CI effect in different age groups may be biased. Analogically, one could claim that the results of the settings comparison may be biased, i.e., in the applied setting, only children (except for one study) and no older adults are included. The opposite situation is noticed in a laboratory setting.
Ammar and colleagues18 reported that CI effect was present only in 20–24 and 25–32-year-old participants (small and moderate ES, respectively) whereas blocked practice was favored in older adults. Again, these contradictions to our findings may be attributed to the different search methods and the number of studies and effect sizes included in both meta-analysis.
Low quality and bias problem
Given the results of the methodological assessment of the included studies, we need to consider that the CI effect as described here may be biased. According to the Quality Assessment Tool for Quantitative Studies, only three articles out of 54 presented moderate or high quality26. None of the study’s protocols was published prior to the study's commencement.
Participants were not likely to be representative in 37 out of 59 studies included in this review. Additionally, the answer was “Can’t tell” in ten other studies. In 47 out of 59 studies, the sample was not representative of the target population. In 38 out of 59 studies, the question about the critical differences between groups prior to the intervention was answered: “Can’t tell”. In 56 out of 59 studies, there was no information on whether the assessor(s) was aware of the intervention or the exposure status of participants. In 39 out of 59 studies, there was no information on whether participants were aware of the study research question. 51 out of 59 studies did not report the withdrawal and dropout numbers and reasons. Unfortunately, studies on the CI effect are of poor quality. When considering all of the limitations of the included studies, we cannot tell whether participants were aware of the study research question. One may conclude that studies on CI may be biased. Therefore, the question initially asked by Al-Mustafa11 and re-asked by Brady7 has to be re-stated again: is "contextual interference a laboratory artifact or sport-skill related''?
Heterogeneity problem
The possibility of substantial heterogeneity in the analyses was considered when planning our review and introducing the broad PICO criteria. Differences in populations such as age and origin, followed by a variety of included motor tasks and outcome measures, could contribute to increased heterogeneity. Additionally, the number of primary studies (and consequently different methodologies such as experiment duration) could determine the level of heterogeneity. According to Van Aert and colleagues: “none of the publication bias methods has desirable statistical properties under extreme heterogeneity in true effect size”108(p.8). Another source of heterogeneity could be the low quality of the included studies.
There are many reasons why I2 values could have been so high. First of all, it may be due to the test we used. We used I2 index instead of Q test that was used by Brady (2004). It is because Q test informs about the presence versus the absence of heterogeneity, whereas I2 index also quantifies the magnitude of heterogeneity124. Second, in all our analyses, more than 24 outcomes were included. In the general analysis, 194 outcomes were used. However, the more studies are included in the heterogeneity tests the higher is I2 value125. As Schroll and colleagues126 noted, if there are very few studies included in the meta-analysis, with relatively few participants, the risk of high heterogeneity as quantified with I2 value (> 50%) is very small, although the heterogeneity may be present. Unfortunately, authors dealing with high heterogeneity cannot do much about it. Increased precision does not solve the problem127, and there is little advice for authors on how to deal with it126.
Limitations
Firstly, there is a dependency within studies problem when multiple outcomes from a single study come from the same sample. Unfortunately, there is no simple answer to how to deal with such a problem. The most reliable approach would be to calculate the correlations between outcomes from the same sample using the raw data. This approach is, however, infeasible—many authors do not want to share their results, many have already lost them, and many authors passed away (given that we were analyzing results from 1966).
Additionally, the most popular approaches include averaging effect sizes derived on the same sample, analyzing each type of outcome separately, and applying three-level mixed models. Again, each of these approaches has its advantages and limitations. In our case, we decided that the most suitable would be to apply the three-level mixed model. Though the model assumes that there is no correlation between outcomes (effects sizes) obtained from the same sample, as Van den Noorgate et al.41 noticed, “An important conclusion is that, although the multilevel model we proposed for dealing with multiple outcomes within the same study in principle assumes no sampling covariation (or independent samples), our simulation study suggests that using an intermediate level of outcomes within studies succeeds in accounting for the sampling covariance in an accurate way, yielding appropriate standard errors and interval estimates for the effects” (p.589). Nevertheless, one may doubt the model since it assumes the effect sizes are independent.
To compare our results, we applied another model, the classical random-effects model; however, we used averaged effect sizes whenever they were derived from the same studies (same population). This approach is not potentially biased due to the dependency problem; however, it loses its informative value since the variance between effect sizes is reduced41.
What is worth mentioning is that both models we applied yielded very similar results.
One could suggest that we could analyze each outcome type, e.g., grouping them according to the skill characteristic (throws, aiming, kicking, etc.) or nature of the outcome (force production, scoring system, reaction time, movement time, kinematic characteristics, etc.). This approach would require a robust theoretical framework to differentiate different outcomes. Our potential readers should consider the limitations and advantages of our analyses.
Secondly, we did not study practice volume or nominal task difficulty in our analyses. These may be important factors contributing to the overall pooled effect size; however, given our review is broad in scope, more detailed analyses could be performed in the subsequent studies.
Thirdly, an analysis focusing exclusively on experience as a contributing factor affecting CI effect could be performed. However, a thorough and detailed definition of experience might be used.
Recommendation for future research
There is a limited number of motor learning studies utilizing young (up to 18 years old) healthy participants in a laboratory setting. Most motor learning studies with older adults (60 years and older) are performed in a laboratory setting. Therefore, we recommend further research on the CI effect, including young participants in a basic (laboratory) setting. We would also suggest future research on the CI effect in older adults (60 years and older) conducted in an applied setting.
In the subsequent studies, researchers could put a strong emphasis on the quality (methodology) of the research.
Conclusions
The Ci effect is a robust phenomenon in motor learning. Our results evinced, however, that, similarly to Brady (2004), this claim is primarily based on laboratory studies in adults and older adults. Experiments conducted in applied settings yielded fewer convincing results. Moreover, high CI does not benefit retention in young participants. It does in adults and older adults.
Practitioners, should consider other factors, e.g., the interaction between the skill level of the performer's motor complexity, cognitive load, and the performer’s intrinsic interest, while deciding how to structure practice and how much CI apply.
Data availability
Data is available in the open repository, https://osf.io/r59zs/?view_only=61397e4508384d13960936a556890962
References
Raviv, L., Lupyan, G. & Green, S. C. How variability shapes learning and generalization. Trends Cogn Sci. 26, 462–483 (2022).
Battig, W. F. Facilitation and interference. In Acquis Ski (ed. Bilodeau, E. A.) 215–244 (Academic Press, 1966).
Lin, C. H. J. et al. Brain–behavior correlates of optimizing learning through interleaved practice. Neuroimage. 56, 1758–1772 (2011).
Schorn, J. M. & Knowlton, B. J. Interleaved practice benefits implicit sequence learning and transfer. Mem. Cogn. 49, 1436–1452 (2021).
Kim, T., Wright, D.L. & Feng, W. Commentary: Variability of practice, information processing, and decision making—How much do we know? Front. Psychol. [Internet]. https://doi.org/10.3389/fpsyg.2021.685749/full. Accessed 12 Aug 2021 (2021).
Shea, J.B. & Morgan, R.L. Contextual interference effects on the acquisition, retention, and transfer of a motor skill. J. Exp. Psychol. Hum. Learn. Mem. [Internet] 5, 179–187. http://content.apa.org/journals/xlm/5/2/179. Accessed 29 Sep 2017 (1979).
Brady, F. Contextual interference: A meta-analytic study. Percept. Mot. Skills [Internet]. 99, 116–126. https://doi.org/10.2466/pms.99.1.116-126 (2017).
Coker, C. A. Motor Learning and Control for Practitioners 3rd edn. (Routledge, 2017).
Magill, R. A. & Anderson, D. I. Motor Learning and Control: Concepts and Applications 11th edn. (McGraw-Hill Education, 2017).
Wright, D. L. & Kim, T. Contextual interference: New findings, insights, and implications for skill acquisition. In Skill Acquisition in Sport: Research, Theory and Practice 3rd edn (eds Hodges, N. J. & Williams, A. M.) 99–118 (Routledge, 2020).
Al-Mustafa, A.A. Contextual Interference: Laboratory Artifact or Sport Skill Learning Related. Unpublished Dissertation. (University of Pittsburgh, 1989).
Barreiros, J., Figueiredo, T. & Godinho, M. The contextual interference effect in applied settings. Eur. Phys. Educ. Rev. [Internet] 13, 195–208 https://doi.org/10.1177/1356336X07076876 (2007).
Lee, T. D. & Simon, D. Contextual interference. In Skill Acquisition in Sport: Research, Theory and Practice (eds Williams, A. M. & Hodges, E. J.) 29–44 (Routledge, 2004).
Magill, R.A. & Hall, K.G. A review of the contextual interference effect in motor skill acquisition. Hum. Mov. Sci. [Internet] 9, 241–89. http://www.sciencedirect.com/science/article/pii/016794579090005X (1990).
Merbah, S. & Meulemans, T. Learning a motor skill: Effects of blocked versus random practice a review. Psychol. Belg. [Internet] 51, 15–48. http://orbi.ulg.ac.be/bitstream/2268/105261/1/Merbah&Meulemans2011PsychologicaBelgica.pdf (2011).
Wright, D., Verwey, W., Buchanen, J., Chen, J., Rhee, J. & Immink, M. Consolidating behavioral and neurophysiologic findings to explain the influence of contextual interference during motor sequence learning. Psychon. Bull. Rev. [Internet] 23, 1–21 https://doi.org/10.3758/s13423-015-0887-3. Accessed 25 Sep 2017 (2016).
Henz, D., John, A., Merz, C. & Schöllhorn, W.I. Post-task effects on EEG brain activity differ for various differential learning and contextual interference protocols. Front. Hum. Neurosci. (2018).
Ammar, A. et al. The myth of contextual interference learning benefit in sports practice: A systematic review and meta-analysis. Educ. Res. Rev. 39, 100537 (2023).
Brady, F. A theoretical and empirical review of the contextual interference effect and the learning of motor skills. Quest [Internet] 50, 266–293. https://doi.org/10.1080/00336297.1998.10484285. Accessed 26 Sep 2017 (2017).
Lee, T. D. Contextual interference: Generalizability and limitations. In Skill Acquisition in Sport: Research, Theory and Practice 2nd edn (eds Hodges, N. J. & Williams, A. M.) 105–119 (Routledge, 2012).
Lage, G. M., Faria, L. O., Ambrósio, N. F. A., Borges, A. M. P. & Apolinário-Souza, T. What is the level of contextual interference in serial practice? A meta-analytic review. J. Mot. Learn. Dev. 10, 224–242 (2021).
Graser, J. V., Bastiaenen, C.H.G. & van Hedel, H.J.A. The role of the practice order: A systematic review about contextual interference in children. PLoS One 14 (2019).
Sattelmayer, M., Elsig, S., Hilfiker, R. & Baer, G. A systematic review and meta-analysis of selected motor learning principles in physiotherapy and medical education. BMC Med. Educ. (BioMed Central Ltd.) (2016).
Methley, A.M., Campbell, S., Chew-Graham, C., McNally, R. & Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. (2014).
Page, M. J. & Moher, D. Evaluations of the uptake and impact of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement and extensions: A scoping review. Syst. Rev. 6, 11 (2017).
Thomas, H., Ciliska, D., Dobbins, M. & Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid.-Based Nurs. 1, 176–184 (2004).
Diekelmann, S. & Born, J. The memory function of sleep. Nat. Rev. Neurosci. 11, 114–126 (2010).
Yang, G. et al. Sleep promotes branch-specific formation of dendritic spines after learning. Science (80-) 344, 1173–1178 (2014).
Dundar, Y. & Fleeman, N. Applying inclusion and exclusion criteria. In Doing a Systematic Review: A Student's Guide (Boland, A., Cherry, G.M., Dickson, R. eds.). 79–91 (SAGE, 2017).
Shi, J. et al. Optimally estimating the sample standard deviation from the five-number summary. Res. Synth. Methods 11, 641–654 (2020).
Shi, J., Luo, D., Wan, X., Liu, Y., Liu, J., Bian, Z. et al. Detecting the skewness of data from the sample size and the five-number summary. ArXiv (2020).
Wan, X., Wang, W., Liu, J. & Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 14, 14 (2014).
Luo, D., Wan, X., Liu, J. & Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 27, 1785–1805 (2018).
Deeks, J. & Higgins, J. Statistical algorithms in review manager 5. Stat. Methods Gr. Cochrane Collab. [Internet]. https://training.cochrane.org/handbook/current/statistical-methods-revman5 (2010).
Higgins, J.P.T. & Deeks, J. Chapter 6: Choosing effect measures and computing estimates of effect. In (Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M, et al. eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 63 [Internet]. https://www.training.cochrane.org/handbook (Cochrane, 2022).
Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J. et al. Cochrane Handbook for Systematic Reviews of Interventions | Cochrane Training. Version 6.2 (updated Feb 2021). (Cochrane, 2021).
Deeks, J. J., Higgins, J. P. T. & Altman, D. G. Analysing data and undertaking meta-analyses. Cochrane Handb Syst Rev Interv. 2019, 241–284 (2019).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences. 2nd Ed. (Routledge, 1988).
Assink, M. & Wibbelink, C. J. M. Fitting three-level meta-analytic models in R: A step-by-step tutorial. Quant. Methods Psychol. 12, 154–174 (2016).
Cheung, M. W. L. Modeling dependent effect sizes with three-level meta-analyses: A structural equation modeling approach. Psychol. Methods 19, 211–229 (2014).
Van den Noortgate, W., López-López, J.A., Marín-Martínez, F. & Sánchez-Meca, J. Three-level meta-analysis of dependent effect sizes. Behav. Res. Methods [Internet] 45, 576–594 https://doi.org/10.3758/s13428-012-0261-6. Accessed 28 Apr 2024 (2013).
Becker, B. J. Multivariate meta-analysis. In The Handbook of Applied Multivariate Statistics and Mathematical Modeling (eds Tinsley, H. E. A. & Brown, E. D.) 499–525 (Academic Press, 2000).
Cheung, S. F. & Chan, D. K. S. Dependent correlations in meta-analysis. Educ. Psychol. Meas. 68, 760–777. https://doi.org/10.1177/0013164408315263 (2008).
Thomas, H. Quality Assessment Tool for Quantitative Studies. Effective Public Health Practice Project (McMaster University, 2003).
Moher, D. et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev. Esp. Nutr. Hum. Diet. 20, 148–160 (2016).
Ste-Marie, D. M., Clark, S. E., Findlay, L. C. & Latimer, A. E. High levels of contextual interference enhance handwriting skill acquisition. J. Mot. Behav. 36, 115–126 (2010).
Porter, J. M. & Magill, R. A. Systematically increasing contextual interference is beneficial for learning sport skills. J. Sport Sci. 28, 1277–1285 (2010).
Shea, C. H., Lai, Q., Wright, D. L., Immink, M. & Black, C. Consistent and variable practice conditions: Effects on relative and absolute timing. J. Mot. Behav. 33, 139–152 (2001).
Chua, L. K. et al. Practice variability promotes an external focus of attention and enhances motor skill learning. Hum. Mov. Sci. 64, 307–319 (2019).
Broadbent, D.P., Causer, J., Williams, A.M. & Ford, P.R. The role of error processing in the contextual interference effect during the training of perceptual-cognitive skills. J. Exp. Psychol. Hum. Percept. Perform. [Internet] 43, 1329–1342 /fulltext/2017-12046-001.html (2017).
Sherwood, D. E. The benefits of random variable practice for spatial accuracy and error detection in a rapid aiming task. Res. Q. Exerc. Sport. 67, 35–43 (1996).
Beik, M., Taheri, H., Saberi Kakhki, A. & Ghoshuni, M. Neural mechanisms of the contextual interference effect and parameter similarity on motor learning in older adults: An EEG study. Front. Aging Neurosci. 12, 173 (2020).
Wong, A. W. K., Whitehill, T. L., Ma, E. P. M. & Masters, R. Effects of practice schedules on speech motor learning. Int. J. Speech Lang. Pathol. 15, 511–523 (2013).
Porter, J.M., Landin, D., Hebert, E.P. & Baum, B. The effects of three levels of contextual interference on performance outcomes and movement patterns in golf skills. Int. J. Sports Sci. Coach. 2, 243–255 https://doi.org/10.1260/174795407782233100 (2007).
Porter, J. M. & Saemi, E. Moderately skilled learners benefit by practicing with systematic increases in contextual interference. Int. J. Coach Sci. 4, 61–71 (2010).
Del Rey, P., Liu, X. & Simpson, K. J. Does retroactive inhibition influence contextual interference effects?. Res. Q. Exerc. Sport 65, 120–126 (1994).
French, K. E., Rink, J. E. & Werner, P. H. Effects of contextual interference on retention of three volleyball skills. Percept. Mot. Skills 71, 179–186 (1990).
Goodwin, J. E. & Meeuwsen, H. J. Investigation of the contextual interference effect in the manipulation of the motor parameter of over-all force. Percept. Mot. Skills 83, 735–743 (1996).
Naimo, M. A. et al. Contextual interference effects on the acquisition of skill and strength of the bench press. Hum. Mov. Sci. 32, 472–484 (2013).
Beik, M., Taheri, H., Saberi Kakhki, A. & Ghoshuni, M. Algorithm-based practice schedule and task similarity enhance motor learning in older adults. J. Mot. Behav. 53, 458–470 (2021).
Kim, T., Kim, H. & Wright, D. L. Improving consolidation by applying anodal transcranial direct current stimulation at primary motor cortex during repetitive practice. Neurobiol. Learn. Mem. 178, 107365 (2021).
Porter, C., Greenwood, D., Panchuk, D. & Pepping, G. J. Learner-adapted practice promotes skill transfer in unskilled adults learning the basketball set shot. Eur. J. Sport Sci. 20, 61–71 (2020).
Kaipa, R. & Mariam, K. R. Role of constant, random and blocked practice in an electromyography-based oral motor learning task. J. Mot. Behav. 50, 599–613 (2018).
Parab, S., Bose, M. & Ganesan, S. Influence of random and blocked practice schedules on motor learning in children aged 6–12 years. Crit. Rev. Phys. Rehabil. Med. 30, 239–254 (2018).
Li, Y. & Lima, R. P. Rehearsal of task variations and contextual interference effect in a field setting. Percept. Mot. Skills 94, 750–752 (2002).
Green, S. & Sherwood, D. E. The benefits of random variable practice for accuracy and temporal error detection in a rapid aiming task. Res. Q. Exerc. Sport 71, 398–402 (2000).
Brady, F. Contextual interference and teaching golf skills. Percept. Mot. Skills 84, 347–350 (1997).
Fazeli, D., Taheri, H. R. & Saberi, K. A. Random versus blocked practice to enhance mental representation in golf putting. Percept. Mot. Skills 124, 674–688 (2017).
Bortoli, L., Robazza, C., Durigon, V. & Carra, C. Effects of contextual interference on learning technical sports skills. Percept. Mot. Skills 75, 555–562 (1992).
Pasand, F., Fooladiyanzadeh, H. & Nazemzadegan, G. The effect of gradual increase in contextual interference on acquisition, retention and transfer of volleyball skillsce on acquisition, retention and transfer of volleyball skills. Int. J. Kinesiol. Sport Sci. 4, 72–77 (2016).
Zetou, E., Michalopoulou, M., Giazitzi, K. & Kioumourtzoglou, E. Contextual interference effects in learning volleyball skills. Percept Mot. Skills 104, 995–1004 (2007).
Cheong, J. P. G., Lay, B., Robert Grove, J., Medic, N. & Razman, R. Practicing field hockey skills along the contextual interference continuum: A comparison of five practice schedules. J. Sports Sci. Med. 11, 304 (2012).
Cheong, J. P. G., Lay, B. & Razman, R. Investigating the contextual interference effect using combination sports skills in open and closed skill environments. J. Sports Sci. Med. 15, 167 (2016).
Jeon, M. J. et al. Block and random practice: A wii fit dynamic balance training in older adults. Res. Q Exerc. Sport 92, 352–360 (2020).
Broadbent, D. P., Causer, J., Ford, P. R. & Williams, A. M. Contextual interference effect on perceptual-cognitive skills training. Med. Sci. Sports Exerc. 47, 1243–1250 (2015).
Frömer, R., Stürmer, B. & Sommer, W. (Don’t) Mind the effort: Effects of contextual interference on ERP indicators of motor preparation. Psychophysiology. 53, 1577–1586 (2016).
Moreno, J. et al. Contextual interference in learning precision skills. Percept. Mot. Skills 97, 121–128 (2003).
Bertollo, M., Berchicci, M., Carraro, A., Comani, S. & Robazza, C. Blocked and random practice organization in the learning of rhythmic dance step sequences. Percept. Mot. Skills 110, 77–84 (2010).
Pollatou, E., Kioumourtzoglou, E., Agelousis, N. & Mavromatis, G. Contextual interference effects in learning novel motor skills. Percept. Mot. Skills 84, 487–496 (1997).
Jiménez-Díaz, J., Morera-Castro, M. & Salazar, W. The contextual interference effect on the performance of fundamental motor skills in adults. Hum. Mov. 19, 20–25 (2018).
Saemi, E., Porter, J. M., Ghotbi Varzaneh, A., Zarghami, M. & Shafinia, P. Practicing along the contextual interference continuum: A comparison of three practice schedules in an elementary physical education setting. Kinesiology. 44, 191–198 (2012).
Tsutsui, S., Satoh, M. & Yamamoto, K. Contextual interference modulated by pitcher skill level. Int. J. Sport Health Sci. 3, 12 (2013).
Vera, J. G. & Montilla, M. M. Practice schedule and acquisition, retention, and transfer of a throwing task in 6-yr-old children. Percept. Mot. Skills 96, 1015–1024 (2003).
Smith, P. J. K. & Davies, M. Applying contextual interference to the Pawlata roll. J. Sports Sci. 13, 455–462 (1995).
Moretto, N. A., Marcori, A. J. & Okazaki, V. H. A. Contextual interference effects on motor skill acquisition, retention and transfer in sport riffle schooting. Hum. Mov. 19, 99–104 (2018).
Rivard, J. D. et al. The effect of blocked versus random task practice schedules on the acquisition and retention of surgical skills. Am. J. Surg. 209, 93–100 (2015).
Shewokis, P. A. et al. Acquisition, retention and transfer of simulated laparoscopic tasks using fNIR and a contextual interference paradigm. Am. J. Surg. 213, 336–345 (2017).
Li, Y. & Wright, D. L. An assessment of the attention demands during random- and blocked-practice schedules. Q. J. Exp. Psychol. Sect. A Hum. Exp. Psychol. 53, 591–606 (2000).
Simon, D. A. Contextual interference effects with two tasks. Percept. Mot. Skills 105, 177–183 (2007).
Simon, D. A., Lee, T. D. & Cullen, J. D. Win-shift, lose-stay: Contingent switching and contextual interference in motor learning. Percept. Mot. Skills 107, 407–418 (2008).
Wright, D. L., Li, Y. & Whitacre, C. The contribution of elaborative processing to the contextual interference effect. Res. Q. Exerc. Sport 63, 30–37 (1992).
Lin, C. H. et al. Contextual interference enhances motor learning through increased resting brain connectivity during memory consolidation. Neuroimage. 181, 1–15 (2018).
Lin, C. H. J. et al. Age related differences in the neural substrates of motor sequence learning after interleaved and repetitive practice. Neuroimage. 62, 2007–2020 (2012).
Beik, M. & Fazeli, D. The effect of learner-adapted practice schedule and task similarity on motivation and motor learning in older adults. Psychol. Sport Exerc. 54, 101911 (2021).
Chalavi, S. et al. The neurochemical basis of the contextual interference effect. Neurobiol. Aging 66, 85–96 (2018).
Immink, M. A., Pointon, M., Wright, D. L. & Marino, F. E. Prefrontal cortex activation during motor sequence learning under interleaved and repetitive practice: A two-channel near-infrared spectroscopy study. Front. Hum. Neurosci. 15, 229 (2021).
Russell, D. M. & Newell, K. M. How persistent and general is the contextual interference effect?. Res. Q. Exerc. Sport 78, 318–327 (2007).
Porter, J. M. & Beckerman, T. Practicing with gradual increases in contextual interference enhances visuomotor learning. Kinesiology. 48, 244–250 (2016).
Smith, P. J. K. Task duration in contextual interference. Percept. Mot. Skills 95, 1155–1162 (2002).
Kim, T., Chen, J., Verwey, W. B. & Wright, D. L. Improving novel motor learning through prior high contextual interference training. Acta Psychol. Amst. 182, 31 (2018).
Thomas, J. L. et al. Using error-estimation to probe the psychological processes underlying contextual interference effects. Hum. Mov. Sci. 79, 102854 (2021).
Broadbent, D. P., Causer, J., Mark Williams, A. & Ford, P. R. The role of error processing in the contextual interference effect during the training of perceptual-cognitive skills. J. Exp. Psychol. Hum. Percept. Perform. 43, 1329 (2017).
Aiken, C. A. & Genter, A. M. The effects of blocked and random practice on the learning of three variations of the golf chip shot. Int. J. Perform. Anal. Sport 18, 339–349 (2018).
Waqqash, E. & Low, J. Effects of contextual interference (CI) in basic squash shots practice. Malays. J. Sport Sci. Recreat. 11, 13–19 (2015).
Smith, P. J. K. & Davies, M. Applying contextual interference to the Pawlata roll. J. Sport Sci. 13, 455–462 (2008).
De Souza, M. G. T. X., Nunes, M. E. S., Corrêa, U. C. & Dos Santos, S. The contextual interference effect on sport-specific motor learning in older adults. Hum. Mov. 16, 112–118 (2015).
Broadbent, D.P., Causer, J., Ford, P.R. & Williams, A.M. Contextual interference effect on perceptual-cognitive skills training. Med. Sci. Sports Exerc. [Internet] 47, 1243–1250 https://pubmed.ncbi.nlm.nih.gov/25255127/ (2015).
Van Aert, R. C. M., Wicherts, J. M. & Van Assen, M. A. L. M. Publication bias examined in meta-analyses from psychology and medicine: A meta-meta-analysis. PLoS One. 14, e0215052 (2019).
Lee, T. D. & White, M. A. Influence of an unskilled model’s practice schedule on observational motor learning. Hum. Mov. Sci. 9, 349–367 (1990).
Hebert, E. P., Landin, D. & Solmon, M. A. Practice schedule effects on the performance and learning of low- and high-skilled students: An applied study. Res. Q. Exerc. Sport 67, 52–58 (1996).
Wulf, G. & Shea, C. H. Principles derived from the study of simple skills do not generalize to complex skill learning. Psychon. Bull. Rev. Psychon. Soc. Inc. 2002, 185–211 (2002).
Landin, D. & Hebert, E. P. A comparison of three practice schedules along the contextual interference continuum. Res. Q. Exerc. Sport 68, 357–361 (1997).
Sekiya, H. & Magill, R. A. The contextual interference effect in learning force and timing parameters of the same generalized program. J. Hum. Mov. Stud. 39, 45–71 (2000).
Sekiya, H., Magill, R. A. & Anderson, D. I. The contextual interference effect in parameter modifications of the same generalized motor program. Res. Q. Exerc. Sport 67, 59–68 (1996).
Sekiya, H., Magill, R. A., Sidaway, B. & Anderson, D. I. The contextual interference effect for skill variations from the same and different generalized motor programs. Res. Q. Exerc. Sport 65, 330–338 (1994).
Wulf, G. & Lee, T. D. Contextual interference in movements of the same class: Differential effects on program and parameter learning. J. Mot. Behav. 25, 254–263 (1993).
Smith, P. J. K. Applying contextual interference to snowboarding skills. Percept. Mot. Skills 95, 999–1005 (2002).
Smith, P. J. K., Gregory, S. K. & Davies, M. Alternating versus blocked practice in learning a cartwheel. Percept. Mot. Skills 96, 1255–1264 (2003).
Wrisberg, C. A. & Liu, Z. The effect of contextual variety on the practice, retention, and transfer of an applied motor skill. Res. Q. Exerc. Sport. 62, 406–412 (1991).
Hall, K. G. & Magill, R. A. Variability of practice and contextual interference in motor skill learning. J. Mot. Behav. 27, 299–309 (1995).
Lee, T. D., Wulf, G. & Schmidt, R. A. Contextual interference in motor learning: Dissociated effects due to the nature of task variations. Q. J. Exp. Psychol. Sect. A 44, 627–644 (1992).
Shea, J. B. & Titzer, R. C. The influence of reminder trials on contextual interference effects. J. Mot. Behav. 25, 264–274 (1993).
Bortoli, L., Spagolla, G. & Robazza, C. Variability effects on retention of a motor skill in elementary school children. Percept. Mot. Skills 93, 51–63 (2001).
Huedo-Medina, T., Sanchez-Meca, J., Marin-Martinez, F. & Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index?. Psychol. Methods 11, 193 (2006).
Rücker, G., Schwarzer, G., Carpenter, J. R. & Schumacher, M. Undue reliance on I2 in assessing heterogeneity may mislead. BMC Med. Res. Methodol. 8, 1–9 (2008).
Schroll, J. B., Moustgaard, R. & Gøtzsche, P. C. Dealing with substantial heterogeneity in Cochrane reviews. Cross-sectional study. BMC Med. Res. Methodol. 11, 1–8 (2011).
Alba, A. C. et al. High statistical heterogeneity is more frequent in meta-analysis of continuous than binary outcomes. J. Clin. Epidemiol. 70, 129–135 (2016).
Acknowledgements
All appendices are available at (https://osf.io/r59zs/?view_only=61397e4508384d13960936a556890962). We would like to thank all the authors who responded to our e-mails or messages and provided us with more information about their studies. The work was supported by the grant project with registration number MUNI/A/1470/2023 at Masaryk University Brno, Faculty of Sports Studies.
Author information
Authors and Affiliations
Contributions
AMW: Conceptualization; Writing-original draft; Writing–Review & Editing, Methodology, Investigation, Data curation, Formal analysis; Visualization, Resources. SHC: Conceptualization; Supervision, Writing-original draft; Writing-Review & Editing, Project Administration, Methodology, Formal analysis, Visualization, Resources. PS: Investigation, Data curation, Resources. PK: Statistical analysis assistance. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Czyż, S.H., Wójcik, A.M., Solarská, P. et al. High contextual interference improves retention in motor learning: systematic review and meta-analysis. Sci Rep 14, 15974 (2024). https://doi.org/10.1038/s41598-024-65753-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-65753-3
- Springer Nature Limited