
Abstract
Dry eye syndrome (DES) is a tear film disorder caused by increased tear evaporation or decreased production. The heavy workload on the eye and the increased usage of digital screens may decrease blink frequency, leading to an increased evaporation rate and an upsurge in the incidence and severity of DES. This study aims to assess the severity of DES symptoms and the risk factors among university students. A cross-sectional study was conducted at Umm AlQura University to evaluate the severity of DES among students and explore its potential association with digital screen use. Validated questionnaires were used to assess the severity of DES and digital screen usage. The study included 457 participants, of which 13% had symptoms suggestive of severe DES. Furthermore, multiple risk factors had a significant association with the severity of DES, including gender, use of monitor filters, monitor and room brightness, and smoking habits. DES symptoms were prevalent among university students, particularly female students. Although there was no significant association with the duration of screen usage and collage distribution. Other factors however, such as the usage of screen monitors and the brightness of both the monitor and the room, were significantly associated with the severity of DES symptoms.
Similar content being viewed by others


Introduction
Dry eye syndrome (DES) or dry eye disease (DED) is a tear film disorder caused by increased tear evaporation or decreased tear production1. DES is common in adults worldwide, affecting between 1 out of 5 to 1 out 11 individuals2,3. A study conducted among adults in Saudi Arabia, with the majority of participants being females, revealed that 38.4% of participants were diagnosed with DES. While another 36.8% experienced the same symptoms going undiagnosed. The high prevalence was attributed to environmental factors such as dry and hot weather in Saudi Arabia4.
A shift in learning methods characterizes the modern era; university students are extensively engaged with digital screens during online learning, leading to a substantial workload on their eyes. Excess use of digital screens, also called visual display terminals (VDT) can reduce blink frequency and facilitate tear evaporation, resulting in the development of DES5. Therefore, digital screening practices using laptops, tablets, television, and/or smartphones, should be investigated among university students, who are considered a high-risk group6,7.
Risk factors for DES include age, female gender, environmental factors such as air pollution, and digital screens1,3, have been identified in many previous studies. Although many studies have explored DES among university students, they yielded inconsistent results due to variations in geographical locations and methodologies. Therefore, we aim to assess the prevalence of DES symptoms among university students in our region and assess how different risk factors, mainly digital screen practices, can influence the severity of DES.
Methods
Study design
A cross-sectional study was conducted at Umm Alqura University (UQU) in Makkah, Saudi Arabia. Ethical approval was obtained from the Medical and Biological Ethics Research Committee of Umm Alqura University (No. HAPO-02-K-012-2023-12-1932), and all methods were performed in compliance with the relevant guidelines and regulations. We distributed an online questionnaire from May to June of 2023 among undergraduate students through the official university E-mail to four scientific and literary colleges using snowball sampling. Participants were informed that participation was voluntary. Visiting students from outside the university were excluded from the study.
Questionnaire methods
Informed consent was obtained from all participants before starting the questionnaire. A specific question to verify UQU enrolment was used for inclusion criteria. Demographic data such as age, gender, and college affiliation were included in the questionnaire.
The severity of dry eye syndrome was assessed using the Ocular Surface Disease Index (OSDI), a twelve-question questionnaire categorized into eye symptoms, vision function, and environmental factors. Responses were rated on a scale from 0 (none of the time) to 4 (all the time) over the previous week. The sum score from the answered question was multiplied by twenty-five, divided by the number of all questions answered. Accordingly, the final score ranged from 0 to 100, categorized as the following: 0–13 normal, 13–22 mild, 23–32 moderate, and > 32 severe8,9.
A validated questionnaire was used to investigate digital screen habits10, which incorporated eight questions related to screen usage. Participants were asked about potential risk factors related to dry eye, including the duration of using glasses and contact lenses, smoking habits, and virtual reality device use. Participants were also asked about using artificial tears and dark mode on electronic devices and if they considered consulting an ophthalmologist for their symptoms.
Sample size
To calculate the required sample size, we used OpenEpi version 3.0. The confidence interval is 95%, the frequency is 50%, and the design effect is 1. The total number of students at Umm Al-Qura University, based on the UQU official website, is 92,63411. The required sample size for this study is 383 participants. The number of participants based on the inclusion and exclusion criteria was 457.
Statistical analysis
Microsoft Excel and Statistical Package for Social Studies (SPSS 26) were used for the analysis. Frequencies were calculated for categorical variables. The Chi-square test compared categorical variables. The numerical data was normally distributed. Therefore, mean and standard deviation were used. Univariate analysis was done to find the association between the severity of dry eye syndrome and gender, college, usage of screens, and risk factors. A p-value < 0.05 was considered significant.
Results
The study includes 457 participants of both genders and various UQU colleges. The mean age was 22 years and two months, with a standard deviation of 2 years (Table 1). 48% (N = 221) of the participants did not complain of DES symptoms, whereas 52% (N = 236) experienced DES symptoms of varying severity (Fig. 1). Of note, 40.3% of participants reported their symptoms to a physician.

Prevalence and severity of dry eye syndrome.
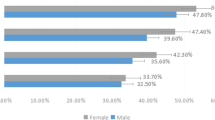
Tables 2 and 3 highlight factors associated with the severity of DES. Gender exhibited a significant association (p-value = < 0.001), with 60% of female participants exhibiting DES symptoms compared to 40% of males. Similarly, females tended to experience more severe DES symptoms than their male counterparts. Neither college affiliation demonstrated a significant difference in terms of DES prevalence nor screen usage factors including screen time duration, distance from the screen, seating position, screening breaking times and duration, awareness of the 20–20-20 rule, and usage of dark mode. However, other factors, such as the usage of monitor filters (p-value ≤ 0.001), screen brightness (p-value ≤ 0.001), and room brightness (p-value = 0.004), exhibited significant associations with DES symptom severity.
DES risk factors association with symptoms severity was evaluated and showed the following: usage of synthetic tears (p-value ≤ 0.001), wearing glasses (p-value ≤ 0.001), wearing contact lenses (p-value ≤ 0.001), smoking habits (p-value ≤ 0.001), and usage of virtual reality (VR) glasses (p-value ≤ 0.001), wearing glasses (p-value = 0.003) (Table 4).
Discussion
While several studies have explored DES symptoms among university students worldwide, there is a scarcity of research evaluating DES in Saudi Arabian universities and exploring its correlation with risk factors. This study found that more than half of the participants experienced dry eye symptoms with varying degrees of severity. In comparison, researchers in Thailand found that less than 1 out of 10 students have dry eye disease12. This considerable disparity in the prevalence of DES symptoms could be related to the influence of the local environment and climate. Thailand's tropical high-humidity climate differs significantly from the Middle East desert climate, and this divergence in climate and humidity may play a crucial role in maintaining ocular moisture and reducing tear evaporation. This conclusion is supported by a study conducted by Berg et al., indicating a strong correlation between humidity levels and the eye's dryness13.
The study result indicates a significant variation in the severity of DES based on gender, as females show more severe DES than males. This finding correlates with the results of three cross-sectional studies conducted in Al-Ahsa, Saudi Arabia14, The United Arab Emirates15, and the United States16, which demonstrate that female has more severe DES than males. Although the exact reason for this gender-related variation is not clear, it has been suggested that hormonal changes in females may contribute to this finding17.
Surprisingly, we did not find a significant correlation between the severity of DES and the duration of screen time. In contrast, several studies found a strong relationship between DES severity and digital screen use18. Another Saudi study has a similar result of increasing DES severity and long duration of using digital screens4. The discrepancy in results between this study and others may be attributed to students' young age or other confounders, for example, the use of protective tools from screen light like blue light filters. Blue light has been implicated in exacerbating dry eye symptoms by causing oxidative damage to the epithelium cells of the cornea and leading to the worsening of dry eye symptoms19.
In today's world, the daily use of digital devices and prolonged exposure to digital screen lights are inevitable. However, there are modifiable factors that can help reduce the prevalence and severity of DES. Screen brightness is one of the most important modifiable factors, as this study found a strong correlation between screen brightness and the severity of DES symptoms. This finding is substantiated by several published studies. For example, a cross-sectional study conducted in India suggests reducing the screen's brightness can be an effective method to lower the risk of developing dry eye20. Decreasing the screen's brightness will reduce the amount of light exposure to the eyes, which may decrease eye strain and tear evaporation. In addition, decreasing eye strain promotes regular frequency of eye blinking21.
The study's limitation is it did not include clinical assessments, such as visual acuity and the Schrimmer test. A notable strength of our study lies in using a validated instrument (OSDI) to assess the severity of DES. However, future research, including clinical assessment of eye dryness, is highly recommended to enhance diagnostic accuracy.
Conclusion
This study revealed a high prevalence of DES symptoms among university students, particularly female students, in Makkah, Saudi Arabia. Although there was no significant association with the duration of screen usage and collage distribution. Other factors however, such as the usage of screen monitors and the brightness of both the monitor and the room, were significantly associated with the severity of DES symptoms.
Data availability
All the data related to this study are available from the corresponding author upon reasonable request.
References
Stapleton, F. et al. TFOS DEWS II epidemiology report. Ocul. Surf. 15(3), 334–365 (2017).
Papas, E. B. The global prevalence of dry eye disease: A Bayesian view. Ophthalmic Physiol. Opt. 41(6), 1254–1266 (2021).
Qian, L. & Wei, W. Identified risk factors for dry eye syndrome: A systematic review and meta-analysis. PLoS One. 17(8), e0271267 (2022).
Helayel, H. et al. Prevalence and risk factors of dry eye disease among adults in Saudi Arabia. Saudi J. Med. Med. Sci. 11(3), 242 (2023).
Uchino, M. et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: the Osaka study. Am. J. Ophthalmol. 156, 759–766. https://doi.org/10.1016/j.ajo.2013.05.040 (2013).
Kawashima, M. et al. Association of systemic comorbidities with dry eye disease. J. Clin. Med. 9(7), 1–12 (2020).
Cartes, C. et al. Dry eye and visual display terminal-related symptoms among university students during the coronavirus disease pandemic. Ophthalmic Epidemiol. 29(3), 245–251. https://doi.org/10.1080/09286586.2021.1943457 (2022).
Pastor-zaplana, J. Á., Borrás, F., Gallar, J. & Acosta, M. C. OSDI questions on daily life activities allow to detect subclinical dry eye in young contact lens users. J. Clin. Med. 11(9), 2626 (2022).
Schiffman, R. M., Christianson, M. D., Jacobsen, G., Hirsch, J. D. & Reis, B. L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 118(5), 615–621 (2000).
Al Tawil, L. et al. Prevalence of self-reported computer vision syndrome symptoms and its associated factors among university students. Eur. J. Ophthalmol. 30(1), 189–195 (2020).
UQU Statistics | Umm Al-Qura University [Internet]. [cited 2023 Nov 3]. https://uqu.edu.sa/en/main/1072.
Supiyaphun, C., Jongkhajornpong, P., Rattanasiri, S. & Lekhanont, K. Prevalence and risk factors of dry eye disease among University Students in Bangkok, Thailand. PLoS One 16(10), e0258217 (2021).
Berg, E. J. et al. Climatic and environmental correlates of dry eye disease severity: A report from the Dry Eye Assessment and Management (DREAM) study. Transl. Vis. Sci. Technol. 9(5), 1–11 (2020).
Alshamrani, A. A. et al. Prevalence and risk factors of dry eye symptoms in a Saudi Arabian population. Middle East Afr. J. Ophthalmol. 24(2), 67 (2017).
Alkabbani, S., Jeyaseelan, L., Rao, A. P., Thakur, S. P. & Warhekar, P. T. The prevalence, severity, and risk factors for dry eye disease in Dubai—A cross sectional study. BMC Ophthalmol. 21(1), 1–7 (2021).
Schaumberg, D. A., Sullivan, D. A., Buring, J. E. & Dana, M. R. Prevalence of dry eye syndrome among US women. Am. J. Ophthalmol. 136(2), 318–326 (2003).
Borrelli, M., Frings, A., Geerling, G. & Finis, D. Gender-specific differences in signs and symptoms of dry eye disease. Curr. Eye Res. 46(3), 294–301 (2021).
Al-Mohtaseb, Z., Schachter, S., Lee, B. S., Garlich, J. & Trattler, W. The relationship between dry eye disease and digital screen use. Clin. Ophthalmol. 15, 3811–3820 (2021).
Yadav, P., Yadav, A. & Verma, M. A study on the effect and prevention of blue light on eyes. Int. J. Res. Appl. Sci. Eng. Technol. 11(3), 7–12 (2023).
Mufti, M., Imran Sayeed, S., Jaan, I. & Nazir, S. Does digital screen exposure cause dry eye?. Indian J. Clin. Anat. Physiol. 6(1), 68–72 (2019).
Mehra, D. & Galor, A. Digital screen use and dry eye: A review. Asia Pac. J. Ophthalmol. (Phila) 9(6), 491–497 (2020).
Author information
Authors and Affiliations
Contributions
A.Alqurashi, H. Almaghrabi and M. Alahmadi Conception and design the methodology. A. Alotaibi and A. Jastaniah the study figure and tables. A. Bukhari and M. Binhussein statistical analysis and interpretation of results. B. Othman and A. Khojah critical revisions and supervision. All authors participated in writing the study manuscript and reviewed the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alqurashi, A., Almaghrabi, H., Alahmadi, M. et al. The severity of dry eye symptoms and risk factors among university students in Saudi Arabia: a cross-sectional study. Sci Rep 14, 15149 (2024). https://doi.org/10.1038/s41598-024-65297-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-65297-6
- Springer Nature Limited