
Abstract
Experiences in early childhood form the bedrock of future human potential. In impoverished settings, structured early childhood education (ECE) in preschool years can augment overall childhood and later human abilities. The current study evaluates preschool learning exposure and childhood cognition, using longitudinal follow-up of a community-based birth cohort in Vellore, south India. The birth cohort study site in Vellore recruited 251 newborns between 2010 and 2012 from dense urban settlements and further followed up into childhood. Preschool enrolment details were obtained from parents. Childhood cognition was assessed by Weschler’s preschool primary scale of intelligence (WPPSI) and Malin’s intelligence scale for Indian Children (MISIC) at 5 and 9 years of age respectively. Bivariate and multivariate regression analyses were performed with adjustments for socio-economic status (SES), maternal education, stunting status and home environment. Out of 251 new-borns recruited into the MAL-ED birth cohort, 212 (84.46%) and 205 (81.7%) children were available for the 5 year and 9 year follow-up respectively. At 5 years, structured ECE of 18 to 24 months duration was significantly associated with higher cognition scores, with the highest increase in processing speed [β: 19.55 (11.26–27.77)], followed by full-scale intelligence [β: 6.75 (2.96–10.550)], even after adjustments for SES, maternal cognition, home factors and early childhood stunting status. Similarly adjusted analysis at 9 years showed that children who attended 1.5–2 years of structured ECE persisted to have higher cognition, especially in the performance domain [β: 8.82 (2.60–15.03)], followed by the full-scale intelligence [β: 7.24 (2.52–11.90)]. Follow-up of an Indian birth cohort showed that structured ECE exposure was associated with better school entry cognition as well as mid-childhood cognition. Strengthening ECE through a multi-pronged approach could facilitate to maximize cognitive potential of human capital.
Similar content being viewed by others

Introduction
Cognition or intelligence can be defined as a ‘combination of multiple abilities in a child’ as proposed by Howard Gardner1. The first 1000 days of life starting from the antenatal period in the mother’s womb, to the perinatal period and the first 2 years of life, is crucial for child’s cognitive development, as maximum brain development and maturation happen during this period2. Factors such as early childhood malnutrition, infections, perinatal asphyxia, iron deficiency, lead toxicity and poverty are detrimental for cognitive development in children3,4,5. Children from poorer households are more likely to experience unsupportive parenting, lack of caregiver education, more stressful events, lack of stimulating environment including play materials and poor education, which in turn result in poor cognitive development and scholastic performance. This compromise in education and subsequent earning capacity in these children further produces an inter-generational transmission of poverty2. On the other hand, positive and stimulating environment prevailing at home and appropriate learning opportunities during preschool years can augment a child’s developmental and cognitive abilities6.
Global evidence suggests that early childhood education (ECE) offered at a better quality can positively impact a child’s intellectual, social and emotional development, and continued learning in future7,8. In a Brazilian cohort, children who received structured ECE, compared to those who did not, had higher cognition scores by 8 units at 5 years of age, after adjusting for home environment and socioeconomic status6. Similarly, ECE programmes in low-and-middle income country (LMIC) settings such as in Bangladesh have promoted academic achievements in mathematics, writing and reading domains for children in their primary grades9. In a preschool environment, in addition to direct learning opportunities in a structured manner, children can also have peer social interactions which can aid their indirect learning experiences. Thus, a centre-based education for pre-schoolers can help to attain better motor coordination, arithmetic skills, memory and concentration in children and may override many adverse childhood experiences6,10,11.
In India, the National Early Childhood Care and Education (ECCE) policy recommends that children between 3 and 6 years receive early education and care from Anganwadi centres, which are community-based12,13,14. Multi-age grouping is followed in which students of different ages and identified age levels are grouped in a single classroom to provide effective instruction. The medium of interaction in the ECCE centre should be the home language or mother tongue. In the early years, the focus would be on listening and speaking activities, facilitated through free play with peers. In the region where the study was done, the ECCE Programme in Tamil language was conducted 5 days a week and for a minimum of 4 h duration,
The ECE programs typically aim to enhance intellectual and social abilities of children which can form a fulcrum for their subsequent learning development. They had considerable positive short-term effects and somewhat smaller long-term effects on cognitive development more so for children from socio-economically disadvantaged families. Studies have shown that sustained high-quality early care and education can mitigate the consequences of poverty into adulthood15,16. Nevertheless, some studies and an international review highlight sub-optimal evidence of long-term effects of ECE17. Possible reasons for even a school-level ‘fade-out’ of ECE could be the quality of ECE, the absence of sustaining environments later and differing skillsets for learning in different age groups18. Another commonly cited explanation of the ‘fade-out’ effect of ECE programs on early academic skills is that it changes with time, and the gains often disappear after children transition to elementary school15,18. Thus, it is important to understand if structured ECE interventions have a long-term effect on cognition in the later childhood period, as this could help policymakers assess cost–benefit aspects better. In this context, the current study evaluates the association between structured ECE and cognition at 5 and 9 years of age in a birth cohort in Vellore, India. For this study, structured ECE was defined as specific structured language and learning inputs from early childhood curriculum and was provided in this area by both private and government aided schools in preschool settings. It is hypothesised that structured ECE will have a positive association with both 5- and 9 year cognition.
Methods
This paper presents the analysis of a birth cohort follow-up, as part of a multi-country cohort study done in eight LMICs evaluating the role of enteric infections in early life on growth and development in children (‘The Etiology, Risk Factors and Interactions of Enteric Infections and Malnutrition and the Consequences for Child Health and Development (MAL-ED) Network Cohort)19. The study site in Vellore, India recruited 251 newborns between 2010 and 2012 from dense urban slum settlements following parental consent20. Children were intensively followed up through home visits till two years of age to capture information on sociodemographic details, morbidity status, anthropometry, and dietary intake, with subsequent follow-up visits made at 3, 4, 5, 7 and 9 years of age. This study was approved by the Institutional Review Board, Christian Medical College, Vellore for initial recruitment as well as follow-up visits (IRB 6769 for the original cohort and follow-up, IRB 11821 for the 9 year follow-up) and was conducted following the guidelines laid by World Medical Association Declaration of Helsinki. Before each recruitment, we obtained parental informed consent in written format and for the 9-year follow-up, additional child assent.
Exposure variables
To evaluate child’s stunting status, trained Field research assistants (FRA) carried out standardized anthropometry measures using an infantometer for recording the length up to 2 years, and a stadiometer thereafter, till 9 years of age to the nearest cm. Z scores for length/height measurements were calculated based on Multicentre Growth Reference Study standards and children were classified as stunted at each time point if Z scores were below − 2 SD. Maternal intelligence quotient (IQ) raw scores were assessed using Raven’s Progressive Matrices by a single, trained psychologist. The Home Observation for the Measurement of the Environment (HOME) scale was administered by a trained social worker at 2 years to measure overall support received by the child at home from caregivers. At 5 years, caregivers were contacted for information about the number of months of structured ECE received by their children. The socioeconomic status (SES) assessment was based on the Water and Sanitation, Assets, Maternal education, and Income (WAMI) scores.
Outcome measures
A single, trained psychologist conducted cognition evaluation for children in the community study clinic using Weschler’s Preschool Primary Scale of Intelligence (WPPSI) and Malin’s intelligence scale for Indian children (MISIC) at 5 and 9 years respectively3,21. The WPPSI scale was translated, and pilot-tested in local settings to assess cognition under verbal, performance, and processing speed domains. The MISIC scale which was adapted for use in the Indian setting from the original Wechsler scale, evaluated cognition under verbal and performance domains. Raw scores obtained by children under each domain were converted into IQ scores for analysis.
Statistical analysis
Data was collected in paper forms and entered in the double-entry database system maintained by the central Data coordination centre of the MAL-ED study for the initial part of the birth cohort study. Descriptive statistics were used to summarize sex, SES and early childhood stunting status in percentages. Children living in households with WAMI scores ≥ 33rd percentile were classified as those belonging to relatively high SES. Stunting status of children at 2 and 5 years was used to group children into those who were never stunted, stunted at 2 years but recovered by 5 years, and, persistently stunted at 2 and 5 years. Based on tertile scores of structured ECE attendance expressed in months, children were classified into three groups. Children in group 1 had no exposure to structured ECE, whereas those in groups 2 and 3 attended 1–17 and 18–24 months, respectively in a structured preschool. HOME scores were summarized as median and interquartile (IQR) scores. Child’s IQ scores under each domain were presented as median (IQR) and box plots were used to visualize relationship between IQ scores, and groups based on preschool and structured preschool attendance. Correlation co-efficients were computed to check for correlation between domain scores of cognition measures at 5 and 9 years. To measure the association between structured ECE and IQ scores, bivariate and multivariate regression analyses were performed. The normality of dependent variables was assessed using the Shapiro–Wilk test. Linear regression was performed only for performance IQ (PIQ) at 5 years, while quantile regression was used to fit other domain scores such as verbal IQ (VIQ), processing speed IQ (PSIQ) and full-scale IQ (FSIQ) since normality assumptions for linear regression analysis were not met. Similarly, the predictor model for VIQ at 9 years was based on linear regression, while PIQ and total IQ scores at 9 years were modelled using quantile regression. Multivariable models included independent variables that were statistically significant in bivariate analysis at p < 0.05, and collinearity between the variables was analysed using correlation statistics. R2 values and the Hosmer–Lemeshow goodness-of-fit test were considered for assessing model fitness in the case of linear regression models. Beta coefficients along with 95% confidence intervals (CI) were reported and a p-value less than 0.05 was considered as statistical significance. Statistical analysis was performed using STATA version 14 (Stata Statistical Software: Release 14, StataCorp LP, College Station, TX).
Ethics approval
This study was approved by the Institutional Review Board, Christian Medical College, Vellore for initial recruitment as well as follow-up visits (IRB 6769 for the original cohort and follow-up; IRB 11821 for the 9 year follow-up). Participants were enrolled after due written informed consent before inclusion in the study. This research was conducted ethically following the World Medical Association Declaration of Helsinki.
Results
A cohort of 251 newborns were recruited as part of the Vellore cohort of MAL-ED by screening 301 pregnant women from the study area between 2010 and 2012. At recruitment, a female preponderance (55%) was observed in the cohort. About 212 (84.46%) and 205 (81.67%) children were available for follow-up at 5 and 9 years21 and the most common reason for non-participation was migration of the family outside study area. The 5-year recruitment was conducted between 2015 February and 2017 February. The 9 year recruitment was planned between 2019 February and 2021 February. There was a disruption in recruitment for 6–7 months in 2020 due to the Covid-19 pandemic. We completed cognitive and other clinic-based assessments for all children by April 2021.
There was no significant difference in cohort characteristics such as sex and socioeconomic status between the follow-up time points (Table 1). Of 212 children followed up at 5 years, 41 (19.34%) were stunted at two years but recovered by 5 years, whereas 58 (27.36%) children were found to be stunted both at two and five years. Proportion of children who attended structured ECE was 54.25% with median months of attendance 8 months.
Median (IQR) WPPSI IQ scores measured at 5 years under verbal, performance, processing speed and full-scale domain were 81 (77–85), 84 (79–90), 103 (88–113) and 84 (79–89) respectively (Fig. 1). Bivariate analysis of cognition scores across tertile categories of structured ECE showed that children belonging to the highest tertile (18–24 months of attendance) had significantly higher IQ scores by 3, 6.15, 16 and 7 units in VIQ, PIQ, PSIQ and FSIQ domains respectively at 5 years, compared to those in the lowest tertile (nil attendance to structured preschool) (Table 2). Further, multivariate analysis accounting for maternal cognition, HOME scores, SES and early life stunting status showed that structured ECE between 18 and 24 months (highest tertile) was significantly associated with higher cognition scores in children at 5 years, with highest increase in PSIQ domain [β: 19.55 (11.26–27.77)], followed by FSIQ [β: 6.75 (2.96–10.55)], PIQ [β: 5.54 (2.11–8.98)] and VIQ domains [β: 3.32 (0.74–5.91)], compared to those who did not attend structured ECE (lowest tertile). It is notable that children in the second tertile of structured ECE with a median duration of 1–17 months also had higher PIQ and PSIQ in the bivariate analysis compared to those in the lowest tertile (nil attendance), however, this association was not found to be statistically significant in the multivariate analysis (Table 3). A sensitivity analysis was conducted categorizing the duration of structured ECE under two different scenarios to support the main analysis based on tertile categorization of ECE exposure. In the first scenario, structured ECE duration was categorized year-wise as per the existing education curriculum in India into ‘no attendance’, ‘1–12 months’ and ‘13–24 months’. Children exposed to 13–24 months of ECE had a significant increase in FSIQ by 4.8 compared to those who did not attend structured ECE [β: 4.82 (2.1–7.5)] in multivariate analysis. In the second scenario, structured ECE duration was divided as quartiles into ‘no attendance’, ‘1–8 months’, ‘8–18 months’ and ‘ > 18 months’ of exposure and included in multivariate analysis. Compared to children who did not have structured ECE, those exposed to ‘8–18 months’ and ‘ > 18 months’ had a significant increase in FSIQ scores by 3.4 [β: 3.4 (0.5–6.3)] and 6.4 [β: 6.4 (3.2–9.6)], respectively (data not shown).

Comparison of cognition scores across tertile groups based on ECE attendance in the MAL-ED cohort.
Median (IQR) cognition scores measured at 9 years under verbal, performance, and total IQ scores were 94.4 (87.2–100.6), 91.6 (82.9–101.2) and 93.4 (85.5–100.2) respectively. Correlation coefficients between verbal IQ, performance IQ and total scores IQ at 5 and 9 years were 0.6, 0.6 and 0.7 respectively (data not shown). Exposure to structured ECE showed a positive association with VIQ, PIQ and total IQ scores at 9 years. In bivariate analysis, children in the highest tertile category (18–24 months) of structured preschool attendance showed about 7–10 points increase in IQ scores across various domains of cognition, with effect size being highest in the PIQ domain compared to those who did not attend structured preschool (Table 4). This association remained significant in the multivariate model, with children in the highest tertile category scoring higher IQ scores than those in the lowest tertile, after adjusting for maternal IQ, SES and early-life stunting. Structured preschool exposure for about 18–24 months had the greatest impact on PIQ domain with a higher effect size [β: 8.82 (2.60–15.03)], followed by total IQ [β: 7.24 (2.52–11.90)] and verbal IQ domains [β: 5.25 (1.88–8.62)], compared to those without structured preschool attendance (Table 5). Similar to 5 years analysis, a sensitivity analysis was conducted categorizing the duration of structured ECE under two different scenarios. In the first scenario, where structured ECE duration was categorized year-wise into ‘no attendance’, ‘1–12 months’ and ‘13–24 months’, children exposed to 13–24 months of ECE had an increase in FSIQ by 4.5 compared to those who did not attend structured ECE [β: 4.5 (0.3–8.6)] in multivariate analysis. In the second scenario, where structured ECE duration was divided into quartiles, it was observed that children with structured ECE of ‘ > 18–24 months’ had a significant increase in FSIQ scores by 7.7 compared to those who did not have any exposure to ECE [β: 7.8 (3.0–12.4)] (data not shown).
Discussion
This prospective follow-up study done among children living in an urban Indian slum setting evaluated the association between structured ECE and cognition scores at 5 and 9 years of life. Attending structured ECE was associated with higher cognition scores by 3–19 points at 5 years, with the highest increase seen in the processing speed domain of cognition, despite corrections with maternal cognition, SES, home factors, and early childhood stunting, compared to those who did not attend. This association between structured ECE and cognition remained significant even in later childhood, where an increase in IQ scores by 5–9 points at 9 years was observed after correcting for SES, maternal cognition, home factors, and childhood stunting status.
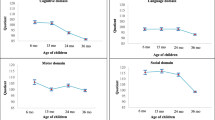
Global evidence states that early childhood adversities, particularly, poor home environment negatively impact cognitive abilities during childhood and continue to impact even in adult life22. In the current birth cohort studied in Vellore, a nurturing home environment in early childhood increased developmental cognition scores, while responsive caregiving resulted in augmented language development as evidenced by a previous publication from the same cohort23. It should also be highlighted that developmental trend analysis of this LMIC birth cohort showed a decline in overall developmental scores including that of cognition and language between 6 and 36 months of age, owing to SES, home environments, childhood stunting and low blood iron status23. A similar association was reported from a Brazilian cohort where children from healthier home environments had better cognition scores by 5 points in the fifth year of follow-up6.
The negative impacts that early childhood adversities have on cognition can be mitigated by appropriate psychosocial stimulation as reported in the same Brazilian cohort, where children attending nursery classes had higher cognition scores by 8 points at follow-up6. The present study concurs with this finding where structured ECE was associated with higher full-scale IQ scores by 7 units at 5 years. Another important finding of this study is the sustenance of this positive impact on cognition even at 9 years of age. This finding is in line with a Uruguay study which showed that preschool education had a positive impact on academic achievements both at the time of entering primary school and six years later24. Similar persisting effects of good quality ECE were reported from Abecedarian low-income cohort and the ‘1991 NICHD study of early childcare and youth development’, where ECE was associated with significant life success benefits as evidenced by additional years of education, better employment and vocational opportunities, and better wages15,16.
Preschool years represent a crucial period for the development of cognitive, linguistic, social, and psychomotor competencies in children. Early childhood care and education help to overcome environmental adversities due to impoverishment since the plasticity of the developing brain allows the reorganisation of brain circuits in response to psychosocial stimulation8,25. Another plausibility for the impact of centre-based early childhood interventions on academic achievements in later life would be based on the ‘cognitive advantage hypothesis’ where children from impoverished settings were able to capitalize the cognitive gains acquired due to interventions into academic achievements later in their life15. Aptly, the 75th World Health Assembly included opportunities for early learning in the Nurturing Care Framework to optimise early child development26. The current paper adds further evidence to this in terms of the need for a structured learning opportunity in early childhood.
In line with WHO and UNESCO’s recommendation of strengthening ECE as a cost-effective strategy for a country to make sustainable progress, the preschool education programme under the Integrated Child Development Services (ICDS) scheme has percolated in length and breadth of the country reaching out to tens of millions of children in India8,27,28,29,30.A co-prioritisation of preschool education, along with nutritional rehabilitation, has been highlighted by recent government initiatives and is in the right direction. A study from Maharashtra during 2004–05, introduced an ECE package in Anganwadis which included refresher training sessions to Anganwadi worker and financial support to purchase play materials. This intervention was found helpful in increasing IQ scores by 10 points in children compared to controls and is in concurrence with our findings31. Recent evidence from Tamil Nadu demonstrated the effectiveness of introducing an extra worker exclusively concentrating on ECE within the existing Anganwadi system, which resulted in exclusive ECE opportunities and an increase in cognition scores in mathematics, language and executive domains was noted in these children at 18 months, post-intervention12. Different methods to provide structured educational inputs in early childhood along with nutritional measures within the ICDS system can be explored by further studies in other Indian states to aid policy decisions for the country.
Genetic influences of cognitive abilities cannot be overlooked. In our current analysis as well as published literature from the same cohort, maternal cognitive capacity was shown to have a significant association not only with child development, and cognitive abilities but also with early childhood home environment3,21,23,25. Our analyses in the present study were corrected for maternal cognition recognising this genetic leverage.
There are many limitations to the current analysis. The cohort had a comparatively small sample size. We should also keep in mind that the Wechsler scale used at 5 years of age was not completely adapted for Indian settings. Both cognitive assessment measures used in the current analysis evaluate logical intelligence, but not other components of intelligence including but not limited to emotional intelligence, visuospatial intelligence, musical intelligence, etc. Quality of preschool and primary school education variables were not available for consideration in this study as well. Strengths of the study include minimal loss to follow-up, availability of good quality of early childhood data and India-specific cognitive analysis at 9 years of age.
Conclusions
This cohort study done in an impoverished urban Indian setting has brought out the positive association of attending structured ECE on school entry cognition at 5 years and mid-childhood cognition at 9 years of life. Strengthening ECE through a multi-pronged approach of structured preschool curriculum, provision of adequate play materials, providing trained manpower and enabling centres with information and communication tools could facilitate to maximize the cognitive potential of human capital in India.
Data availability
MAL-ED dataset till 5 years of age is uploaded on www.clinepidb.org. Further dataset can be shared by the Corresponding Author, on reasonable request.
References
Gardner, H. The Theory of Multiple Intelligence (10th Anniversary Edition) (Basic Books, 1993).
Biesalski, H. K. The 1000-day window and cognitive development. In World Review of Nutrition and Dietetics (eds Biesalski, H. K. & Black, R. E.) 1–15 (S. Karger AG, 2016).
Koshy, B. et al. Body iron and lead status in early childhood and its effects on development and cognition: A longitudinal study from urban Vellore. Public Health Nutr. 23, 1896–1906 (2020).
MAL-ED Network Investigators. Early childhood cognitive development is affected by interactions among illness, diet, enteropathogens and the home environment: Findings from the MAL-ED birth cohort study. BMJ Glob. Health https://doi.org/10.1136/bmjgh-2018-000752 (2018).
McCormick, B. J. J. et al. Early life experiences and trajectories of cognitive development. Pediatrics 146, e20193660 (2020).
Santos, D. N. et al. Determinants of cognitive function in childhood: A cohort study in a middle income context. BMC Public Health 8, 202 (2008).
Kim, J. H. Preschool participation and students’ learning outcomes in primary school: Evidence from national reform of pre-primary education in Ethiopia. Int. J. Educ. Dev. 94, 102659 (2022).
United Nations Educational, Scientific and Cultural Organisation. The Contribution of Early Childhood Education to a Sustainable Society (UNESCO, 2008).
Aboud, F. E. & Hossain, K. The impact of preprimary school on primary school achievement in Bangladesh. Early Child. Res. Q. 26, 237–246 (2011).
Bulgarelli, D. & Molina, P. Social cognition in preschoolers: Effects of early experience and individual differences. Front. Psychol. https://doi.org/10.3389/fpsyg.2016.01762 (2016).
Stich, H. L., Baune, B. T., Caniato, R. N. & Krämer, A. Associations between preschool attendance and developmental impairments in pre-school children in a six-year retrospective survey. BMC Public Health. 6, 260 (2006).
Ganimian AJ, Muralidharan K, Walters CR. Augmenting state capacity for child development: experimental evidence from India. National Bureau of Economic Research. https://www.nber.org/papers/w28780 (Accessed 23 March 2023) (2021).
Ministry of Women and Child Development. National early Childhood Care and Education (ECCE) Curriculum Framework. New Delhi: MOWCD. Available from: Microsoft Word - 2. National ECCE Curr Framework final .doc (wcd.nic.in) (Accessed 23 March 2023).
Ministry of Women and Child Development. Guidelines for Mission Saksham Anganwadi and Poshan 2.0. New Delhi: MOWCD. Available from: Final Saksham Guidelines with covering letter (1).pdf (wcd.nic.in) (Accessed 23 March 2023) (2022).
Campbell, F. A. et al. Young adult outcomes of the Abecedarian and CARE early childhood educational interventions. Early Child. Res. Q. 23, 452–466 (2008).
Bustamante, A. S., Dearing, E., Zachrisson, H. D. & Vandell, D. L. Adult outcomes of sustained high-quality early child care and education: Do they vary by family income?. Child. Dev. 93(2), 502–523 (2022).
Burger, K. How does early childhood care and education affect cognitive development? An international review of the effects of early interventions for children from different social backgrounds. Early Child. Res. Q. 25, 140–165 (2010).
Burchinal, M. et al. Examining three hypotheses for pre-kindergarten fade-out. Dev. Psychol. 58(3), 453–469 (2022).
MAL-ED Network Investigators. The MAL-ED study: A multinational and multidisciplinary approach to understand the relationship between enteric pathogens, malnutrition, gut physiology, physical growth, cognitive development, and immune responses in infants and children up to 2 years of age in resource-poor environments. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 59(Suppl 4), S193-206 (2014).
John, S. M. et al. Establishment of the MAL-ED birth cohort study site in Vellore, Southern India. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 59(Suppl 4), S295-299 (2014).
Koshy, B. et al. Are early childhood stunting and catch-up growth associated with school age cognition? - Evidence from an Indian birth cohort. PLoS One 17, e0264010 (2022).
Richards, M. & Wadsworth, M. E. J. Long term effects of early adversity on cognitive function. Arch. Dis. Child. 89, 922–927 (2004).
Koshy, B. et al. Developmental trends in early childhood and their predictors from an Indian birth cohort. BMC Public Health 21, 1083 (2021).
Aguilar, R. & Tansini, R. Joint analysis of preschool attendance and school performance in the short and long-run. Int. J. Educ. Dev. 32, 224–231 (2012).
Koshy, B. et al. Home environment:Short term trends and predictors in early childhood from an Indian community birth cohort. Child Care Health Dev. 47(3), 336–348 (2021).
World Health Organization. Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential (WHO, 2018).
Jain, A. et al. Anganwadi worker time use in Madhya Pradesh, India: A cross-sectional study. BMC Health Serv. Res. 20, 1130 (2020).
Lall, G., Roy, R., Chandrika, K. S. & Divan, G. “The early years are like a foundation for the future” Perspectives, facilitators and challenges of Anganwadi Workers’ in supporting early child development interventions in Hyderabad, India: Qualitative findings from A Scalable Programme Incorporating Early Child Development Interventions (ASPIRE). MedRxiv https://doi.org/10.1101/2023.01.11.23284414v1 (2023).
Ministry of Women and Child Development. Pre-School Education Kit (PSE KIT). New Delhi: MOWCD. https://wcd.nic.in/sites/default/files/Pre-School/20Education/20Kit.pdf (Accessed 23 March 2023) (2017).
National Council of Educational Research and Training. The Preschool curriculum. New Delhi:NCERT. https://ncert.nic.in/dee/pdf/Combined_Pre_school_curriculumEng.pdf (Accessed 23 March 2023) (2019).
Ade, A., Gupta, S. S., Maliye, C., Deshmukh, P. R. & Garg, B. S. Effect of improvement of pre-school education through Anganwadi center on intelligence and development quotient of children. Indian J. Pediatr. 77, 541–546 (2010).
Acknowledgements
Authors thank children, their families and staff of the MAL-ED Network project.
Funding
The Etiology, Risk Factors and Interactions of Enteric Infections and Malnutrition and the Consequence for Child Health and Development Project (MAL-ED) was a collaborative project supported by the Bill and Melinda Gates Foundation (BMGF), the Foundation for the NIH and the National Institutes of Health/Fogarty International Center (Grant number – OPP 47075). The 9 year follow-up of this Mal-ed India cohort was supported by an Intermediate clinical and public health (CPH) research fellowship awarded by the DBT-Wellcome Trust India Alliance to BK. (Fellowship grant number IA/CPHI/19/1/504611). Sponsors/Funders had no role in the study design, data collection and analysis, decision to publish or preparation of manuscript.
Author information
Authors and Affiliations
Contributions
Beena Koshy, Manikandan Srinivasan, Rangan Srinivasaraghavan, Venkata Raghava Mohan and Gagandeep Kang contributed to the study conception and design. Material preparation, data collection and analysis were performed by Beena Koshy, Manikandan Srinivasan, Reeba Roshan, Venkata Raghava Mohan, Sushil John and Karthikeyan Ramanujam. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koshy, B., Srinivasan, M., Srinivasaraghavan, R. et al. Structured early childhood education exposure and childhood cognition – Evidence from an Indian birth cohort. Sci Rep 14, 12951 (2024). https://doi.org/10.1038/s41598-024-63861-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-63861-8
- Springer Nature Limited