
Abstract
Accumulating evidence from observational studies have suggested an association between gastroesophageal reflux disease (GERD) and non-alcoholic fatty liver disease (NAFLD). However, due to that such studies are prone to biases, we imported Mendelian randomization (MR) to explore whether the causal association between two diseases exsit. Hence, we aimed to analysis the potential association with MR. The single nucleotide polymorphisms (SNPs) of GERD were retrieved from the genome-wide association study dataset as the exposure. The SNPs of NAFLD were taken from the FinnGen dataset as the outcome. The relationship was analyzed with the assistance of inverse variance weighted, MR-Egger, and weighted median. We also uitilized the MR-Egger intercept, Cochran’s Q test, leave-one-out analysis, MR-PRESSO, and Steiger directionality test to evaluate the robustness of the causal association. The meta-analysis were also implemented to give an overall evaluation. Finally, our analysis showed a causal relationship between GERD and NAFLD with aid of MR and meta-analysis (OR 1.71 95% CI 1.40–2.09; P < 0.0001).
Similar content being viewed by others


Introduction
Gastroesophageal reflux disease (GERD) is regarded as one of the most common gastrointestinal (GI) diseases at present, characterized by the backflow of acid into the esophagus which can cuase heartburn and regurgitation and futher impair the quality of patients’ life1,2. Medication with proton pump inhibitors (PPIs) is the routine therapy, which, however, can only alleviate the manifestation of GERD instead of eradicating the disease3. GERD is a common disease around the world, and the evidence shows the incidence is still increasing, especially in America and Asia, with the incidence being up to about 23% in North America and 11.7% in Asia4,5.
Non-alcoholic fatty liver disease (NAFLD) refers to a condition distinguished by the accumulation of fat in the liver that is not related to inordinate alcohol consumption and any specific etiological liver diseases, which is the principle cause of chronic hepatic diseases and poses a huge burdern on the national health and economy. The diagnosis of NAFLD is not clear, but liver biopsy can be extremely helpful6. NAFLD is often seen as the precursor of the metabolic syndrome. The most frequent risk factors of NAFLD involve obesity, hypertension, type II diabetes mellitus (T2DM), dietary habits, physical activity, and socioeconomic factors7,8.
A lot of cohort and observational studies have displayed that people suffering from NAFLD had a higher susceptibility to GERD, and one clinical trial indicated that the risk of reflux esophagitis would increase 16% among people with NAFLD (OR 1.16 95% CI 1.13–1.20) as compared to those without NAFLD9,10,11,12. In addition, a meta-analysis showed that the incidence of NAFLD was higher in people with GERD compared with healthy individuals, with an amalgamated OR of 2.07 (OR 2.07 95% CI, 1.54–2.79)13. However, the evidence for these associations was inconsistent, a cohort study found no clear significance between two diseases14. Another study suggested that GERD is the consequence, but not the cause of NAFLD15. Nonetheless, there is a paucity of studies investigating the causation between GERD and NAFLD.
Routine observational studies are prone to biases, such as reverse causality and residual confounding, owing to that conventionally measured exposures are often disturbed by a variety of behavioral and physiological factors16. Mendelian randomization (MR), a statistical approach to explore the causation between the exposure and the outcome, utilizes genetic variants as instrumental variables (IVs) to make causal inferences about the effect of an exposure on an outcome. MR takes advantage of randomization to avoid confounding errors due to the genetic variants are randomly assigned and are not influenced by confounding factors16,17,18. In addition, it is clear that the direction of causality is from the genetic polymorphism to the outcome in the MR analysis. Furthermore, a meta-analysis is a statistical method that combines the results of different studies about the same topic, which somewhat can solve conflicts. The major advantage relies on its ability of offering a precise and overall result as well as assessing potential sources of heterogeneity19. Therefore, we aimed to employ the MR and meta-analysis to elucidate whether there was a causal association between GERD and NAFLD, and if so, to estimate the magnitude of the causal effect.
Materials and methods
Data sources and selection of instrumental variables
The genome-wide association study (GWAS) dataset and the FinnGen dataset were used to perform the MR analysis. To sum up recent available data, We searched the GWAS data of gastroesophageal reflux disease (GERD) from the GWAS (https://www.ebi.ac.uk/) and FinnGen database (https://www.finngen.fi/en)20,21,22 and finally got a total of 10 groups of data for next analysis.
(Supplemental Table 1). The data of NAFLD were gained from FinnGen database which included 2275 cases and 375,002 controls, and we retrieved 20,170,233 SNPs from it. All datasets are obtained from European to avoid the potential deviation due to population stratification.
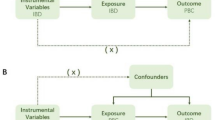
Mendelian randomization analysis requires IVs to meet three significant assumptions: (i) the IVs are strongly related to exposure (relevance); (ii) the IVs are independent of outcome (independence); (iii) the IVs have nothing to do with confounders (exclusion restriction)18,19,23 (Fig. 1). First, we selected single nucleotide polymorphisms (SNPs) of GERD that met the standard of genome-wide significance (P < 5 × 10–8). The F-statistic is calculated and F > 10 is required to ensure the strength of the relationship between IVs and phenotype (exposure)24. Besides, SNPs that may have linkage disequilibrium (LD) were removed (R2 > 0.001) due to consideration of the violation for the independence of genetic variants25,26. In addition, we also eliminated genetic variants of palindromic and incompatible alleles in the process of harmonizing exposure and outcome. By the search of GWAS database (http://www.phenoscanner.medschl.cam.ac.uk), we aimed to run out on the confounder-associated SNPs according to assumption (iii) with a threshold of P < 1 × 10–6.

Graphical dipiction of the study design and MR assumptions in a two-sample MR design: (i) relevance; (ii) exclusiveness; (iii) independence.
Statistical analysis for Mendelian randomization
To analyze the possible causal effects between GERD and NAFLD, we chose the Inverse Variance Weighted (IVW) method as our leading strategy. In the presence of multiple genetic variants, the IVW can account for each genetic variant by averaging their effects to provide an overall causal estimate16. MR-Egger extends the IVW method by incorporating the analysis of horizontal pleiotropy through MR-Egger intercept27. The weighted median method can provide valid MR estimates even when up to half of the SNPs violate the InSIDE assumption28. The results of simple mode and weighted mode can be consistent even if the majority of instruments are invalid. The power of them is smaller than IVW and weighted median, but lager than MR-Egger29. Therefore, we can see that the other four methods (MR-Egger, Weighted median, simple mode, and weighted mode) can take effect in a looser scene, but give up some statistical power. Accodingly, we regarded them as supplements, but only when the directions of these five methods remain consistent could the MR analysis be rendered meaningful.
To test the robustness of the MR findings, heterogeneity and pleiotropy test are indispensable. We imported Cochran’s Q test to calculate the heterogeneity of the IVW. A leave-one-out analysis was also performed to test whether the potential causal association between exposure and outcome could be seriously confounded by a single SNP. MR-PRESSO and MR-Egger were implemented to test pleiotropy. MR-Egger intercept analysis was aimed to check the average pleiotropic effect, which revealed that if there was a non-zero intercept, the IVW analysis may not hold water due to pleiotropy. Only P values of above checking methods all over 0.05 rendered the conclusion effective. Finally, in order to avoid reserve causation, Steiger directionality test was utilized to ensure the unidirectionality of MR findings30.
All MR analysis were two-sided and performed on the platform of Rstudio (version 4.1.3) with the TwoSampleMR package (version 0.5.8). Full documentation was able to be retrieved at https://mrcieu.github.io/TwoSampleMR. The study design is shown in Fig. 1.
Statistical analysis for meta-analysis
For the three groups derived from MR analysis, we then performed meta-analysis to evaluate summarized odds ratio (OR) and 95% confidence intervals (CI). If the heterogeneity existed, the OR would be calculated via random-effects models, otherwise fixed-effects models. We opted to use I-square tests to test heterogeneity. Only when I2-value < 50% and P > 0.05 could the result of meta-analysis be deemed as homogeneous.
The meta-analysis was performed on the platform of Rstudio (version 4.1.3) with the meta package.
Ethical approval
No additional ethics approval was needed because all data in the study was previously collected, analyzed, and published.
Result
Instrumental variables for MR
After screening for genome-wide significance (P-value), LD (R2 < 0.001), and the evaluation of F (F > 10), only three groups of data of exposure was reserved for MR and meta-analysis (Table 1). The other seven sets were abandoned because the value of F does not satisfy the requirement. Moreover, to include more SNPs that contributed to GERD, a relatively relaxed threshold were applied with P < 5 × 10–7 for the Group 2 (GWAS ID: ebi-a-GCST90018848) and P < 5 × 10–6 for the Group 3 (GWAS ID: finn-b-K11_REFLUX), which had previously utilized in many MR researches31. We also removed SNPs that were associated with confounders of NAFLD according to literatures (obesity, hypertension, type II diabetes mellitus, dietary habits, physical activity, and socioeconomic factors)8. Lastly, suitable IVs were generated (Group 1: 22 SNPs; Group 2: 7 SNPs; Group 3: 29 SNPs) for the next MR analysis (Supplemental Table 2).
Mendelian randomization analysis
The IVW analysis displayed GERD was associated with a higher morbidity of NAFLD (Group 1: OR = 1.81; 95%CI 1.15–2.83; P = 0.0098; Group 2: OR = 1.94; 95%CI 1.15–3.27; P = 0.013; Group 3: OR = 1.63; 95%CI 1.28–2.09; P < 0.0001). This result was consistent with the results of weighted median (WM) (Group 1: OR = 2.35; 95%CI 1.26–4.39; P = 0.0075; Group 2: OR = 2.24; 95%CI 1.15–4.36; P = 0.018; Group 3: OR = 1.75; 95%CI 1.23–2.49; P = 0.0019). The MR-Egger showed no association (all P > 0.05). The directions all kept consistent. Cochran’s Q test of IVW and MR Egger showed no heterogeneity between IVs (all P > 0.05), and the results of MR-Egger intercept analysis and MRPRESSO approved no horizontal pleiotropy existed (all P > 0.05) (Table 2 and Supplemental Tables 3, 4, 5, 6).
Leave-one-out cross-validation was utilized to calculate the MR result of the left IVs after removing them one by one. The β value remained above zero regardless of which genetic variants were removed, suggesting that each variant performed a positive influence on the outcome. With the assistance of the Steiger test, the direction of our analysis confirmed that there was no reverse causality (all P < 0.001) (Table 2, Figs. 2, 3 and Supplemental Fig. 1, 2, 3).

The MR results of the causal effect of GERD on NAFLD (with Forest plot).

Scatter plots and Funnel plots of genetic associations with GERD against the genetic associations with NAFLD. (A) and (B) The scatter plot and funnel plot of the association between GERD (id: ebi-a-GCST90000514) and NAFLD. (C) and (D) The scatter plot and funnel plot of the association between GERD (id: ebi-a-GCST90018848) and NAFLD. (E) and (F) The scatter plot of the association between GERD (id: finn-b-K11_REFLUX) and NAFLD.
Of note, the issue of potential overlapping between databases (Group 2 and Group 3) is worth explaining. The exposure and outcome of Group 220 may both have partial samples from FinnGen, while for Group 3 they both from FinnGen. The influence of potential overlapping (called weak instrument bias) can be measured by Type 1 error rates. We used the formulae of website built by Burgess et al.32 (https://sb452.shinyapps.io/overlap) to calculate the probability of making Type 1 error and the results showed that the rates of the two groups (Group 1, Group 2) were both approximately 5%, which could be acceptable and indirectly reflected a lower degree of overlap.
Meta-analysis
Taking IVW as the major method, we conducted meta-analysis on it for an overall outcome. The result did not show any statistical heterogeneity (I2 = 0.0%; H = 1.00; P = 0.81). Accordingly, the fixed-effects model were chosen to perform the result (OR 1.71 95% CI 1.40–2.09; P < 0.0001) (Fig. 4 and Supplemental Table 7). Meanwhile, the Egger’s test (P = 0.26), Begg’s test (P = 0.33) and the visualization of funnel plot showed no evidence of publication bias (Supplemental Fig. 4).

Forest plot of results from MR analysis.
Discussion
To our knowledge, this study is the first MR analysis to reveal the causation between GERD and NAFLD. We found the overall risk of getting NAFLD is about 71% in people with GERD (OR 1.71 95% CI 1.40–2.09; P < 0.0001) in MR and meta analysis, by virtue of the GWAS and FinnGen databases10. This research is also consistent with Wijarnpreecha and Lee13,33.
The link between GERD and NAFLD has not been entirely understood. Several possible explanations may account for it.
There is evidence that people suffering from GERD are inclined to acquire insulin resistance (IR)34. The reflux of acid stimulates esophageal epithelial cells to produce chemokines, which subsequently activate various immune cells. Then these activated cells will produce myriad pro-inflammatory cytokines such as IL-6, IL-1, and TNF-alpha. On the one hand, these cytokines give rise to insulin resistance, making insulin lose its capability of inhibiting apoptosis. Utimately, NAFLD develops as a result of the accumulation of free fatty acids in the liver35,36. On the other hand, Cytokines tend to recruit Kupffer cells to intervene in inflammation and suppress lipid metabolism, ultimately leading to NAFLD37.
Reactive oxygen species (ROS) have been reported to play an important role in the pathogenesis of varied gastrointestinal (GI) diseases, including GERD and liver cirrhosis38,39. Acid exposure and sequential ROS generation will cause the damage to mucosal damage35.Simultaneously, ROS can be detrimental to the liver and accelerate the pathogenesis of NAFLD40.
There is evidence that visceral obesity, but not BMI, is closely correlated with the development of GERD and NAFLD11,41,42,43. The visceral adipose tissue (VAT) accumulated in the abdomen leads to the increase of intragastric pressure, which then contributes to abnormal acid reflux, and inescapably GERD44,45. Besides, the accumulation of free fatty acids in the liver and adipocytokine dysregulation induced by VAT will foster the chronic inflammation and promote the pathogenesis of NAFLD11,46.
Additionally, GERD patients tend to take PPIs, serving as the most effective treatment. In recent years, copious studies have reported that the long-term use of PPIs may induce the intestinal dysbiosis, affecting the composition of the gut microbiota and pushing the bacterial overgrowth47. On that occasion, the bacterial transit from luminal surface to the liver circulation is uplifted, thus causing inflammatory response in the liver and deteriorating its condition. At last, as mentioned above, inflammatory cytokines will produce NAFLD48.
Limitation
However, some limitations still exist in the study. First, due to the lack of data on other races, the genetic variants of exposure and outcome were both retrieved from European ancestry. Thus, expanding the causal relationship discovered to other races was not appropriate, which suggested the lack of universality. However, the limited population frees the discovery from the bias of the different races of exposure and outcome. Second, although MR analysis avoids the drawbacks of observational studies, such as reverse causality and residual confounding, it is susceptible to pleiotropy. The use of the weighted median can solve this problem, because it works even if half of the SNPs are not valid22,23. Moreover, the MR-Egger intercept test is also joined to minimize the bias from pleiotropy. Third, despite that we removed the SNPs associated with confounders according to assumption (iii), this type of selection was based on the present GWAS database. We acknowledge that the analysis cannot control for unknown confounders, which may violate assumption (iii) and bias the analysis. Fourth, the study has only demonstrated that people with GERD are more likely to develop NAFLD, based on the existing databases. The specific mechanisms between the two diseases are warranting further examination. Finally, we used a dataset of currently searchable large samples for analysis. As the database increase and update, the result may change accordingly.
Conclusion
In conclusion, our MR study combined with meta-analysis indicated the credible causal association between GERD and NAFLD. Considering the high prevalence of both diseases, further investigations may contribute to the development of new prevention and treatment strategies.
Data availability
All the GWAS summary data in this study can be downloaded from the public repositories. The SNPs of GERD were from open EBI GWAS database (https://www.ebi.ac.uk/). The SNPs of otorhinolaryngological diseases could be retrieved from FinnGen database (http://www.finngen.fi/en).
Abbreviations
- CI:
-
Confidence interval
- GERD:
-
Gastroesophageal reflux disease
- GWAS:
-
Genome-wide association study
- GI:
-
Gastrointestinal
- IL:
-
Interlukin
- IR:
-
Insulin resistance
- IV:
-
Instrumental variable
- IVW:
-
Inverse Variance Weighted
- MR:
-
Mendelian randomization
- NAFLD:
-
Non-alcoholic fatty liver disease
- OR:
-
Odds ratio
- PPI:
-
Proton pump inhibitor
- ROS:
-
Reactive oxygen species
- SNP:
-
Single nucleotide polymorphism
- T2DM:
-
Type II diabetes mellitus
- TNF:
-
Tumor necrosis factor
References
Gyawali, C. P. et al. Modern diagnosis of GERD: The Lyon Consensus. Gut 67(7), 1351–1362. https://doi.org/10.1136/gutjnl-2017-314722 (2018).
Azer, S. A. & Reddivari, A. K. R. Reflux Esophagitis (StatPearls Publishing, 2023).
Rettura, F. et al. Refractory gastroesophageal reflux disease: A management update. Front. Med. 8, 765061. https://doi.org/10.3389/fmed.2021.765061 (2021).
Jung, H. K. Epidemiology of gastroesophageal reflux disease in Asia: A systematic review. J. Neurogastroenterol. motil. 17(1), 14–27. https://doi.org/10.5056/jnm.2011.17.1.14 (2011).
El-Serag, H. B., Sweet, S., Winchester, C. C. & Dent, J. Update on the epidemiology of gastro-oesophageal reflux disease: A systematic review. Gut 63(6), 871–880. https://doi.org/10.1136/gutjnl-2012-304269 (2014).
Pouwels, S. et al. Non-alcoholic fatty liver disease (NAFLD): A review of pathophysiology clinical management and effects of weight loss. BMC Endocr. Disord. 22(1), 63. https://doi.org/10.1186/s12902-022-00980-1 (2022).
Younossi, Z. et al. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 15(1), 11–20. https://doi.org/10.1038/nrgastro.2017.109 (2018).
Huang, T. D., Behary, J. & Zekry, A. Non-alcoholic fatty liver disease: A review of epidemiology, risk factors, diagnosis and management. Intern. Med. J. 50(9), 1038–1047. https://doi.org/10.1111/imj.14709 (2020).
Yang, H. J. et al. Nonalcoholic fatty liver disease is associated with increased risk of reflux esophagitis. Dig. Dis. Sci. 62(12), 3605–3613. https://doi.org/10.1007/s10620-017-4805-6 (2017).
Mikolasevic, I. et al. Association between gastroesophageal reflux disease and elastographic parameters of liver steatosis and fibrosis: Controlled attenuation parameter and liver stiffness measurements. Can. J. Gastroenterol. Hepatol. 2021, 6670065. https://doi.org/10.1155/2021/6670065 (2021).
Fujiwara, M. et al. The symptoms of gastroesophageal reflux disease correlate with high body mass index, the aspartate aminotransferase/alanine aminotransferase ratio and insulin resistance in Japanese patients with non-alcoholic fatty liver disease. Int. Med. (Tokyo, Jpn.) 54(24), 3099–3104. https://doi.org/10.2169/internalmedicine.54.4297 (2015).
Miele, L. et al. Non-alcoholic fatty liver disease is associated with high prevalence of gastro-oesophageal reflux symptoms Digestive and liver disease. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 44(12), 1032–1036. https://doi.org/10.1016/j.dld.2012.08.005 (2012).
Wijarnpreecha, K., Panjawatanan, P., Thongprayoon, C., Jaruvongvanich, V. & Ungprasert, P. Association between gastroesophageal reflux disease and nonalcoholic fatty liver disease: A meta-analysis. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 23(6), 311–317. https://doi.org/10.4103/sjg.SJG_161_17 (2017).
Min, Y. W. et al. Non-alcoholic fatty liver disease and the development of reflux esophagitis: A cohort study. J. Gastroenterol. Hepatol. 33(5), 1053–1058. https://doi.org/10.1111/jgh.14042 (2018).
Catanzaro, R. et al. Nonalcoholic fatty liver disease increases risk for gastroesophageal reflux symptoms. Dig. Dis. Sci. 59(8), 1939–1945. https://doi.org/10.1007/s10620-014-3113-7 (2014).
Davey Smith, G. & Hemani, G. Mendelian randomization: Genetic anchors for causal inference in epidemiological studies. Hum. Mol. Genet. 23(R1), R89-98. https://doi.org/10.1093/hmg/ddu328 (2014).
Bowden, J. & Holmes, M. V. Meta-analysis and Mendelian randomization: A review. Res. Synth. Methods. 10(4), 486–496. https://doi.org/10.1002/jrsm.1346 (2019).
Smith, G. D. & Ebrahim, S. Mendelian randomization: Prospects, potentials, and limitations. Int. J. Epidemiol. 33(1), 30–42. https://doi.org/10.1093/ije/dyh132 (2004).
Lee, Y. H. An overview of meta-analysis for clinicians. Korean J. Int. Med. 33(2), 277–283. https://doi.org/10.3904/kjim.2016.195 (2018).
Ong, J. S. et al. Multitrait genetic association analysis identifies 50 new risk loci for gastro-oesophageal reflux, seven new loci for Barrett’s oesophagus and provides insights into clinical heterogeneity in reflux diagnosis. Gut 71(6), 1053–1061. https://doi.org/10.1136/gutjnl-2020-323906 (2022).
Sakaue, S. et al. A cross-population atlas of genetic associations for 220 human phenotypes. Nat. Genet. 53(10), 1415–1424. https://doi.org/10.1038/s41588-021-00931-x (2021).
Dönertaş, H. M., Fabian, D. K., Valenzuela, M. F., Partridge, L. & Thornton, J. M. Common genetic associations between age-related diseases. Nature aging. 1(4), 400–412. https://doi.org/10.1038/s43587-021-00051-5 (2021).
Sekula, P., Del Greco, M. F., Pattaro, C. & Köttgen, A. Mendelian randomization as an approach to assess causality using observational data. J. Am. Soc. Nephrol. JASN 27(11), 3253–3265. https://doi.org/10.1681/asn.2016010098 (2016).
Burgess, S. & Thompson, S. G. Avoiding bias from weak instruments in Mendelian randomization studies. Int. J. Epidemiol. 40(3), 755–764. https://doi.org/10.1093/ije/dyr036 (2011).
VanderWeele, T. J., TchetgenTchetgen, E. J., Cornelis, M. & Kraft, P. Methodological challenges in mendelian randomization. Epidemiol. (Camb., Mass). 25(3), 427–435. https://doi.org/10.1097/ede.0000000000000081 (2014).
Didelez, V. & Sheehan, N. Mendelian randomization as an instrumental variable approach to causal inference. Stat. Methods Med. Res. 16(4), 309–330. https://doi.org/10.1177/0962280206077743 (2007).
Burgess, S. & Thompson, S. G. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur. J. Epidemiol. 32(5), 377–389. https://doi.org/10.1007/s10654-017-0255-x (2017).
Burgess, S., Foley, C. N., Allara, E., Staley, J. R. & Howson, J. M. M. A robust and efficient method for Mendelian randomization with hundreds of genetic variants. Nat. Commun. 11(1), 376. https://doi.org/10.1038/s41467-019-14156-4 (2020).
Hartwig, F. P., Davey Smith, G. & Bowden, J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int. J. Epidemiol. 46(6), 1985–1998. https://doi.org/10.1093/ije/dyx102 (2017).
Xiao, G. et al. Causality of genetically determined metabolites on anxiety disorders: A two-sample Mendelian randomization study. J. Transl. Med. 20(1), 475. https://doi.org/10.1186/s12967-022-03691-2 (2022).
Chen, X. et al. Depression and prostate cancer risk: A Mendelian randomization study. Cancer Med. 9(23), 9160–9167. https://doi.org/10.1002/cam4.3493 (2020).
Pierce, B. L. & Burgess, S. Efficient design for Mendelian randomization studies: Subsample and 2-sample instrumental variable estimators. Am. J. Epidemiol. 178(7), 1177–1184. https://doi.org/10.1093/aje/kwt084 (2013).
Lee, S. et al. Erosive esophagitis is associated with fatty liver in school workers. Gastroenterology. 140(5), S-256 (2011).
Budiyani, L., Purnamasari, D., Simadibrata, M. & Abdullah, M. Differences in the insulin resistance levels measured by HOMA-IR between patients with erosive and non-erosive gastroesophageal reflux disease. J. ASEAN Fed. Endocr. Soc. 32(2), 139–144. https://doi.org/10.15605/jafes.032.02.07 (2017).
Rehman, K. et al. Role of interleukin-6 in development of insulin resistance and type 2 diabetes mellitus. Crit. Rev. Eukaryot. Gene Expr. 27(3), 229–236. https://doi.org/10.1615/CritRevEukaryotGeneExpr.2017019712 (2017).
Cobbina, E. & Akhlaghi, F. Non-alcoholic fatty liver disease (NAFLD)—Pathogenesis, classification, and effect on drug metabolizing enzymes and transporters. Drug Metab. Rev. 49(2), 197–211. https://doi.org/10.1080/03602532.2017.1293683 (2017).
Watt, M. J., Miotto, P. M., De Nardo, W. & Montgomery, M. K. The liver as an endocrine organ-linking nafld and insulin resistance. Endocr. Rev. 40(5), 1367–1393. https://doi.org/10.1210/er.2019-00034 (2019).
Kim, Y. J., Kim, E. H. & Hahm, K. B. Oxidative stress in inflammation-based gastrointestinal tract diseases: Challenges and opportunities. J. Gastroenterol. Hepatol. 27(6), 1004–1010. https://doi.org/10.1111/j.1440-1746.2012.07108.x (2012).
Ustaoglu, A. et al. Mucosal pathogenesis in gastro-esophageal reflux disease. Neurogastroenterol. Motil. 32(12), e14022. https://doi.org/10.1111/nmo.14022 (2020).
Nassir, F. NAFLD: Mechanisms treatments and biomarkers. Biomolecules https://doi.org/10.3390/biom12060824 (2022).
Chang, P. & Friedenberg, F. Obesity and GERD. Gastroenterol. Clin. North Am. 43(1), 161–173. https://doi.org/10.1016/j.gtc.2013.11.009 (2014).
Chen, X. et al. Associations between abdominal obesity indices and nonalcoholic fatty liver disease: Chinese visceral adiposity index. Front. Endocrinol. 13, 831960. https://doi.org/10.3389/fendo.2022.831960 (2022).
Fujikawa, Y. et al. High prevalence of gastroesophageal reflux symptoms in patients with non-alcoholic fatty liver disease associated with serum levels of triglyceride and cholesterol but not simple visceral obesity. Digestion 86(3), 228–237. https://doi.org/10.1159/000341418 (2012).
Camilleri, M., Malhi, H. & Acosta, A. Gastrointestinal complications of obesity. Gastroenterology 152(7), 1656–1670. https://doi.org/10.1053/j.gastro.2016.12.052 (2017).
Nehlig, A. Effects of coffee on the gastro-intestinal tract: A narrative review and literature update. Nutrients https://doi.org/10.3390/nu14020399 (2022).
Milić, S., Lulić, D. & Štimac, D. Non-alcoholic fatty liver disease and obesity: Biochemical, metabolic and clinical presentations. World J. Gastroenterol. 20(28), 9330–9337. https://doi.org/10.3748/wjg.v20.i28.9330 (2014).
Shi, Y. C. et al. Effects of proton pump inhibitors on the gastrointestinal microbiota in gastroesophageal reflux disease. Genom. Proteom. Bioinform. 17(1), 52–63. https://doi.org/10.1016/j.gpb.2018.12.004 (2019).
Singh, A. et al. Association between anti-acid therapies and advanced fibrosis in type 2 diabetics with biopsy-proven non-alcoholic fatty liver disease. Indian J. Gastroenterol. Off. J. Indian Soc. Gastroenterol. 39(6), 591–598. https://doi.org/10.1007/s12664-020-01087-y (2020).
Acknowledgements
Data described in the manuscript, code book, and analytic code will be made available upon request pending application. We appreciate the participants and investigators of the FinnGen study for the SNPs of otorhinolaryngological diseases (ENT diseases) and the open GWAS database for the SNPs about GERD. We thank the website (https://www.pngkey.com/) for the icons in Figure 1. We are also grateful for the instructions from Jia-Nan Wang.
Author information
Authors and Affiliations
Contributions
L.X. designed this study, drafted the manuscript, collected and analyzed the data. L.W.Z. and Z.F.P. revised the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Leng, X., Liao, WZ. & Zheng, FP. Gastroesophageal reflux disease and non-alcoholic fatty liver disease: a two-sample Mendelian randomization combined with meta-analysis. Sci Rep 14, 12633 (2024). https://doi.org/10.1038/s41598-024-63646-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-63646-z
- Springer Nature Limited