
Abstract
Psychological interventions delivered by non-specialist providers have shown mixed results for treating maternal depression. mHealth solutions hold the possibility for unobtrusive behavioural data collection to identify challenges and reinforce change in psychological interventions. We conducted a proof-of-concept study using passive sensing integrated into a depression intervention delivered by non-specialists to twenty-four adolescents and young mothers (30% 15–17 years old; 70% 18–25 years old) with infants (< 12 months old) in rural Nepal. All mothers showed a reduction in depression symptoms as measured with the Beck Depression Inventory. There were trends toward increased movement away from the house (greater distance measured through GPS data) and more time spent away from the infant (less time in proximity measured with the Bluetooth beacon) as the depression symptoms improved. There was considerable heterogeneity in these changes and other passively collected data (speech, physical activity) throughout the intervention. This proof-of-concept demonstrated that passive sensing can be feasibly used in low-resource settings and can personalize psychological interventions. Care must be taken when implementing such an approach to ensure confidentiality, data protection, and meaningful interpretation of data to enhance psychological interventions.
Similar content being viewed by others

Introduction
Depression is one of the most prevalent psychiatric disorders in the postpartum period with an estimated 3–32% prevalence among women in low- and middle-income countries (LMICs)1. In LMICs, lack of treatment for postpartum depression (PPD) is associated with a range of negative mental and physical health outcomes and considerable distress and disability for young mothers and their children, including low responsiveness towards the infant and poor infant cognitive development PPD is recognised as a significant risk factor for the child of a depressed mother to develop depression themselves later in life. With poor maternal and child health outcomes, the need to develop effective strategies to reduce PPD is critical.
Although there are several effective interventions to manage depression, one of the greatest challenges in the field of mental health is the lack of skilled mental health professionals to deliver these interventions to those in need2. There has been development and testing of interventions for PPD delivered by paraprofessionals in LMICs3. However, non-specialist interventions have shown mixed results, and limited long-term benefits4. Many of the currently used interventions delivered by non-specialists, such as lay counsellors, are rooted in the theory of behavioural activation (BA)3. BA helps individuals identify their most important goals, clarify why these goals are important and then identify behaviours that will help them move towards achieving their goals5. BA is a highly flexible process, and counsellors can adapt it to individuals’ circumstances. By focusing on goals and behaviour, BA is a potentially useful intervention for lay counsellors to deliver to individuals with PPD. The challenge is to identify the different circumstances that individuals face and how these circumstances may impact their mental health. Passive sensing technologies in mobile phones and non-invasive wearable devices have the potential to supplement BA interventions by collecting data that can be transformed by machine learning to enhance the delivery of psychological interventions by monitoring behavioural patterns and reinforcing behavioural change6.
Digital phenotypes are the biographical data profiles of individuals generated from passively collected personal data. They provide the person-context pairs that define the individual’s moment-by-moment situated experiences in their physical, digital and social environments7. Analysis of passively collected data, such as mobile phone usage, can provide insight into the challenge’s individuals face in their everyday lives and the effects of those challenges on their mental health. This may be used to tailor interventions to the individual’s needs and circumstances8,9.
To illustrate, passive data collection through wearable devices has been utilized to monitor sleep patterns, revealing correlations between sleep disturbances and mood disorders10,11. This approach enables the tailoring of interventions focused on improving sleep hygiene, which is crucial in treating mood disorders. Similarly, monitoring physical activity through smartphones and wearable devices has been instrumental in identifying the relationship between decreased physical activity and depressive symptoms12. As one of the most important features in models designed to estimate depressive symptoms12, activity data could facilitate the development of interventions that encourage and monitor physical activity, addressing a key aspect of depression management. Furthermore, passive data collection has proven effective in monitoring social rhythms in individuals with schizophrenia and bipolar disorder, providing insights into changes in social behaviour. By modelling this metric from digital footprints, interventions can be personalized to help stabilize daily routines without the need for self-reporting13,14. Lastly, voice analysis through passive data collection offers a novel approach to detecting affective disorders, enabling tailored interventions that focus on emotion regulation techniques and provided timely support when signs of emotional distress are identified15.
Mobile phone-based passive sensing enables measurement of human mobility through the global positioning system (GPS), physical activity through accelerometers, exposure to environmental sounds including human speech through processed audio recordings, and proximity to children and others using Bluetooth technology. Further, physiological data (e.g., heart rate, sleep patterns) can be collected from wearables such as smartwatches. These data can all be collected relatively unobtrusively from the individual and used to create a personal data profile that represents the individual’s behavioural characteristics16,17. These data are available through edge devices such as smartphones and smartwatches and uploaded to the cloud where they are processed, combined and analysed using machine learning approaches such as multilinear principal component analysis and convolutional neural networks to provide information for paraprofessionals delivering psychological interventions. In this study, we aimed to integrate a passive sensing platform that collects audio, GPS location, mother–child proximity, and physical activity into a psychological intervention delivered by paraprofessional counsellors in rural Nepal to test for proof of concept6.
Methods
Study design and participants
The proof-of-concept study followed formative development work18,19,20. This paper reports on the final single-arm intervention where the StandStrong counsellor app19 was provided to lay counsellors offering a 5-session BA intervention, entitled the Healthy Activity Program (HAP)21, to systematically visualize the passive sensing data of depressed adolescent and young mothers during care. The passive sensing data were designed to be used to provide tailored counselling sessions to the mothers6. All research was conducted in consultation with a community advisory board made up of female community health volunteers and auxiliary nurse midwives from seven health facilities.
Study setting
Nepal is classified as a lower-middle-income country and among the poorest in South Asia22. Mental health services are not widely available in this context, though Nepal does lead compared to similar LMIC counterparts with recent mental health policies and primary mental health service implementation. In larger cities, some government and private hospitals offer services23. In Chitwan, a district in the Bagmati Province, a southern region of Nepal, specialist mental health services are provided by two psychiatrists and a psychiatric ward in the district hospital. These resources see Chitwan having more capacity than most other areas in Nepal. This is in part because, for the past decade, Chitwan has been the Nepal implementation district for the Program for Improving Mental Health Care (PRIME). The psychological treatment for postpartum depression that was offered in this study emerged from intervention trials as part of PRIME24.
Intervention and mHealth platform
The healthy activity programme (HAP)
HAP consists of approximately 5–8 sessions divided into three phases. A comprehensive overview of the HAP intervention development has been previously published21. In summary (Fig. 1), Phase I (assessment and psychoeducation) is completed over the course of two sessions. Session 1 introduces Initial assessments for psychosocial well-being and self-care. Session 2 follows a week later with Psychoeducation based on HAP and self-care. Phase II also contains two sessions both focusing on problem solving. Finally, in Phase III, a single session is spent focusing on relapse prevention & wrap-up.

Schematic overview of the content covered in each of the five Healthy Activity Programme sessions as implemented in Nepal.
Electronic behaviour monitor app
Passive sensing data was collected using a low-cost Android smartphone and a Bluetooth Low Energy beacon (Radius Networks) attached in a pouch to the child’s clothing. The Electronic Behaviour Monitor (EBM) v2.0 was installed on the smartphone and configured to run every 15 min between 4:00 AM and 9:59 PM daily. The EBM app passively collected data for 30 s every time it was triggered for 18 h a day. Data collected are short audio recordings (.wav) from the mobile phone mic, GPS location using the Android LocationManager (lat, lon, accuracy), mother–child proximity established by scanning from the mobile phone running the EBM for Bluetooth advertising packets (id, RSSI) from a Bluetooth beacon (RadBeacon, Radius Networks), and physical activity (walking, running, tilting, still, driving, unknown) using the Activity Recognition API provided by Android. As network connectivity was a concern, the EBM was designed as an offline-first app with all data being saved to a folder on the smartphones SD card. A research assistant visited the home once a week to download the data from the SD card and then uploaded it to the study cloud database on return to the office19. More information about the EBM platform and findings relating to the acceptability and feasibility of the approach are available20,25.
StandStrong platform
The Sensing Technologies for Maternal Depression Treatment in Low Resource Settings (StandStrong) Provider Platform was designed to surface behavioural insights about how HAP was affecting participants behaviour19. The platform gives providers easy access to review the passive data collected by the EBM app and thereby provides personalized HAP sessions to mothers. The app’s home screen was a feed of data cards designed to visualize the passively collected data. Data cards included visualisations for proximity, activity, GPS movement and proximity / daily routine. Finally, when goals (similar to setting a 10,000-step walking goal) were achieved, the provider was notified and they were able to directly message the participant from within the StandStrong App to the participants Viber, a popular messaging app in Nepal.
Assessment tools
The Patient Health Questionnaire (PHQ-9) was administered as part of the screening assessment to confirm eligibility. The PHQ-9 is a widely used tool for assessing depression25,26. It contains 9 items rated on a 0 to 3 frequency scale. In Nepal, a cut-off score of 9 or more was selected for this study based on validation findings from a primary care population in Chitwan; this cut-off yields a 94% sensitivity and 69% specificity27. The Beck Depression Inventory (BDI) is a 21-item scale rated on 0 to 3 severity scale28. The BDI has been validated for use in Nepal with an established cut-off score of 10 for moderate depression (sensitivity = 0.73, specificity = 0.91)29. The BDI was selected as the primary outcome for this study because it is routinely used in clinical practice in Nepal as a measure of symptom improvement and the diversity of items allowed for more comprehensive symptom monitoring compared to the PHQ-9 (i.e., 21 symptoms in the BDI, including behavioural symptoms, compared to 9 symptoms in the PHQ). The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) was used to assess impairment in functioning due to health problems in the past 30 days30. It is a 12-item scale and provides with 5-point response score from 1 ‘none’ to 5 ‘Extreme/cannot do’31. The WHODAS has been adapted32, and used widely been used in Nepal33. These locally adapted and validated scales were supplemented with qualitative data collected through in-depth interviews with participating mothers and providers.
Ethics declaration
This study was approved by the Nepal Health Research Council (#327/2018) and George Washington University's Institutional Review Board (#051,845). All methods were performed in accordance with the relevant guidelines and regulations of both IRBs and countries. Informed consent was obtained from all participants.
Procedures
Female research assistants recruited adolescent mothers from postnatal clinics and immunization camps in Chitwan, Nepal. After informed consent, the PHQ-9 was administered as a screening tool. In addition to requiring a PHQ-9 score higher than or equal to 9, eligibility criteria included (a) mothers between the ages of 15–25 years, and (b) infants younger than 12 months of age. Once a participant was screened for depression and informed consent completed, a study team member visited her home for family informed consent. For participants under the age of 18 years, we asked for a written parental permission form and assent form. Once enrolled, the mothers received passive sensing technology (smartphone with EBM app installed and Bluetooth beacon on the baby) and enrolled in a 5-week HAP programme. During the sessions, the counsellor used the passive sensing data to tailor the therapy and incorporated the data visualization to share the mother’s behavioural changes. The counsellor used the data with the participants in the sessions to keep track of the behavioural changes, for example, they used it for mood monitoring associated with their daily activities. The participant would maintain a log of their daily life and then also rate their mood on how they felt at that time. The discussion of these data was then supplemented by the counsellor using the passive data looking at if they left the house, how far they walked, and if they spent time with their child. They also jointly reviewed the GPS map which showed a heatmap of hot spots that were frequently visited outside of their homes which introduced interesting discussions about physical activity and social support. The counsellor used this passive data to enrich and probe further into the client’s self-reports.
For the passive data collection, audio was assessed for the presence or absence of speech using the Pyannote Voice Activity Detection (VAD) model34. The activity was classified into 7 categories using the Activity Recognition API by Google on the Android platform. Proximity information was collected by recording RSSI values, a measure of signal strength, between the beacon worn by the child and the smartphone carried by the mother. These data were recoded into a binary categorical variable (presences/absence). Finally, GPS data was processed using the scikit-mobility Python package35.
Analysis
The primary outcome, to demonstrate the effectiveness of the tech-enhanced HAP intervention, was the BDI. We intended to recruit 26 depressed mothers to reliably determine these outcomes. Sample characteristics at baseline including BDI, WHODAS, mothers' education and occupation, child’s age, and primary caregiver were all summarised with descriptive statistics. Clinical change and survival analyses for the primary outcome (BDI) were performed using SPSS 24. Passive data were aggregated by week and changes over time were calculated using pandas in Python 3.8. Correlation matrices and change statistics were calculated for the primary clinical outcome (BDI) along with changes in passive data using Spearman rho due to the non-normality of data. A time to remission approach was used for the survival analysis. For each participant, weekly BDI scores were recorded, with the 'event' occurring at the first instance of a BDI score falling below the established cutoff point. For participants who did not achieve a score below the cutoff during the study, their data were right-censored at the last observation point. Qualitative data were inductively coded by two independent coders to produce a set of emerging themes. A more complete analysis of the qualitative data is planned for a future paper. Thematic codes relating to the usefulness of the passive data in the delivery of care were extracted for this paper.
Results
A total of 782 mothers were screened at health posts during infant immunization camps. Among the mothers screened, 320 were 15–25 years old, and had an infant under 12 months (Table 1). There were 26 categorized as depressed (PHQ-9 ≥ 9). Two dropped out before data collection began and were not included in the analysis. Of the remaining 24 mothers included in the analysis, the mean age of the mother was 21 (SD 2.06) with 17 (70.83%) having a secondary level of education. Mothers had been married on average 4.46 years and had between one and three children, with the oldest child averaging 6.06 years old. Only 2 (8.33%) of the mothers had husbands who were unemployed, with 3 (12.50%) working abroad and spending long periods away from home. Fifty percent of the households had 4 occupants with a maximum household occupancy of 11 people. In 50% of the homes, the mother was the primary caretaker of the child during the day. PHQ-9 scores at screening averaged 12.13 (SD 2.85) with BDI and WHODAS scores on day one having a mean of 25.63 (SD 5.45) and 14.08 (SD 9.17) respectively. By the end of the study interview over six weeks later these scores had dropped to 5.48 (SD 4.65) and 8.81 (SD 8.56) respectively.
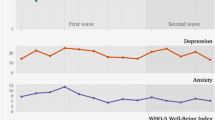
Figure 2 provides an overview of weekly data patterns seen in data from the four passive sensors. The sum of the average straight-line distance travelled increases from 41.9 to 103 km over the course of the six weeks. Time spent in proximity (10 m) between mother and child (beacon and phone) is seen to decrease from 70% in week 1 through to 53% in week 6. The amount of speech detected and the percentage of time walking remain fairly consistent across the six weeks. BDI scores are presented for comparison and can be seen to fall from 25.6 at screening to 5.8 at the final measurement.

Depression, and sensing data by week with confidence intervals; (a) average straight-line distance travelled per week; (b) the percentage of time mother and child were detected in (10 m) proximity of each other; (c) percent of weekly recordings in which speech was detected; (d) percent weekly walking activity detected; and e) BDI score by week (week 0 = at screening).
Pearson correlations for these data are presented in Table 2 with a moderate negative correlation between week of intervention and BDI scores. The percentage of time together was weakly negatively correlated with intervention week. Figure 3 presents the survival curve for BDI score through time. Although most mothers remained above the BDI cut-off of 10 over the first three weeks, by week 5, 53% of mothers were no longer above the cut-off for mild depression.

Kaplan Meyer survival curve for BDI score and weeks of treatment.
The only statistically significant change registered between week 1 and week 6 was the BDI score (Table 3). Walking activity, time in close proximity, and presence of speech were not associated with significant change between weeks 1 and 6. GPS data was not available in week 1 and week 6 for 23 of the participants making it infeasible to look at change through time. Qualitative insights into participants experience of passive sensing being integrated into counselling sessions is provided in Table 4.
Discussion
A five-session HAP intervention delivered by trained lay counsellors in Nepal showed a significant reduction in symptoms of depression. These findings add to the growing body of literature on the effectiveness of task-shifting mental health support to lay counsellors trained in interventions that utilise the principles of BA36. Noticeable trends in passive sensing data were observed across the 6 weeks of intervention. GPS data is one of the more well-established passive sensing data types with, for example, studies showing increased homestay among depressed adults37. Data from this study support these findings with the weekly average of straight-line distance travelled increasing in a somewhat linear pattern. The small sample size does mean this trend needs to be interpreted with caution as measures of dispersion show large weekly variability. Proximity between mother and infant is novel and not well explored in the literature. In examining Bluetooth proximity data, it is important to consider the role of the mother in child caregiving. Preliminary analyses suggest that mothers identified as primary caretakers are more frequently within a 10-m range of their children. Further statistical analysis could elucidate whether these differences are significant, providing deeper insights into maternal engagement patterns based on their caregiving role. Additionally, the 10-m threshold used in this study typically encompasses the indoor space (affected quite heavily by furniture and the thickness of the walls) of a standard home in the study area. Therefore, mothers might still be within this range while performing indoor or be outside performing household tasks but be picked up as “apart” by our Bluetooth system. Future studies might benefit from a finer resolution of proximity measurements or the incorporation of environmental context to better capture the dynamics of mother–child interactions. Alternatives to Bluetooth such as Ultrawideband radios exist and provide resolutions closer than the 10 m accuracy typical of Bluetooth-based systems. Our data show a slow decrease in the amount of time spent within the general proximity of each other. This interpretation is supported by the extended max distance travelled as the weeks went on. On the other hand, it is not possible to refute the possibility that the beacon was just being worn less by the child as research fatigue set in. If the beacon was turned off more frequently or was not put into the pouch given to each child to carry the beacon, we might anticipate a similar pattern.
Audio data show consistently high levels of speech detection throughout the six weeks. An initial analysis of these data using the AudioSet model, trained and released by Google, found that 43% of all samples contained speech data18. For this paper, audio data were passed through the pyannote voice activity detection model. Although less capable of detecting the range of environmental audio that the AudioSet model can handle, the pyannote model sacrifices breadth for narrow speech detection accuracy. The model is lightweight and could be deployed on an edge device such as a mobile phone or watch as one way to increase the acceptability of audio recordings in the home. The detection of speech in 80% of the audio samples raises important considerations regarding the auditory environment of the home. It is evident that deeper insight could be gained if it was possible to distinguish between maternal speech directly engaged with the child and other household speech captured by the device such as from the television, radio, or other adults in the house talking to each other. This distinction is fundamental, as shown by38 infants who experienced more child-directed speech became more efficient in processing familiar words in real time and had larger expressive vocabularies by the age of 24 months, although speech simply overheard by the child was unrelated to vocabulary outcomes. Future analyses could include categorizing the types of speech interactions and their potential developmental impacts on the child.
A key principle of BA, on which HAP is built, is that movement (physical activity) can be supportive of improved mood. However, we did not observe an increase in physical activity (i.e., walking). Most data recorded a state of “still” (i.e., not moving). A number of possible explanations exist. One interpretation might be that the mothers were actually not very active and that they maintained this low rate of activity throughout the study. The second possible interpretation is that the granularity of the recoding was too coarse to pick up the walking activity that took place in the gaps between the 15-min recoding interval. Finally, it might be that the mobile phone was simply not always carried on the mother’s person and rather was placed on a table or other surface in the home. Together, these data are interesting but cannot be generalized given the small sample size and the heterogeneity among the mothers’ patterns throughout HAP treatment.
The limitations uncovered during the implementation of digital phenotyping in the home of mothers with PPD are interesting and possibly useful to others who would undertake similar work. First, as reported by20 data volumes in our study are seen to decrease the longer data are collected. Increased effort is needed from the field team as the implementation timeframe grows longer to ensure important data are not lost. Lay counsellors can also potentially promote the continued use of devices by maintaining the use of passive data findings throughout HAP delivery. Validity checks are also highly recommended. These could be as simple as a randomly timed check-in every few days to enquire about where they are, what they are doing, who they are with, and whether they have the app and beacon attached and on. These data can then later be used to corroborate what is seen in the passive data.
Another possible approach is to move the passive data collection from the phone to the smart watch. The watch is easier to carry around all day at home than a phone and additionally, the collection of heart rate data, available on almost all smartwatches these days, could be used to filter out other sensor data collected when a heartbeat is not present at that time point. In other words, if the watch is been worn, a heartbeat will be detected. This improves the interpretability of the data is it removes the concern that the watch may be lying on the bedside table. One final approach that may improve data interpretability is the triangulation of different data streams into a single multimodal analysis. For instance, if the proximity sensor suggests that the mother is not with the child, it may be difficult to interpret what exactly is triggering this reading. If the proximity data is triangulated with activity, and it is noted that the mother is walking and GPS data suggests she is outside the house, then it is more plausible to infer that she is indeed away from her child.
Once solutions similar to those suggested above have been implemented and interpretation and data validity are more solid, the possibility becomes real that person-centred interventions could be developed around the different latent class sub-types presented in the data. Although criticism exists that digital phenotyping depersonalises care by bucketing people together rather than treating each person as an individual39,40, the reality is that many lay counsellor-led interventions end up being reduced to fixed steps from a manualised intervention with limited variety and personalisation being provided41. With the approach outlined in this paper, the opportunity exists to support lay counsellors to provide high-quality care that is responsive to the individual life patterns their clients are experiencing. In addition to the effort needed to ensure that the passive data are reliable and interpretable, counsellors also require significant training if they are to understand how these data can be integrated into the care they provide. Simply providing a dashboard of data will not suffice. Training, examples, and guidelines are all needed to help lay counsellors understand what the passive data means for the therapy they are providing to each individual client.
Passive sensing technology, to date, has predominantly been explored in the area of detection and diagnosis of mental health conditions. However, there is tremendous potential for passive sensing to enhance the delivery of psychological interventions. This is the first application, to our knowledge, of paraprofessional counsellors in a low-resource setting who are guiding their treatment of postpartum depression among adolescent and young mothers using passive sensing technology. Passive sensing can be impactful in delivering personalized care because of real-time measurement of behaviour, including mother-infant interaction, which is important to improve both mothers’ and infants’ health outcomes.
Data availability
Dataset generated and or analysed during the current study are available from the corresponding author upon request.
References
Baron, E. C. et al. Maternal mental health in primary care in five low-and middle-income countries: A situational analysis. BMC Health Serv. Res. 16, 1–16 (2016).
Kakuma, R. et al. Human resources for mental health care: Current situation and strategies for action. The Lancet 378, 1654–1663 (2011).
Singla, D. R. et al. Psychological treatments for the world: Lessons from low-and middle-income countries. Annu. Rev. Clin. Psychol. 13, 149–181 (2017).
Maselko, J. et al. Effectiveness of a peer-delivered, psychosocial intervention on maternal depression and child development at 3 years postnatal: A cluster randomised trial in Pakistan. The Lancet Psychiatry 7, 775–787 (2020).
Stein, A. T., Carl, E., Cuijpers, P., Karyotaki, E. & Smits, J. A. Looking beyond depression: A meta-analysis of the effect of behavioral activation on depression, anxiety, and activation. Psychol. Med. 51, 1491–1504 (2021).
Poudyal, A. et al. Wearable digital sensors to identify risks of postpartum depression and personalize psychological treatment for adolescent mothers: Protocol for a mixed methods exploratory study in rural Nepal. JMIR Res. Protoc. 8, e14734 (2019).
Torous, J., Kiang, M. V., Lorme, J. & Onnela, J.-P. New tools for new research in psychiatry: A scalable and customizable platform to empower data driven smartphone research. JMIR Mental Health 3, e5165 (2016).
Schulte-Strathaus, J. C., Rauschenberg, C., Baumeister, H. & Reininghaus, U. Digital Phenotyping and Mobile Sensing: New Developments in Psychoinformatics 427–439 (Springer, 2022).
Aung, M. H., Matthews, M. & Choudhury, T. Sensing behavioral symptoms of mental health and delivering personalized interventions using mobile technologies. Depress Anxiety. 34(7), 603–609 (2017).
Maatoug, R. et al. Digital phenotype of mood disorders: A conceptual and critical review. Front. Psychiatry. 13, 895860 (2022).
De Angel, V. et al. Digital health tools for the passive monitoring of depression: A systematic review of methods. NPJ Digit Med. 5(1), 3 (2022).
Pedrelli, P. et al. Monitoring changes in depression severity using wearable and mobile sensors. Front. Psychiatry. 11, 584711 (2020).
Henson, P., Barnett, I., Keshavan, M. & Torous, J. Towards clinically actionable digital phenotyping targets in schizophrenia. NPJ Schizophr. 6(1), 1–7 (2020).
Abdullah, S. et al. Automatic detection of social rhythms in bipolar disorder. J. Am. Med. Inform. Assoc. 23(3), 538–543 (2016).
Ma, X., Yang, H., Chen, Q., Huang, D. & Wang, Y. DepAudioNet: An efficient deep model for audio based depression classification. In: Proceedings of the 6th International Workshop on Audio/Visual Emotion Challenge. Amsterdam The Netherlands: ACM; 2016. pp 35–42.
Huckvale, K., Venkatesh, S. & Christensen, H. Toward clinical digital phenotyping: A timely opportunity to consider purpose, quality, and safety. NPJ Digital Med. 2, 1–11 (2019).
Byanjankar, P. et al. Utilizing passive sensing data to provide personalized psychological care in low-resource settings. Gates Open Res. 4, 1 (2020).
Poudyal, A. et al. What does social support sound like? Challenges and opportunities for using passive episodic audio collection to assess the social environment. Front. Public Health 9, 633606 (2021).
Hagaman, A. et al. “Now, I have my baby so I don’t go anywhere”: A mixed method approach to the ‘everyday’and young motherhood integrating qualitative interviews and passive digital data from mobile devices. Plos one 17, e0269443 (2022).
Maharjan, S. M. et al. Passive sensing on mobile devices to improve mental health services with adolescent and young mothers in low-resource settings: The role of families in feasibility and acceptability. BMC Med. Inform. Decis. Mak. 21, 1–19 (2021).
Patel, V. et al. The effectiveness and cost-effectiveness of lay counsellor-delivered psychological treatments for harmful and dependent drinking and moderate to severe depression in primary care in India: PREMIUM study protocol for randomized controlled trials. Trials 15, 1–14 (2014).
Bank, T. W. Nepal overview. (2021).
Rai, Y., Gurung, D. & Gautam, K. Insight and challenges: Mental health services in Nepal. BJPsych Int. 18, E5 (2021).
Jordans, M. J. et al. Effectiveness of psychological treatments for depression and alcohol use disorder delivered by community-based counsellors: Two pragmatic randomised controlled trials within primary healthcare in Nepal. Br. J. Psychiatry 215, 485–493 (2019).
Byanjankar, P. et al. Utilizing passive sensing data to provide personalized psychological care in low-resource settings. Gates Open Res. 2(4), 118. https://doi.org/10.12688/gatesopenres.13117.2.PMID:33709058;PMCID:PMC7940775 (2021).
Spitzer, R. L. The PHQ-9. J. Gen. Internal Med. 16, 606–613 (2001).
Kohrt, B. A., Luitel, N. P., Acharya, P. & Jordans, M. J. Detection of depression in low resource settings: Validation of the Patient Health Questionnaire (PHQ-9) and cultural concepts of distress in Nepal. BMC Psychiatry 16, 1–14 (2016).
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J. & Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 4, 561–571 (1961).
Kohrt, B. A., Kunz, R. D., Koirala, N. R., Sharma, V. D. & Nepal, M. K. Validation of a Nepali version of the Beck Depression Inventory. Nepalese J. Psychiatry 2, 123–130 (2002).
Ustun, T. B., Kostanjesek, N., Chatterji, S., Rehm, J. & Organization, W. H. in Measuring health and disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0)/edited by TB Üstün, N. Kostanjsek, S. Chatterji, J. Rehm (2010).
Andrews, G., Kemp, A., Sunderland, M., Von Korff, M. & Ustun, T. B. Normative data for the 12 item WHO Disability Assessment Schedule 20. PloS One 4, e8343 (2009).
Risal, A. et al. Adapting world health organization disability assessment schedule 2.0 for Nepal. BMC Psychol. 9, 1–10 (2021).
Luitel, N. P. et al. Conflict and mental health: A cross-sectional epidemiological study in Nepal. Social Psychiatry Psychiatric Epidemiol. 48, 183–193 (2013).
Bredin, H. et al. in ICASSP 2020–2020 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP). 7124–7128 (IEEE).
Pappalardo, L., Simini, F., Barlacchi, G. & Pellungrini, R. scikit-mobility: A Python library for the analysis, generation and risk assessment of mobility data. https://arxiv.org/abs/1907.07062 (2019).
Karyotaki, E. et al. Association of task-shared psychological interventions with depression outcomes in low-and middle-income countries: A systematic review and individual patient data meta-analysis. JAMA psychiatry (2022).
Laiou, P. et al. The association between home stay and symptom severity in major depressive disorder: Preliminary findings from a multicenter observational study using geolocation data from smartphones. JMIR mHealth and uHealth 10, e28095 (2022).
Weisleder, A. & Fernald, A. Talking to children matters: Early language experience strengthens processing and builds vocabulary. Psychol. Sci. 24(11), 2143–2152. https://doi.org/10.1177/0956797613488145 (2013).
Birk, R. H. & Samuel, G. Digital phenotyping for mental health: Reviewing the challenges of using data to monitor and predict mental health problems. Curr. Psychiatry Rep. 24, 523–528 (2022).
Tekin, Ş. Is big data the new stethoscope? Perils of digital phenotyping to address mental illness. Philos. Technol. 34, 447–461 (2021).
Patel, V. Scaling up person-centered psychosocial interventions: Global mental Health’s next challenge. SSM-Mental Health 2, 100072 (2022).
Acknowledgements
The authors would like to acknowledge the Chitwan StandStrong Community Advisory Board for their contributions to the successful completion of this study. Anvita Bhardwaj and Sauharda Rai are acknowledged for their contribution to the development of the StandStrong study. Many thanks to the collaborating staff at the Transcultural Psychosocial Organization Nepal: Anup Adhikari, Bindu Aryal, Kamal Gautam, Suraj Koirala, Sovita Lohani, Nagendra Luitel, Aasha Mahato, Bhagwati Sapkota Kendra Mahato and Bibek KC. The authors acknowledge the support of Nepal Health Research Council (NHRC).
Funding
The StandStrong project has been funded by the Bill and Melinda Gates Foundation (Grant Number #OPP1189927).
Author information
Authors and Affiliations
Contributions
A.V.H.: Study conceptualisation, design, data analysis, writing of the first draft, and approved the final version of the manuscript. A.P.: Study conceptualisation, study coordination, data analysis, reviewed the results and approved the final version of the manuscript. A.H.: Study conceptualisation, design, data analysis, and reviewed the results and approved the final version of the manuscript. S.M.M.: Study Coordination, data collection and oversight. Review of the results and approval of the final version of the manuscript. P.B.: Data Analysis, review of results and approval of the final version of the manuscript. D.B.: Study design, data analysis, and review of the results and approval of the final version of the manuscript. A.T.: Data collection, data analysis, and review of the results and approval of the final version of the manuscript. B.K.: Study conceptualisation, design, data analysis, and reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van Heerden, A., Poudyal, A., Hagaman, A. et al. Integration of passive sensing technology to enhance delivery of psychological interventions for mothers with depression: the StandStrong study. Sci Rep 14, 13535 (2024). https://doi.org/10.1038/s41598-024-63232-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-63232-3
- Springer Nature Limited