
Abstract
In a retrospective study, 54 patients with treatment-resistant major depressive disorder (TRD) completed a free-viewing task in which they had to freely explore pairs of faces (an emotional face (happy or sad) opposite to a neutral face). Attentional bias to emotional faces was calculated for early and sustained attention. We observed a significant negative correlation between depression severity as measured by the 10-item Montgomery-Åsberg Depression Rating Scale (MADRS) and sustained attention to happy faces. In addition, we observed a positive correlation between depression severity and sustained attention to sad faces. No significant correlation between depression severity and early attention was found for either happy or sad faces. Although conclusions from the current study are limited by the lack of comparison with a control group, the eye-tracking free-viewing task appears to be a relevant, accessible and easy-to-use tool for measuring depression severity through emotional attentional biases in TRD.
Similar content being viewed by others


Introduction
Major depressive disorder (MDD) is one of the most common mental health disorders, affecting 4.4% of the world’s population1. In addition to the classic clinical symptoms (e.g., feelings of guilt, sadness), MDD is also characterized by cognitive impairments that contribute to the overall burden of the illness. Among these, deficits in emotional processing have attracted a particular interest because of their hypothesized role in the onset and maintenance of depressive symptoms2. Several studies have shown that, compared to healthy controls, people with MDD exhibit a bias toward negative stimuli over positive or neutral information3, and conversely, tend to neglect positive information4.
Interestingly, significant relationships were observed between depression severity and the intensity of emotional biases. One study using different types of stimuli (e.g., emotional words, scenes, and faces) found an association between depression severity and attention to negative information5, while another study using only emotional words found no relationship6, calling for further research on this topic.
Better characterizing attentional biases to emotional stimuli in MDD patients is crucial, as they have been shown to be a stable vulnerability factor for depression2, to persist in remitted depression and to predict future depressive symptomatology7.
It is worth noting that the mentioned studies investigating attentional biases in MDD have primarily used motor reaction time tasks and indirect measures of attention such as the stroop, dot-probe or cueing tasks. However, these tasks primarily assess early attention allocation (direction bias) which is thought to be less impaired in MDD than sustained attention allocation (duration bias)8,9. In addition, reaction time measures used to assess attentional processes have extremely low reliability10 and do not accurately capture emotional processing in patients who have difficulty responding by pressing a keyboard, due to psychomotor retardation or catatonic symptoms. Eye-tracking can overcome these limitations by providing a direct and objective measure of sustained and early attention through the recording of eye movement.
Free-viewing eye-tracking meta-analysis and review have reported that patients with MDD show a robust attentional bias away from positive stimuli and a less robust bias toward negative stimuli, compared to controls9,11. Importantly, patients with MDD show a more pronounced attentional bias toward negative stimuli than participants with subclinical depression11. Several studies have examined the relationship between depression severity and attentional bias toward emotional faces using eye-tracking in patients with MDD, but have yielded inconsistent conclusions. Some have focused solely on investigating the relationship between symptom severity and sustained attentional bias for both positive and negative information12,13,14 revealing no significant correlation. Conversely, other studies have used a free-viewing task to examine both early and sustained attention, leading to conflicting results. For instance, Duque and Vázquez15 identified a significant correlation only between the depression severity and the sustained attentional bias for sad faces, whereas Bodenschatz et al.16 reported no such correlation.
To address these discrepancies presumed to stem from methodological differences, the present study aims to investigate the relationship between both sustained and early attentional biases for emotional faces (happy and sad) and depression severity in patients with moderate to severe treatment-resistant MDD (TRD) with stable medication for 4 weeks. In this study, we hypothesized that there would be inverse correlations between attentional bias to positive and negative emotions and the severity of depression. The ultimate goal of this study is to establish eye tracking in a free-viewing task as a reliable tool for assessing the severity of depression.
Results
Clinical and sociodemographic characteristics
Clinical and sociodemographic characteristics are detailed in Table 1.
Relationship between depression severity and sustained emotional attentional bias
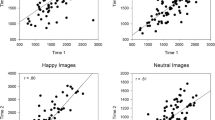
A significant negative correlation between depression severity and sustained attention bias for happy faces (pcorr < 0.01; r = -0.40; IC95% = [− 0.61; − 0.15]) was observed with strong evidence in favor of H1 (BF10 = 14.77; Fig. 1A). There was also a significant positive correlation between depression severity and sustained attention bias for sad faces (pcorr < 0.001; r = 0.51; IC95% = [0.28; 0.68]) with decisive evidence in favor of H1 (BF10 = 281.8; Fig. 1B). Multiple linear regression analyses showed no effect of age or sex on sustained attentional bias (see Table 2).

Correlation between depression severity and emotional bias for sustained attention. (A) Significant negative correlation between depression severity and sustained attention bias for happy faces (r = − 0.40; pcorr < 0.01; BF10 = 14.77). (B) Significant positive correlation between depression severity and sustained attention bias for sad faces (r = 0.51; pcorr < 0.001; BF10 = 281.8).
For sustained attentional bias toward happy faces, the multiple linear regression model accounted for 19.7% of the variation in the attentional bias to happy faces and reached statistical significance (F(3,50) = 4.088, p = 0.011; R = 0.444; adj. R square = 0.149). The results show that only the MADRS score was statistically significant in predicting the attentional bias to happy faces while sex and age were not. For sustained attentional bias to sad face, the overall model explained 26.8% of the variation in the attentional bias to sad faces and was significant (F(3,50) = 6.093, p = 0.001; R = 0.517; adj. R square = 0.224). Again, the results show that only the MADRS score was statistically significant in predicting the attentional bias to sad faces while sex and age were not (Table 2).
Relationship between depression severity and early emotional attentional bias
Analyses revealed no significant correlation between the depression severity and the laterality quotient for either happy faces (pcorr = 0.052; r = 0.34; IC95% = [0.08; 0.56]; substantial evidence in favor of H1: BF10 = 6.846, n = 53) or sad faces (pcorr = 0.90; r = -0.17; IC95% = [− 0.11; 0.42]; anecdotal evidence in favor of H0: BF10 = 0.35).
Discussion
We aimed to characterize the relationship between depression severity and emotional bias using a straightforward measure of sustained and early attention in patients with TRD.
Regarding sustained attention, the analyses showed strong evidence for a negative correlation between emotional bias to happy faces and the depression severity, and decisive evidence for a positive correlation between emotional bias to sad faces and the depression severity. This suggests that the more severe the depression, the more time participants spent looking at sad faces and the less time they spent looking at happy faces compared to neutral faces. Strengthening this robust association between depression severity and attentional bias, multiple linear regression analyses show that only the MADRS score is a predictor of sustained attentional bias, while gender and age do not contribute significantly to the prediction. Some of these findings are supported by previous eye-tracking studies, which have reported a more pronounced attentional bias in patients diagnosed with MDD compare to participants with subclinical depression11, a positive correlation between depression severity and sustained attentional bias to sad faces15, a longer DTs to sad faces, and a lack of bias to happy faces compared to controls17,18.
Regarding early attentional biases, no significant relationships were observed between the orientation of the first saccade to sad and happy faces and the depression severity. These findings are consistent with several previous eye-tracking studies showing that people with MDD do not show an initial orientation bias to emotional stimuli8,9.
The current study replicates and extends previous findings by showing in the same FVT study that there is an association between sustained emotional bias for both positive and negative stimuli and depression severity, but not with early emotional attentional bias. Although these results are encouraging some limitations that curtail the generalization of the results must be noted. First, our statistical model only controls for the effect of MADRS score, age and sex on cognitive bias, but it is known that other variables could have an impact on this cognitive function, such as treatments or disease characteristics (course of the disease, duration of episode, number of relapses, etc.). Second, it should be noted that results were obtained in patients with TRD, a specific subgroup of patients that may present differences from a clinical19 and neurobiological point of view20. However, the inclusion of treatment-resistant patients with stable antidepressant treatment for at least 4 weeks allowed us to control for the potential beneficial effect of medication on emotional processing, including FVT21. Third, the study suffers from lack of a comparison group (either healthy volunteers or people with subclinical depression). Finally, the number of face pairs presented may seem small, but this allows us to propose a task that can be completed quickly and integrated into the patient's examination routine (< 5 min). Then, because we only included ‘sad’ and ‘happy’ faces, the generalization of the current conclusions to other emotions is limited.
Finally, using a task that is accessible and easy to integrate into patients' assessment routines, we showed that sustained attentional bias toward sad and away from happy faces increases with depression severity. The FVT may be a useful tool for objective assessment of depression severity in clinical settings.
Material and method
This retrospective study was approved by a local ethics committee (Comité d’Ethique de la REcherche du VInatier—CEREVI, id number #2023/006, on April 24th, 2023), was performed in accordance with relevant French guidelines and regulations using data from an authorized anonymized database (Commission Nationale de l’Informatique et des Libertés CNIL, MR-003-2017-002), and in accordance with the Declaration of Helsinki. All participants (and/or their legal guardians when applicable) gave written informed consent for participation and for publication of the study. This retrospective study was not registered in a public database prior to its execution.
Sample
We reviewed data from patients who attended our clinical unit for treatment-resistant depression between December 2018 and December 2022. Treatment-resistant depression was defined as a failure to respond to two or more antidepressant regimens despite adequate dose and duration and adherence to treatment22. The 10-item Montgomery-Asberg Depression Rating Scale (MADRS10)23 was used to assess depression severity. It is a clinician-rated questionnaire known for its validity and inter-rater reliability24. It is designed to assess depression severity through 10 items that focuses on the symptoms of depression (e.g., sadness, tension, and pessimistic thoughts).
Patients were eligible if they had a DSM-5 diagnosis of MDD, have moderate to severe depression as indicated by a MADRS10 score ≥ 20 even on stable medication (dosage and molecule) for 4 weeks, and have completed the free viewing task (FVT) on the day of their first visit to our clinical unit. Exclusion criteria included neurological (e.g., dementia) or psychiatric comorbidities, unanalyzable eye-tracking data, incomplete clinical information, or withdrawal of consent. Of the 61 eligible patients, 7 patients were not included due to unprocessable eye-tracking data, resulting in a final analyzed sample of 54 participants with moderate to severe depression.
Eye tracking free-viewing task
The FVT consisted of showing pairs of faces: one emotional (happy or sad) and one neutral, presented randomly for 3500 ms to the right and left of a fixation cross lasting 1500 ms. We presented 23 pairs of stimuli: 11 happy-neutral and 12 sad-neutral pairs, with 12 different identities (6 males, 6 females). The faces were extracted from the Ekman and Friesen open set25. Throughout the task, gaze position and eye movements were recorded with an eye-tracking system (SMI SensoMotoric Instruments with BeGaze 3.6.52, Teltow, Germany).
Eye tracking measurement analysis
Early (direction bias) and sustained (duration bias) attention allocation was assessed per participant based on eye-movements recording26.
Dwell time (DT), the total time (ms) of all fixations on the faces, was used to measure sustained attention allocation (duration bias). The difference between emotional and neutral DTs was used to calculate an emotional bias score.
The orientation of the first saccade, corresponding to the first face the participant looked at, was used to measure early attention allocation (direction bias). A laterality quotient was calculated as the difference between the number of times the participant made a first saccade to the emotional face and the number of times where the first saccades were to the neutral face, divided by the total number of trials.
For both measures, a positive value indicates a bias toward emotional faces, while a negative value indicates a bias toward neutral faces.
Statistical analysis
We used Pearson’s correlations with Bonferroni adjustment (pcorr) to examine the relationship between sustained and early emotional attentional biases and depression severity (MADRS10 scores). To complement the frequentist statistics, we also performed Bayesian analyses using BF10, which provided us with a likelihood ratio of the alternative hypothesis (i.e., H1: correlation between variables) to the null hypothesis (i.e., H0: no correlation). Finally, to provide a more comprehensive understanding of the findings, multiple linear regression analyses were conducted to assess the predictive significance of the MADRS score, age, and sex on sustained attentional bias to happy faces and sustained attentional bias to sad faces. All statistical analyses were performed using Rstudio version 2021.09.2+382 (Richmond Hill, Canada).
Data availability
The data that support the findings of this study are available on request from the corresponding author, [J.B.]. The data are not publicly available due to local restrictions (e.g., their containing information that could compromise the privacy of research participants).
References
WHO. Depression and Other Common Mental Disorders: Global Health Estimates (Springer, 2017).
Gotlib, I. H. & Joormann, J. Cognition and depression: Current status and future directions. Annu. Rev. Clin. Psychol. 6, 285–312 (2010).
Leyman, L., De-Raedt, R., Schacht, R. & Koster, E. H. W. Attentional biases for angry faces in unipolar depression. Psychol. Med. 37, 393 (2007).
Matthews, G. R. & Antes, J. R. Visual attention and depression: Cognitive biases in the eye fixations of the dysphoric and the nondepressed. Cogn. Ther. Res. 16, 359–371 (1992).
Baert, S., De Raedt, R. & Koster, E. H. W. Depression-related attentional bias: The influence of symptom severity and symptom specificity. Cogn. Emot. 24, 1044–1052 (2010).
Krings, A., Heeren, A., Fontaine, P. & Blairy, S. Attentional biases in depression: Relation to disorder severity, rumination, and anhedonia. Compr. Psychiatry 100, 152173 (2020).
Shamai-Leshem, D., Linetzky, M. & Bar-Haim, Y. Attention biases in previously depressed individuals: A meta-analysis and implications for depression recurrence. Cogn. Ther. Res. 46, 1033–1048 (2022).
Caseras, X., Garner, M., Bradley, B. P. & Mogg, K. Biases in visual orienting to negative and positive scenes in dysphoria: An eye movement study. J. Abnorm. Psychol. 116, 491–497 (2007).
Suslow, T., Hußlack, A., Kersting, A. & Bodenschatz, C. M. Attentional biases to emotional information in clinical depression: A systematic and meta-analytic review of eye tracking findings. J. Affect. Disord. 274, 632–642 (2020).
Carlson, J. M., Fang, L., Coughtry-Carpenter, C. & Foley, J. Reliability of attention bias and attention bias variability to climate change images in the dot-probe task. Front. Psychol. 13, 1021858 (2023).
Armstrong, T. & Olatunji, B. O. Eye tracking of attention in the affective disorders: A meta-analytic review and synthesis. Clin. Psychol. Rev. 32, 704–723 (2012).
Disner, S. G., Shumake, J. D. & Beevers, C. G. Self-referential schemas and attentional bias predict severity and naturalistic course of depression symptoms. Cogn. Emot. 31, 632–644 (2017).
Klawohn, J. et al. Aberrant attentional bias to sad faces in depression and the role of stressful life events: Evidence from an eye-tracking paradigm. Behav. Res. Ther. 135, 103762 (2020).
Woolridge, S. M., Harrison, G. W., Best, M. W. & Bowie, C. R. Attention bias modification in depression: A randomized trial using a novel, reward-based, eye-tracking approach. J. Behav. Ther. Exp. Psychiatry 71, 101621 (2021).
Duque, A. & Vázquez, C. Double attention bias for positive and negative emotional faces in clinical depression: Evidence from an eye-tracking study. J. Behav. Ther. Exp. Psychiatry 46, 107–114 (2015).
Bodenschatz, C. M., Skopinceva, M., Ruß, T. & Suslow, T. Attentional bias and childhood maltreatment in clinical depression—an eye-tracking study. J. Psychiatr. Res. 112, 83–88 (2019).
Lazarov, A., Ben-Zion, Z., Shamai, D., Pine, D. S. & Bar-Haim, Y. Free viewing of sad and happy faces in depression: A potential target for attention bias modification. J. Affect. Disord. 238, 94–100 (2018).
Lu, S. et al. Attentional bias scores in patients with depression and effects of age: A controlled, eye-tracking study. J. Int. Med. Res. 45, 1518–1527 (2017).
Kornstein, S. G. & Schneider, R. K. Clinical features of treatment-resistant depression. J. Clin. Psychiatry 62, 18–25 (2001).
Runia, N. et al. The neurobiology of treatment-resistant depression: A systematic review of neuroimaging studies. Neurosci. Biobehav. Rev. 132, 433–448 (2022).
Wells, T. T., Clerkin, E. M., Ellis, A. J. & Beevers, C. G. Effect of antidepressant medication use on emotional information processing in major depression. AJP 171, 195–200 (2014).
McIntyre, R. S. et al. Treatment-resistant depression: Definition, prevalence, detection, management, and investigational interventions. World Psychiatry 22, 394–412 (2023).
Montgomery, S. A. & Åsberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 134, 382–389 (1979).
Davidson, J., Turnbull, C. D., Strickland, R., Miller, R. & Graves, K. The Montgomery-Åsberg Depression Scale: Reliability and validity. Acta Psychiatr. Scand. 73, 544–548 (1986).
Ekman, P. & Friesen, W. V. Pictures of Facial Affect (Consulting Psychologists Press, 1976).
Werthmann, J., Jansen, A. & Roefs, A. Make up your mind about food: A healthy mindset attenuates attention for high-calorie food in restrained eaters. Appetite 105, 53–59 (2016).
Acknowledgements
The authors thank the study nurses of the PSYR2 team and the Ugo Cerletti Unit. This research was funded by the joint Scientific council of CH Le Vinatier with the University Lumière Lyon 2 (#CSLV 09, RM).
Author information
Authors and Affiliations
Contributions
L.I., C.N. & J.B. wrote the first draft of the manuscript. W.V. & B.B. helped with the statistical analysis. G.P. & R.M. performed the clinical investigation and assessment. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Imbert, L., Neige, C., Moirand, R. et al. Eye-tracking evidence of a relationship between attentional bias for emotional faces and depression severity in patients with treatment-resistant depression. Sci Rep 14, 12000 (2024). https://doi.org/10.1038/s41598-024-62251-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-62251-4
- Springer Nature Limited