
Abstract
Radiotherapy is the standard treatment for glioblastoma (GBM), but the overall survival rate for radiotherapy treated GBM patients is poor. The use of adjuvant and concomitant temozolomide (TMZ) improves the outcome; however, the effectiveness of this treatment varies according to MGMT levels. Herein, we evaluated whether MGMT expression affected the radioresponse of human GBM, GBM stem-like cells (GSCs), and melanoma. Our results indicated a correlation between MGMT promoter methylation status and MGMT expression. MGMT-producing cell lines ACPK1, GBMJ1, A375, and MM415 displayed enhanced radiosensitivity when MGMT was silenced using siRNA or when inhibited by lomeguatrib, whereas the OSU61, NSC11, WM852, and WM266-4 cell lines, which do not normally produce MGMT, displayed reduced radiosensitivity when MGMT was overexpressed. Mechanistically lomeguatrib prolonged radiation-induced γH2AX retention in MGMT-producing cells without specific cell cycle changes, suggesting that lomeguatrib-induced radiosensitization in these cells is due to radiation-induced DNA double-stranded break (DSB) repair inhibition. The DNA-DSB repair inhibition resulted in cell death via mitotic catastrophe in MGMT-producing cells. Overall, our results demonstrate that MGMT expression regulates radioresponse in GBM, GSC, and melanoma, implying a role for MGMT as a target for radiosensitization.
Similar content being viewed by others


Introduction
Glioblastoma (GBM) is the most aggressive subgroup of malignant gliomas. The median survival of patients with GBM treated with surgical resection alone is approximately six months1, and for those treated with the most aggressive combined treatment modalities, including surgery, chemotherapy, and radiotherapy, increases to approximately 14–17 months2. This improvement is partially due to the inclusion of temozolomide (TMZ), an oral alkylating agent, as a concomitant therapy to radiation, acting as a radiation modifier3,4. However, the combination effect of radiation and TMZ on GBM treatment varies, depending on the presence or absence of O6-methylguanine-DNA methyltransferase (MGMT) expression, which is regulated by MGMT promoter methylation status5,6, a known potential predictor of GBM treatment response to TMZ and a major determinant of a patient’s prognosis6.
MGMT is essential for maintaining DNA integrity7 and is a key factor in the mechanism of tumor resistance to alkylating agents8. Alkylating agents are highly reactive molecules that bind to DNA, and the DNA site they most frequently methylate is the O6 position of guanine, which creates O6-methylguanine (O6-meG)9,10. The O6-meG produced under these circumstances has cytotoxic and mutagenic potential11,12. MGMT recognizes the O6-meG base lesion induced by alkylating agents and transfers the methyl adducts from O6-meG to itself, restoring the guanine base; then MGMT is auto-inactivated, ubiquitinated, and degraded13. Through this mechanism, MGMT induces resistance to alkylating agents, so whether MGMT is expressed in tumors can affect the therapeutic effects of alkylating agents alone or in combination with radiation6. MGMT expression is regulated by the methylation of the CpG island within the MGMT promoter rather than gene deletion, mutation, rearrangement, or unstable RNA14,15,16. Thus, methylation-specific PCR (MCP) is frequently used to detect the methylation status within the MGMT promoter, stratifying patients’ tumor samples into MGMT methylated and unmethylated17,18. For reference, MGMT(−) means that there is almost no methylation of the MGMT promoter and the presence of MGMT protein expression, but in the case of MGMT(+), there is methylation of the MGMT promoter and no expression of MGMT protein.
MGMT inhibitors control MGMT expression and activity in the tumor. Because O6-BG, an MGMT inhibitor, can pass through the blood–brain barrier, it has been used in clinical trials as a sensitizer for alkylating agents to the gliomas19. Phase I, II, and III clinical trial results of combination O6-BG and TMZ treatment of cancers, such as brain tumors, melanoma, lymphoma, and colon cancer, indicated that this combination was effective in tumor suppression20,21,22,23. However, it has been reported that O6-BG increases the risk of hydrocephalus, CSF leak, and CSF/brain infection in glioblastoma patients24 and that combination of O6-BG with other glioblastoma treatments (radiation or BCNU) may cause additional toxicity25. Lomeguatrib (O6-BTG), another MGMT inhibitor used in this study, not only efficiently inactivated the in vitro and in vivo MGMT level or activity in various tumors, but also effectively increased tumor sensitivity to TMZ26,27,28,29. Lomeguatrib was recently reported to be effective as a radiosensitizer in GBM cell lines carrying unmethylated MGMT promoters30, but robust studies to define the role of MGMT itself or MGMT inhibitors on radioresponse had not been performed.
In this study, we evaluated the effects of in vitro molecular biological regulation of MGMT in GBM, GSC, and melanoma cell lines and found that MGMT expression differentially regulates the radioresponse of these tumors. In addition, radioresponse regulation via MGMT control in GBM, GSCs, and melanoma was associated with persistence of radiation-induced γH2AX foci and radiation-induced cell death by mitotic catastrophe, suggesting that MGMT is associated with repair of radiation-induced DNA double-strand breaks (DSBs) in GBM, GSCs, and melanoma.
Materials and methods
Cell lines and treatments
We confirm that all methods were carried out in accordance with relevant guidelines and regulations, approved by the NIH safety committee. Adherent glioblastoma cell lines (GBMs [ACPK1 and OSU61]), glioblastoma stem-like cell lines (GSCs [GBMJ1 and NSC11]), and melanoma cell lines (A375, MM415, WM852, and WM266-4) were used in this study. Primary glioblastoma cell lines ACPK1 and OSU61 used in this study were isolated from glioblastoma patient biopsies and authenticated by a neuropathologist at The Ohio State University. These cells were isolated in accordance with The Ohio State University Intuitional Review Boards for IRB (2009C0065 and 2014C0115), and IBC (2009R0169). The neurosphere-forming GBMJ1 and NSC1131 (Dr. Frederick Lang, MD Anderson Cancer Center) cells were maintained in stem cell medium (DMEM/F12), supplemented with B27 (Thermo Fisher Scientific), basic fibroblast growth factor (bFGF), and epidermal growth factor (EGF) (50 ng/ml each, Sigma-Aldrich) at 37℃, 5% CO2. For in vitro experiments, GBMJ1 and NSC11 neurospheres were disaggregated into single-cell suspensions using TryplE Express enzyme (Thermo Fisher Scientific) and seeded onto Biocoat™ poly-l-lysine-coated multi-well plates (Corning) or chamber slides (Sigma-Aldrich). A375, MM415, WM852, and WM266-4 cells were obtained from the ATCC and grown in DMEM (Invitrogen) and RPMI 1640 (Invitrogen) with 10% fetal bovine serum and maintained at 37℃, 5% CO2. Lomeguatrib (O6-BTG) purchased from Selleckchem (Cat. S8056) was reconstituted in DMSO (100 mM) and stored at -20℃. Cells were irradiated as monolayer cultures using an XRad 320 X-ray source (Precision XRay Inc.) at a dose rate of 2.5 Gy/min.
Genomic DNA extraction and methylation-specific PCR analysis
Genomic DNA was isolated using the Monarch Genomic DNA Purification Kit (New England Biolabs), then used for MGMT promoter methylation-specific (MSP) PCR analysis. The DNA was treated with bisulfite using the EZ DNA Methylation-Gold™ Kit (Zymo Research), according to the manufacturer’s instructions. MSP was performed using a nested, two-step approach. The stage-1 PCR products were diluted 50- to 100-fold, then 5 to 10 μl were subjected to stage-2 PCR, using primers specific to the methylated or unmethylated template. Primer sequences used in the stage-1 amplification of MGMT genes32, and primer sequences used to selectively amplify unmethylated or methylated alleles of the MGMT genes in the stage-2 PCR have been previously described33. The PCR products were resolved using 4% low melting point agarose gels.
Reverse transcription PCR and quantitative real-time PCR
Total RNA was isolated using Direct-zol RNA Miniprep Kits (Zymo Research). Reverse transcription PCR (RT-PCR) reactions were performed using the ImProm-II™ Reverse Transcription System (Promega) for 5 min at 25 ℃ for annealing, 60 min at 42 ℃ for extension, and 15 min at 70 ℃ for reverse transcriptase inactivation. MGMT mRNA levels were determined by quantitative real-time PCR (qRT-PCR) using the TaqMan™ Universal Master Mix II, with UNG (Thermo Fisher Scientific) and MGMT Taqman probes (Hs00172470_m1; Thermo Fisher Scientific). The amplification signal of the target gene was normalized to that of GAPDH in the same reaction.
Transient transfection of small interfering RNA
MGMT-specific small, interfering RNA (siRNA) based on the sequence of human MGMT was purchased from Qiagen (FlexiTube siRNA—Hs_MGMT_1): sense5′-CCAGACAGGUGUUAUGGAATT-3′ and antisense 5′-UUCCAUAACACCUGUCUGGTG -3′. MGMT-producing cell lines were transfected with 25 nM si (negative control) and siMGMT in a serum-free medium for overnight incubation using Lipofectamine™ RNAiMAX (Thermo Fisher Scientific) according to the manufacturer’s protocol. Cells were further incubated in the growth medium at 37 ℃ for 48 h. MGMT knockdown of was verified by immunoblot analysis.
Plasmid construction and transfections
Plasmids were constructed via standard recombinant cloning techniques and all changes were verified by DNA sequencing. Human MGMT cDNA (MGMT [untagged]-human O6-methylguanine-DNA methyltransferase_wild type; OriGene [cat # SC322190]) was amplified via PCR and cloned into pcDNA3.1-Flag vectors. The pcDNA3.1-Flag-MGMT vector was generated using primers 5ʹ- TGACAAGCTTATGCTGGGACAGCCCGCGCCCCTAGAA-3ʹ (HindIII) and 5ʹ- TCCGAATTCCTAGTTTCGGCCAGCAGGCGGGGAGCCCGA-3ʹ (EcoRI). MGMT was then inserted between the HindIII and EcoRI restriction sites in pEGFP-N1 vectors. Transfection with these plasmids was performed using Lipofectamine™ 3000 (Thermo Fisher Scientific) in accordance with the manufacturer’s guidelines. MGMT overexpression levels were determined by immunoblot analysis and imaging using a Zeiss upright fluorescent microscope.
Clonogenic assays
ACPK1, A375, and MM415 cells were trypsinized and seeded onto six-well tissue culture plates (50 to 3200 cells per well, depending on the radiation dose). After allowing cells time to attach (16 h), cultures received lomeguatrib for 16 h prior to 1–6 Gy irradiation. The lomeguatrib-containing medium was removed 24 h after irradiation, the cells rinsed, and fresh, drug-free media was added. For GSC analysis, GBMJ1 cells were disaggregated into single-cell suspensions and seeded into poly-l-lysine-coated six-well plates (200 to 6,400 cells per well, depending on the radiation dose). After allowing cells time to attach (16 h), cultures received lomeguatrib (100 µM) for 16 h prior to 1–4 Gy radiation. The lomeguatrib-containing medium was removed 24 h after irradiation, the cells rinsed, and fresh, drug-free media was added. Colonies were stained with 0.1% crystal violet 10 to 12 days after seeding ACPK1, A375, and MM415 cells, or 14 to 21 days after seeding GBMJ1 cells. For OSU61, NSC11, WM852, and WM266-4, clonogenic assays were performed as described above 48 h after transfection with the pEGFP-N1-MGMT vector, but they were not treated with lomeguatrib. The number of colonies containing at least 50 cells were counted and the surviving fractions calculated. Data presented are the mean ± SE from at least three independent experiments.
Flow cytometric analysis of cell cycle
Flow cytometry was used to evaluate the cell cycle phase distribution. The drug treatment protocols used were the same as those described for the clonogenic assays. Following treatment of lomeguatrib for 24 h, cells were harvested at various time points, fixed with 70% ethanol, and stained with propidium iodide (Sigma-Aldrich). DNA content for cell-cycle analysis was determined with a LSR Fortessa™ flow cytometer (BD Biosciences).
Immunoblot analysis
Whole-cell pellets of all cell types were collected in RIPA lysis buffer (Thermo Fisher Scientific) for protein extraction. Total protein was quantified using a BCA protein assay (Thermo Fisher Scientific). Proteins were separated by SDS-PAGE (Mini-Protean TGX™ Gels [Bio-Rad]), transferred to a nitrocellulose membrane (Bio-Rad), and probed with antibodies targeting MGMT (1:1000; abcam [ab108630]), GFP (1:1000; Roche [11814460001]), and β-actin (1:10,000; Cell Signaling [#3700]). Bands were visualized with IR Dye Secondary Antibodies (LI-COR) and quantified using an Odyssey CLx Image System (LI-COR).
Immunofluorescent staining for γH2AX foci and mitotic catastrophe detection
Visualization of γH2AX foci and mitotic catastrophe was performed as described previously34. ACPK1, A375, and MM415 cells were grown on 18 × 18-mm cover glasses and treated with lomeguatrib (100 µM) before irradiation (4 Gy). GBMJ1 cells were grown on 18 × 18-mm cover glasses coated by poly-l-lysine solution (Sigma-Aldrich) and treated with lomeguatrib (50 µM) for 16 h before irradiation (4 Gy). Cells were imaged using a Zeiss upright fluorescent microscope and γH2AX foci were counted in 50 cells per treatment group using Image J. In the case of mitotic catastrophe, nuclear fragmentation was defined as the presence of ≥ 2 lobes within single cells, and 100 cells were scored for each condition. Data presented are the mean ± SEM for three independent experiments. Statistical significance was calculated by Student’s t-test.
Results
MGMT promoter methylation status and MGMT expression is a non-binary function in GBMs and Melanoma
MGMT promoter methylation status35,36 detected using methylation-specific PCR (MSP) shown in Fig. 1A exhibits mixed methylated/unmethylated status for three MGMT(−) GBMs—ACPK1, OSU61, and GBMJ1 cells. The NSC11 MGMT(+) promoter was almost exclusively methylated. Likewise, the two MGMT(−) melanoma cell lines, A375 and MM415, showed mixed methylated/unmethylated results for their promoters. The MGMT(+) melanoma cell lines, WM852 and WM266-4, showed mostly methylated promoters (Fig. 1D). To determine whether the degree of methylation of the MGMT promoter affects the MGMT at translational and transcriptional levels, we performed qRT-PCR and immunoblot analysis on each cell line. As expected, the relative amount of mRNA was proportional to the unmethylated promoter band for both histologies (Fig. 1B and E). Likewise, the amount of protein measured was proportional to the level of mRNA (Fig. 1C and F). These results suggest that MGMT promoter methylation is not a binary function and that MGMT protein level gradations exist within MGMT(−) cells.

MGMT expression levels in GBM, GSCs and melanoma cell lines. (A and D) The methylation-specific PCR (MSP) analyses of the MGMT promoter from GBMs, GSCs, and melanoma cell lines. Note the bands in the unmethylated (U, 93 bp) and methylated (M, 81 bp) lanes for GBM, GSCs, and melanoma cell lines, reflecting the unmethylated/methylated MGMT promoter. Percentages represent the proportion of methylation (M) and unmethylation (U) on the MGMT promoter in each cell line. (B and E) Transcript levels of MGMT mRNA in GBM, GSCs, and melanoma cell lines were determined by qRT-PCR. (C and F) MGMT levels in GBM, GSCs, and melanoma cell lines were determined by immunoblot analysis. Data are the mean ± SEM for three independent experiments.
Silencing MGMT enhances radiosensitivity in GBM and melanoma cells expressing MGMT
To determine whether MGMT expression is related to radioresponse, clonogenic cell survival assays were performed using MGMT-producing cells (ACPK1, GBMJ1, A375, and MM415). MGMT-producing cells were transfected with 25 nM si (negative control) and siMGMT for 48 h before performing clonogenic cell survival assays. Immunoblot analysis showed that siMGMT downregulated MGMT expression in MGMT-producing cells (Figs. 2A and B). Clonogenic cell survival assays of MGMT-producing cells after siMGMT transfection showed an increase in the radiosensitivity of ACPK1, GBMJ1, A375, and MM415 cells, with dose-enhancement factors (DEFs) ranging from 1.32 to 1.4 (Figs. 2C and D). The siRNA concentration we selected was confirmed to have no additional cytotoxicity as measured by a decrease in plating efficiency (PE) of each cell line. Additionally, to exclude off-target effects due to siMGMT, we transfected siMGMT into NSC11, which are non-MGMT-producing cells, and then performed a clonogenic assay, and as a result, we confirmed that siMGMT had no effect on the radioresponse of NSC11 cells (Supplmentary Fig. S3). These data indicate that the depletion of endogenous MGMT by siMGMT increases the radiosensitivity of MGMT-producing cells after irradiation.

The effect of siMGMT on the radioresponse of MGMT-producing cells. (A and B) ACPK1, GBMJ1, A375, and MM415 cells were transfected with or without 25 nM siMGMT for 48 h. MGMT levels were determined by immunoblot analysis. (C and D) ACPK1, GBMJ1, A375, and MM415 cells were transfected with 25 nM of si (negative control) and siMGMT before radiation. Surviving fraction (Log) curves were generated after normalizing for the cytotoxicity generated by siMGMT alone. Data are the mean ± SEM for three independent experiments. * P < 0.05 and ** P < 0.005 by Student’s t-test.
Lomeguatrib inhibits MGMT and enhances the radiosensitivity of MGMT-producing cell lines
Clonogenic survival assays were conducted to determine whether lomeguatrib, an MGMT inhibitor that promotes MGMT degradation through the ubiquitin–proteasome pathway37, increases the radiosensitivity of MGMT-producing cells. MGMT immunoblot analysis was used to determine the lomeguatrib concentration and exposure time required to inhibit MGMT Fig. 3A and B show MGMT-producing cells that were treated with various concentrations of lomeguatrib (25, 50, 100, and 150 µM) for 24 or 48 h, and the results showed a significant reduction in MGMT expression levels 24 h after lomeguatrib treatment. A dose- and time-dependent decrease in MGMT levels was observed at all tested concentrations. Based on these results, clonogenic survival assays of lomeguatrib-treated cells were performed, and, as shown in Figs. 3C and D, the results indicated that treatment with lomeguatrib increased the radiosensitivity of ACPK1, GBMJ1, A375, and MM415 cells, with DEFs at a surviving fraction of 0.1 ranging from 1.38 to 1.77. The lomeguatrib concentration we selected was confirmed to have no cytotoxicity when measured by plating efficiency (PE) of each cell line. These data suggest that inhibition of MGMT using lomeguatrib increased radiosensitivity, recapitulating the siMGMT studies.

The effect of lomeguatrib on radioresponse of MGMT-producing cells. (A and B) ACPK1, GBMJ1, A375, and MM415 cells were treated with a gradient (25 µM, 50 µM, 100 µM, and 150 µM) of lomeguatrib for the indicated times (24 h and 48 h). MGMT levels were determined by immunoblot analysis. (C and D) ACPK1, GBMJ1, A375, and MM415 cells were treated with the designated concentrations of lomeguatrib (ACPK1, A375, and MM415—100 µM and GBMJ1—50 µM) for 16 h before radiation. Surviving fraction (Log) curves were generated after normalizing for the cytotoxicity generated by lomeguatrib alone. * P < 0.05 and ** P < 0.005 by Student’s t-test.
Lomeguatrib increases radiation-induced DNA damage and mitotic catastrophe without affecting the cell cycle in MGMT-producing cell lines
To determine lomeguatrib’s mechanism of radiosensitization of MGMT-producing cells, the presence of γH2AX foci, an indicator of DNA damage38, and its dispersal, which is associated with radiation-induced DNA damage repair39, were evaluated. Cells were treated with lomeguatrib (ACPK1, A375, and MM415 at 100 µmol/L and GBMJ1 at 50 µmol/L) prior to radiation (4 Gy), and γH2AX foci determined at 1 and 24 h post-radiation. As shown in Fig. 4A and supplementary Fig. S2A, when MGMT-producing cells were pretreated with lomeguatrib alone, there was no significant increase in the number of γH2AX foci, indicating that drug treatment alone did not cause DNA damage. Radiation treatment led to a significant increase in the number of γH2AX foci at 1 h, which decreased to background levels by 24 h as the DNA damage was repaired. In each cell line, combined radiation and lomeguatrib treatment resulted in a significantly higher number of foci at 24 h compared to cells receiving only radiation, which is consistent with DNA damage repair inhibition and radiosensitization (Fig. 4A and Supplementary Fig. S4A).

The effect of lomeguatrib on radiation-induced γH2AX foci and mitotic catastrophe in MGMT-producing cells. (A) The quantitative assessment of γH2AX foci per cell at 1 h and 24 h after radiation is shown. Foci were counted in at least 50 cells per experiment and representative histograph images obtained from control, lomeguatrib-only, radiation (4 Gy)-only, and lomeguatrib/radiation combination treatment. Data are the mean ± SEM for three independent experiments, and statistical significance was determined by Student’s t-test. *P < 0.05 and **P < 0.005 (radiation versus lomeguatrib/radiation). (B) The quantitative assessment of nuclear fragmentation per cell at 24 h and 72 h after radiation is shown. Nuclear fragmentation (defined as the presence of two or more distinct lobes within a single cell) was evaluated in at least 100 cells per treatment per experiment and representative histograph images obtained from control cells and cells pretreated with lomeguatrib alone, radiation (4 Gy) alone, and combination treatment of lomeguatrib with radiation. Data are the mean ± SEM for three to four independent experiments. Statistical significance was determined by Student’s t-test. *P < 0.05 and ***P < 0.0005 (radiation versus Lomeguatrib + radiation).
Cell cycle distribution was measured to determine whether the lomeguatrib-induced radiosensitization was due to a redistribution of cells into a more sensitive phase of the cell cycle. As shown in Supplementary Fig. S2, there was essentially no consistent difference in the cell cycle distribution with lomeguatrib treatment alone compared to the control (DMSO) for each cell line. Figure 4A and Supplementary Fig. S2 and S4A suggest that combination treatment with radiation and lomeguatrib can attenuate the cellular repair of radiation-induced DNA damage without redistributing into a more sensitive phase of the cell cycle.
To investigate whether lomeguatrib affected radiation-induced mitotic catastrophe, a common death mechanism in cells with unrepaired DNA-DSBs, immunostaining using α-tubulin was performed. Figure 4B and Supplementary Fig. S4B show that, at 16 or 72 h, the percentage of all cells undergoing mitotic catastrophe after treatment with lomeguatrib alone was insignificant compared to the control. However, there was an increase in the number of lomeguatrib and radiation-treated cells undergoing mitotic catastrophe at 72 h in all cells compared to the irradiation-only cells. Therefore, our data, in combination with previous γH2AX results, suggest that the attenuation of radiation-induced DNA damage repair by lomeguatrib leads to mitotic catastrophe.
Intracellular overexpression of MGMT increases the radioresistance of non-MGMT-producing cells
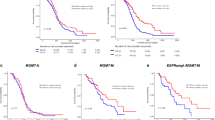
To further define the role of MGMT on radioresponse, MGMT was exogenously added to non-MGMT-producing cells (GBM [OSU61], GSCs [NSC11] and melanoma cells [WM852 and WM266-4]) and assessed using a clonogenic cell survival assay. As shown in Fig. 5A and Supplementary Fig. S5, non-MGMT-producing cells were transfected with 1 µg GFP-MGMT (WT) vector for 48 h, and the immunoblot analysis/histograph results showed that exogenous GFP-MGMT (WT) expression was predominantly localized to the nucleus. As shown in Figs. 5 B and C, transfection with the GFP-MGMT (WT) vector increased the radioresistance of OSU61, NSC11, WM852, and WM266-4 cells with DMFs at a surviving fraction of 0.1, ranging from 1.25 to 1.42. Therefore, our data indicates that overexpression of exogenous MGMT in non-MGMT-producing cells increases the radioresistance of these cells.

The effect of MGMT overexpression on the radioresponse in non-MGMT-producing cells. (A) MGMT protein expression was assessed via western blot analysis following transfection of 1 µg GFP-MGMT vector in non-MGMT-producing cells (OSU61, NSC11, WM852 and WM266-4) for 48 h. (B and C) OSU61, NSC11, WM852 and WM266-4 cells were transfected with 1 µg of GFP-control vector and GFP-MGMT vector before radiation. Surviving fraction (Log) curves were generated after normalizing for the cytotoxicity generated by GFP-MGMT vector alone. DMF values were calculated at a surviving fraction (Log) of 0.1. Data are the mean ± SEM for three independent experiments. * P < 0.05 by Student’s t-test.
Discussion
Radiotherapy in combination with the alkylating agent temozolomide (TMZ) has been the standard treatment for most patients with glioblastoma (GBM) for almost 20 years5. This combination therapy led to a statistically significant improvement in overall survival; however, the absolute effect was only 2.5 m. In a complementary biomarker paper, it was shown that the methylation status was correlated to RT/ TMZ response rate, as patients with a methylated MGMT promotor had a survival benefit compared to those with unmethylated MGMT promotors6. Additionally, it was shown that the methylation status of the MGMT promoter also predicted for survival with irradiation (RT) alone. Of course, because there is no treatment group that did not receive radiation, factors other than the methylation of the MGMT promoter can not be ruled out. However, patients with a methylated MGMT promoter who only received RT survived longer than those patients with unmethylated tumors (15.3 m vs. 11.8 m). Thus, MGMT may play a role in the standard response to irradiation and evaluation of this served as the basis for our study.
Through MSP, qRT-PCR, and immunoblot analysis, we confirmed that there was a correlation between the methylation status of the MGMT promoters in each of our cell lines—GBM (ACPK1 and OSU61), GSCs (GBMJ1 and NSC11), and melanoma (A375, MM415, WM852, and WM266-4)—and their MGMT mRNA and protein expression (Fig. 1). Although there have been reports of mismatches between the methylation status of the MGMT promoter and endogenous MGMT expression40, the methylation status of the MGMT promoter dictates the use of TMZ in brain tumor care. However, our data also showed that the presence of MGMT protein was not binary but showed a variable level within MGMT(−) cell lines. Thus, our cell lines were classified as MGMT-producing (GBM [ACPK1], GSCs [GBMJ1], and melanoma [A375 and MM415]) or non-MGMT-producing (GBM [OSU61], GSCs [NSC11, and melanoma [WM852 and WM266-4]). To evaluate whether in vitro depletion of MGMT in human GBM, GSCs, and melanoma regulated their radioresponse, clonogenic survival assays were performed and showed that the radiosensitivity of each MGMT(−) cell line was significantly different when MGMT was depleted or inhibited. Moreover, we showed an enhancement of radioresistance when exogenous MGMT expression in non-MGMT-producing cells is induced via introducing a GFP-MGMT vector. Together, these results suggest that MGMT protein plays a role in the radioresponse of both glioma and melanoma cell lines.
To translate our findings to the clinic, we used the MGMT inhibitor lomeguatrib. Lomeguatrib treatment of MGMT-producing cell lines did not significantly affect the distribution of cells within the cell cycle and, thus, did not cause a redistribution of cells into a more sensitive phase of the cell cycle. This is consistent with previous work, which showed that lomeguatrib treatment of GBM cell lines and human anaplastic astrocytoma cell lines does not induce specific phase changes in the cell cycle41,42. Next, we evaluated DNA DSB repair by measuring γH2AX foci. γH2AX foci form at DNA DSBs and can be used as a sensitive indicator of DSB formation and repair39,43,44,45. Our study shows the number of γH2AX foci in the MGMT-producing cell line of the lomeguatrib-only treatment group was not different from that of the control group, that there was no difference in the number of γH2AX foci between the radiation-only and combination treatment groups after 1 h of radiation, and that the number of γH2AX foci in the lomeguatrib/radiation combination treatment group of MGMT-producing cell lines was significantly greater at 24 h after radiation than that of individual treatments. These data suggest that lomeguatrib treatment alone does not cause DNA DSB, the combination treatment does not cause more breaks than RT alone, but that the lomeguatrib treatment leads to an inhibition of DSB repair. Additionally, as shown here, lomeguatrib treatment of MGMT-producing cell lines significantly increased radiation-induced mitotic catastrophe. Therefore, we suggest that the cause of the significant increase in radiation-induced radiosensitivity by lomeguatrib treatment of MGMT-producing cell lines is due to non-repaired DNA DSBs leading to cellular death through mitotic catastrophe.
Data availability
All data generated and analyzed in this study are included in the manuscript and its supplementary files.
References
Wilson, T. A., Karajannis, M. A. & Harter, D. H. Glioblastoma multiforme: State of the art and future therapeutics. Surg. Neurol. Int. 5, 64. https://doi.org/10.4103/2152-7806.132138 (2014).
Omuro, A. & DeAngelis, L. M. Glioblastoma and other malignant gliomas: A clinical review. Jama-J. Am. Med. Assoc. 310, 1842–1850. https://doi.org/10.1001/jama.2013.280319 (2013).
Stupp, R. et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC–NCIC trial. Lancet Oncol. 10, 459–466. https://doi.org/10.1016/S1470-2045(09)70025-7 (2009).
Stupp, R. et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New Engl. J. Med. 352, 987–996. https://doi.org/10.1056/NEJMoa0433305 (2005).
Esteller, M. et al. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. New Engl. J. Med. 343, 1350–1354. https://doi.org/10.1056/Nejm200011093431901 (2000).
Hegi, M. E. et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. New Engl. J. Med. 352, 997–1003. https://doi.org/10.1056/NEJMoa043331 (2005).
Gerson, S. L. MGMT: Its role in cancer aetiology and cancer therapeutics. Nat Rev Cancer 4, 296–307. https://doi.org/10.1038/nrc1319 (2004).
Hotta, T. et al. O6-alkylguanine-DNA alkyltransferase activity of human-malignant glioma and its clinical implications. J. Neuro-Oncol. 21, 135–140. https://doi.org/10.1007/Bf01052897 (1994).
Jansens, B. Cancer principles & practice of oncology review. Cancer Forum 35, 70–70 (2011).
Colvin, M. & Hilton, J. Pharmacology of cyclophosphamide and metabolites. Cancer Treat. Rep. 65, 89–95 (1981).
Brennand, J. & Margison, G. P. Reduction of the toxicity and mutagenicity of alkylating-agents in mammalian-cells harboring the Escherichia-Coli alkyltransferase gene. P. Natl. Acad. Sci. USA 83, 6292–6296. https://doi.org/10.1073/pnas.83.17.6292 (1986).
Mitra, G. et al. Molecular analysis of O6-substituted guanine-induced mutagenesis of ras oncogenes. P. Natl. Acad. Sci. USA 86, 8650–8654. https://doi.org/10.1073/pnas.86.22.8650 (1989).
Liu, L. L. & Gerson, S. L. Targeted modulation of MGMT: Clinical implications. Clin. Cancer Res. 12, 328–331. https://doi.org/10.1158/1078-0432.Ccr-05-2543 (2006).
Day, R. S. et al. Defective repair of alkylated DNA by human-tumor and Sv40-transformed human cell strains. Nature 288, 724–727. https://doi.org/10.1038/288724a0 (1980).
Fornace, A. J., Papathanasiou, M. A., Hollander, M. C. & Yarosh, D. B. Expression of the O6-methylguanine-DNA methyltransferase gene MGMT in Mer+ and Mer-human tumor-cells. Cancer Res. 50, 7908–7911 (1990).
Pieper, R. O., Futscher, B. W., Dong, Q., Ellis, T. M. & Erickson, L. C. Comparison of O6-methylguanine DNA methyltransferase (MGMT) messenger-RNA levels in Mer+ and Mer- human tumor-cell lines containing the MGMT gene by the polymerase chain-reaction technique. Cancer Commun. 2, 13–20. https://doi.org/10.3727/095535490820874812 (1990).
Uno, M. et al. Correlation of MGMT promoter methylation status with gene and protein expression levels in glioblastoma. Clinics 66, 1747–1755. https://doi.org/10.1590/s1807-59322011001000013 (2011).
Yachi, K. et al. Relevance of Msp assay for the detection of MGMT promoter hypermethylation in glioblastomas. Neuro-Oncology 11, 944–944 (2009).
Middleton, M. R. & Margison, G. P. Improvement of chemotherapy efficacy by inactivation of a DNA-repair pathway. Lancet Oncol. 4, 37–44. https://doi.org/10.1016/S1470-2045(03)00959-8 (2003).
Quinn, J. A. et al. Phase I trial of temozolomide plus O6-benzylguanine for patients with recurrent or progressive malignant glioma. J. Clin. Oncol. 23, 7178–7187. https://doi.org/10.1200/Jco.2005.06.502 (2005).
Quinn, J. A. et al. Phase I trial of temozolomide plus O6-benzylguanine 5-day regimen with recurrent malignant glioma. Neuro-Oncology 11, 556–561. https://doi.org/10.1215/15228517-2009-007 (2009).
Verbeek, B., Southgate, T. D., Gilham, D. E. & Margison, G. P. O6-methylguanine-DNA methyltransferase inactivation and chemotherapy. Brit. Med. Bull. 85, 17–33. https://doi.org/10.1093/bmb/ldm036 (2008).
Broniscer, A. et al. Phase I trial of single-dose temozolomide and continuous administration of O6-benzylguanine in children with brain tumors: A pediatric brain tumor consortium report. Clin. Cancer Res. 13, 6712–6718. https://doi.org/10.1158/1078-0432.Ccr-07-1016 (2007).
Quinn, J. A. et al. Phase II trial of gliadel plus O6-benzylguanine in adults with recurrent glioblastoma multiforme. Clin. Cancer Res. 15, 1064–1068. https://doi.org/10.1158/1078-0432.CCR-08-2130 (2009).
Blumenthal, D. T. et al. A phase III study of radiation therapy (RT) and O6-benzylguanine + BCNU versus RT and BCNU alone and methylation status in newly diagnosed glioblastoma and gliosarcoma: Southwest oncology group (SWOG) study S0001. Int. J. Clin. Oncol. 20, 650–658. https://doi.org/10.1007/s10147-014-0769-0 (2015).
Barvaux, V. A. et al. Sensitization of a human ovarian cancer cell line to temozolomide by simultaneous attenuation of the Bcl-2 antiapoptotic protein and DNA repair by O6-alkylguanine-DNA alkyltransferase. Mol. Cancer Ther. 3, 1215–1220 (2004).
Turriziani, M. et al. O6-(4-bromothenyl)guanine (PaTrin-2), a novel inhibitor of O6-alkylguanine DNA alkyl-transferase, increases the inhibitory activity of temozolomide against human acute leukaemia cells in vitro. Pharmacol. Res. 53(317), 323. https://doi.org/10.1016/j.phrs.2005.12.001 (2006).
Middleton, M. R. et al. O6-(4-bromothenyl)guanine improves the therapeutic index of temozolomide against A375M melanoma xenografts. Int. J. Cancer 85, 248–252 (2000).
Clemons, M. et al. O6-(4-bromothenyl)guanine reverses temozolomide resistance in human breast tumour MCF-7 cells and xenografts. Brit. J. Cancer 93, 1152–1156. https://doi.org/10.1038/sj.bjc.6602833 (2005).
Kirstein, A., Schilling, D., Combs, S. E. & Schmid, T. E. Lomeguatrib increases the radiosensitivity of MGMT unmethylated human glioblastoma multiforme cell lines. Int. J. Mol. Sci. 22, 6781 (2021).
McCord, A. M., Jamal, M., Williams, E. S., Camphausen, K. & Tofilon, P. J. CD133+ glioblastoma stem-like cells are radiosensitive with a defective DNA damage response compared with established cell lines. Clin. Cancer Res. 15, 5145–5153. https://doi.org/10.1158/1078-0432.Ccr-09-0263 (2009).
Palmisano, W. A. et al. Predicting lung cancer by detecting aberrant promoter methylation in sputum. Cancer Res. 60, 5954–5958 (2000).
Esteller, M., Hamilton, S. R., Burger, P. C., Baylin, S. B. & Herman, J. G. Inactivation of the DNA repair gene O6-methylguanine-DNA methyltransferase by promoter hypermethylation is a common event in primary human neoplasia. Cancer Res. 59, 793–797 (1999).
Lehman, S. L., Schwartz, K. R., Maheshwari, S., Camphausen, K. & Tofilon, P. J. CX-5461 induces radiosensitization through modification of the DNA damage response and not inhibition of RNA polymerase I. Sci. Rep-Uk 12, 4059 (2022).
Pyko, I. V. et al. Glycogen synthase kinase 3 inhibition sensitizes human glioblastoma cells to temozolomide by affecting O-methylguanine DNA methyltransferase promoter methylation via c-Myc signaling. Carcinogenesis 34, 2206–2217. https://doi.org/10.1093/carcin/bgt182 (2013).
Costa, B. M. et al. Prognostic value of MGMT promoter methylation in glioblastoma patients treated with temozolomide-based chemoradiation: A Portuguese multicentre study. Oncol. Rep. 23, 1655–1662. https://doi.org/10.3892/or_00000808 (2010).
Srivenugopal, K. S., Yuan, X. H., Friedman, H. S. & AliOsman, F. Ubiquitination-dependent proteolysis of O6-methylguanine-DNA methyltransferase in human and murine tumor cells following inactivation with O6-benzylguanine or 1,3-bis(2-chloroethyl)-1-nitrosourea. Biochemistry-Us 35, 1328–1334. https://doi.org/10.1021/bi9518205 (1996).
Rogakou, E. P., Pilch, D. R., Orr, A. H., Ivanova, V. S. & Bonner, W. M. DNA double-stranded breaks induce histone H2AX phosphorylation on serine 139. J. Biol. Chem. 273(5858), 5868. https://doi.org/10.1074/jbc.273.10.5858 (1998).
Löbrich, M. et al. γH2AX foci analysis for monitoring DNA double-strand break repair strengths, limitations and optimization. Cell Cycle 9, 662–669. https://doi.org/10.4161/cc.9.4.10764 (2010).
Butler, M. et al. MGMT status as a clinical biomarker in glioblastoma. Trends Cancer 6, 380–391. https://doi.org/10.1016/j.trecan.2020.02.010 (2020).
Taspinar, M. et al. Effect of lomeguatrib-temozolomide combination on MGMT promoter methylation and expression in primary glioblastoma tumor cells. Tumor Biol. 34, 1935–1947. https://doi.org/10.1007/s13277-013-0738-7 (2013).
Ugur, H. C. et al. Chemotherapeutic resistance in anaplastic astrocytoma cell lines treated with a temozolomide-lomeguatrib combination. Mol. Biol. Rep. 41, 697–703. https://doi.org/10.1007/s11033-013-2908-5 (2014).
Costes, S. V., Chiolo, I., Pluth, J. M., Barcellos-Hoff, M. H. & Jakob, B. Spatiotemporal characterization of ionizing radiation induced DNA damage foci and their relation to chromatin organization. Mutat. Res-Rev. Mutat. 704, 78–87. https://doi.org/10.1016/j.mrrev.2009.12.006 (2010).
Rothkamm, K. & Löbrich, M. Evidence for a lack of DNA double-strand break repair in human cells exposed to very low x-ray doses. P. Natl. Acad. Sci. USA 100, 5057–5062. https://doi.org/10.1073/pnas.0830918100 (2003).
Schmid, T. E. et al. Differences in the kinetics of γ-H2AX fluorescence decay after exposure to low and high LET radiation. Int. J. Radiat. Biol. 86, 682–691. https://doi.org/10.3109/09553001003734543 (2010).
Funding
Open access funding provided by the National Institutes of Health. Financial support provided by Intramural Program, National Cancer Institute (ZIA SC 010372) to Kevin Camphausen. NSC11 was provided by the MD Anderson Tumor Research program and developed through the MD Anderson Brain Cancer SPORE (P50CA127001).
Author information
Authors and Affiliations
Contributions
H.S.Y., P.J.T., and K.C. designed the study. H.S.Y. and T.R.K. acquired and analyzed the data. K. P. provided cell lines for the study. H.S.Y., P.J.T., and K.C. wrote the manuscript, and all authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yun, H.S., Kramp, T.R., Palanichamy, K. et al. MGMT inhibition regulates radioresponse in GBM, GSC, and melanoma. Sci Rep 14, 12363 (2024). https://doi.org/10.1038/s41598-024-61240-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-61240-x
- Springer Nature Limited