
Abstract
The associations between people with severe mental illnesses (SMI) and the risks of stroke, suicide, and death remain unclear. We examined healthcare service usage among adults with and without SMI and explored the risk of stroke, suicide, and death. We divided 18–80-year-old adults with SMI into catastrophic and non-catastrophic illness groups. These groups were subjected to a 1:5:5 propensity score matching with people without SMI. Data on demographic characteristics, economic factors, environmental factors, comorbid conditions, self-injury behavior, the number of outpatients and ED visits, and hospitalization were collected. The primary outcomes were risks of stroke, suicide, and death. We included 19,570 people with catastrophic SMI, 97,850 with non-catastrophic SMI, and 97,850 controls. Patients with SMI, especially those with catastrophic illnesses, had higher stroke risk, suicide, and death than those without SMI. People with SMI used health services more frequently than those without SMI. Patients with a history of hospitalization or ED access had a higher risk of stroke, suicide, and death. Our data indicate that special attention should be given to patients with SMI, particularly those with a history of healthcare service utilization, such as through more extended hospital stays with high-intensity interventions.
Similar content being viewed by others


Introduction
People with severe mental illness (SMI), including schizophrenia, bipolar disorder (BD), schizoaffective disorder, and major depressive disorder, have a disproportionately high mortality rate—two to three times that of the general population1,2,3. In Taiwan, these patients have a higher risk of death than the general population and significantly lower life expectancy at birth than the national standard (lower by 11.99–15.53 years in men and 6.83–15.48 years in women) 4, which may be due to natural or unnatural causes. Severe mental disorders are a well-established risk factor for suicidality5. More specifically, the lifetime risk of suicide is as high as 15% in people with affective disorders and 10% in those with schizophrenia. The risk of suicide in people with BD is 20–30 times higher than in the general population6.
Compared with suicide and accidental deaths, most people with SMI die from natural causes similar to those in the general population, including heart disease, cancer, cerebrovascular diseases, and lung and respiratory diseases, contributing the most to their years of lost life7. The findings revealed in the meta-analysis indicate that the elevated risk of premature death in individuals with BD cannot be solely attributed to suicide and unnatural causes; rather, somatic comorbidities also play a significant role 8. These SMI patients have poorer somatic health and often consume more healthcare resources. People with psychotic disorders had high levels of use of health services, both in absolute terms and relative to people without psychotic disorders9. According to a retrospective cohort study based on the population in Scotland, individuals with schizophrenia, BD, or depression exhibited a higher relative risk of stroke compared to those without psychiatric disorders10.
The National Health Insurance (NHI) program in Taiwan, implemented in 1995, provides most healthcare services to nearly 99.96% of the Taiwanese population11. Our objectives were to examine and explore the occurrence and associated factors of stroke, suicide, and mortality in individuals with SMI enrolled in the NHI program, as compared to a control group. Besides, patients who frequently visit the emergency department (ED) have a higher mortality rate than those who visit the ED less than once per year12. Moreover, compared with the general population, not only were people with ED visits more likely to die by suicide, but also were those with hospitalizations13. Hence, we additionally aimed to comprehend the utilization of health services among individuals in the Taiwanese population who experienced stroke, suicide, and mortality.
Results
After 1:5:5 matching, 215,270 patients were included: 19,570 in the catastrophic SMI group, 97,850 in the SMI group, and 97,850 in the control group. Their characteristics are presented in Table 1. The mean age of the three groups was approximately 41 years. The distributions of sex, age groups, and CCI were not statistically different among the three groups after matching. In addition, the SMI groups had lower education levels, a lower proportion of married individuals, and lower incomes. Moreover, compared with the control group, the SMI groups had a higher percentage of patients with self-harm behavior, use of outpatient department (OPD) medical services, emergency services, and hospital admissions.
Table 2 presents the differences among the three groups by bivariate analysis of the log-rank test. Table 3 shows the results of the Cox proportional hazards model. After adjustment for the other variables, the highest risk of stroke was noted in the SMI group (HR = 1.33, 95% CI 1.22–1.45, p < 0.001), followed by the catastrophic SMI group (HR = 1.20, 95% CI 1.06–1.36, p = 0.004). The catastrophic SMI group had the highest risk of suicide (HR = 20.53, 95% CI 15.50–27.19, p < 0.001) and death (HR = 2.60, 95% CI 2.41–2.80, p < 0.001; Table 3) comparing with those without SMI.
According to the variables in the adjusted model (Table 3), women were associated with a lower risk of stroke (HR = 0.53, 95% CI 0.48–0.60, p < 0.001), suicide (HR = 0.38, 95% CI 0.26–0.55, p < 0.001), and death (HR = 0.40, 95% CI 0.37–0.43, p < 0.001). Moreover, a trend of increasing stroke and death risk, but not suicide risk, was observed with an increase in age. Older adults (≥ 65 years) had a 40.39-fold risk of stroke and a 5.25-fold risk of suicide compared with young adults (≤ 24 years).
Compared with people without comorbidities, the higher the CCI, the higher the stroke risk (CCI ≥ 3: HR = 2.24, followed by CCI = 2: HR = 1.79, and CCI = 1: HR = 1.27). After controlling for all other variables, individuals with education levels higher than senior high school had a 0.45–0.6-fold (95% CI 0.41–0.76) lower risk of stroke, suicide, and death. Divorced people had the highest risk of suicide (HR = 1.47, 95% CI 1.24–1.74, p < 0.001) and death (HR = 1.13, 95% CI 1.04–1.22, p = 0.003) compared with other individuals. People whose monthly salary was NT$22,808–28,800 had the highest risk of suicide and death (HR = 1.26, 95% CI 1.11–1.43; HR = 1.17, 95% CI 1.11–1.23) (Table 3).
A history of self-harm was associated with a higher risk of suicide (HR = 3.12, 95% CI 1.72–5.67, p < 0.001). A higher frequency of outpatient visits was associated with a lower risk of death. ED visits and admission also were associated with the risk of stroke, suicide, and death (Table 3). According to the univariate Poisson regression test, the catastrophic SMI group had the highest incidence of stroke, suicide, and death (3.13, 3.05, and 11.94 per 1000 person-years, respectively), followed by the SMI group (2.79, 1.41, and 6.68 per 1000 person-years, respectively; Table 4).
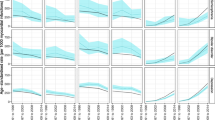
Supplementary Figures A, B, and C present the covariate-adjusted cumulative incidence curves of stroke, suicide, and death among people with SMI compared with the control group according to the Cox proportional hazard model.
Discussion
In the current nationwide cohort study, we observed higher rates of stroke, suicide, and death in patients with SMI than in those without SMI. Patients with SMI with catastrophic illness certificates were at the highest risk. Additionally, people with SMI used health services more frequently than those without SMI. Patients hospitalized or accessed ED services were at higher risk of stroke, suicide, and death. However, patients with higher outpatient use had a lower risk of death, with no effect on stroke and suicide. Our results are similar to another population-based cohort study from New Zealand, which reported an association between psychiatric disorders and self-harm behavior14. Mental disorders were associated with the onset of physical illness, multiple physical illness diagnoses, higher hospitalizations, and early mortality14.
Our data indicated that SMI was associated with a higher risk of stroke, consistent with several studies15,16. A meta-analysis of six cohort studies confirmed a modest but significant positive association between schizophrenia and stroke morbidity and mortality17; patients with BD had a significantly increased risk of stroke18. Numerous mechanisms have been proposed to explain the association between SMI and stroke. For instance, SMI correlates with adverse effects of drug therapy19 and behavioral alterations such as smoking20, inadequate physical activity, and insufficient dietary/caloric intake21. These behavioral changes, in turn, are linked to the etiology of diverse diseases, including diabetes and cardiovascular disease, which could serve as contributors to the occurrence of stroke and premature mortality. In addition, insufficient health care availability22 may increase natural-cause mortality in psychiatric patients. Disparities in mortality rates and reduced life expectancy serve as markers of health inequalities, and people with mental illness do not benefit equally from social and healthcare advancements experienced by the general population23. Because of the NHI program in Taiwan, in our study, patients with SMI had higher rates of medical service use than the controls, indicating no barriers to using medical services. Nonetheless, our data lacks specific information on medical care details and quality. This is our limitation in displaying the purpose of the medical service visit and the service quality. Besides, people with SMI are less likely to receive preventive care services (such as screening for cardiovascular risk factors) and high-quality care than those without SMI24. Moreover, certain research findings suggest challenges for individuals with SMI in effectively managing their chronic conditions25. Schizophrenia is correlated with a diminished likelihood of receiving high-quality diabetes care, contributing to an elevated risk of diabetes-related emergency department visits and hospitalizations26. Notably, there is a notable deficiency in the prescription of various common medications, particularly those addressing cardiovascular issues, in individuals with SMI, including those diagnosed with schizophrenia27. Thus, considerable gaps remain in routine health care for many people with mental illness24. These gaps include physicians focusing on mental illness rather than physical health, inconsistent adherence to health checks and treatment, and poor communication. Patients with SMI tend to have lower socioeconomic backgrounds, which may make it more difficult for them to use medical resources appropriately23. Taiwan’s psychiatric medical care is highly developed and covered under the NHI, enabling people to seek treatment in community psychiatric clinics or hospitals; they can also go to other departments to receive medical treatment for physical diseases. In our study, we found that a relatively high proportion of older patients were first diagnosed with SMI between 2008 and 2011, considering the age at which SMI is most likely to occur. Our research relies on observations sourced from the National Health Insurance database, and the observed phenomenon might be attributed to the substantial time lapse between the onset and formal diagnosis of SMI. Diagnostic delays can stem from various factors, including patients' limited insight or societal taboos discouraging them from seeking medical treatment. Additionally, some instances arise from healthcare professionals downplaying the diagnosis of SMI and instead categorizing milder mental conditions as the primary diagnosis28.
We observed no increased suicide risk in new-onset strokes in patients with SMI. Selective survival and competing causes of death may explain this pattern. Individuals with lower socioeconomic status may die earlier for other reasons so that only the healthiest survive into old age29. It has been suggested that higher rates of selective survival among vulnerable, high-mortality populations lead to higher proportions of healthy older individuals who may have lower suicide rates. Because stroke is more common in old age30, those with SMI surviving into old age who develop stroke may not be at increased suicide risk.
In addition to a high risk of death from natural causes, SMI has also been associated with a higher risk of suicide6,31, consistent with our results. Furthermore, some studies have concluded that older adults have the highest suicide rates32, which also agrees with our data. In our analysis, a CCI score of ≥ 3 was associated with the highest suicide risk, in line with other studies33. Furthermore, consistent with Gallego et al. 34, we observed that a history of suicide attempts was associated with higher suicide rates. This finding has been corroborated by large systematic reviews by Beghi et al.35, 76 studies, and Larkin et al.36, 129 studies. Therefore, patients aged ≥ 65 with SMIs, new arrivals to local mental health services, patients with multiple chronic diseases, divorced or widowed individuals, and those with low education levels should receive multidimensional assistance.
Studies have attempted to predict suicidal behavior from electronic health records. The factors predicting suicide include post-psychiatric hospitalization37, prediction of suicide or accidental death following civilian general hospital discharge38, and prediction of suicide attempt or suicide following outpatient visits. For example, Barak-Corren and colleagues39 used health records data from two large academic health systems to predict suicide attempts or deaths among outpatients with ≥ 3 visits. In our analysis, we observed that suicide cases had a higher rate of ED visits, hospitalization, and previous self-harm records. These characteristics may be helpful for the prediction of suicide in the Taiwanese medical service system.
Given this clinically significant overlap, patients with mental illness should be asked if they have used medical services adequately. It remains unclear what proportion of physical health needs and treatment is unmet in this population compared with individuals without documented mental illness. However, epidemiologic research in community and clinical settings reveals a strong association between mental disorders and increased healthcare service utilization40. Psychiatric disorders are often associated with frequent outpatient services in Taiwan41. Analytical results do not replace clinical judgment, but risk scores can inform individual clinical decision-making and quality improvement plans. Our results may help provide a risk score to help determine risk stratification. We will also suggest further studies related to “mortality risk factors associated with severe mental illnesses” and “reasons associated with emergency department visits and hospitalizations for SMI patients.”
Strengths and limitations
This study used a national population database to avoid selection and participation bias42. Other strengths include the large sample size and number of events and the long follow-up time, which increase the likelihood of finding significance even if the differences are slight; therefore, all results should be interpreted in terms of the clinical importance of the differences and provide strong evidence for understanding possible factors in the real world.
This study has several limitations. First, the NHIRD lacks data on important confounders for increased stroke and mortality, including smoking, dietary habits, and physical activity, precluding the adjustment for these confounders in our regression models. Second, health system records do not reflect crucial social risk factors for suicidal behavior, such as unemployment, bereavement, or relationship breakdown. Suicidal behavior may reflect an interaction of clinical risk factors, adverse life events, and available means of self-harm. Moreover, the monthly income is based on NHI premium–based salary and not actual income data. Third, no information is available on the severity of illness at the time of suicide. The lack of seriousness and clinical status of SMI precludes the determination of the association between mental status and outcome. However, we tried to use the catastrophic disease system to help define severity. Our results are still valid as a reference for clinical care. Fourth, we lack information on substance abuse. The prevalence of comorbidity between SMI and substance use disorder (SUD) is substantial, with estimates indicating that up to 75% of SMI patients also have SUD, and approximately 60% of adults with SUD exhibit some form of SMI. The presence of coexisting disorders is associated with an increased likelihood of adverse health outcomes, suicide, unplanned hospital admissions, and premature mortality43.
Clinical implications
The higher rates of stroke, suicide, and death in our cohort of patients with SMI suggest that special attention should be given to their health and well-being and strategies to improve them. Our data indicate that the higher the ED utilization and hospitalization rate, the higher the risk of suicide, stroke, and death. These findings highlight opportunities to improve both disease and suicide prevention. A significant effort to prevent suicide in all patients with SMI in the ED appears warranted, especially among those with self-harming behaviors, multiple chronic diseases, and high ED utilization. Hospitalization is also a risk of death by suicide compared with people who are not hospitalized. The period of hospitalization provides an opportunity for potentially high-intensity interventions. When dealing with patients with SMI, clinicians should consider more extended hospital stays, which may help initiate high-intensity physical and mental health interventions, before discharging them to outpatient care. Additionally, it is crucial for clinicians to prioritize individuals with high ED and hospitalization utilization, as they may harbor potential SMI cases. Developing a model for case management could aid in enhancing the health condition of these patients and potentially reduce the overutilization of medical services.
Materials and methods
Data sources
This nationwide population-based cohort study used data from Taiwan’s National Health Insurance Research Database (NHIRD)44. In addition, in this study, we used the Longitudinal Health Insurance Database, the Taiwan Cause of Death Statistics, and the Household Registration File managed by the Ministry of the Interior. These databases were provided by the Health and Welfare Data Science Center under the Ministry of Health and Welfare (MOHW). Personally identifiable information was de-identified before its release. Therefore, the collected data comply with personal data protection regulations.
Study population
The data of patients aged 18–80 who received the first diagnosis of SMI between 2008 and 2010 were extracted from the NHIRD. SMI was identified through International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes as follows: at least one instance of hospitalization or ≥ three outpatient visits within 365 days with the diagnosis of depression (ICD-9-CM: 296.2X, 296.3X, 300.4X), BD (ICD-9-CM: 296.XX, excluding 296.2X and 296.3X), or schizophrenia (ICD-9-CM: 295.XX), respectively.
This study divided patients with SMI into catastrophic and non-catastrophic illness groups. The index date for these two groups was the date of the new diagnosis, and that for the control group was the first day of the matching year. The catastrophic illness group comprised patients a physician diagnosed as having a “catastrophic illness” and a catastrophic illness certificate dated between 2008 and 2010. People with serious illnesses who met the National Health Insurance’s definition of catastrophic illnesses as diagnosed by physicians, including 30 categories of patients such as cancers, chronic mental illness, chronic renal failure, type I diabetes, autoimmune disease, congenital factor disorder, stroke, congenital hypothyroidism, etc. Patients with catastrophic illnesses were exempted from copayment and thus avoided financial burden for its long-term health care. Psychiatric conditions such as schizophrenia, schizoaffective disorder, BD, and major depressive disorder may be considered. In cases where a patient exhibits a decline in occupational function, the physician assists them in obtaining a certificate for catastrophic illnesses. Patients with a catastrophic illness certificate receive care for a disease or related condition within the certificate’s validity period, without paying out-of-pocket costs for outpatient or inpatient treatment. However, these patients must follow standard treatment and payment procedures when seeking care for unrelated illnesses45.
For the control group, 3 million cases were randomly selected from the National Health Insurance Beneficiaries File, and those with a primary or secondary diagnosis of SMI from 2000 to 2017 were excluded. To reduce substantial differences in patient characteristics between the three groups, a 1:5:5 propensity score matching was conducted among the catastrophic illness, illness, and control groups year by year according to sex, age, and severity of comorbidities, thereby decreasing the selection bias. A greedy nearest neighbor algorithm was used for matching. In addition, we excluded individuals with a diagnosis of any catastrophic illness other than depression, BD, and schizophrenia, as well as those diagnosed as having cancer or stroke before the index year. The patient selection flowchart is presented in Fig. 1.

Flowchart of patient selection. SMI: severe mental illness (depression, bipolar disorder, or schizophrenia).
Definition of variables
In this study, the following variables were included: (a) Demographic characteristics: sex, age, education level, and marital status. (b) Economic factors: monthly salary divided into seven bands. (c) Environmental factors: urbanization level of the patients’ areas of residence, with the 359 townships, cities, and districts across Taiwan categorized from level 1 (most urban) to level 7 (most rural)46. (d) Comorbid conditions: The comorbidity severity was used as an indicator of health status and was measured using the modified version of the Charlson comorbidity index (CCI) by Deyo et al.47. based on the CCI scores calculated using medical records up to 2 years before the index date, the sample was divided into four groups (0, 1, 2, and ≥ 3). (e) Healthcare service access: We observed some of the medical situations of the research participants in the year before the index date, including self-harm behavior, the number of outpatient visits, the number of ED visits, and the history of hospitalization. The number of outpatient visits was divided into quartiles: ≤ Q1, Q1–Q2, Q2–Q3, and > Q3.
Main outcomes and comorbidities
We analyzed the risk of stroke, suicide, and death in people with SMI from the index date through the end of 2017. Self-harm behavior (ICD-9 codes E950–E959 and ICD-10 codes X60–X84) and comorbidities were defined by their diagnosis within one year before the index date. We also observed whether the patients had a stroke, defined as a primary or secondary diagnosis with the ICD-9 codes 430–437 and ICD-10 codes I60–I67 and G45-G46. Suicide was determined using multiple causes of death with ICD-10 codes X60–X84 and Y870.
Statistical analysis
Descriptive statistics were adopted to describe the socioeconomic status and other control variables. The chi-square test was performed to compare the education level, sex, age, marital status, CCI, and urbanization level of the region of residence among the groups. A log-rank test48 was also used to compare the incidence of stroke, suicide, and death among patients with the catastrophic illness, illness, and control groups. Besides, health conditions, socioeconomic status, and observed medical situations during the year before the index date were also observed. Furthermore, the stratified Cox proportional hazard model was used to explore the risk of stroke, suicide, and death in the three groups after matching after controlling for relevant variables. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. Covariate-adjusted survival curves for stroke, suicide, and death among people with different groups according to the Cox proportional hazard model are presented in the figures. Finally, the between-group differences in the incidence of stroke, suicide, and death per thousand person-years were determined using the univariate Poisson regression test. All statistical analyses were performed using SAS (version 9.4 for Windows; SAS Institute, Cary, NC, USA). A p-value of < 0.05 was considered statistically significant.
Ethics approval and consent to participate
The NHIRD encrypts patient information to protect their privacy and provides researchers with anonymous identification numbers associated with relevant information, including sex, date of birth, medical services received, and prescriptions. Therefore, patient consent is not required to access the NHIRD. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. This retrospective observational study was approved by the Research Ethics Committee of China Medical University Hospital, Taiwan (CMUH109-REC1-016).
Data availability
The data supporting this study’s findings are available from the National Health Insurance Research Database published by the Ministry of Health and Welfare (https://www.mohw.gov.tw/np-108-2.html), Taiwan. Still, restrictions apply to the availability of these data, which were used under license for the current study and are not publicly available. Due to legal regulations imposed by the Taiwanese government related to the Personal Information Protection Act, the database cannot be made publicly available. Furthermore, any raw data are not allowed to be removed from the Health and Welfare Data Science Center. Therefore, the restrictions prohibited the authors from making the minimal data set publicly available. Data are however available from the authors upon reasonable request and with permission of the Health and Welfare Data Science Center, the Ministry of Health and Welfare, Taiwan.
References
De Hert, M. et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry 10, 52–77 (2011).
Laursen, T. M., Musliner, K. L., Benros, M. E., Vestergaard, M. & Munk-Olsen, T. Mortality and life expectancy in persons with severe unipolar depression. J. Affect. Disord. 193, 203–207 (2016).
Walker, E. R., McGee, R. E. & Druss, B. G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiat. 72, 334–341 (2015).
Pan, Y. J., Yeh, L. L., Chan, H. Y. & Chang, C. K. Excess mortality and shortened life expectancy in people with major mental illnesses in Taiwan. Epidemiol. Psychiatr. Sci. 29, e156 (2020).
Fu, X. L. et al. Suicide rates among people with serious mental illness: A systematic review and meta-analysis. Psychol. Med. 53, 351–361 (2023).
Plans, L. et al. Association between completed suicide and bipolar disorder: A systematic review of the literature. J. Affect. Disord. 242, 111–122 (2019).
Colton, C. W. & Manderscheid, R. W. Congruencies in increased mortality rates, years of potential life lost, and causes of death among public mental health clients in eight states. Prev. Chronic Dis. 3, A42 (2006).
Biazus, T. B. et al. All-cause and cause-specific mortality among people with bipolar disorder: A large-scale systematic review and meta-analysis. Mol. Psychiatry 28, 2508–2524 (2023).
Carr, V. J. et al. Patterns of service use among persons with schizophrenia and other psychotic disorders. Psychiatr. Serv. 54, 226–235 (2003).
Jackson, C. A. et al. Incidence of ischaemic heart disease and stroke among people with psychiatric disorders: Retrospective cohort study. Br. J. Psychiatry 217, 442–449 (2020).
National Health Insurance Research Database T. http://nhird.nhri.org.tw/en/index.htm
Gunnarsdottir, O. S. & Rafnsson, V. Mortality of the users of a hospital emergency department. Emerg. Med. J. 23, 269–273 (2006).
Ahmedani, B. K. et al. Variation in patterns of health care before suicide: A population case-control study. Prev. Med. 127, 105796 (2019).
Richmond-Rakerd, L. S., D’Souza, S., Milne, B. J., Caspi, A. & Moffitt, T. E. Longitudinal associations of mental disorders with physical diseases and mortality among 2.3 million New Zealand citizens. JAMA Netw. Open 4, e2033448 (2021).
Bahorik, A. L., Satre, D. D., Kline-Simon, A. H., Weisner, C. M. & Campbell, C. I. Serious mental illness and medical comorbidities: Findings from an integrated health care system. J. Psychosom. Res. 100, 35–45 (2017).
Young, J. Q., Kline-Simon, A. H., Mordecai, D. J. & Weisner, C. Prevalence of behavioral health disorders and associated chronic disease burden in a commercially insured health system: Findings of a case-control study. Gen. Hosp. Psychiatry 37, 101–108 (2015).
Li, M., Fan, Y. L., Tang, Z. Y. & Cheng, X. S. Schizophrenia and risk of stroke: A meta-analysis of cohort studies. Int. J. Cardiol. 173, 588–590 (2014).
Prieto, M. L. et al. Risk of myocardial infarction and stroke in bipolar disorder: A systematic review and exploratory meta-analysis. Acta Psychiatr. Scand. 130, 342–353 (2014).
Mazereel, V., Detraux, J., Vancampfort, D., van Winkel, R. & De Hert, M. Impact of psychotropic medication effects on obesity and the metabolic syndrome in people with serious mental illness. Front. Endocrinol. 11, 573479 (2020).
Itkin, O., Nemets, B. & Einat, H. Smoking habits in bipolar and schizophrenic outpatients in Southern Israel. J. Clin. Psychiatry 62, 269–272 (2001).
Stanley, S. & Laugharne, J. The impact of lifestyle factors on the physical health of people with a mental illness: A brief review. Int. J. Behav. Med. 21, 275–281 (2014).
Laursen, T. M., Munk-Olsen, T., Agerbo, E., Gasse, C. & Mortensen, P. B. Somatic hospital contacts, invasive cardiac procedures, and mortality from heart disease in patients with severe mental disorder. Arch. Gen. Psychiatry 66, 713–720 (2009).
Zabeen, S., Lawn, S., Venning, A. & Fairweather, K. Why do people with severe mental illness have poor cardiovascular health?-The need for implementing a recovery-based self-management approach. Int. J. Environ. Res. Public Health 18, 12556 (2021).
Mitchell, A. J., Malone, D. & Doebbeling, C. C. Quality of medical care for people with and without comorbid mental illness and substance misuse: Systematic review of comparative studies. Br. J. Psychiatry 194, 491–499 (2009).
Druss, B. G. et al. The health and recovery peer (harp) program: A peer-led intervention to improve medical self-management for persons with serious mental illness. Schizophr. Res. 118, 264–270 (2010).
Kurdyak, P. et al. Diabetes quality of care and outcomes: Comparison of individuals with and without schizophrenia. Gen. Hosp. Psychiatry 46, 7–13 (2017).
Mitchell, A. J., Lord, O. & Malone, D. Differences in the prescribing of medication for physical disorders in individuals with v. without mental illness: Meta-analysis. Br. J. Psychiatry 201, 435–443 (2012).
Scott, J. et al. A systematic review and meta-analysis of delayed help-seeking, delayed diagnosis and duration of untreated illness in bipolar disorders. Acta Psychiatr. Scand. 146, 389–405 (2022).
Markides, K. S. & Machalek, R. Selective survival, aging and society. Arch. Gerontol. Geriatr. 3, 207–222 (1984).
Benjamin, E. J. et al. Heart disease and stroke statistics-2018 update: A report from the American heart association. Circulation 137, e67–e492 (2018).
Turecki, G. & Brent, D. A. Suicide and suicidal behaviour. Lancet 387, 1227–1239 (2016).
Raue, P. J., Ghesquiere, A. R. & Bruce, M. L. Suicide risk in primary care: Identification and management in older adults. Curr. Psychiatry Rep. 16, 466 (2014).
Cabello, M. et al. Cross-national prevalence and factors associated with suicide ideation and attempts in older and young-and-middle age people. Aging Ment. Health 24, 1533–1542 (2020).
Gallego, J. A. et al. Predictors of suicide attempts in 3.322 patients with affective disorders and schizophrenia spectrum disorders. Psychiatry Res. 228, 791–796 (2015).
Beghi, M., Rosenbaum, J. F., Cerri, C. & Cornaggia, C. M. Risk factors for fatal and nonfatal repetition of suicide attempts: A literature review. Neuropsychiatr. Dis. Treat. 9, 1725–1736 (2013).
Larkin, C., Di Blasi, Z. & Arensman, E. Risk factors for repetition of self-harm: A systematic review of prospective hospital-based studies. PLoS One 9, e84282 (2014).
Kessler, R. C. et al. Predicting suicides after psychiatric hospitalization in us army soldiers: The army study to assess risk and resilience in servicemembers (army STARRS). JAMA Psychiatry 72, 49–57 (2015).
McCoy, T. H. Jr., Castro, V. M., Roberson, A. M., Snapper, L. A. & Perlis, R. H. Improving prediction of suicide and accidental death after discharge from general hospitals with natural language processing. JAMA Psychiatry 73, 1064–1071 (2016).
Barak-Corren, Y. et al. Predicting suicidal behavior from longitudinal electronic health records. Am. J. Psychiatry 174, 154–162 (2017).
Schmitz, N. & Kruse, J. The relationship between mental disorders and medical service utilization in a representative community sample. Soc. Psychiatry Psychiatr. Epidemiol. 37, 380–386 (2002).
Wang, C., Cheng, S. F., Hung, J. L. & Tang, P. L. Highly frequent utilization of outpatient services in a national health insurance system—analysis of associated factors and underlying co-morbidity. Curr. Med. Res. Opin. 36, 1761–1767 (2020).
Hsing, A. W. & Ioannidis, J. P. Nationwide population science: Lessons from the Taiwan national health insurance research database. JAMA Intern. Med. 175, 1527–1529 (2015).
Alsuhaibani, R., Smith, D. C., Lowrie, R., Aljhani, S. & Paudyal, V. Scope, quality and inclusivity of international clinical guidelines on mental health and substance abuse in relation to dual diagnosis, social and community outcomes: A systematic review. BMC Psychiatry 21, 209 (2021).
Lin, L. Y., Warren-Gash, C., Smeeth, L. & Chen, P. C. Data resource profile: The national health insurance research database (NHIRD). Epidemiol. Health 40, e2018062 (2018).
National Health Insurance Administration MoHaW, Taiwan (ROC): Medical Services Care for Special Groups Patients with Catastrophic Illnesses or Rare Diseases (Accessed 17 January 2022); https://www.nhi.gov.tw/english/Content_List.aspx?n=F5B8E49CB4548C60&topn=1D1ECC54F86E9050
Liu, C.-Y. et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 4, 1–22 (2006).
Deyo, R. A., Cherkin, D. C. & Ciol, M. A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45, 613–619 (1992).
Mantel, N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother. Rep. 50, 163–170 (1966).
Acknowledgements
We appreciate using the National Health Insurance Research Database from the Science Center, the Ministry of Health and Welfare, Taiwan. We are also grateful to Health Data Science Center, China Medical University Hospital, for providing administrative, technical, and funding support.
Funding
This work was partially supported by grants (DMR-107-093; DMR-109-106; DMR-HHC-109-14) from China Medical University Hospital, Taiwan.
Author information
Authors and Affiliations
Contributions
C.-H.L., P.-T.K., and W.-C.T. conceived the study. C.-H.L., C.-S.C., and W.-C.T. designed the study. P.-T.K. and W.-Y.C. performed the data analysis. W.-Y.C. prepared all tables and figures. C.-H.L., C.-S.C., P.-T.K., and W.-C.T. interpreted the results. C.-H.L. and W.-C.T. obtained financial support. C.-H.L. drafted the manuscript. C.-H.L., P.-T.K., and W.-C.T. reviewed the manuscript, and all authors critically revised and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
{kind=link}
Cite this article
Liao, CH., Chang, CS., Kung, PT. et al. Stroke and suicide among people with severe mental illnesses. Sci Rep 14, 4991 (2024). https://doi.org/10.1038/s41598-024-55564-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-55564-x
- Springer Nature Limited