
Abstract
Limited studies are available on vitamin B6 status in domestic cats. To this end, we evaluated glutamate–oxaloacetate transaminase (GOT) activity in hemolysates with and without pyridoxal 5′-phosphate addition in two feline populations: a cohort of 60 healthy, domestic (sexually intact and specific pathogen-free) cats maintained under strictly controlled conditions with appropriate diets housed at the Feline Nutrition and Pet Care Center, and a cohort of 57 cats randomly selected between December 2022 to January 2023 that visited the Veterinary Medicine Teaching Hospital to seek care under different circumstances. The GOT activity expressed as the ratio with and without pyridoxal 5′-phosphate addition (primary activation ratio; PAR) decreased significantly with age in the healthy cohort. The PAR values normalized to age established a cut-off for vitamin B6 deficiency in both cohorts, identifying 17 of 101 animals as vitamin B6 deficient. Using machine learning, a partition-based model (decision tree) was built to identify the most important factors that predicted vitamin B6 deficiency while using the resulting tree to make predictions for new observations. This analysis, performed with all 101 cats, revealed that the diagnosis of an infectious, chronic or acute condition (0.55) was the main contributor, followed by age (0.26), and body condition score (optimal-overweight; 0.19). Thus, our study supports that vitamin B6 supplementation may be indicated in junior to adult animals diagnosed with an infectious, chronic, or acute conditions or healthy cats with body weight ranging from optimal to overweight. In older cats, even if healthy, underweight to optimal cats appear to be at risk of vitamin B6 deficiency.
Similar content being viewed by others

Introduction
The term vitamin B6 refers to six interconvertible compounds that share a 2-methyl-3-hydroxypyridine structure with variable substituents at positions C4 and C5, i.e., pyridoxine (PN), pyridoxamine (PM), pyridoxal (PL), and their phosphorylated derivatives pyridoxine 5′-phosphate (PNP), pyridoxamine 5′-phosphate (PMP) and pyridoxal 5′-phosphate (PLP).
PLP is the coenzyme form of vitamin B6 that is a cofactor in > 160 different catalytic functions, including transamination. Most PLP-dependent enzymes are involved in amino acid metabolism, organic acids, glucose, sphingolipids, and fatty acids, with an essential role in the metabolism of neurotransmitters, such as dopamine, serotonin, glycine, glutamate, γ-aminobutyric acid (GABA)1,2.
In humans, overt vitamin B6 deficiency caused by dietary insufficiency is rare in developed countries since it is present in most foods. Consequently, B6 deficiency occurs in combination with other B vitamins or is linked to some lifestyle habits (contraceptive drugs3, smoking4,5,6,7, alcoholism8,9,10,11) and diseases (celiac disease12, diabetes13,14 or inflammatory conditions15,16,17,18). Secondary vitamin B6 deficiency may result from mutations causing defects in B6 salvage pathways19,20, inborn errors causing accumulation of intermediates that react with PLP, and intake of drugs that reduce the availability of PLP21. In addition, epidemiological human studies reported age-dependent changes in vitamin B6 status, which may reflect differences in B6 metabolism22,23,24,25. Low vitamin B6 intake in humans is associated with an increased risk of age-related diseases7 (e.g., cardiovascular disease26,27,28,29,30 and cancer3,31,32); however, conflicting results have been reported on B6 intake and disease risk33,34. Despite the wealth of studies in humans, only few reports are available on B6 status in domestic pets, including cats.
Twelve studies (8 original research articles), spanning from 1959 to 1998, have focused on the status of vitamin B6 in cats. The first three studies (late 50s to early 60s) showed that vitamin B6 deficiency in cats induces microcytic hypochromic anemia with high serum iron and the development of convulsions and kidney lesions, failure to grow, emaciation, convulsions, anemia, oxalate nephrocalcinosis, and ataxia, and if left on the diet, seizures, and death35,36,37. In vitro, isolated cerebral cortex slices from the deficient animals showed decreased formation of γ-aminobutyric acid and decreased oxygen uptake when glucose was the substrate37. With a gap of almost 28 years, five studies emerged spanning from 1989 to 1998. In growing kittens, vitamin B6 deficiency induced reduced body weight gain, food intake, plasma pyridoxal phosphate, and pyridoxal, hemoglobin, and hematocrit, with elevated urinary oxalate, plasma tyrosine, and plasma cystathionine38. Also, vitamin B6 deficiency in growing kittens resulted in abnormal histopathology, particularly active tubular degeneration and oxalate deposition39. Dietary protein concentrations in growing kittens (as it is in humans, mice and chickens) influenced the B6 requirements: kittens fed a 30% casein diet required 1–2 mg pyridoxine/kg diet38 whereas when fed a 60% casein diet, the requirement was ≥ 2 mg40. A novel expansion of these reports was provided by the finding that brainstem auditory evoked potentials were affected by vitamin B6 deficiency in cats, linking prolonged inter-wave intervals to slowed axonal conduction velocity secondary to defective myelination41. Relevant to species differences (i.e., rat vs. cats), evaluation of PLP-dependent liver tyrosine aminotransferase in cats showed little diurnal variation, no correlation with food deprivation, and a twofold increase in its activity with a high-protein diet vs. a low-protein one, reflecting the key role of this vitamin in protein metabolism. Vitamin B6 deficiency for 9 weeks decreased hepatic tyrosine aminotransferase by 64–75%42.
Thus, no studies reported vitamin B6 status in cats as they age; only the B6 requirement for sustaining growth in kittens37,38,39,40 or maintenance in adults35,36,41,42. In contrast, in humans, it is known that PLP concentrations vary in a sex43,44 and age-dependent manner43,45,46,47,48. As the life expectancy of domestic cats increases, the occurrence of behavioral problems seen in senior cats, such as cognitive dysfunction syndrome, is significant. While the cause of this syndrome is unclear, it has been suggested that it may result from age-related neurodegeneration and defects at the neurotransmission levels, in which vitamin B6 plays a crucial role37,41. Notably, a rigorous meta-analysis revealed no benefit for folate in combination with vitamin B12 and/or B6 dietary supplementation over placebo in elderly human populations with diminished cognitive function secondary to Alzheimer's disease or dementia49. However, the 4 studies that met the eligibility criteria indicate that earlier dietary supplementation is more effective at delaying or decreasing the severity of the cognitive decline or disease risk44.
However, to our knowledge, no thorough vitamin B6 status assessment in cats with age is available, and less so factors that may contribute to vitamin B6 deficiency. This knowledge gap undermines the resources pet owners and clinicians need to make informed decisions regarding dietary supplements and pet food manufacturers' formulation of senior diets.
Based on human studies, we hypothesized that a B6-dependent functional biomarker in readily accessible biological fluids such as blood decreases with age in cats. Erythrocyte PLP content is a more relevant marker of vitamin B6 status than plasma PLP content because the former serves as an intracellular enzymatic cofactor6,50. It is directly correlated with vitamin B6 intake51,52,53, plasma PLP54, PL55,56 and PA52, urinary PA excretion52, and degree of PLP saturation of the erythrocyte aspartate transaminase, responding within weeks to vitamin B6 depletion and repletion52,53,57. Furthermore, erythrocyte PLP content seems a more reliable marker under conditions and diseases associated with inflammation54, altered alkaline phosphatase, and low albumin56. However, assessing the total content of PLP does not address the binding of PLP to the apoenzymes to form a functionally active holoenzyme. The functional category includes evaluating PLP-dependent transaminase activities in tissues42, including red blood cells. Red blood cells are rich in the PLP-dependent glutamate–oxaloacetate transaminase (GOT)58, whose activity responds to changes in vitamin B6 status and in-vitro-supplied PLP48,59. The specific test includes assessing GOT's activity and that induced by the in vitro addition of saturating concentrations of PLP. The results are the primary activation ratio (PAR60) and the specific activity ratio obtained with and without PLP addition. Thus, a higher PAR reflects a lower vitamin B6 status. Advantages of evaluating this ratio include overcoming differences related to various methods and subject variability48,61, in addition to serving as a long-term indicator of vitamin B6 status about the life span of the erythrocytes50 and vitamin B6 intake62. Most importantly, the GOT activity test is not associated with albumin, alkaline phosphatase activity63,64, some immune indices65, and kidney function.
To this end, we evaluated the PLP-dependent GOT activity in hemolysates with and without PLP addition in two feline populations: a cohort of 60 healthy, domestic cats (sexually intact and specific pathogen-free) maintained under strictly controlled conditions with appropriate diets (Feline Nutrition and Pet Care Center, School of Veterinary Medicine, the University of California-Davis, named hereafter as Cat Colony) and a cohort of 57 cats randomly selected between December 2022 to January 2023 that were brought to the Veterinary Medicine Teaching Hospital at the University of California-Davis (VMTH) to seek care under different circumstances with available blood samples (Tables 1, 2). Our second goal was to analyze the data based on the animal's age, sex, body condition score, and clinical condition to elucidate the main factors driving vitamin B6 deficiencies in domestic cats.
Results
Vitamin B6 status in domestic research cats
Blood samples were collected from 47 mostly female, specific-pathogen-free, sexually intact cats (41 females, 6 males) ranging from 1 to 17 y old (Fig. 1A; Table 1). This cohort had an almost equal representation of junior (≤ 2 y; n = 13), adults (3 to 6 y; n = 11), and mature cats (7–10 y; n = 15) with less representation of seniors (11–14 y; n = 7) and geriatric cats (≥ 15 y; n = 1). Although some cats residing at the Cat Colony were positive for feline coronavirus (tested as a part of the routine panel), they were asymptomatic and considered healthy by the standing staff and veterinarians.

Age, sex, and body score condition distribution in domestic cats from the Feline Nutrition and PetCare Center (Cat Colony). (A) Age and sex distribution of the 47 domestic cats from the Cat Colony. (B) Association between body condition score and age in cats. The equation represents the linear fitting; P value is from Pearson's.
To assess the overall fitness status, we used the body condition score. This parameter estimates adipose tissue, similar to the human body mass index66. The scale used in this study spans from 1 (emaciated) to 9 (grossly obese), with a score of 5 being optimal66. The average body condition of this cohort indicated that most cats had a healthy body weight (mean ± SD = 5 ± 1). For those with scores available (n = 42), the body condition score showed a positive association with age without reaching statistical significance (Fig. 1B). The higher body condition score with age may be linked to various medical conditions such as atopic dermatitis, hypertension, diabetes, asthma, ophthalmic diseases, and allergies67; however, all cats at the time of blood withdrawal were healthy with no signs of any of these conditions.
In this healthy cohort, the specific GOT activity (expressed as units/mg protein) was assessed in red blood cell samples with and without the addition of saturating PLP concentrations. First, the experimental data on GOT activities without PLP addition were analyzed by using a stepwise regression to limit regressor effect probabilities, determine the method of selecting effects, begin or stop the selection process, and run a model by including covariates age, BCS, and sex or, if using only females, BCS, and age. The minimum Bayesian Information Criterion (BIC) defined the model selection criteria as the stopping rule. The model was then run using least squares fit with significant terms (Supplementary information). As age was the only one with statistical significance when considering both sexes (P = 0.049) and marginally only with females (P = 0.109), the associations between GOT activities without PLP addition and age were fitted to a linear regression model. The GOT activity without PLP addition with both sexes declined steadily with age from 1 to 17 y (Fig. 2A), whereas upon PLP addition, the significance of the correlation with age was lost with both sexes and females only (Fig. 2B; Supplementary information).

Glutamate–oxaloacetate transaminase specific activity with and without vitamin B6 addition as a function of age. GOT activity was evaluated in hemolysates as described in detail under “Materials and methods” without (A) and with (B) PLP addition. The data are presented as a function of the cat's age. Equations represent the linear fittings, and the P values are from Pearson's. The primary activation ratio (ratio of the GOT-specific activity with and without PLP addition) is shown as a function of age (C).
As the degree of saturation of erythrocytic GOT by PLP is used as a status indicator of B668,69, we calculated the primary activation ratio (the ratio of GOT activity with and without PLP supplementation). As indicated above, with the GOT activities, we performed an analysis based on the best stepwise model followed by the least square one. This analysis indicated that only age was statistically significant when using data from both sexes or females (P < 0.0001; Supplementary information). As such, we used a linear regression model to fit the PAR data with age. The PAR increased linearly with the age of cats (Fig. 2C; P < 0.0001), following a trend similar to that reported for humans (i.e., high in newborns and gradually decreasing throughout the lifespan70,71). The linear regression between PAR and age was still highly significant, with no significant slope changes even with female data only (Supplementary information). The effect of PLP addition on GOT activity in samples from older animals was between 2 and 3 times greater than on the GOT in the younger ones (10 vs. 1 y old). These results are consistent with the incubation of hemolysates with PLP from older subjects, resulting in a greater activation of GOT than in samples from younger subjects, reflecting lower vitamin B6 levels in the blood of elders72,73,74. These reports and the results presented here indicate that PLP is present in red blood cells in suboptimal concentrations for maximal GOT activity.
As described in the “Materials and methods”, the PAR values were corrected for age to establish a cut-off value for identifying vitamin B6 deficiency. Accordingly, values ≥ 1.25 of the age-adjusted mean indicated vitamin B6 deficiency. Under this condition, 6 cats (5 females, one male) were identified as having abnormally high PAR values normalized to age. The age and BCS distributions of these 6 cats indicated that the vitamin B6 deficiency was spread across ages by including two juniors (age; BCS: 1 and 2 y; 4 and 6), one adult (3 y; 5), two mature (7 and 8 y; 5 and 4), and one senior (14 y; 4) with most cats having abnormal BCS values (three underweight and one overweight). Although asymptomatic, three cats were positive for feline covid virus.
Vitamin B6 status in domestic client-owned cats
Blood samples were collected from 54 male (n = 35) and female (n = 19) cats that visited the VMTH for a medical consultation between December 2022 and January 2023, from which blood samples were available ranging from 3 months to 17 y old of age (Fig. 3A; Table 2). This cohort had more males (male-to-female ratio = 1.8 from the VMTH vs. 0.15 from the Cat Colony) and a more comprehensive representation of ages than those at the Cat Colony: junior (1–2 y; n = 7), adults (3 to 6 y; n = 13), mature cats (7–10 y; n = 14), seniors (11–14 y; n = 14) and geriatric cats (≥ 15 y; n = 6). Significantly different from the cohort from the Cat Colony, most animals were not sexually intact (all males were neutered except one, and all females were spayed). The most common diagnosis was chronic kidney disease, followed by lymphoma, heart disease, and hypocobalaminemia (Table 2). The diet of most cats was unknown, but for those with information on dietary habits, most were fed commercially available brands such as Purina, Royal Canin, and Costco (Table 2). Similar to the Cat Colony data (Fig. 1B), the VMTH cohort did not show a statistically significant correlation between body condition scores and age (Fig. 3B).

Age, sex, and body score condition distribution in domestic cats from the Veterinary Medicine Teaching Hospital from Dec 2022–Jan 2023. (A) Age and sex distribution of a subset of 54 domestic cats from all those seen at the VMTH between Dec 2022 and Jan 2023. (B) Association between body condition scores and cat's age. The equation represents the linear fitting.
As described before, the specific GOT activity was assessed in whole blood samples with and without the addition of saturating PLP concentrations. The GOT activities without or with PLP addition did not show a statistically significant correlation with age (Fig. 4A,B). The differences in the y-axis intercept of these plots compared to those obtained with the Cat Colony cohorts reflect the utilization of isolated red blood cells (Cat Colony) vs. whole blood hemolysates (VMTH cohort). Indeed, the ratio of the y-intercepts was in average 2.25 Cat Colony/VMTH cohorts, consistent with the volume of red blood cells to total blood.

Glutamate–oxaloacetate transaminase specific activity with and without vitamin B6 addition as a function of age. GOT activity was evaluated in hemolysates as described in detail under “Materials and methods” without (A) and with (B) PLP addition. The data are presented as a function of the cat's age. Equations represent the linear fittings, and the P values are from Pearson's. The primary activation ratio (ratio of the GOT-specific activity with and without PLP addition) is shown as a function of age (C).
The PAR with the VMTH cohort showed a positive and statistical correlation (Fig. 4C), consistent with the results obtained before with the Cat Colony cohort (Fig. 2C). When the analysis was run separated by sexes, the correlations and slopes were similar (n males = 35, PAR = 9.03 + 0.126 * Age with r2 = 0.313; P = 0.067; n females = 19, PAR = 8.42 + 0.119 * Age, r2 = 0.313, P = 0.192) with a higher significance for males likely due to the larger number of animals. Indeed, a power analysis indicated that at a fixed alpha of 0.05, the power for females was 0.249, whereas that for males was 0.451. These results were not consistent with those of humans, showing a gender effect for PLP levels43.
As described in the “Materials and methods”, the PAR values were corrected for age by using the equation obtained with the healthy Cat Colony cohort. Under this condition, 11 cats (2 spayed females, 8 neutered males, and one sexually intact male) were identified as having abnormally high PAR values normalized to age. This B6 deficient population represented the 20.3% of those tested from the VMTH cohort, as expected, a value lower than that of the Cat Colony cohort (12.8%) but without reaching statistical significance (P = 0.317; Chi-squared test). The age distribution of these 11 cats included 7 juniors (0.25 y, 0.33 y, 0.83 y, three 1-y-old, 2 y), three adults (two 3 y-old, 4 y), and one mature (7 y). In terms of BCS, most cats had abnormal BCS (64%; 3 underweight and 4 overweight).
Contributors to vitamin B6 status in cats
Higher PAR effect may reflect not only poorer vitamin B6 status, but also lower plasma phosphatase activity (activity required to release pyridoxal from PLP for tissue uptake), and lower hepatic albumin secretion (needed for PLP transport) as suggested for humans72,73,74,75. To ascertain whether PLP or other factors were contributors to this effect, we recalculated the data from the Cat Colony and the VMTH (n = 101) in terms of a specific activity ratio (i.e., average specific GOT activity from junior divided by the average specific GOT activity from each age group, namely adults, mature, seniors, and geriatric). The initial specific activity ratio without PLP addition decreased with the addition of PLP (from 2.4 ± 0.2 to 1.2 ± 0.2; Fig. 5A). As the GOT activity from older animals with PLP addition was similar to that of younger animals (ratio close to 1), it was concluded that PLP addition accounts for most differences in enzymatic activities between younger and older animals, precluding a significant role for additional factors (83.3% for PLP, 16.6% to other factors). This result is similar to that reported for humans in which PLP status had a major contribution (77%). However, as in humans, the role of factors other than B6 that accounted for the residual difference in GOT activities cannot be excluded (for humans 23%75).

Characterization of the cats identified as B6-deficient. (A) Differential activation by PLP of GOT from samples obtained from junior (≤ 2 y old) and old (adults, mature, seniors, and geriatric) cats from the Cat Colony and VMTH (n = 101). Data were presented as the ratio of the specific GOT activity (average junior/average adult, average junior/ average senior, average junior/average/senior, and average junior/average geriatric) with and without PLP addition. P-value was obtained from Student's t-test with equal variance. (B) Classification of the 17 cats (11 from VMTH and 6 from the Cat Colony) identified as vitamin B6 deficient based on age and body condition score (BCS). (C) Diseases or conditions diagnosed in the 17 cats identified as vitamin B6 deficient. If a cat was diagnosed with more than one condition, all were included as separate entries.
To explore other putative contributors to the vitamin B6 status in domestic cats, we gathered more information on the 17 cats identified as vitamin B6 deficient (6 from the Cat Colony and 11 from the VMTH) as judged by the age-normalized PAR threshold. The sex distribution in those cats identified as B6 deficient was almost equal (41.2% females and the rest males). These percentages aligned to the distributions already noted in each of the cohorts tested. Based on the body condition scores (Fig. 5B), B6-deficient cats were distributed almost equally across the three categories of BCS (below 5, at 5 or above 5). In terms of age, most cats with vitamin B6 deficiency were the junior-adult age range (9 and 4 or 13 of 17; Fig. 2B). For older cats, those with BCS ranging from underweight to normal were linked to vitamin B6 deficiency.
Changes in vitamin B6 status have been linked to numerous human diseases and conditions. For instance, GOT apoenzyme contents increase in diseases related to necrotic processes, while decreases had been reported following alcohol intake48,61. Low plasma PLP in older human adults is not explained by low dietary vitamin B6 or low protein intake24,76, deficit in absorption, impaired synthesis or retention of PLP in erythrocytes or liver77. However, some78 but not all77,79 studies suggest increased catabolism related or not to age-dependent decreases in albumin and, in particular, with an increase in alkaline phosphatase64,77,80. At the same time, the rise in plasma PA (which may be taken wrongly as increased catabolism) in both older men and women may partly be explained by impaired renal function80. The data from the 17 vitamin B6-deficient cats were analyzed in terms of medical diagnosis (Fig. 5C). As the diagnoses were varied, we used the clustering and classification of the disease’s paradigm developed by Webster et al.81. This analysis indicated that most cats had a chronic disease (58.8%), followed by acute (23.5%), immune (17.6%) and infectious diseases (11.8%).
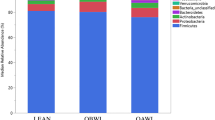
While the analysis of the 17 cats identified as B6-deficient was informative, we turned to use machine learning to build a partition-based model (or decision Tree) to identify the most important factors that predict vitamin B6 deficiency in all 101 cats and use the resulting tree to make predictions for new observations. Essentially a decision tree is a type of supervised machine learning used to categorize or make predictions based on how a previous set of questions were answered. In our case, we used a partition of 60%, 20% and 20% for training, validation (made with stratified sampling) and testing (Fig. 6; Supplementary information). The model is a form of supervised learning, meaning that the model is trained and tested on a set of data that contains the desired categorization (in our case, vitamin B6 deficiency). The model resulted in 5 splits, in which young (junior to adults) with a diagnosis of infectious, chronic or acute were more likely to be vitamin B6 deficient. Within the young and healthy ones, those with body weights from normal to overweight seemed to be more likely to be vitamin B6 deficient. In older animals (mature, senior and geriatric), underweight to normal body weight seemed to play a more prominent role (Fig. 6). In terms of contributions, the main factor influencing vitamin B6 deficiency was the diagnosis of an infectious, chronic or acute condition, followed by age, and BCS. Sex, in contrast to humans, did not seem to be significant with the cohort analyzed.

Decision tree of vitamin B6 deficiency in cats. A decision or partition tree was built by utilizing data from 101 cats. The variables utilized were vitamin B6 status (deficient or DEF and normal), age (either as young or old; young, included junior and adult whereas old included the rest), BCS (optimal or OPT, underweight or UW or overweight OW), diagnosis (healthy, chronic, acute, immune, infectious, other), and sex (female or male regardless of their neutered or spayed status). The feature best split was used which maximized splitting and pruning of the tree branches to prevent overfitting. Complete report is found under the Supplementary information.
Concluding remarks
In this study, and for the first time, a functional biomarker of vitamin B6 status has been obtained from domestic cats and established a clear path to define vitamin B6 deficiency. The PAR declined with age, and by normalizing these values to age, we established a cut-off value that could be used to identify vitamin B6 deficiency. We also identified key contributors to vitamin B6 deficiency for the first time: disease, followed by age and BCS. Current regulatory minimum for B6 in cat foods is 4 mg/kg dry matter or 1 mg/1000 kcal. These amounts are double the NRC minimum requirement for adult maintenance. However, we would like to stress that these values are for healthy, adult cats. As indicated before, for growing, healthy kittens, 1–2 mg and > 2 mg of B6 seemed required for diets with 30% or 60% protein, respectively40. Since our study showed that diagnosis of an infectious, chronic, or acute condition, age, and body condition score seem to affect B6 status in cats, the normalized PAR values may estimate the range of B6 supplementation needed. Given that the average PAR values for those cats deficient in B6 was 1.5 ± 0.2 (n = 17; mean ± SD), then assuming that the PAR is proportional to the deficiency, it would not be unreasonable to suggest a 50% supplementation of B6 in the form of B-complex, or B6 given separately, in junior-adult cats with any of the above mentioned medical conditions or healthy ones with body weights from normal to overweight. Similar to our results, in humans, various chronic diseases were associated with low levels of plasma PLP82, including rheumatoid arthritis, inflammatory bowel disease, cardiovascular disease, deep vein thrombosis, diabetes, and cancer1,14,15,83,84,85,86,87,88,89,90. An inverse relationship was found between the inflammatory marker C-reactive protein and plasma PLP status91,92, the acute-phase protein alpha1-acid glycoprotein, tumor necrosis factor-α, and the proinflammatory cytokine interleukin-6 in rheumatoid arthritis and rheumatoid arthritis and inflammatory bowel disease15,87,93.
In older cats, body weights from normal to underweight seem to be linked to B6 deficiency. Our data suggested that low food intake and/or age-linked malassimilation might play a role in B6 deficiency status based on the increased energy requirements and compromised digestibility in older cats94,95,96 which is linked to a higher proportion of underweight elderly cats with lower body condition scores97. In this regard, the cats from the Cat Colony are fed a diet with appropriate nutrient concentrations (Purina Cat Chow Complete Formula), and no indication of dietary issues was recorded in the VMTH records for the cohort of cats tested.
Our study supports that vitamin B6 dietary supplementation may be indicated in junior to adult animals diagnosed with an infectious, chronic, or acute condition or healthy cats with body weight ranging from optimal to overweight. In older cats, even if healthy, underweight to optimal cats appear to be at risk of vitamin B6 deficiency.
It is important to note the study's limitations: while this report analyzed the largest feline population for vitamin B6 deficiency, the many different medical diagnoses of those from the VMTH made it difficult to identify a specific one. In addition, some of the medical records had limited information in terms of the detailed history of the animals. The content of B6 in diets for those animals at the VMTH was hampered by the proprietary nature of some of the formulations. We also cannot exclude the possible effect of differences in neuter/spay status and sex between the Cat Colony and VMTH. The former had mainly females, none were neutered/spayed, and all were from either a single colony (Cat Colony) or single hospital (VMTH). While a functional biomarker of B6 was informative in identifying B6 deficiency, further research, ideally prospective in nature, would need to be performed to identify the efficacy of specific vitamin B6 supplementation regimens. Finally, further studies are needed to thoroughly characterize both positive and negative clinical effects of B6 supplementation.
Materials and methods
Ethics statement
The ethics of this study was approved by the IACUC (protocol number 21780). All experimental procedures were strictly performed per the ethical requirements of IACUC at the University of California Davis.
ARRIVE guidelines
This study was fully aligned with the ARRIVE 2.0 guidelines98, ensuring transparent and comprehensive reporting of the research methods utilized in this study and its outcomes. Adhering to these guidelines enhances research quality and reproducibility, underscoring our commitment to upholding rigorous standards and promoting transparency in our findings. We confirm that all experiments were performed in accordance with relevant guidelines and regulations.
Animal subjects
The experimental protocol adhered to the Guide for the Care and Use of Laboratory Animals (NRC 1985) and was approved by the Institutional Animal Care and Use Committee (IACUC) of the University of California-Davis. The study population included 60 sexually intact, specific-pathogen-free domestic shorthair cats (Felis catus) aged 1 to 17 y from the Feline Nutrition and Pet Care Center School of Veterinary Medicine, the University of California-Davis (Table 1). Pathogens tested in this cohort included feline calici, herpes, leukemia, and immunodeficiency viruses (all negative). All animals present in the colony between March and July 2021 were included in this study, and these criteria were established a priori. All cats underwent a veterinary examination and were determined to be healthy and able to participate in the study as judged by the standing veterinarians in the facility.
Cats in this facility are housed in large group enclosures with enrichment. Cats were group-housed in large wire cages (2.5 × 2.5 × 2.5 m) in humidity- and temperature-controlled rooms (21 ± 2 °C) with a light: dark cycle of 14 h:10 h. The cats had habitual free access to tap water and a commercially available, balanced, dry expanded diet formulated for all life stages (Purina Cat Chow Complete Formula, Nestle Purina PetCare Company, St. Louis, MO; minimum 1 mg pyridoxine/1000 kcal99). Staff veterinarians evaluated the body condition score with a scale from 1 to 9 and a score of 5 as optimal66.
The other study population included 54 cats aged 3 months to 17 years old brought to the Veterinary Medical Teaching Hospital at the University of California, Davis, between December 2022 and January 2023 to seek care under different circumstances (Table 2). At the hospital, each cat was assessed by various clinicians, technical staff, and veterinary students who took the consultation (assigned by availability and expertise). Thus, all information on the chart of each cat was done by different clinicians specialized in small animal medicine, independently of those at the Cat Colony.
Sample collection
Blood collection across subjects from the Cat Colony was done randomly, and the number of subjects bled/day varied depending on the technician's schedule and workload. Blood collection was adequately performed for most cats while the animal was awake using the appropriate restraint. Restraint was necessary to prevent movement resulting in blood vessel or other organ lacerations and serious complications. Only trained staff performed this procedure by following the criteria to determine the maximum, safe amount of blood to withdraw. The approximate single blood draw was < 5 ml for a 5 kg cat, following the University's IACUC guidelines. This volume represents an estimate depending on the animal's size, health, and hydration status. Cats were not returned to their enclosure until complete hemostasis (i.e., no more blood coming from the collection site as determined using gauze and direct pressure). Up to several minutes of pressure sometimes was required following jugular vein puncture. Collecting blood from the medial saphenous, cephalic, and jugular is recommended for cats. We chose to use the latter site because it does not require anesthesia, and the trained staff have ample experience with this procedure.
Blood samples collected at the VMTH followed standard and approved protocols.
All blood samples from both populations were collected using disposable syringes and needles; samples were transferred into 2‐ml tubes containing K2EDTA (Sarstedt, Nümbrecht, Germany). For measurement of enzymatic activities and protein concentrations, 6 ml of blood was aliquoted into 3 EDTA tubes (2 mL/tube). Blood samples were stored at 4 °C until analysis and were analyzed 7–8 h after phlebotomy. Blood samples were collected in the morning to avoid any putative diurnal cycles. After centrifugation at 3000×g at 4 °C, plasma was removed, and the equivalent 1 ml of packed red blood cells was washed in phosphate-buffered saline three times and suspended in 1 ml of a 1% solution of Triton X‐100 double density, peroxide‐free detergent (Sigma, St. Louis, MO, USA). If needed, washed and permeabilized red cells were stored at − 30 °C for a maximum of 3 months or at − 70 °C for up to 18 months. After homogenization and incubation at 25 °C for 10‐min, the hemolysate was centrifuged at 13,000g for 10 min at 4 °C.
GOT activity assessment
Blood hemolysates (10 µl) were homogenized and diluted 1/100 with 50 mM phosphate buffer (pH 7.5) containing 0.2% bovine albumin and 2 mM K2EDTA. 1/20 with phosphate saline buffer. Each sample was run in duplicates. If values exceeded a coefficient of variation higher than 10%, they were re-assessed. Each sample was tested without and with 20 µM PLP addition. For each of these conditions, a blank and a complete system were run (for a total of 8 wells/sample) in which the "blank" contained 0.1 M Tris–HCl, 0.5 EDTA, 0.2 mM freshly prepared NADH, 10 µM l-aspartate (pH 8.0), and 10 mU malate dehydrogenase. In contrast, the complete system had 4–5 µl of diluted hemolysates. The decrease in absorbance at 340 nm was followed for 15 min in a Tecan Microplate reader at 37 °C. The blank rates were subtracted from those rates with hemolysates. All reagents were of analytical grade and obtained from Sigma Chemical Company. The assay of this enzyme followed essentially that published by Buetler100. The following parameters and ratios were calculated for each blood sample: the GOT activity with and without addition of PLP was expressed in units of enzymatic activity per mg protein (1 U = 1 µmol × min−1) and calculated as [ΔAbs 340 nm/min × (6.22 µmol/ml)−1] = µmol/min × (ml)−1 × (mg of protein × ml−1)−1 = U/mg. The primary activation ratio (PAR) is the ratio of the activity in the presence of a given PLP concentration (saturating) to that in the absence of added PLP. Protein determination was performed using the bicinchoninic acid method (Pierce™BCA protein assay kit, catalog #23225).
Considering that the PAR values correlated with age, the mean PAR values were corrected for age to result in cut-off values used to identify marginal vitamin B6 deficiency. Since the PAR values normalized to age followed a normal distribution (Supplementary information), 1.65 × SD results in a tail that gives a probability of 5% of the data being excluded from the distribution. If this value is added to the mean, anything above this value has a < 5% probability of being significant.
Statistical analyses
Enzymatic activities were assessed in technical triplicates. Descriptive statistics were generated for each parameter and analyzed for normality by the Kolmogorov‐Smirnov test. For all analyses, P ≤ 0.05 was considered significant. Data from GOT activities and PAR were analyzed by using the Fit Model feature under JMP Pro software (version 17.0.0), selecting stepwise regression and using as covariates age, BCS, and sex or if using only one sex, BCS, and age. The model selection criteria were defined by the minimum Bayesian Information Criterion (BIC) as the stopping rule. Then the model was then run using least squares fit (Supplementary information). The decision tree was run as a partition-based model and utilizing a 60:20:20 for the training, validation (stratified sampling) and testing as indicated under Supplementary information.
Data availability
All data generated and analyzed in this study are included in the published article.
References
Friso, S. et al. Low plasma vitamin B-6 concentrations and modulation of coronary artery disease risk. Am. J. Clin. Nutr. 79, 992–998. https://doi.org/10.1093/ajcn/79.6.992 (2004).
Zempleni, J. Pharmacokinetics of vitamin B6 supplements in humans. J. Am. Coll. Nutr. 14, 579–586. https://doi.org/10.1080/07315724.1995.10718546 (1995).
Luhby, A. L. et al. Vitamin B 6 metabolism in users of oral contraceptive agents. I. Abnormal urinary xanthurenic acid excretion and its correction by pyridoxine. Am. J. Clin. Nutr. 24, 684–693. https://doi.org/10.1093/ajcn/24.6.684 (1971).
Shaper, A. G., Wannamethee, S. G. & Whincup, P. H. Serum albumin and risk of stroke, coronary heart disease, and mortality: The role of cigarette smoking. J. Clin. Epidemiol. 57, 195–202. https://doi.org/10.1016/j.jclinepi.2003.07.001 (2004).
Ulvik, A. et al. Long- and short-term effects of tobacco smoking on circulating concentrations of B vitamins. Clin. Chem. 56, 755–763. https://doi.org/10.1373/clinchem.2009.137513 (2010).
Vermaak, W. J. et al. Vitamin B-6 nutrition status and cigarette smoking. Am. J. Clin. Nutr. 51, 1058–1061. https://doi.org/10.1093/ajcn/51.6.1058 (1990).
Walmsley, C. M., Bates, C. J., Prentice, A. & Cole, T. J. Relationship between cigarette smoking and nutrient intakes and blood status indices of older people living in the UK: Further analysis of data from the National Diet and Nutrition Survey of people aged 65 years and over, 1994/95. Public Health Nutr. 2, 199–208. https://doi.org/10.1017/s1368980099000257 (1999).
Beulens, J. W. et al. Kinetics of homocysteine metabolism after moderate alcohol consumption. Alcohol Clin. Exp. Res. 29, 739–745. https://doi.org/10.1097/01.alc.0000163507.76773.1a (2005).
Cravo, M. L. et al. Hyperhomocysteinemia in chronic alcoholism: Correlation with folate, vitamin B-12, and vitamin B-6 status. Am. J. Clin. Nutr. 63, 220–224. https://doi.org/10.1093/ajcn/63.2.220 (1996).
Gloria, L. et al. Nutritional deficiencies in chronic alcoholics: Relation to dietary intake and alcohol consumption. Am. J. Gastroenterol. 92, 485–489 (1997).
Medici, V. et al. Impaired homocysteine transsulfuration is an indicator of alcoholic liver disease. J. Hepatol. 53, 551–557. https://doi.org/10.1016/j.jhep.2010.03.029 (2010).
Merrill, A. H. Jr. & Henderson, J. M. Diseases associated with defects in vitamin B6 metabolism or utilization. Annu. Rev. Nutr. 7, 137–156. https://doi.org/10.1146/annurev.nu.07.070187.001033 (1987).
Masse, P. G., Boudreau, J., Tranchant, C. C., Ouellette, R. & Ericson, K. L. Type 1 diabetes impairs vitamin B(6) metabolism at an early stage of women’s adulthood. Appl. Physiol. Nutr. Metab. 37, 167–175. https://doi.org/10.1139/h11-146 (2012).
Friedman, A. N., Hunsicker, L. G., Selhub, J. & Bostom, A. G. Clinical and nutritional correlates of C-reactive protein in type 2 diabetic nephropathy. Atherosclerosis 172, 121–125. https://doi.org/10.1016/j.atherosclerosis.2003.09.011 (2004).
Roubenoff, R. et al. Abnormal vitamin B6 status in rheumatoid cachexia. Association with spontaneous tumor necrosis factor alpha production and markers of inflammation. Arthritis Rheum. 38, 105–109. https://doi.org/10.1002/art.1780380116 (1995).
Oxenkrug, G. F. Interferon-gamma-inducible kynurenines/pteridines inflammation cascade: Implications for aging and aging-associated psychiatric and medical disorders. J. Neural Transm. 118, 75–85. https://doi.org/10.1007/s00702-010-0475-7 (2011).
Chiang, E. P., Bagley, P. J., Selhub, J., Nadeau, M. & Roubenoff, R. Abnormal vitamin B(6) status is associated with severity of symptoms in patients with rheumatoid arthritis. Am. J. Med. 114, 283–287. https://doi.org/10.1016/s0002-9343(02)01528-0 (2003).
Selhub, J. et al. Dietary vitamin B6 intake modulates colonic inflammation in the IL10−/− model of inflammatory bowel disease. J. Nutr. Biochem. 24, 2138–2143. https://doi.org/10.1016/j.jnutbio.2013.08.005 (2013).
Hazra, A. et al. Genome-wide significant predictors of metabolites in the one-carbon metabolism pathway. Hum. Mol. Genet. 18, 4677–4687. https://doi.org/10.1093/hmg/ddp428 (2009).
Tanaka, T. et al. Genome-wide association study of vitamin B6, vitamin B12, folate, and homocysteine blood concentrations. Am. J. Hum. Genet. 84, 477–482. https://doi.org/10.1016/j.ajhg.2009.02.011 (2009).
Linnet, K., Bossuyt, P. M., Moons, K. G. & Reitsma, J. B. Quantifying the accuracy of a diagnostic test or marker. Clin. Chem. 58, 1292–1301. https://doi.org/10.1373/clinchem.2012.182543 (2012).
Fabian, E., Bogner, M., Kickinger, A., Wagner, K. H. & Elmadfa, I. Vitamin status in elderly people in relation to the use of nutritional supplements. J. Nutr. Health Aging 16, 206–212. https://doi.org/10.1007/s12603-011-0159-5 (2012).
Rose, C. S. et al. Age differences in vitamin B6 status of 617 men. Am. J. Clin. Nutr. 29, 847–853. https://doi.org/10.1093/ajcn/29.8.847 (1976).
Bates, C. J., Pentieva, K. D., Prentice, A., Mansoor, M. A. & Finch, S. Plasma pyridoxal phosphate and pyridoxic acid and their relationship to plasma homocysteine in a representative sample of British men and women aged 65 years and over. Br. J. Nutr. 81, 191–201. https://doi.org/10.1017/S0007114599000380 (1999).
Bor, M. V. et al. Plasma vitamin B6 vitamers before and after oral vitamin B6 treatment: A randomized placebo-controlled study. Clin. Chem. 49, 155–161. https://doi.org/10.1373/49.1.155 (2003).
Rose, R. C. et al. Transport and metabolism of vitamins. Fed. Proc. 45, 30–39 (1986).
Kang-Yoon, S. A., Kirksey, A., Giacoia, G. P. & West, K. D. Vitamin B-6 adequacy in neonatal nutrition: Associations with preterm delivery, type of feeding, and vitamin B-6 supplementation. Am. J. Clin. Nutr. 62, 932–942. https://doi.org/10.1093/ajcn/62.5.932 (1995).
Pedersen, E. R. et al. Urinary excretion of kynurenine and tryptophan, cardiovascular events, and mortality after elective coronary angiography. Eur. Heart J. 34, 2689–2696. https://doi.org/10.1093/eurheartj/eht264 (2013).
Rimm, E. B. et al. Folate and vitamin B6 from diet and supplements in relation to risk of coronary heart disease among women. JAMA 279, 359–364. https://doi.org/10.1001/jama.279.5.359 (1998).
Pawlak, K., Domaniewski, T., Mysliwiec, M. & Pawlak, D. The kynurenines are associated with oxidative stress, inflammation and the prevalence of cardiovascular disease in patients with end-stage renal disease. Atherosclerosis 204, 309–314. https://doi.org/10.1016/j.atherosclerosis.2008.08.014 (2009).
Johansson, M. et al. Serum B vitamin levels and risk of lung cancer. JAMA 303, 2377–2385. https://doi.org/10.1001/jama.2010.808 (2010).
Theodoratou, E. et al. Dietary vitamin B6 intake and the risk of colorectal cancer. Cancer Epidemiol. Biomark. Prev. 17, 171–182. https://doi.org/10.1158/1055-9965.EPI-07-0621 (2008).
van den Berg, H., van der Gaag, M. & Hendriks, H. Influence of lifestyle on vitamin bioavailability. Int. J. Vitam. Nutr. Res. 72, 53–59. https://doi.org/10.1024/0300-9831.72.1.53 (2002).
Carter, T. C. et al. Common Variants at Putative Regulatory Sites of the Tissue Nonspecific Alkaline Phosphatase Gene Influence Circulating Pyridoxal 5'-Phosphate Concentration in Healthy Adults. J. Nutr. 145, 1386–1393. https://doi.org/10.3945/jn.114.208769 (2015).
Dasilva, A. C. et al. The domestic cat as a laboratory animal for experimental nutrition studies. 7. Pyridoxine deficiency. J. Nutr. 68, 213 (1959).
Gershoff, S. N., Faragalla, F. F., Nelson, D. A. & Andrus, S. B. Vitamin B6 deficiency and oxalate nephrocalcinosis in the cat. Am. J. Med. 27, 72–80. https://doi.org/10.1016/0002-9343(59)90062-2 (1959).
McKhann, G. M., Mickelsen, O. & Tower, D. B. Oxidative metabolism of incubated cerebral cortex slices from pyridoxine-deficient kittens. Am. J. Physiol. 200, 34–38. https://doi.org/10.1152/ajplegacy.1961.200.1.34 (1961).
Bai, S. C., Sampson, D. A., Morris, J. G. & Rogers, Q. R. Vitamin B-6 requirement of growing kittens. J. Nutr. 119, 1020–1027. https://doi.org/10.1093/jn/119.7.1020 (1989).
Blanchard, P. C., Bai, S. C., Rogers, Q. R. & Morris, J. G. Pathology associated with vitamin B-6 deficiency in growing kittens. J. Nutr. 121, S77-78. https://doi.org/10.1093/jn/121.suppl_11.S77 (1991).
Bai, S. C., Sampson, D. A., Morris, J. G. & Rogers, Q. R. The level of dietary protein affects the vitamin B-6 requirement of cats. J. Nutr. 121, 1054–1061. https://doi.org/10.1093/jn/121.7.1054 (1991).
Buckmaster, P. S., Holliday, T. A., Bai, S. C. & Rogers, Q. R. Brainstem auditory evoked potential interwave intervals are prolonged in vitamin B-6-deficient cats. J. Nutr. 123, 20–26. https://doi.org/10.1093/jn/123.1.20 (1993).
Bai, S. C., Rogers, Q. R., Wong, D. L., Sampson, D. A. & Morris, J. G. Vitamin B-6 deficiency and level of dietary protein affect hepatic tyrosine aminotransferase activity in cats. J. Nutr. 128, 1995–2000. https://doi.org/10.1093/jn/128.11.1995 (1998).
Gonzalez-Gross, M. et al. Gender and age influence blood folate, vitamin B12, vitamin B6, and homocysteine levels in European adolescents: The Helena Study. Nutr. Res. 32, 817–826. https://doi.org/10.1016/j.nutres.2012.09.016 (2012).
Kerr, M. A. et al. Folate, related B vitamins, and homocysteine in childhood and adolescence: Potential implications for disease risk in later life. Pediatrics 123, 627–635. https://doi.org/10.1542/peds.2008-1049 (2009).
Al-Tahan, J., Gonzalez-Gross, M. & Pietrzik, K. B-vitamin status and intake in European adolescents. A review of the literature. Nutr. Hosp. 21, 452–465 (2006).
Bates, C. J., Mansoor, M. A., Gregory, J., Pentiev, K. & Prentice, A. Correlates of plasma homocysteine, cysteine and cysteinyl-glycine in respondents in the British National Diet and Nutrition Survey of young people aged 4–18 years, and a comparison with the survey of people aged 65 years and over. Br. J. Nutr. 87, 71–79. https://doi.org/10.1079/bjn2001479 (2002).
Joosten, E. et al. Metabolic evidence that deficiencies of vitamin B-12 (cobalamin), folate, and vitamin B-6 occur commonly in elderly people. Am. J. Clin. Nutr. 58, 468–476. https://doi.org/10.1093/ajcn/58.4.468 (1993).
Spinneker, A. et al. Vitamin B6 status, deficiency and its consequences—An overview. Nutr. Hosp. 22, 7–24 (2007).
Zhang, D. M., Ye, J. X., Mu, J. S. & Cui, X. P. Efficacy of vitamin B supplementation on cognition in elderly patients with cognitive-related diseases. J. Geriatr. Psychiatry Neurol. 30, 50–59. https://doi.org/10.1177/0891988716673466 (2017).
Leklem, J. E. Vitamin B-6: A status report. J. Nutr. 120(Suppl 11), 1503–1507. https://doi.org/10.1093/jn/120.suppl_11.1503 (1990).
Hansen, C. M., Leklem, J. E. & Miller, L. T. Changes in vitamin B-6 status indicators of women fed a constant protein diet with varying levels of vitamin B-6. Am. J. Clin. Nutr. 66, 1379–1387. https://doi.org/10.1093/ajcn/66.6.1379 (1997).
Hansen, C. M., Shultz, T. D., Kwak, H. K., Memon, H. S. & Leklem, J. E. Assessment of vitamin B-6 status in young women consuming a controlled diet containing four levels of vitamin B-6 provides an estimated average requirement and recommended dietary allowance. J. Nutr. 131, 1777–1786. https://doi.org/10.1093/jn/131.6.1777 (2001).
Huang, Y. C., Chen, W., Evans, M. A., Mitchell, M. E. & Shultz, T. D. Vitamin B-6 requirement and status assessment of young women fed a high-protein diet with various levels of vitamin B-6. Am. J. Clin. Nutr. 67, 208–220. https://doi.org/10.1093/ajcn/67.2.208 (1998).
Talwar, D. et al. Optimisation and validation of a sensitive high-performance liquid chromatography assay for routine measurement of pyridoxal 5-phosphate in human plasma and red cells using pre-column semicarbazide derivatisation. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 792, 333–343. https://doi.org/10.1016/s1570-0232(03)00320-9 (2003).
Talwar, D. et al. Pyridoxal phosphate decreases in plasma but not erythrocytes during systemic inflammatory response. Clin. Chem. 49, 515–518. https://doi.org/10.1373/49.3.515 (2003).
Vasilaki, A. T. et al. Relation between pyridoxal and pyridoxal phosphate concentrations in plasma, red cells, and white cells in patients with critical illness. Am. J. Clin. Nutr. 88, 140–146. https://doi.org/10.1093/ajcn/88.1.140 (2008).
Quasim, T. et al. The relationship between plasma and red cell B-vitamin concentrations in critically-ill patients. Clin. Nutr. 24, 956–960. https://doi.org/10.1016/j.clnu.2005.06.004 (2005).
Kretsch, M. J., Sauberlich, H. E., Skala, J. H. & Johnson, H. L. Vitamin B-6 requirement and status assessment: Young women fed a depletion diet followed by a plant- or animal-protein diet with graded amounts of vitamin B-6. Am. J. Clin. Nutr. 61, 1091–1101. https://doi.org/10.1093/ajcn/61.4.1091 (1995).
Cheng, C. H., Chang, S. J., Lee, B. J., Lin, K. L. & Huang, Y. C. Vitamin B6 supplementation increases immune responses in critically ill patients. Eur. J. Clin. Nutr. 60, 1207–1213. https://doi.org/10.1038/sj.ejcn.1602439 (2006).
Heiskanen, K., Siimes, M. A., Perheentupa, J. & Salmenpera, L. Reference ranges for erythrocyte pyridoxal 5′-phosphate concentration and the erythrocyte aspartate transaminase stimulation test in lactating mothers and their infants. Am. J. Clin. Nutr. 59, 1297–1303. https://doi.org/10.1093/ajcn/59.6.1297 (1994).
Nath, R. Pyridoxine-vitamin B6. Health and Disease Role of Micro Nutrients and Trace Elements, 85–97 (2000).
Chang, S. J., Hsiao, L. J., Lee, Y. C. & Hsuen, S. Y. Vitamin B6 status assessment in relation to dietary intake in high school students aged 16–18 years. Br. J. Nutr. 97, 764–769. https://doi.org/10.1017/S0007114507665167 (2007).
Brussaard, J. H., Lowik, M. R., van den Berg, H., Brants, H. A. & Bemelmans, W. Dietary and other determinants of vitamin B6 parameters. Eur. J. Clin. Nutr. 51(Suppl 3), S39-45 (1997).
Brussaard, J. H., Lowik, M. R., van den Berg, H., Brants, H. A. & Kistemaker, C. Micronutrient status, with special reference to vitamin B6. Eur J Clin Nutr 51(Suppl 3), S32-38 (1997).
Huang, S. C., Wei, J. C., Lin, P. T., Wu, D. J. & Huang, Y. C. Plasma pyridoxal 5′-phosphate is not associated with inflammatory and immune responses after adjusting for serum albumin in patients with rheumatoid arthritis: A preliminary study. Ann. Nutr. Metab. 60, 83–89. https://doi.org/10.1159/000336175 (2012).
Laflamme, D. Development and validation of a body condition score system for cats: A clinical tool. Feline Pract. 25, 13–18 (1997).
Teng, K. T. et al. Associations of body condition score with health conditions related to overweight and obesity in cats. J. Small Anim. Pract. https://doi.org/10.1111/jsap.12905 (2018).
Li, J. H., Cragoe, E. J. Jr. & Lindemann, B. Structure-activity relationship of amiloride analogs as blockers of epithelial Na channels: I. Pyrazine-ring modifications. J. Membr. Biol. 83, 45–56. https://doi.org/10.1007/BF01868737 (1985).
Nakano, H., McMahon, L. G. & Gregory, J. F. 3rd. Pyridoxine-5′-beta–glucoside exhibits incomplete bioavailability as a source of vitamin B-6 and partially inhibits the utilization of co-ingested pyridoxine in humans. J. Nutr. 127, 1508–1513. https://doi.org/10.1093/jn/127.8.1508 (1997).
Kretsch, M. J., Sauberlich, H. E. & Newbrun, E. Electroencephalographic changes and periodontal status during short-term vitamin B-6 depletion of young, nonpregnant women. Am. J. Clin. Nutr. 53, 1266–1274. https://doi.org/10.1093/ajcn/53.5.1266 (1991).
O’Leary, F., Flood, V. M., Petocz, P., Allman-Farinelli, M. & Samman, S. B vitamin status, dietary intake and length of stay in a sample of elderly rehabilitation patients. J. Nutr. Health Aging 15, 485–489. https://doi.org/10.1007/s12603-010-0330-4 (2011).
Hamfelt, A. Age variation of vitamin B6 metabolism in man. Clin. Chim. Acta 10, 48–54. https://doi.org/10.1016/0009-8981(64)90214-1 (1964).
Hamfelt, A. The effect of pyridoxal phosphate on the aminotransferase assay in blood. Scand. J. Clin. Lab. Investig. Suppl. 18(Suppl 92), 181–188 (1966).
Hamfelt, A. Pyridoxal phosphate concentration and aminotransferase activity in human blood cells. Clin. Chim. Acta 16, 19–28. https://doi.org/10.1016/0009-8981(67)90264-1 (1967).
Fischer, I. & Walter, H. Differential activation by pyridoxal phosphate of aspartate aminotransferase from young and old human erythrocytes. Biochim. Biophys. Acta 184, 660–663. https://doi.org/10.1016/0304-4165(69)90287-6 (1969).
Lowik, M. R. et al. Dose-response relationships regarding vitamin B-6 in elderly people: A nationwide nutritional survey (Dutch Nutritional Surveillance System). Am. J. Clin. Nutr. 50, 391–399. https://doi.org/10.1093/ajcn/50.2.391 (1989).
Kant, A. K., Moser-Veillon, P. B. & Reynolds, R. D. Effect of age on changes in plasma, erythrocyte, and urinary B-6 vitamers after an oral vitamin B-6 load. Am. J. Clin. Nutr. 48, 1284–1290. https://doi.org/10.1093/ajcn/48.5.1284 (1988).
Lee, C. M. & Leklem, J. E. Differences in vitamin B6 status indicator responses between young and middle-aged women fed constant diets with two levels of vitamin B6. Am. J. Clin. Nutr. 42, 226–234. https://doi.org/10.1093/ajcn/42.2.226 (1985).
Pannemans, D. L., van den Berg, H. & Westerterp, K. R. The influence of protein intake on vitamin B-6 metabolism differs in young and elderly humans. J. Nutr. 124, 1207–1214. https://doi.org/10.1093/jn/124.8.1207 (1994).
Bates, C. J., Pentieva, K. D. & Prentice, A. An appraisal of vitamin B6 status indices and associated confounders, in young people aged 4–18 years and in people aged 65 years and over, in two national British surveys. Public Health Nutr. 2, 529–535. https://doi.org/10.1017/s1368980099000713 (1999).
Webster, A. J., Gaitskell, K., Turnbull, I., Cairns, B. J. & Clarke, R. Characterisation, identification, clustering, and classification of disease. Sci. Rep. 11, 5405. https://doi.org/10.1038/s41598-021-84860-z (2021).
Paul, L., Ueland, P. M. & Selhub, J. Mechanistic perspective on the relationship between pyridoxal 5′-phosphate and inflammation. Nutr. Rev. 71, 239–244. https://doi.org/10.1111/nure.12014 (2013).
Cattaneo, M., Lombardi, R., Lecchi, A., Bucciarelli, P. & Mannucci, P. M. Low plasma levels of vitamin B(6) are independently associated with a heightened risk of deep-vein thrombosis. Circulation 104, 2442–2446. https://doi.org/10.1161/hc4501.098925 (2001).
Dalery, K. et al. Homocysteine and coronary artery disease in French Canadian subjects: Relation with vitamins B12, B6, pyridoxal phosphate, and folate. Am. J. Cardiol. 75, 1107–1111. https://doi.org/10.1016/s0002-9149(99)80739-5 (1995).
Le Marchand, L. et al. Plasma levels of B vitamins and colorectal cancer risk: The multiethnic cohort study. Cancer Epidemiol. Biomark. Prev. 18, 2195–2201. https://doi.org/10.1158/1055-9965.EPI-09-0141 (2009).
Midttun, O. et al. Low plasma vitamin B-6 status affects metabolism through the kynurenine pathway in cardiovascular patients with systemic inflammation. J. Nutr. 141, 611–617. https://doi.org/10.3945/jn.110.133082 (2011).
Saibeni, S. et al. Low vitamin B(6) plasma levels, a risk factor for thrombosis, in inflammatory bowel disease: Role of inflammation and correlation with acute phase reactants. Am. J. Gastroenterol. 98, 112–117. https://doi.org/10.1111/j.1572-0241.2003.07160.x (2003).
Sanderson, C. R. & Davis, R. E. Serum pyridoxal in patients with gastric pathology. GUT 17, 371–374. https://doi.org/10.1136/gut.17.5.371 (1976).
Wei, E. K. et al. Plasma vitamin B6 and the risk of colorectal cancer and adenoma in women. J. Natl. Cancer Inst. 97, 684–692. https://doi.org/10.1093/jnci/dji116 (2005).
Wilson, R. G. & Davis, R. E. Serum pyridoxal concentrations in children with diabetes mellitus. Pathology 9, 95–98. https://doi.org/10.3109/00313027709085244 (1977).
Friso, S., Jacques, P. F., Wilson, P. W., Rosenberg, I. H. & Selhub, J. Low circulating vitamin B(6) is associated with elevation of the inflammation marker C-reactive protein independently of plasma homocysteine levels. Circulation 103, 2788–2791. https://doi.org/10.1161/01.cir.103.23.2788 (2001).
Morris, M. S., Sakakeeny, L., Jacques, P. F., Picciano, M. F. & Selhub, J. Vitamin B-6 intake is inversely related to, and the requirement is affected by, inflammation status. J. Nutr. 140, 103–110. https://doi.org/10.3945/jn.109.114397 (2010).
Huang, S. C., Wei, J. C., Wu, D. J. & Huang, Y. C. Vitamin B(6) supplementation improves pro-inflammatory responses in patients with rheumatoid arthritis. Eur. J. Clin. Nutr. 64, 1007–1013. https://doi.org/10.1038/ejcn.2010.107 (2010).
Sparkes, A. H. Feeding old cats—an update on new nutritional therapies. Top Companion Anim. Med. 26, 37–42. https://doi.org/10.1053/j.tcam.2011.01.006 (2011).
Fahey, G. C. Jr., Barry, K. A. & Swanson, K. S. Age-related changes in nutrient utilization by companion animals. Annu. Rev. Nutr. 28, 425–445. https://doi.org/10.1146/annurev.nutr.28.061807.155325 (2008).
Peachey, S. E., Dawson, J. M. & Harper, E. J. The effect of ageing on nutrient digestibility by cats fed beef tallow-, sunflower oil- or olive oil-enriched diets. Growth Dev. Aging 63, 61–70 (1999).
Laflamme, D. P. Nutrition for aging cats and dogs and the importance of body condition. Vet. Clin. North Am. Small Anim. Pract. 35, 713–742. https://doi.org/10.1016/j.cvsm.2004.12.011 (2005).
Percie du Sert, N. et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. PLoS Biol. 18, e3000410. https://doi.org/10.1371/journal.pbio.3000410 (2020).
Officials, A. o. A. F. C. (ed Association of American Food Control Officials Official Publication) 107–234 (2023).
Beutler, E. Red Cell Metabolism: A Manual of Biochemical Methods 3rd edn. (Grune & Stratton, 1984).
Acknowledgements
The study was supported by the Center for Companion Animal Health, School of Veterinary Medicine, University of California, Davis (to CG). Ms. V. Chu was supported by the Students Training in Advanced Research (STAR) Program (NIH 5T35OD010956-23).
Funding
This study was funded by a grant to CG from the Center for Companion Animal Health (School of Veterinary Medicine, University of California Davis). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Center for Companion Animal Health or the School of Veterinary Medicine. Ms. Vy Chu was supported by Students Training in Advanced Research (STAR) Program, NIH 5T35OD010956-23.
Author information
Authors and Affiliations
Contributions
Conceptualization, methodology, formal analysis: V.C. and C.G.; data resources: A.J.F., and J.A.L.; data curation: C.G.; writing—original draft preparation: C.G.; collection of blood samples and records: M.M. and V.C.; writing—review and editing: all authors; funding acquisition: C.G. All authors have agreed on the final version of this study.
Corresponding author
Ethics declarations
Competing interests
The funder (CCAH) had no role in the study’s design, in the collection, analysis, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results. No potential financial and non-financial competing interests that could directly or indirectly undermine the objectivity, integrity, and value of this publication through a potential influence on the judgments and actions of authors regarding objective data presentation, analysis, and interpretation were found. Jennifer A. Larsen (JAL) is an investigator in clinical trials sponsored by Royal Canin and Nestlé Purina PetCare. She develops educational materials for Brief Media, Mark Morris Institute, and Healthy Pet magazine. She participates as a speaker or attendee in continuing education events sponsored or organized by Royal Canin, Nestlé Purina PetCare, Nature's Variety, and Hill's Pet Nutrition. Andrea J. Fascetti (AJF) is the Scientific Director of the Feline Nutrition and PetCare Center and Amino Acid Laboratory at the University of California, Davis, providing research support fee-for-service. None of these activities lead to a conflict of interest or influence the collection or interpretation of results. AJF advised Synergy Food Ingredients, Clorox, and received a grant from Nutro, remuneration for lectures, or as an advisor on behalf of Nestlé Purina PetCare, Mars Petcare, and the Pet Food and Mark Morris Institutes. A nutrition resident received funds from Hill's Pet Nutrition Resident Clinical Study Grants program at the time of the study. The Veterinary Medical Teaching Hospital at UCD receives partial support for a Nutrition Technician from Nestlé Purina PetCare and its veterinary nutrition program from Nestlé Purina, Mars Petcare, and Hill's Pet Care. C.G. is an Editorial Board Member of Scientific Reports (Nature Publishing Company). She received compensation as a Field Chief Editor for Frontiers in Molecular Biosciences and honoraria from participating in NIH peer review meetings. The rest of the authors declare no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chu, V., Fascetti, A.J., Larsen, J.A. et al. Factors influencing vitamin B6 status in domestic cats: age, disease, and body condition score. Sci Rep 14, 2037 (2024). https://doi.org/10.1038/s41598-024-52367-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-52367-y
- Springer Nature Limited