
Abstract
The results of randomized controlled trials are unclear about the long-term effect of blood pressure (BP) on kidney function assessed as the glomerular filtration rate (GFR) in persons without chronic kidney disease or diabetes. The limited duration of follow-up and use of imprecise methods for assessing BP and GFR are important reasons why this issue has not been settled. Since a long-term randomized trial is unlikely, we investigated the association between 24-h ambulatory BP (ABP) and measured GFR in a cohort study with a median follow-up of 11 years. The Renal Iohexol Clearance Survey (RENIS) cohort is a representative sample of persons aged 50 to 62 years without baseline cardiovascular disease, diabetes, or kidney disease from the general population of Tromsø in northern Norway. ABP was measured at baseline, and iohexol clearance at baseline and twice during follow-up. The study population comprised 1589 persons with 4127 GFR measurements. Baseline ABP or office BP components were not associated with the GFR change rate in multivariable adjusted conventional regression models. In generalized additive models for location, scale, and shape (GAMLSS), higher daytime systolic, diastolic, and mean arterial ABP were associated with a slight shift of the central part of the GFR distribution toward lower GFR and with higher probability of GFR < 60 mL/min/1.73 m2 during follow-up (p < 0.05). The use of a distributional regression method and precise methods for measuring exposure and outcome were necessary to detect an unfavorable association between BP and GFR in this study of the general population.
Similar content being viewed by others
Introduction
High blood pressure (BP) is the leading risk factor for death and loss of disability-adjusted life years globally and is an important risk factor for end-stage kidney disease (ESKD)1. Whereas randomized controlled trials (RCTs) have established hypertension as a cause of cardiovascular disease beyond a reasonable doubt, similar high-quality evidence does not exist for the prevention of chronic kidney disease (CKD) by treating primary hypertension in persons without diabetes2,3,4,5,6. Indeed, at least two RCTs have found an adverse effect of intensified antihypertensive treatment on the glomerular filtration rate (GFR)4,5. Although this may have been caused by short-term hemodynamic changes that may ultimately lead to beneficial long-term effects, this remains unproven because of the limited duration of follow-up in the RCTs2,3,4,5.
The lack of definitive evidence for the causal association between high BP and loss of kidney function has raised doubts about whether nonmalignant primary hypertension is a cause of CKD in persons without diabetes. In a study of kidney biopsies from live kidney donors by Denic et al., mild hypertension was not associated with the number of nephrons, the single-nephron glomerular filtration rate (GFR), or the total GFR7. In the longitudinal population-based Renal Iohexol Clearance Survey (RENIS), we did not find an association between elevated BP and accelerated mean GFR decline in the general middle-aged population over a median follow-up of 5.6 years8,9. We hypothesized that additional genetic and environmental factors are necessary for elevated BP to cause CKD in some individuals after an even longer observation period.
In the present study, we investigated this hypothesis by analyzing baseline 24-h ambulatory blood pressure (ABP) as a risk factor for change in the GFR measured as iohexol clearance after a follow-up of more than ten years. Since conventional least squares regression methods only analyze changes in the mean of the GFR distribution while assuming its other properties to be constant, we used distributional regression to analyze the associations between ABP and the time change of different percentiles of the GFR distribution10.
Methods
Study population
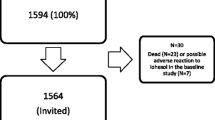
The Renal Iohexol Clearance Survey (RENIS) is a substudy of the Tromsø Study. The Tromsø Study has invited random samples of the general population of the municipality of Tromsø in northern Norway to a series of repeated health surveys11. The RENIS cohort was recruited from all persons between 50 and 62 years of age examined in the sixth Tromsø Study. All persons without self-reported cardiovascular disease, kidney disease or diabetes mellitus were invited, and 1627 persons were included in random order until a prespecified target was met. The cohort underwent measurements of plasma iohexol clearance at baseline in 2007–2009 (RENIS-T6), in 2013–2015 (RENIS-FU) and in 2018–2020 (RENIS-3) (Fig. 1). The inclusion process has been described in detail previously12. All included persons were invited to ABP measurement at baseline, and everybody with a valid measurement was eligible for the present study (Fig. 1). The GFR measurements of a small random sample who had an extra GFR measurement for the purpose of assessing day-to-day variation in RENIS-FU were also included in the analyses.

Persons from the Renal Iohexol Clearance Survey (RENIS) cohort were included in the present investigation. The numbers in ovals represent the numbers of persons from one wave of the investigation included in the next. RENIS-T6 the baseline investigation; RENIS-FU, the first follow-up; RENIS-3, the last follow-up; ABP, ambulatory blood pressure.
This study complied with the Declaration of Helsinki and was approved by the Regional Committee for Medical and Health Research Ethics of Northern Norway. All subjects provided a written informed consent.
Data
The investigations were performed at the Clinical Research Unit of the University Hospital of North Norway. The participants answered questionnaires that included questions about previous diseases, alcohol use, smoking habits, and current medication. Alcohol use was analyzed as a dichotomous variable for the weekly use of alcohol or not. Smoking was analyzed as the number of cigarettes per day currently used. Antihypertensive medication was analyzed as separate dichotomous variables for the use of ACE inhibitors, A2 receptor blockers, beta-blockers, calcium blockers, diuretics or other antihypertensives.
Measurements
Iohexol clearance
GFR was measured as single-sample plasma iohexol clearance, which has been validated against gold standard methods13,14 and has been described in detail previously12,15. Five millilitres of iohexol were injected intravenously and a sample obtained for iohexol measurement at the optimal sampling time for each person calculated by Jacobsson’s equation16. GFR was calculated by a numerical solution of Jacobsson’s three equation 16. To avoid confounding from changes in body size, absolute GFR in mL/min was used. Body surface area-indexed GFR was analyzed in a sensitivity analysis17. Body surface area was estimated by the equation of DuBois and DuBois17.
Blood pressure measurements
Twenty-four-hour ABP was initiated at the day of the baseline GFR measurement using the Spacelab 90207 (Spacelab Inc., Redmond, Washington, USA) as described previously18. The criteria for a valid ABP measurement were adopted from the International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcome study19. Attended office BP was measured after 2 min of rest in the seated position with an automated device (model UA 799; A&D, Tokyo, Japan) by a study nurse18. The daytime to nighttime systolic and diastolic dips were analyzed as one minus the ratio of the mean nighttime to daytime systolic BP (SBP) or diastolic BP (DBP). Ambulatory mean arterial pressure (MAP) was defined as DBP + ((SBP − DBP)/3).
Office hypertension was defined as office SBP ≥ 140 mmHg or office DBP ≥ 90 mmHg or the use of antihypertensive medication according to the guidelines of the European Society of Hypertension20.
Other baseline measurements
Fasting serum glucose, creatinine, cystatin C, triglycerides, and LDL- and HDL-cholesterol were measured with standard methods as described previously18. The urine albumin-creatinine ratio (ACR) was measured as the median of ACR measured on three separate days21. Serum creatinine was measured using an enzymatic assay standardized to the isotope dilution mass spectrometry method (CREA Plus, Roche Diagnostics, GmbH, Mannheim, Germany). Cystatin C was measured by a particle-enhanced turbidimetric immunoassay (Gentian, Moss, Norway) calibrated to the international reference ERM-DA471/IFCC as described previously22. Estimated GFR (eGFR) was calculated using the original Chronic Kidney Disease Epidemiology Collaboration equations published in 2009 and 2012 (eGFRcrea, eGFRcys and eGFRcyscrea)23,24.
Statistical methods
The baseline characteristics of the cohort are given as the mean (standard deviation) or median (interquartile range) for ABP < or ≥ 130/80, the threshold for hypertensive 24-h ABP according to the European Society of Hypertension20. Differences across the ABP levels were analyzed with two-sample t-tests, Wilcoxon rank-sum tests or tests of proportion as appropriate.
We first investigated the relationship between mean GFR and the BP components with general additive mixed models (GAMM)25,26. GAMMs are a generalization of linear mixed models where nonlinear effects of the independent variables can be modeled. The reason for using GAMMs and not linear mixed models was that a previous investigation in the RENIS cohort found sex-specific nonlinear relationships between mean GFR and time12. Accordingly, we adjusted for these relationships in the GAMMs.
The GAMMs had GFR as the dependent variable and a linear term for each BP component as the independent variable in separate models. The models included a random intercept and slope and an unstructured covariance matrix. We analyzed office and ambulatory daytime and nighttime SBP, DBP, and MAP as well as the systolic and diastolic nighttime BP dips. We included both the linear main effects of these BP components and their interaction with time. The coefficient for this interaction represented the association between the component and the GFR change rate. A negative sign for the coefficient signified a steeper GFR decline. The time variable was defined as years since baseline. In addition to the sex-specific nonlinear time variables, we included two sets of linear baseline adjustment variables, including their interactions with time: Model 1: sex and sex-specific variables for baseline age, body weight, height, and dichotomous variables for each class of antihypertensive medication. Model 2: As Model 1 with the addition of pulse frequency, fasting glucose, triglycerides, LDL- and HDL-cholesterol, number of cigarettes currently smoked per day, and a dichotomous variable for weekly alcohol use. Model 3: As Model 2 with the addition of ACR. All study participants were included in the GAMM analyses regardless of whether they were examined at follow-up because mixed models allow for missing observations at one or more points in time27,28.
Next, we analyzed the associations between ABP and the time change of the GFR distribution in generalized additive models for location, scale, and shape (GAMLSS). Conventional least squares regression methods analyze the effect of exposures on the mean of outcomes, whereas other aspects of their probability distributions are assumed to be independent of the exposures. GAMLSS relaxes these assumptions and analyzes the effects of the exposure on the total outcome distribution25,26,29. The GFR distribution used in this investigation was the sinh-arcsinh (SHASH) distribution30, which is specified by the four parameters location, scale, skewness, and tailweight. Variations of these four parameters permit greater flexibility in the probability distribution that can be modeled than the usual normal distribution (see Online Resource and Fig. S1). The GAMLSS models each of the four parameters as a nonlinear function of the ABP component and of their interaction with time as independent variables. Accordingly, the main difference between GAMLSS and conventional regression methods is that GAMLSS analyzes four dependent variables (location, scale, skewness, and tailweight) simultaneously in one model, whereas other methods only analyze one dependent variable (the mean). The location, scale, and tailweight parameters are related (but not exactly equivalent) to the mean, standard deviation, and kurtosis (see Online Resource and Fig. S1). In the function for the location, we included a random intercept and adjustments as in Model 2 in the GAMM above, except that we used one dichotomous variable for the use of any antihypertensive medication to simplify the model. For the same reason, we restricted adjustments in the functions for scale, skewness, and tailweight to sex-specific nonlinear functions of the time variable. We investigated day- and nighttime SBP, DBP, and MAP in separate GAMLSS.
To find the simplest model consistent with the data, we compared the fit of models with the four SHASH parameters specified above with models where one or more of the nonlinear functions for scale, skewness or tailweight were replaced by a constant. Models with all eight possible combinations of replacement by a constant for these three parameters were examined. The Akaike Information Criterion (AIC) was used to compare the fit of the models31. The p-value for the nonlinear interaction between the ABP component and time for each SHASH parameter in each best-fitting model was used to judge whether there was a time-dependent association between the ABP component and the development of the GFR distribution. The finding of an association implied that the corresponding ABP component was a risk factor for time change in the GFR distribution. The p-value for the nonlinear main effect of an ABP component in each best-fitting model was used to judge whether there was a time-independent cross-sectional association between the BP component and GFR.
STATA/MP 17.0 (www.stata.com) and R version 3.6.3 (www.r-project.org) were used for the analyses in this study. The mgcv and mgcViz packages of R were used for the analyses with GAMM and GAMLSS25,26. Statistical significance was set at p < 0.05.
Results
Valid ABP measurements were obtained for 1608 (99%) of the 1627 persons included at baseline. Because of missing values for some of the adjustment variables for 38 persons (Table S1), the study population consisted of 1589 (98%) complete cases (Table S1, Fig. 1). Of these 1589 persons, 1299 had repeated GFR measurements in RENIS-FU and 1154 in RENIS-3. In addition, a random sample of 85 of the participants in RENIS-FU had an extra measurement to measure the day-to-day variation in GFR. Accordingly, the total number of GFR measurements was 4127. Reasons for not attending and comparisons of investigated persons with all eligible persons have been published previously12. The median (IQR) (range) follow-up was 10.7 (6.4–11.3) (0–12.8) years.
Most baseline characteristics (Table 1), including mGFR, differed between the two categories of ABP (p < 0.05), but not eGFRcrea, eGFRcys, eGFRcyscrea, smoking, alcohol use or LDL-cholesterol.
Associations of blood pressure components with the mean GFR change rate
There were no statistically significant linear associations of any of the investigated BP components with the mean GFR change rate in the GAMMs in the fully adjusted model (Table 2). Sensitivity analyses after excluding observations with self-reported incident CVD during follow-up, after excluding persons with antihypertensive treatment and with body surface area adjusted GFR gave similar results (Supplementary Results, Tables S2 and S3).
Nonlinear associations of ambulatory blood pressure with the time change in the GFR distribution
GAMLSS with nonlinear functions for location, scale, and skewness, but with a constant tailweight parameter, had the lowest AIC and best fit for all of the ABP components except nighttime DBP (Model G, Table S4). For nighttime DBP, a model with both constant skewness and tailweight had the lowest AIC (Model C, Table S4).
In these best fitting models, the daytime but not the nighttime ABP components, were associated with nonlinear time changes in the GFR distribution (p < 0.05) (Table 3). Accordingly, only daytime ABP was a risk factor for the time change of GFR. The predicted time changes of the four SHASH parameters at the mean of the adjustment variables for daytime ABP are plotted in Fig. S2, and the complete GFR probability density functions at baseline and the maximum follow-up of 13 years are shown in Fig. 2.

Sex-specific predicted probability density distributions of GFR at baseline (solid curves) and the longest follow-up (dashed curves) for daytime ABP components. Probability density distributions based on GAMLSS are used to show the association of ABP with the complete GFR distributions in addition to association with the mean, as in conventional regression. Separate curves are shown for the 5th (blue) and 95th (red) percentiles of the corresponding ABP component (110 and 152 mmHg for daytime SBP, 68 and 96 mmHg for daytime DBP and 83 and 114 mmHg for daytime MAP). GFR is indicated on the x-axis, and the probability density is indicated on the y-axis.
In contrast, all of the ABP components demonstrated cross-sectional time-independent associations with the location and scale parameters (p < 0.05) (Table 3). The daytime and nighttime SBP were also associated with the skewness parameter (p < 0.05). This indicates that high ABP was associated with a wider GFR distribution, which was skewed toward a lower GFR for systolic ABP at baseline (Figs. 2, 3 and Fig. S2).

Sex-specific distributions of predicted GFR as functions of follow-up. For each plot, separate curves for the 5th (blue) and 95th (red) percentiles of the corresponding ABP component are shown (110 and 152 mmHg for daytime SBP, 68 and 96 mmHg for daytime DBP and 83 and 114 mmHg for daytime MAP). Plots for the ABP components with a statistically significant association with the time change of the GFR distribution and time are shown. The dotted lines represent the 10th and 90th percentiles, the dashed lines represent the 25th and 75th percentiles, and the solid line represents the 50th percentile of the GFR distribution. The predictions are based on the best fitting GAMLSS model in Table 3 with adjustment variables set at their baseline means and random effects set at zero.
The corresponding predicted time change of the 10th, 25th, 50th, 75th and 90th percentiles of the GFR distribution for daytime ABP at the mean of the adjustment variables are shown in Fig. 3. The figure includes separate curves for the 5th and 95th percentiles of the ABP components (110 and 152 mmHg for daytime SBP, 68 and 96 mmHg for daytime DBP and 83 and 114 mmHg for daytime MAP). The difference between the GFR percentiles for these two ABP levels vs. time is plotted in Fig. 4.

Sex-specific differences between the percentiles of GFR presented in Fig. 3 for the 95th and 5th percentiles of ABP components as functions of time. The dotted lines represent differences between the two ABP levels for the 10th and 90th percentiles, the dashed lines for the 25th and 75th percentiles and the solid line for the 50th percentile of the GFR distribution. E.g., the solid line (50th percentile of GFR) for systolic ABP in men is positive at baseline and declines with follow-up to negative values corresponding to the red solid curve (high systolic ABP) declining faster and crossing the blue solid line (low systolic ABP) in Fig. 3.
At baseline, Fig. 4 demonstrates that the central part of the GFR distribution between the 25th and 75th percentiles is greater for high than for low daytime SBP. Over the follow-up period, the differences decreased for high vs. low daytime SBP, DBP and MAP by approximately 2 to 5 mL/min. This indicates a modestly steeper GFR decline for most persons with high daytime ABP. The largest difference between the ABP levels was found for the 10th percentile of the GFR distribution, but this effect was fairly constant over time, except for an increasingly negative difference in daytime SBP in men (Fig. 4). This means that high ABP confers a higher probability of GFR lower than the 10th percentile but that this risk increases over time only for daytime SBP in men. The increasingly positive difference between the 90th percentiles of the GFR distribution for all three daytime ABP components indicates that some people with high daytime ABP developed higher GFR than people with low ABP (Figs. 3 and 4).
Sensitivity analyses with office BP components in the best fitting GAMLSS in Table 3 found no statistically significant associations with the time change of the SHASH parameters (Supplementary Results, Table S5). Sensitivity analyses after exclusion of persons with antihypertensive treatment demonstrated the same pattern of statistically significant time-dependent associations with change in the daytime ABP SHASH parameters as in the total cohort (Supplementary Results, Table S6, Fig. S3).
Ten-year probability of incident GFR less than 60 mL/min/1.73 m2
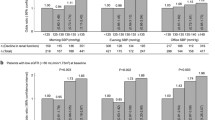
Based on the best fitting GAMLSS for daytime ABP, the predicted ten-year probabilities of a GFR lower than 60 mL/min/1.73 m2 are shown in Fig. 5. For this purpose, the GFR used in the GAMLSS was indexed for the sex-specific mean body surface area. Simulating 5000 samples from the posterior distribution of the regression coefficients was used to construct 95% credible intervals (CI)25. For women, the difference in probability between the 95th and 5th percentiles for daytime SBP was 0.05 (95% CI 0.03 to 0.09), for daytime DBP 0.03 (95% CI 0.002 to 0.07) and for daytime MAP 0.05 (95% CI 0.02 to 0.09). For men, the same differences were 0.04 (95% CI 0.02 to 0.07), 0.02 (95% CI -0.01 to 0.04) and 0.03 (95% CI 0.01 to 0.06).

Sex-specific predicted ten-year probabilities of a GFR less than 60 mL/min/1.73 m2 as functions of daytime SBP, DBP and MAP. The predictions were based on the best fitting GAMLSS model in Table 3 with adjustment variables set at their baseline means and random effects set at zero. The GFR was indexed for sex-specific mean body surface area. The gray bands indicate 95% credible intervals.
Sex
We compared the fit of GAMLSS for daytime ABP in Table 3 with and without sex-specific nonlinear functions for the interaction between ABP components and time. The AIC improved slightly only for daytime SBP (32,636 vs. 32,640), but the effects of the sex-specific terms were not statistically significant. Accordingly, we did not find evidence of sex-specific effects of ABP on the time change of the GFR distribution.
Associations between BP and the time change of estimated GFR
Substituting eGFRcrea, eGFRcys or eGFRcyscrea for GFR as the dependent variable in the fully adjusted GAMM and GAMLSS models demonstrated substantial differences between measured GFR and eGFR, and between the three different eGFRs (see Supplementary Results, Tables S7 and S8, Fig. S4).
Discussion
This study found no association between elevated baseline BP and long-term mean GFR in the multivariable-adjusted conventional regression models (Table 2). With a distributional regression method, higher baseline daytime ABP was a risk factor for the development of a more unfavorable GFR distribution (Figs. 2, 3 and 4). We found an increased risk of a modestly accelerated decline in the central part of the GFR distribution and a small increase in the absolute risk of a low GFR between the 95th and 5th percentiles of daytime SBP (Fig. 5). Accordingly, elevated baseline daytime ABP contributed to a slightly steeper GFR decline in most people and to a small increase in the absolute risk of chronic kidney disease, defined as a low GFR.
To our knowledge, the only other longitudinal investigation of ABP and kidney function in a population-based study was McMullan et al.’s study of ABP and eGFRcrea32. The authors found no association between SBP and incident CKD but did not report results for DBP. Several differences between the study population and methodology may account for the differences from our study, of which the most important were a low participation rate, the use of estimated GFR and the lack of any adjustment for antihypertensive medication32.
Considerable uncertainty exists about the effects of BP on GFR. Although most longitudinal observational studies have found an association between BP and subsequent GFR decline, incident CKD or ESKD33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52, there is no conclusive evidence from RCTs that antihypertensive treatment prevents kidney dysfunction, except in patients with CKD or diabetes2,3,4,5. In a meta-analysis of RCTs with 78,931 participants, BP-lowering treatment had no effect on the risk of kidney failure6. However, the short median follow-up of only 3.4 years of the included studies was a major limitation, which may explain why beneficial effects were difficult to detect.
We found different predicted time changes in the GFR for women and men (Figs. 3 and 5), even if there was no evidence of sex-specific BP effects on time change in the statistical models. This is a consequence of the overall nonlinear sex-specific trajectories of age-related GFR decline, which have been discussed in a previous paper12. Because this effect was included as an adjustment in the GAMLSS in this investigation, its predictions differed between the two sexes due to the nonlinearity of the models, although the overall pattern of changes was the same.
The time change in the GFR distribution showed a paradoxical high GFR with an increasing trend for high daytime ABP (Fig. 4). In addition to the role of high GFR or hyperfiltration as a pathogenetic factor in diabetic kidney disease53, there is also evidence of an association between hypertension and hyperfiltration from a recent Mendelian randomization study54 and from the initial drop in GFR when antihypertensive treatment is started in RCTs55,56,57. This drop has been interpreted as a beneficial effect of reducing hyperfiltration58. Our results suggest that hyperfiltration may persist longer than previously thought in some persons. The ultimate consequences of this are unclear.
Whereas the aim of this study was to study the time change in the GFR distribution, there were statistically significant cross-sectional time-independent associations between all of the ABP components and SHASH parameters (Table 3, Figs. 2, 3 and Fig. S2). This indicates that the associations between ABP and GFR were established at ages younger than the baseline age of our study. The association between nephron endowment and hypertension found by others suggests a congenital association but does not explain these findings59. The associations between ABP and GFR in younger people could have important implications for antihypertensive therapy and should be explored further.
The current study illustrates how different methods influence the results of an observational study of BP and GFR. In addition to the regression model, the method for assessing GFR is decisive: the results when using the eGFRs differ from the measured GFR and between each other (Tables S7 and S8). The explanation is probably confounders that influence both the production rate of creatinine and cystatin C and the GFR60,61,62,63,64,65. Accordingly, caution should be applied when using eGFR in studies of BP and GFR. Also, office BP did not identify time-dependent associations with the GFR distribution (Table S5). This suggests that ABP is a better predictor of GFR than office BP, similar to what has been found for cardiovascular outcomes. Current hypertension guidelines recognize that ABP gives important additional information for the diagnosis of hypertension both in the general population66,67 and in CKD patients68.
The most important strengths of the present study are its use of iohexol clearance and ABP, which are gold standard methods for assessing GFR and BP. To our knowledge, the duration of follow-up also exceeds all previous observational studies and RCTs studying the association between BP and GFR decline, except for two studies with a follow-up of 30 years50,52. Comorbidities that could mediate an indirect effect of BP on GFR may inflate the BP effect, but few previous studies excluded subjects with CVD or diabetes or adjusted for these conditions33,35,37,38. We studied a representative sample of the general population without CVD or diabetes, which is a further strength of our investigation.
The main limitation of this study is that inferences about causality cannot be made from observational studies. The direction of any causal connection between ABP and GFR is also uncertain, as subclinical kidney damage has been suggested as a cause of primary hypertension69. Although there were no linear associations between BP and GFR change in fully adjusted GAMMs, a larger study with greater statistical power may have been able to detect the small effects found with GAMLSS. ABP was only measured at baseline, and we did not consider changes in BP during follow-up. A sensitivity analysis after excluding observations with antihypertensive medications did not indicate that changes in antihypertensive medication during follow-up were important for the results. The study participants were of European ancestry, limiting the generalizability. Since we are not aware of any other population-based cohorts with ABP and serial measurements of GFR, external validation of our findings is currently not possible.
We conclude that investigations of the relationship between BP and kidney function depend critically on the methods for assessing BP and GFR as well as on the statistical methods. By using measurements of GFR and ambulatory BP in a model that relaxes the restrictive assumptions of conventional regression methods, we found that elevated daytime ABP was associated with a shift in the GFR distribution toward lower GFR. This will only be associated with a modest acceleration of GFR decline in most people but increases the risk of CKD. The genetic and environmental causes of low GFR in a minority of persons with high ABP are clinically important and should be the subject of further research. The potential for preserving GFR in these persons through antihypertensive treatment should also be explored, ideally in a long-term RCT with change in measured GFR as the endpoint.
Data availability
The data underlying this article cannot be shared publicly because this was not included in the research permission, due to ethical considerations and the privacy of individuals that participated in the study. The data can be shared on request from the corresponding author as part of research collaboration.
Change history
03 June 2024
A Correction to this paper has been published: https://doi.org/10.1038/s41598-024-63297-0
References
Lozano, R. et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet 380, 2095–2128. https://doi.org/10.1016/S0140-6736(12)61728-0 (2012).
Hsu, C. Y. Does treatment of non-malignant hypertension reduce the incidence of renal dysfunction? A meta-analysis of 10 randomised, controlled trials. J. Hum. Hypertens. 15, 99–106. https://doi.org/10.1038/sj.jhh.1001128 (2001).
Daien, V. et al. Treatment of hypertension with renin-angiotensin system inhibitors and renal dysfunction: A systematic review and meta-analysis. Am. J. Hypertens. 25, 126–132. https://doi.org/10.1038/ajh.2011.180 (2012).
The SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N. Engl. J. Med. 373, 2103–2116. https://doi.org/10.1056/NEJMoa1511939 (2015).
Peralta, C. A. et al. Effect of intensive versus usual blood pressure control on kidney function among individuals with prior lacunar stroke: A post hoc analysis of the secondary prevention of small subcortical Strokes (SPS3) Randomized Trial. Circulation 133, 584–591. https://doi.org/10.1161/circulationaha.115.019657 (2016).
Ettehad, D. et al. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. The Lancet 387, 957–967. https://doi.org/10.1016/S0140-6736(15)01225-8 (2016).
Denic, A. et al. Single-nephron glomerular filtration rate in healthy adults. N. Engl. J. Med. 376, 2349–2357. https://doi.org/10.1056/NEJMoa1614329 (2017).
Eriksen, B. O. et al. Elevated blood pressure is not associated with accelerated glomerular filtration rate decline in the general non-diabetic middle-aged population. Kidney Int. 90, 404–410. https://doi.org/10.1016/j.kint.2016.03.021 (2016).
Eriksen, B. O. et al. Blood pressure and age-related GFR decline in the general population. BMC Nephrol. 18, 77. https://doi.org/10.1186/s12882-017-0496-7 (2017).
Kneib, T., Silbersdorff, A. & Säfken, B. Rage against the mean: A review of distributional regression approaches. Econom. Stat. https://doi.org/10.1016/j.ecosta.2021.07.006 (2021).
Jacobsen, B. K., Eggen, A. E., Mathiesen, E. B., Wilsgaard, T. & Njølstad, I. Cohort profile: The Tromsø Study. Int. J. Epidemiol. 41, 961–967 (2011).
Melsom, T. et al. Sex differences in age-related loss of kidney function. J. Am. Soc. Nephrol. 33, 1891–1902. https://doi.org/10.1681/ASN.2022030323 (2022).
Soveri, I. et al. Measuring GFR: A systematic review. Am. J. Kidney Dis. 64, 411–424. https://doi.org/10.1053/j.ajkd.2014.04.010 (2014).
Delanaye, P. et al. Iohexol plasma clearance for measuring glomerular filtration rate in clinical practice and research: A review. Part 1: How to measure glomerular filtration rate with iohexol?. Clin. Kidney J. 9, 682–699. https://doi.org/10.1093/ckj/sfw070 (2016).
Eriksen, B. O. et al. Comparability of plasma iohexol clearance across population-based cohorts. Am. J. Kidney Dis. 76, 54–62. https://doi.org/10.1053/j.ajkd.2019.10.008 (2020).
Jacobsson, L. A method for the calculation of renal clearance based on a single plasma sample. Clin. Physiol. 3, 297–305 (1983).
DuBois, D. & Dubois, E. F. The measurement of the surface area of man. Arch. Intern. Med. 15, 868–881 (1915).
Mathisen, U. D. et al. Ambulatory blood pressure is associated with measured glomerular filtration rate in the general middle-aged population. J. Hypertens. 30, 497–504. https://doi.org/10.1097/HJH.0b013e32834f973a (2012).
Kikuya, M. et al. Diagnostic thresholds for ambulatory blood pressure monitoring based on 10-year cardiovascular risk. Circulation 115, 2145–2152 (2007).
Williams, B. et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 39, 3021–3104. https://doi.org/10.1093/eurheartj/ehy339 (2018).
Solbu, M. D., Kronborg, J., Eriksen, B. O., Jenssen, T. G. & Toft, I. Cardiovascular risk-factors predict progression of urinary albumin-excretion in a general, non-diabetic population: A gender-specific follow-up study. Atherosclerosis 201, 398–406 (2008).
Eriksen, B. O. et al. Estimated and measured GFR associate differently with retinal vasculopathy in the general population. Nephron 131, 175–184. https://doi.org/10.1159/000441092 (2015).
Levey, A. S. et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 150, 604–612 (2009).
Inker, L. A. et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 367, 20–29. https://doi.org/10.1056/NEJMoa1114248 (2012).
Wood, S. N. Generalized Additive Models (CRC Press, 2017).
Fasiolo, M., Nedellec, R., Goude, Y. & Wood, S. N. Scalable visualisation methods for modern Generalized Additive Models. J. Comput. Graph Stat. 29, 78–86 (2020).
Leffondre, K. et al. Analysis of risk factors associated with renal function trajectory over time: A comparison of different statistical approaches. Nephrol. Dial. Transplant. 30, 1237–1243. https://doi.org/10.1093/ndt/gfu320 (2014).
Twisk, J., de Boer, M., de Vente, W. & Heymans, M. Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J. Clin. Epidemiol. 66, 1022–1028. https://doi.org/10.1016/j.jclinepi.2013.03.017 (2013).
Rigby, R. A. & Stasinopoulos, D. M. Generalized additive models for location, scale and shape. J. R. Stat. Soc. Ser. C 54, 507–554 (2005).
Jones, M. C. & Pewsey, A. Sinh-arcsinh distributions. Biometrika 96, 761–780 (2009).
Burnham, K. P. Model Selection and Multimodel Inference: A Practical Information-Theoretic Approach 2nd edn. (Springer, 2002).
McMullan, C. J., Hickson, D. A., Taylor, H. A. & Forman, J. P. Prospective analysis of the association of ambulatory blood pressure characteristics with incident chronic kidney disease. J. Hypertens. 33, 1939–1946. https://doi.org/10.1097/hjh.0000000000000638 (2015).
Kronborg, J. et al. Predictors of change in estimated GFR: A population-based 7-year follow-up from the Tromsø study. Nephrol. Dial. Transplant. 23, 2818–2826 (2008).
Halbesma, N. et al. Changes in renal risk factors versus renal function outcome during follow-up in a population-based cohort study. Nephrol. Dial. Transplant. 25, 1846–1853 (2010).
Rifkin, D. E. et al. Blood pressure components and decline in kidney function in community-living older adults: The Cardiovascular Health Study. Am. J. Hypertens. 26, 1037–1044. https://doi.org/10.1093/ajh/hpt067 (2013).
Hirayama, A. et al. Blood pressure, proteinuria, and renal function decline: Associations in a large community-based population. Am. J. Hypertens. 28, 1150–1156. https://doi.org/10.1093/ajh/hpv003 (2015).
Wang, Q. et al. Blood pressure and renal function decline: A 7-year prospective cohort study in middle-aged rural Chinese men and women. J. Hypertens. 33, 136–143. https://doi.org/10.1097/hjh.0000000000000360 (2015).
Peralta, C. A. et al. Association of pulse pressure, arterial elasticity, and endothelial function with kidney function decline among adults with estimated GFR >60 mL/min/1.73 m(2): The Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Kidney Dis. 59, 41–49. https://doi.org/10.1053/j.ajkd.2011.08.015 (2012).
Lindeman, R. D., Tobin, J. D. & Shock, N. W. Association between blood pressure and the rate of decline in renal function with age. Kidney Int. 26, 861–868 (1984).
Vupputuri, S. et al. Effect of blood pressure on early decline in kidney function among hypertensive men. Hypertension 42, 1144–1149. https://doi.org/10.1161/01.HYP.0000101695.56635.31 (2003).
Klag, M. J. et al. Blood pressure and end-stage renal disease in men. N. Engl. J. Med. 334, 13–18. https://doi.org/10.1056/Nejm199601043340103 (1996).
Hsu, C. Y., McCulloch, C. E., Darbinian, J., Go, A. S. & Iribarren, C. Elevated blood pressure and risk of end-stage renal disease in subjects without baseline kidney disease. Arch. Intern. Med. 165, 923–928 (2005).
Bash, L. D., Astor, B. C. & Coresh, J. Risk of incident ESRD: A comprehensive look at cardiovascular risk factors and 17 years of follow-up in the Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Kidney Dis. 55, 31–41 (2010).
Schaeffner, E. S., Kurth, T., Bowman, T. S., Gelber, R. P. & Gaziano, J. M. Blood pressure measures and risk of chronic kidney disease in men. Nephrol. Dial. Transplant. 23, 1246–1251. https://doi.org/10.1093/Ndt/Gfm757 (2008).
Fox, C. S. et al. Predictors of new-onset kidney disease in a community-based population. JAMA 291, 844–850 (2004).
Kanno, A. et al. Night-time blood pressure is associated with the development of chronic kidney disease in a general population: The Ohasama Study. J. Hypertens. 31, 2410–2417. https://doi.org/10.1097/HJH.0b013e328364dd0f (2013).
Yamagata, K. et al. Risk factors for chronic kidney disease in a community-based population: A 10-year follow-up study. Kidney Int. 71, 159–166 (2007).
Obermayr, R. P. et al. Predictors of new-onset decline in kidney function in a general middle-European population. Nephrol. Dial. Transplant. 23, 1265–1273. https://doi.org/10.1093/ndt/gfm790 (2008).
Garofalo, C. et al. Hypertension and prehypertension and prediction of development of decreased estimated GFR in the general population: A meta-analysis of cohort studies. Am. J. Kidney Dis. 67, 89–97. https://doi.org/10.1053/j.ajkd.2015.08.027 (2016).
Yu, Z. et al. Association between hypertension and kidney Function decline: The Atherosclerosis Risk in Communities (ARIC) STUDY. Am. J. Kidney Dis. 74, 310–319. https://doi.org/10.1053/j.ajkd.2019.02.015 (2019).
Lee, K. P., Kim, Y. S., Yoon, S. A., Han, K. & Kim, Y. O. Association between blood pressure and renal progression in Korean adults with normal renal function. J. Korean Med. Sci. 35, e312. https://doi.org/10.3346/jkms.2020.35.e312 (2020).
Inker, L. A. et al. Midlife blood pressure and late-life GFR and albuminuria: An elderly general population cohort. Am. J. Kidney Dis. 66, 240–248. https://doi.org/10.1053/j.ajkd.2015.03.030 (2015).
Tonneijck, L. et al. Glomerular hyperfiltration in diabetes: Mechanisms, clinical significance, and treatment. J. Am. Soc. Nephrol. 28, 1023–1039. https://doi.org/10.1681/ASN.2016060666 (2017).
Staplin, N. et al. Determining the relationship between blood pressure, kidney function, and chronic kidney disease: Insights from genetic epidemiology. Hypertension 79, 2671–2681. https://doi.org/10.1161/HYPERTENSIONAHA.122.19354 (2022).
Klahr, S. et al. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. Modification of Diet in Renal Disease Study Group. N. Engl. J. Med. 330, 877–884 (1994).
Wright, J. T. et al. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: Results from the AASK trial. JAMA 288, 2421–2431. https://doi.org/10.1001/jama.288.19.2421 (2002).
Neuen, B. et al. Acute treatment effects on GFR in randomized clinical trials of kidney disease progression. J. Am. Soc. Nephrol. 33, 291–303. https://doi.org/10.1681/asn.2021070948 (2022).
Bakris, G. L. & Weir, M. R. Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: Is this a cause for concern?. Arch. Intern. Med. 160, 685–693 (2000).
Keller, G., Zimmer, G., Mall, G., Ritz, E. & Amann, K. Nephron number in patients with primary hypertension. N. Engl. J. Med. 348, 101–108. https://doi.org/10.1056/Nejmoa020549 (2003).
Rule, A. D., Bailey, K. R., Lieske, J. C., Peyser, P. A. & Turner, S. T. Estimating the glomerular filtration rate from serum creatinine is better than from cystatin C for evaluating risk factors associated with chronic kidney disease. Kidney Int. 83, 1169–1176. https://doi.org/10.1038/ki.2013.7 (2013).
Mathisen, U. D. et al. Estimated GFR is associated with cardiovascular risk factors independently of measured GFR. J. Am. Soc. Nephrol. 22, 927–937 (2011).
Knight, E. L. et al. Factors influencing serum cystatin C levels other than renal function and the impact on renal function measurement. Kidney Int. 65, 1416–1421 (2004).
Stevens, L. A. et al. Factors other than glomerular filtration rate affect serum cystatin C levels. Kidney Int. 75, 652–660 (2009).
Schei, J. et al. Residual associations of inflammatory markers with eGFR after accounting for measured GFR in a community-based cohort without CKD. Clin. J. Am. Soc. Nephrol. 11, 280–286. https://doi.org/10.2215/cjn.07360715 (2016).
Porrini, E. et al. Estimated GFR: Time for a critical appraisal. Nat. Rev. Nephrol. 15, 177–190. https://doi.org/10.1038/s41581-018-0080-9 (2019).
Mancia Chairperson, G. et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J. Hypertens. https://doi.org/10.1097/hjh.0000000000003480 (2023).
Whelton, P. K. et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 71, e127–e248. https://doi.org/10.1016/j.jacc.2017.11.006 (2018).
Cheung, A. K. et al. KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 99, S1-s87. https://doi.org/10.1016/j.kint.2020.11.003 (2021).
Johnson, R. J., Lanaspa, M. A., Gabriela Sanchez-Lozada, L. & Rodriguez-Iturbe, B. The discovery of hypertension: Evolving views on the role of the kidneys, and current hot topics. Am. J. Physiol. Renal Physiol. 308, F167-178. https://doi.org/10.1152/ajprenal.00503.2014 (2015).
Acknowledgements
We thank the Clinical Research Unit (University Hospital of North Norway) for performing the study and the Department of Medical Biochemistry (University Hospital of North Norway) for performing the analyses of iohexol. We are also grateful to all of the participants in the RENIS cohort for their contributions to this investigation. B.O.E. and T.M. are grateful to their comembers in the European Kidney Function Consortium for advice and support.
Funding
Open access funding provided by UiT The Arctic University of Norway (incl University Hospital of North Norway). This study was funded by the North Norwegian Regional Health Authority, which had no role in the design and conduct of the study or the collection, management, analysis, and interpretation of the data, review, or approval of the manuscript for submission.
Author information
Authors and Affiliations
Contributions
B.O.E., U.D.M., T.G.J., and T.M. designed the study. B.O.E., U.D.M., V.T.N.S., and T.M. organized the GFR and ABP measurements and collected the data. B.O.E. and M.F. analyzed the data and made the figures. B.O.E. drafted the paper. B.O.E., M.F., U.D.M., T.M., T.G.J., and V.T.N.S. interpreted the data and revised the paper. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
Toralf Melsom reported payment for a lecture at a local meeting from Novo Nordisk Norway. Trond Geir Jenssen reported payments for lectures from Novo Nordisk, Boehringer Ingelheim and Astra Zeneca, and support for attending a symposium from Astra Zeneca. None of the other authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained errors in the calculation of the time from iohexol injection to sampling for some of the measurements in the third wave of the survey, which resulted in errors in the reported iohexol-clearance measurements. As a result, Tables 2 and 3 and the Supplementary Table S6 were incorrect. Full information regarding the correction made can be found in the correction for this Article.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eriksen, B.O., Fasiolo, M., Mathisen, U.D. et al. Ambulatory blood pressure as risk factor for long-term kidney function decline in the general population: a distributional regression approach. Sci Rep 13, 14296 (2023). https://doi.org/10.1038/s41598-023-41181-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-41181-7
- Springer Nature Limited