
Abstract
To evaluate the radiological differences between diffuse idiopathic skeletal hyperostosis (DISH) and ankylosing spondylitis (AS) using whole spine computed tomography (CT), including the spine and sacroiliac joint (SIJ). The ossification and bridging of spinal ligament and fusion of the facet joint and SIJ were evaluated in 111 patients who were diagnosed with DISH and 27 patients with AS on the whole spine CT. The number of anterior bridging and shape of bridging (candle-wax-type/ smooth-type) were also evaluated. We further evaluated patients with DISH and AS by matching their age and sex. Complete SIJ fusion was more common in AS, whereas anterior and posterior bony bridging around SIJ was more common in DISH. However, 63% of patients with DISH had a partial or complete fusion. In spinal anterior bony bridging, the majority of patients with AS had the smooth-type, whereas those with DISH had the candle-wax-type. However, some of the patients with DISH (11%) had smooth-type. Intervertebral facet joint fusion is more common in AS. The number of anterior spinal bony bridging was greater in AS than in DISH, especially in the lumbar spine. These results are useful in differentiating DISH from AS and should therefore be considered when making a diagnosis.
Similar content being viewed by others


Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is characterised by calcification and ossification of the anterior vertebral body and peripheral entheses, leading to the bony bridging of multiple vertebral bodies1. The prevalence varies between 2.9% in the Asian population aged > 50 years to 42.0% in European men aged > 65 years2,3,4. The reported risk factors for DISH are old age, male gender and metabolic factors such as obesity, hypertension and type 2 diabetes mellitus5,6.
To diagnose DISH, various criteria have been used in the clinical setting. Of these, Resnick criteria are the most commonly used7, which diagnoses DISH in the spine based on radiographic features based on (1) ‘flowing’ ossification of at least four contiguous vertebral bodies, 2) relative preservation of the intervertebral disc space and 3) absence of apophyseal joint ankylosis and sacroiliac joint (SIJ) erosion, sclerosis, or intraarticular osseous fusion8. DISH is also characterised by swelling ossification of the anterior longitudinal ligament1. As the number of bone bridging of the vertebrae increases, spinal ankylosis becomes severe, which sometimes causes unstable three-column spinal fracture by minor trauma9.
Ankylosing spondylitis (AS) is also known to cause severe spinal ankylosis and is characterised by a chronic inflammatory disease and the presence of the HLA-B27 antigen1,10,11. The prevalence varies 0.03–1.8%12,13. Symptoms usually appear in the 20–30’s and rarely occur after the age of 40 years1. The modified New York criteria show that AS diagnosis is based on radiographic features, including sacroiliitis grade ≥ 2 bilaterally or grade 3–4 unilaterally14. AS is also characterised by annulus fibrosus ossification and adjacent vertebral body bridging anteriorly and laterally known as a ‘bamboo spine’1.
Although the pathological characteristics of AS are different from that of DISH, patients with DISH may radiologically present with SIJ fusion and/or smooth bony bridging of the vertebrae in clinical practice1,15,16. However, no previous reports have compared radiological features of DISH and AS using spinopelvic computed tomography (CT), including the whole spine and SIJ. Moreover, no studies have specifically focused on the characteristics and degrees of SI fusion and spinal ankylosis. Hence, this study aimed to identify the difference in the reconstructed whole spine CT images between DISH and AS to radiologically differentiate the disease from each another.
Materials and methods
The Ethics Committee of Tokyo Medical and Dental University Hospital approved this study (M2020-235) and informed consent was waived since it was a retrospective, anonymized study. All methods were carried out in accordance with relevant guidelines and regulations.
Study design and population
This study was conducted by the Japanese Multicenter Research Organisation for Ossification of the Spinal Ligament with the assistance of the Japanese Ministry of Health, Labour and Welfare. This study was performed using ossification of the posterior longitudinal ligament whole spine CT database, in which 50% of the patients have co-existing DISH17,18. DISH was diagnosed with anterior longitudinal ligament ossification in at least four contiguous vertebral bodies as previously reported17,18. Previous reports15,19,20 demonstrated that pelvic findings were excluded from the diagnostic criteria. Patients with AS were retrospectively enrolled in three institutions. Rheumatologists diagnosed AS using the modified New York criteria14,20. The inclusion criteria were as follows: age > 20 years; and CT images available to determine the location of ossification, bony bridging, and union in the spine and SIJ. The CT images were obtained with 0.5–1.0 mm thick sections using a 64 or 80-row multi-detector unit. The acquisition parameters were 120–150 kV, using auto exposure control.
This study included 138 patients: 111 with DISH (83 males and 28 females; 68.0 ± 11.8 years) and 27 with AS (21 males and 6 females; 47.0 ± 12.5 years). In patients with AS, the duration of symptoms was an average of 18.7 ± 10.0 years. In clinical data, 82% of patients with AS were HLA-B27 positive and 36% were C-reactive protein positive (≥ 0.3 mg/dL). Regarding the medical treatment, 75% of patients with AS used biologics (46%: adalimumab, 26%: infliximab, and 3%: golimumab). We further evaluated patients with DISH and AS by matching their age and sex (DISH: 13 males, 4 females; AS: 13 males, 4 females).
Measured data
Demographic data including age and sex were collected. Furthermore, radiological data of SIJ were collected, such as joint fusion, anterior bony bridging, posterior bony bridging and entheseal bony bridging, which were defined as previously described19 (Fig. 1A–D). Joint fusion was defined as a transverse bony projection within the SIJ that connects the sacrum and ilium19. SIJ fusion was classified into none, one-side partial, both sides partial, one-side complete and another side partial and both sides complete. Complete SIJ fusion was defined as intraarticular bony bridging observed at approximately the whole SIJ area on axial CT images. Partial fusion was defined as intraarticular bony bridging observed at the part of the SIJ area. Anterior bony bridging was defined as an arched bony projection beyond the anterior margin of the SIJ, bridging the ilium and sacrum and without involving the intraarticular part of the joint19. Posterior bony bridging was defined as an arched bony projection beyond the posterior margin of the SIJ, bridging the ilium and sacrum and without involving the intraarticular part of the joint19. Entheseal bony bridging was defined as a transverse bony projection within the posterior sacroiliac ligaments that connect the sacrum and ilium19. Bridging is classified into none, one-side and both sides. Two examiners evaluated the CT images, and interobserver agreement was calculated to evaluate SIJ fusion and anterior, posterior and entheseal bony bridging using 21 samples. The mean interobserver kappa coefficient agreement was 0.78 (95% confidence interval, 0.57–0.97), indicating substantial agreement. The whole spine CT data of ligaments, including anterior bony bridging of the vertebral body and spontaneous facet fusion, were also collected. Anterior bony bridging of the vertebral body was defined as candle-wax-type if it bulged > 3 mm from the anterior vertebral body wall and as smooth-type if it was < 3 mm (Fig. 1E). The number of anterior bony bridging of the vertebral body was evaluated in the cervical, thoracic (T) 1–T6, T7–T12, lumbar and whole spinal regions. Facet fusion was also classified into none, one-side and both sides (Fig. 1F).

CT images of the spine and SIJ. (A) Axial CT image of SIJ shows anterior bony bridging (arrow) and partial fusion of joint (arrowhead). (B) Axial CT image of SIJ shows complete joint fusion. (C) Axial CT image of SIJ shows posterior bony bridging (arrowhead). (D) Axial CT image of SIJ shows anterior bony bridging (arrow) and entheseal bony bridging (arrowhead). (E-1) Sagittal CT image of the whole spine shows 70–100% candle-wax-type. (E-2) Sagittal CT image of the whole spine shows 30–70% candle-wax-type. (E-3) Sagittal CT image of the whole spine shows 0–30% candle-wax-type. (F-1) Sagittal CT image of the facet shows no fusion. (F-2) Sagittal CT image of the facet shows fusion.
Statistical analysis
Differences between DISH and AS were analysed using the Mann–Whitney U-test for continuous variables and Fisher’s exact test for nominal variables. The JMP software version 12 (SAS Institute, Cary, North Carolina, USA) was used for all statistical analyses, and a P-value of < 0.05 was considered to indicate statistical significance.
Results
Characteristics of radiographic data
Table 1 shows the SIJ fusion, anterior, posterior and entheseal bony bridging analyses. Complete SIJ fusion was significantly higher in patients with AS than in those with DISH (AS: none 18.5%, one-side partial 0.0%, both sides partial 14.8%, one-side complete and another side partial 3.7% and both sides complete 63.0%; DISH: none 37.3%, one-side partial 21.8%, both sides partial 38.2%, one-side complete and another side partial 0.9% and both sides complete 1.8%; P < 0.001). Regarding SIJ, 63% of patients with DISH had a partial or complete fusion, whereas 19% of patients with AS did not demonstrate any evidence of SIJ fusion (Table 1). However, Anterior bony bridging (DISH: one-side 25.5% and both sides 41.8%; AS: one-side 0.0% and both sides 7.4%; P < 0.001) and posterior bridging (DISH: one-side 20.0% and both sides 16.4%; AS: one-side 11.1% and both sides 0.0%; P = 0.025) were higher in patients with DISH than those with AS (Table 1). After the age/sex matching, SIJ fusion was also significantly higher in patients with AS than those with DISH (P < 0.001), and anterior bony bridging (P < 0.001) was significantly higher in patients with DISH than those with AS (Table 2).
Table 3 demonstrates the anterior bone bridging analysis on reconstructed spinal images. Anterior bony bridging was significantly higher in patients with AS than those with DISH in the lumbar (DISH: 0.4 ± 0.9, AS: 1.7 ± 2.2; P = 0.009). The percentage of candle-wax-type bone bridging was significantly higher in patients with DISH than those with AS (DISH: 0–30%, 11%; 30–70%, 10%; and 70–100%, 79%; AS: 0–30%, 79%; 30–70%, 21%; 70–100%, 0%; P < 0.001) (Table 3). This result was similar after age/sex matching (Table 3). Notably, 11% of patients with DISH had only 0–30% of candle-wax bridging, whereas up to 21% of patients with AS had 30–70% of candle-wax bridging.
Regarding the spinal facet fusion status, 83% of AS patients had facet fusion, whereas 61% of DISH patients had fusion. The number of both-side facet fusion was significantly higher in patients with AS than in those with DISH in T1–T6 (P = 0.004), either in T7–T12 (P < 0.001), in the lumbar spine (P < 0.001) and in the whole spine (P < 0.001) (Table 4). Conversely, the number of no facet fusion was higher in patients with DISH in T1–T6 (P = 0.002), T7–T12 (P < 0.001), lumbar (P < 0.001) and whole spine (P < 0.001) (Table 4). This result was similar after age/sex matching (Table 4).
Case presentation
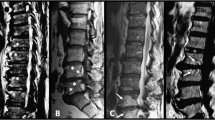
A 70-year-old male patient showed a typical radiological feature of DISH: 70–100% candle-wax-type anterior bony bridging (Fig. 2A), whereas an 82-year-old male patient with DISH showed only 0–30% candle-wax-type bridging (Fig. 2B). A 54-year-old male patient with AS demonstrated typical features of AS 0–30% candle-wax-type (Fig. 2C). A 78-year-old male patient with DISH showed no SIJ fusion but anterior bony bridging of the right-sided SIJ (Fig. 2D), whereas a 75-year-old male patient with DISH had complete SIJ fusion (Fig. 2E). A 63-year-old male patient with AS showed typical complete SIJ fusion (Fig. 2F).

CT images of the case presentation. (A) Sagittal CT image of the whole spine shows 70–100% candle-wax-type in a 70-year-old male patient with DISH. (B) Sagittal CT image of the whole spine shows 0–30% candle-wax-type in an 82-year-old male patient with DISH. (C) Sagittal CT image of the whole spine shows 0–30% candle-wax-type in a 54-year-old male patient with AS. (D) Axial CT image of SIJ shows anterior bony bridging of the right side and no joint fusion in a 78-year-old male patient with DISH. (E) Axial CT image of the SIJ shows complete joint fusion in a 75-year-old male patient with DISH. (F) Axial CT image of the SIJ shows complete joint fusion in a 63-year-old male patient with AS.
Discussion
DISH is generally diagnosed using the Resnick criteria7,8, which are defined by swelling ossification of the anterior longitudinal ligament1 and absence of apophyseal joint ankylosis and SIJ erosion, sclerosis, or intraarticular osseous fusion8. Conversely, AS is often diagnosed using the modified New York criteria14,21. AS is characterised by annulus fibrosus ossification and adjacent vertebral body bridging anteriorly and laterally known as a ‘bamboo spine’1 and SIJ sclerosis, joint space narrowing, erosion, or fusion1. Some reports indicate that DISH and AS can be differentiated based on these radiological characteristics1. However, we sometimes encounter patients who do not have typical radiological findings defined in the abovementioned criteria and are difficult to differentiate between these two diseases. Therefore, this current study compared the detailed radiological characteristics of DISH and AS on spinopelvic CT images.
Previous literature has described that in the later phase of AS, SIJ shows sclerosis, joint space narrowing, erosion, or osseous fusion1. Conversely, in the SIJ of patients with DISH, only ligamentous area obliteration and mild synovial area narrowing can occur; however, SIJ fusion is not observed1. However, some other studies have reported that 23% of DISH is associated with fusion15,19, even though the DISH diagnosis does not require this involvement based on the Resnick criteria8. A previous study suggested that SIJ fusion occurring both in patients with DISH and AS may be possibly due to similar developmental pathways, leading to inflammation-associated enthesitis in younger patients in AS and more mechanistically associated enthesopathy in older patients with DISH19. In this study, as the percentage of partial and complete SIJ fusion was higher in AS than in DISH, up to 63% of patients with DISH had partial or complete SIJ fusion. The SIJ fusion rate in this study was larger than that in previous studies possibly due to the evaluation method in which we included partial SIJ fusion. However, this study demonstrated that SIJ fusion was frequently observed not only in patients with AS but in those with DISH and that might not be the necessary criteria to differentiate DISH from AS.
In the radiological evaluation of anterior and posterior bridging around the SIJ, previous studies have reported that patients with DISH have high anterior and posterior bridging rates around the SIJ. In their reports, 71.6%15, 48%19 and 30%22 of patients with DISH had anterior bony bridging and 5.4%15, 20%19 and 17%22 of patients with DISH had posterior bony bridging. In this study, we found that anterior and posterior bony bridging around the SIJ was significantly more common in DISH than in AS. We separately evaluated one-side and both-side bridging on the SIJ and found that both-side bridging was much higher in DISH than in AS either in anterior or posterior bridging. This finding may be useful for differentiating AS from DISH.
In the anterior spinal bony bridging of the vertebrae, inflammation occurs at the attachment of the annulus fibrosus, and the healing process results in AS syndesmophytes1. Conversely, bridging in DISH results from an ossification process involving the anterior longitudinal ligament1. Although both AS and DISH are characterised by anterior bony bridging, that of AS is generally characterised by smooth bridging ‘bamboo spine’ and that of DISH is by ossification of candle-wax-type ‘flowing mantles’1. We defined both of them as anterior bony bridging. The number of anterior spinal bony bridging was greater in AS than in DISH, especially in the lumbar spine. These results are similar after age and sex matching. As previously reported, DISH mainly affects the thoracic spine18,23. However, our study showed that AS tends to affect the lumbar spine, which may also be one of the differentiating points between DISH and AS.
In analysing the shape of spinal bridging, as expected, the rate of candle-wax-type was much higher in DISH than in AS. This result is consistent with that of a previous report1. However, a certain percentage of patients with DISH had surprisingly smooth-type bridging (0–30% candle-wax-type: 10.8%). Conversely, some patients with AS had candle-wax-type bridging (30–70% candle-wax-type: 20.8%). To the best of our knowledge, this is the first study to reveal that anterior bony bridging in patients with DISH occasionally demonstrated ‘AS-like’ bony bridging. Our findings refute that of the previously reported1,5,8, i.e. the typical appearance of bony bridging in DISH. Physicians should consider that candle-wax-type bridging is not always present in DISH, and this appearance alone cannot prove its diagnosis.
In evaluating the facet joint fusion, the DISH diagnosis requires the absence of joint fusion8. A previous study showed that facet joint ankylosis in AS is more common than that in DISH, and a small number of cervical ones with DISH were observed in whole-body magnetic resonance imaging20. They showed no thoracic and lumbar facet ankylosis in DISH. Another study reported that thoracic and lumbar facets in patients with AS had more inflammatory lesions24. We also found that both-side facet fusions of the thoracic, lumbar and whole spine were more common in AS than in DISH, and results were similar after age and sex matching (Table 4). Interestingly, 61% of patients with DISH had at least one facet fusion in our study. We first demonstrated that facet fusions occur at a high rate not only in AS but also in DISH. For the differential diagnosis of DISH and AS, spinal facet fusion exists should be considered in a certain number of patients with DISH in addition to SIJ fusion.
This study has some limitations. First, the sample size of patients with AS was relatively small because AS is uncommon in our country. However, most of the important comparisons reached statistically significant difference. Second, the number of bony bridging and fusion depends on the patient’s age. However, results after age matching showed a similar tendency. Third, although rare, there may be concurrent patients of AS and DISH, as reported in the past10. Fourth, we could not obtain functional from AS patients included in this study. Large-scale, prospective study is therefore needed to clarify relationships between clinical data and radiological findings.
In conclusion, both sides of complete SIJ fusion are common in patients with AS, and anterior/posterior bridging around the SIJ is common in patients with DISH. However, a considerable number of patients with DISH have SIJ fusion. In the anterior spinal bridging, patients with AS are characterised by smooth bridging, which commonly occurs in the lumbar spine of patients with AS when compared to those with DISH. Conversely, patients with DISH are characterised by candle-wax-type bridging, which commonly occurs in the thoracic spine. However, interestingly, a certain percentage of patients with DISH had smooth-type bridging and some patients with AS had candle-wax-type bridging. Furthermore, a considerable number of patients with DISH showed spinal facet fusion. These facts should be considered when making a diagnosis for AS or DISH.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Olivieri, I. et al. Diffuse idiopathic skeletal hyperostosis: differentiation from ankylosing spondylitis. Curr. Rheumatol. Rep. 11, 321–328. https://doi.org/10.1007/s11926-009-0046-9 (2009).
Kim, S. K. et al. The prevalence of diffuse idiopathic skeletal hyperostosis in Korea. J. Rheumatol. 31, 2032–2035 (2004).
Nascimento, F. A. et al. Diffuse idiopathic skeletal hyperostosis: A review. Surg. Neurol. Int. 5, S122-125. https://doi.org/10.4103/2152-7806.130675 (2014).
Holton, K. F. et al. Diffuse idiopathic skeletal hyperostosis and its relation to back pain among older men: The MrOS Study. Semin. Arthritis Rheum. 41, 131–138. https://doi.org/10.1016/j.semarthrit.2011.01.001 (2011).
Mader, R., Verlaan, J. J. & Buskila, D. in Nat. Rev. Rheumatol. Vol. 9 741–750 (2013).
Pillai, S. & Littlejohn, G. Metabolic factors in diffuse idiopathic skeletal hyperostosis—A review of clinical data. Open Rheumatol. J. 8, 116–128. https://doi.org/10.2174/1874312901408010116 (2014).
Kuperus, J. S. et al. Classification criteria for diffuse idiopathic skeletal hyperostosis: A lack of consensus. Rheumatology (Oxford) 56, 1123–1134. https://doi.org/10.1093/rheumatology/kex056 (2017).
Resnick, D. & Niwayama, G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 119, 559–568. https://doi.org/10.1148/119.3.559 (1976).
Katoh, H. et al. A comparison of cervical and thoracolumbar fractures associated with diffuse idiopathic skeletal hyperostosis—A nationwide multicenter study. J. Clin. Med. https://doi.org/10.3390/jcm9010208 (2020).
Kuperus, J. S. et al. Simultaneous occurrence of ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis: A systematic review. Rheumatology (Oxford) 57, 2120–2128. https://doi.org/10.1093/rheumatology/key211 (2018).
Braun, J. & Sieper, J. Ankylosing spondylitis. Lancet 369, 1379–1390. https://doi.org/10.1016/s0140-6736(07)60635-7 (2007).
Exarchou, S. et al. The prevalence of clinically diagnosed ankylosing spondylitis and its clinical manifestations: A nationwide register study. Arthritis Res. Ther. 17, 118. https://doi.org/10.1186/s13075-015-0627-0 (2015).
Akkoc, N. & Khan, M. A. in Ankylosing Spondylitis and the Spondyloarthropathies 117–131 (Elsevier, 2006).
van der Linden, S., Valkenburg, H. A. & Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 27, 361–368. https://doi.org/10.1002/art.1780270401 (1984).
Yahara, Y. et al. Sacroiliac joint variation associated with diffuse idiopathic skeletal hyperostosis. BMC Musculoskelet. Disord. 21, 93. https://doi.org/10.1186/s12891-020-3105-z (2020).
Nguyen, T. C. T. et al. Morphological characteristics of DISH in patients with OPLL and its association with high-sensitivity CRP: Inflammatory DISH. Rheumatology (Oxford) https://doi.org/10.1093/rheumatology/keac051 (2022).
Hirai, T. et al. Associations between clinical findings and severity of diffuse idiopathic skeletal hyperostosis in patients with ossification of the posterior longitudinal ligament. J. Clin. Med. https://doi.org/10.3390/jcm10184137 (2021).
Nishimura, S. et al. Prevalence and distribution of diffuse idiopathic skeletal hyperostosis on whole-spine computed tomography in patients with cervical ossification of the posterior longitudinal ligament: A multicenter study. Clin. Spine Surg. 31, E460–E465. https://doi.org/10.1097/BSD.0000000000000701 (2018).
Leibushor, N., Slonimsky, E., Aharoni, D., Lidar, M. & Eshed, I. CT abnormalities in the sacroiliac joints of patients with diffuse idiopathic skeletal hyperostosis. AJR Am. J. Roentgenol. 208, 834–837. https://doi.org/10.2214/ajr.16.16994 (2017).
Weiss, B. G., Bachmann, L. M., Pfirrmann, C. W., Kissling, R. O. & Zubler, V. Whole body magnetic resonance imaging features in diffuse idiopathic skeletal hyperostosis in conjunction with clinical variables to whole body MRI and clinical variables in ankylosing spondylitis. J. Rheumatol. 43, 335–342. https://doi.org/10.3899/jrheum.150162 (2016).
McVeigh, C. M. & Cairns, A. P. Diagnosis and management of ankylosing spondylitis. BMJ 333, 581–585. https://doi.org/10.1136/bmj.38954.689583.DE (2006).
Adel, H. et al. CT-based evaluation of diffuse idiopathic skeletal hyperostosis in adult population; prevalence, associations and interobserver agreement. J. Clin. Densitom. 23, 44–52. https://doi.org/10.1016/j.jocd.2018.12.001 (2020).
Kim, B. S. et al. Prevalence of diffuse idiopathic skeletal hyperostosis diagnosed by whole spine computed tomography: A preliminary study. Clin. Orthop. Surg. 10, 41–46. https://doi.org/10.4055/cios.2018.10.1.41 (2018).
Maksymowych, W. P., Crowther, S. M., Dhillon, S. S., Conner-Spady, B. & Lambert, R. G. Systematic assessment of inflammation by magnetic resonance imaging in the posterior elements of the spine in ankylosing spondylitis. Arthritis Care Res. (Hoboken) 62, 4–10. https://doi.org/10.1002/acr.20007 (2010).
Acknowledgements
We would like to thank enago (https://www.enago.jp) for English language editing.
Funding
This work was supported by a Health and Labour Science Research grant (number 201610008B) and a grant from the Japan Agency for Medical Research and Development (number 16ek0109136h0002).
Author information
Authors and Affiliations
Contributions
T.T. and T.Y. conceived and designed the study. All authors collected the data. T.T. and T.Y. prepared the manuscript, and all authors reviewed and edited the manuscript. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Takahashi, T., Yoshii, T., Mori, K. et al. Comparison of radiological characteristics between diffuse idiopathic skeletal hyperostosis and ankylosing spondylitis: a multicenter study. Sci Rep 13, 1849 (2023). https://doi.org/10.1038/s41598-023-28946-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-28946-w
- Springer Nature Limited