
Abstract
Measuring Huntingtin (HTT) protein in peripheral cells represents an essential step in biomarker discovery for Huntington’s Disease (HD), however to date, investigations into the salivary expression of HTT has been lacking. In the current study, we quantified total HTT (tHTT) and mutant HTT (mHTT) protein in matched blood and saliva samples using single molecule counting (SMC) immunoassays: 2B7-D7F7 (tHTT) and 2B7-MW1 (mHTT). Matched samples, and clinical data, were collected from 95 subjects: n = 19 manifest HD, n = 34 premanifest HD (PM), and n = 42 normal controls (NC). Total HTT and mHTT levels were not correlated in blood and saliva. Plasma tHTT was significantly associated with age, and participant sex; whereas salivary mHTT was significantly correlated with age, CAG repeat length and CAP score. Plasma and salivary tHTT did not differ across cohorts. Salivary and plasma mHTT were significantly increased in PM compared to NC; salivary mHTT was also significantly increased in HD compared to NC. Only salivary tHTT and mHTT were significantly correlated with clinical measures. Salivary HTT is uniquely associated with clinical measures of HD and offers significant promise as a relevant, non-invasive HD biomarker. Its use could be immediately implemented into both translational and clinical research applications.
Similar content being viewed by others


Introduction
Huntington’s Disease (HD) is a progressive, genetic neurodegenerative disorder caused by unstable CAG repeat expansions in the first exon of the Huntingtin gene (HTT). This mutation translates into a polyglutamine repeat in the Huntingtin protein, the length of which varies by CAG repeat expansion number. Pathogenesis in HD arises largely from the expression of the mutant huntingtin protein (mHTT), leading to the formation of toxic soluble protein oligomers and insoluble aggregates that contribute to the disruption of many intracellular, predominantly cortical and striatal pathways. The pathological expression of mHTT leads to the progressive development of a range of clinical signs and symptoms, which may begin with subtle cognitive and behavioral changes followed by the onset of involuntary motor symptoms, ultimately leading to a premature death 15–20 years after onset1,2,3,4. Conversely, full-length huntingtin protein has proposed roles in neurogenesis, axonal transport and synaptic transmission, as well as in preventing apoptosis and excitotoxicity5. Previous studies have reported associations between cerebrospinal (CSF) mHTT and functional, cognitive and motor symptom progression6,7,8, and we have previously reported an association between salivary total huntingtin protein (tHTT) levels and disease progression9. To our knowledge, no study has comprehensively analyzed salivary mHTT in HD, or compared salivary tHTT and mHTT to levels in plasma. The aim of this study was therefore to quantify levels of tHTT and mHTT in saliva and plasma of premanifest and manifest HD patients, as well as normal controls, and investigate associations between these markers with clinical measures.
Methods
Human subjects
This study was approved by the University of California, San Diego (UCSD) Institutional Review Board, in accordance with the requirements of the Code of Federal Regulations on the Protection of Human Subjects, and conducted in accordance with the Declaration of Helsinki. Patients were recruited from the UCSD Huntington’s Disease Society of America (HDSA) Center of Excellence, and carried a genetic confirmation of the HTT mutation with family history of the disorder. Premanifest (PM) HD individuals had more than ≥ 38 CAG repeats, and a Unified Huntington's Disease Rating Scale (UHDRS) diagnostic confidence rating below 4. Manifest HD patients had a diagnostic confidence rating of 4, indicating that a clinician had ≥ 99% certainty that the patient presented with “‘unequivocal presence of an otherwise unexplained extrapyramidal movement disorder”10. The UHDRS was developed by the Huntington Study Group, and is used as a major outcome measure in controlled clinical trials10,11. Normal controls (NC) had no reported history of neurological conditions, psychiatric disorders or gout, and no use of psychoactive substances or medications. All participants gave written informed consent prior to sample collection. Demographic and disease data were collected at the time of sample collection, including sex, age, CAG repeat length, and years of education.
Clinical assessment
PM and HD study participants underwent a single clinical assessment, which included cognitive testing, behavioral and functional measures, and motor ratings. The cognitive battery included the Mini-Mental State Examination (MMSE)12, Montreal Cognitive Assessment (MoCA)13, Symbol Digit Modalities test (SDMT)14 and Stroop word reading test (SWR). Behavioral and psychiatric changes were assessed using the short form Problem Behaviors Assessment (PBA-s)15 and the Hospital Anxiety and Depression Scale/Snaith Irritability Scale (HADS-SIS)16. Functional proficiency was evaluated using the UHDRS10 Total Functional Capacity (TFC). Motor dysfunction was assessed using the UHDRS Total Motor Score (TMS). The sum of all maximal chorea sub-scores were also noted10. The SWR, SDMT, TFC and TMS were also incorporated into the composite UHDRS score (cUHDRS) as an additional measure of disease progression17. Predicted years to 60% probability of manifest disease onset was calculated using a formula which incorporate CAG repeat length and current age, determined by Langbehn and colleagues18. The normalized prognostic index (PIN) score for predicting PM disease progression19, which incorporates patient CAG repeat length, age, SDMT score, and TMS19 was also calculated, as an additional measure of disease progression.
Sample collection
Blood from consenting individuals was drawn by venipuncture into 2 ml lavender/EDTA tubes. EDTA/whole blood was mixed well by inversion and spun at 900 g for 15 min. The supernatant was isolated, aliquoted into 1 ml aliquots, snap frozen and stored at − 80 °C. All donors were asked to refrain from smoking, eating, drinking, or oral hygiene procedures for at least 1 h prior to sample collection. Saliva samples were collected between 10 a.m. and 4 p.m. using the passive drool method according to previously established protocols20. Roughly 2 ml of unstimulated whole saliva was obtained. Samples were immediately frozen at − 20 °C at the time of collection, then stored at − 80 °C. At the time of use, saliva samples were thawed and centrifuged (10,000×g; 10 min; 4 °C) to remove insoluble material and cellular debris. All blood and saliva samples were kept cold prior to the running of assays, to reduce the likelihood of protein degradation.
Biomarker protein analysis
Levels of tHTT and mHTT protein in saliva and plasma were analyzed at IRBM S.p.A, Italy. Prior to analysis, plasma samples were processed by centrifugation (14000 rpm × 10 min at 4 °C) to remove debrides, and absolute Tween-20 was added to the resulting supernatant. Saliva samples were diluted 1:1 in 2× Lysis buffer (2× phosphate buffered saline, 0.8% Triton-X, protease inhibitor) in order to avoid proteolysis from digestive enzymes. Then samples were then clarified from debrides by centrifugation (14000 rpm × 10 min at 4 °C). Total HTT and mHTT was measured in each biofluid using the 2B7-D7F7 Single Molecule Counting (SMC) assay and three technical replicates21 for tHTT, mHTT was measured using the 2B7-MW1 SMC assay and two technical replicatesHTT22, on an Erenna® platform. The 2B7-MW1 SMC assay is specific for mHTT, whereas the 2B7-D7F7 assay quantifies HTT protein in a polyglutamine length-independent manner (mHTT and non-expanded wild-type HTT combined)21,22. Plasma samples were analyzed using 15 μL/well for 2B7-D7F7 SMC assay and 135 μL/well for the 2B7-MW1 SMC assay. Saliva samples were analyzed using 150 μL/well for 2B7-D7F7 SMC assay and for 2B7-MW1 SMC assay22. A calculated concentration above the lower limit of quantification (LLoQ) was obtained for 99% of tHTT and 54% mHTT in plasma, and 95% tHTT and 62% mHTT in saliva. Most values below LLoQ belonged to the control cohort (Table 1). Values below the lower limit of quantification (LLoQ) were substituted with 2.5 fM (half LLoQ) for analysis.
Western blot analysis
Total protein levels were measured a DC Protein Assay (Bio-Rad Laboratories, Hercules, CA, USA) on the day of and prior to gel electrophoresis. Samples were diluted to 800 pg/ml with deionized water, and then mixed 3:4 with NuPAGE™ LDS Sample Buffer (4×) (Thermo Fisher Scientific, MA, USA). The samples were denatured for 10 min at 70 °C, and 15 µg total protein was subsequently loaded into wells of a NuPAGE™ 3 to 8%, Tris–Acetate, 1.5 mm, Mini Protein Gel (Thermo Fisher Scientific), Proteins were separated at 150 V with NuPAGE™ 1 × Tris–Acetate Running Buffer until the sample buffer had migrated to 1 cm from the bottom of the gel (approximately 1 h). The proteins were then transferred to a Thermo Fisher nitrocellulose membrane at a constant 40 mA overnight with icepack cooling and NuPAGE™ 1× LDS Transfer Buffer. The nitrocellulose membranes were probed with Ponceau S staining (Cell Signalling Technology, Frankfurt, Germany), blocked for 1 h in Tris buffered saline with 20% Tween-20 (Thermo Fisher Scientific) and 5% non-fat milk powder (5% NFMP TBST). The nitrocellulose membranes were then probed via overnight incubation with either 1:500 anti-total HTT antibody (4E10, Santa Cruz Biotechnology, Inc., CA, USA) or anti-mutant HTT antibody (MW1, Developmental Studies Hybridoma Bank, IA, USA) in 5% NFMP TBST, followed by 1:10,000 goat anti-mouse IgG:HRP-conjugated antibody (Merck, NY, USA) in 5% NFMP TBST for 1 h. 4E10 and MW1 antibody are well characterized for tHTT and mHTT, respectively23,24,25. Bands were detected with Pierce™ ECL Western Blotting Substrate, imaged for 5 min (4E10) or 8 min (MW1) on a FluoroChem M Imaging system (Bio-techne, MN, USA). Molecular weight markers were determined using the PageRuler™ Unstained Protein Ladder, with bands marked in pencil following Ponceau S staining, and imaged using the white-light function on the FluoroChem M Imaging system.
Statistical analysis
Analyses were conducted with GraphPad Prism version 8.4.2 for Windows (GraphPad Software, La Jolla, CA, USA). Twelve matched saliva and blood samples from HTT-mutation carriers (13% of total cohort) were collected and analyzed separately as part of a unique, second batch (batch 2); significant batch variation was accounted for through global linear normalization of these samples, using the ratio of the batch 1 HTT-mutation carrier sample mean divided by the batch 2 sample mean, for each analyte (Suppl. Fig. 1)26,27. Overall, three participants had both salivary tHTT and mHTT below the lower limit of detection, and one participant had both plasma tHTT and mHTT below the lower limit of detection; these values were excluded. One additional salivary tHTT value and one plasma tHTT value were identified visually as outliers and excluded (Suppl Fig. 2). Analyses which corrected for covariates were conducted using IBM® SPSS® Statistics version 25 for Windows (IBM Corp., NY, USA). As unquantified values below LLoQ were substituted with a value of 2.5 fM, all comparison which used continuous data were tested using non-parametric analyses. Mutant HTT values were log-transformed for graphical presentation, after statistical testing. The comparison of plasma and salivary tHTT levels by diagnostic group was conducted using Mann–Whitney U-test, followed by Quade’s non-parametric analysis of covariance (Quade’s ANCOVA), correcting for covariates. Due to the high proportion of LLoQ-substituted mHTT values, particularly in the control cohort, comparisons between diagnostic cohorts for mHTT were conducted using Fisher’s exact test for values over and below LLoQ. All tests conducted were two-sided.
Results
Participant characteristics
Plasma and saliva were collected from 95 individuals: 42 NC, 34 PM and 19 HD. Demographic characteristics are summarized in Table 2. Cohorts differed significantly by age (Kruskal–Wallis χ2 = 10.86, p = 0.004); the PM cohort was significantly younger than the NC cohort (p = 0.003). HD patients had significantly higher CAP scores (p = 0.0001) compared to the PM cohort (Table 2). Plasma tHTT (r = 0.29, p = 0.005), and salivary mHTT (r = − 0.27, p = 0.01) but not plasma mHTT or salivary tHTT, was significantly correlated with age, irrespective of diagnostic cohort. Plasma tHTT, but no other HTT measure, was moderately correlated with years of education (r = 0.20, p = 0.05). Salivary mHTT, but no other HTT measure, was significantly correlated with CAG repeat length (r = 0.33, p = 0.02) and CAP score (r = 0.34, p = 0.01). Plasma tHTT (U = 723, p = 0.005), but no other measure, differed significantly by participant sex.
Diagnostic potential of plasma and salivary tHTT and mHTT
Total HTT (Fig. 1a) and mHTT levels (Fig. 1b) were not correlated in saliva and plasma.

Associations between plasma and salivary tHTT (a) and mHTT (b) in HTT mutation-carriers. Data in (b) was log-transformed for graphical presentation after statistical testing. Statistical comparisons conducted using Spearman’s rho.
Plasma tHTT and salivary tHTT were not significantly different across diagnostic groups (> 0.05) (Fig. 2a). The number of plasma tHTT values below LLOQ across different diagnostic cohorts was just above statistical significance (χ2 = 5.70, p = 0.058); posthoc chi-square tests showed that there were significantly more plasma mHTT values below LLOQ in the NC cohort compared to PM (χ2 = 5.53, p = 0.02; OR, 95% CI = 3.5, 1.2–10.5) but no difference between NC and HD, or PM and HD (p > 0.05) (Fig. 2b). The number of salivary mHTT values below LLOQ were significantly different across diagnostic cohorts (χ2 = 7.54, p = 0.02); posthoc chi-square tests showed that there were significantly more salivary mHTT values below LLOQ in the NC cohort, compared to PM (χ2 = 5.16, p = 0.02, OR, 95% CI = 3.7, 1.2–10.2), and compared to HD (χ2 = 4.22, p = 0.04; OR, 95% CI = 4.9, 1.1–23.5), but no difference between PM and HD cohorts (p > 0.05) (Fig. 2b).

Total HTT (a) and mutant HTT (b) levels in saliva and plasma of normal controls (NC), premanifest HD individuals (PM) and manifest HD patients (HD). Plasma and salivary tHTT did not differ by diagnostic cohort (a). Plasma mHTT was more frequently below the Lower Limit of Quantification (LLoQ) in NC compared to PM, and salivary mHTT levels were more frequently below LLoQ in NC compared to HD and PM (b). Total HTT significance determined by Kruskal–Wallis test; mHTT significance determined by Fisher’s exact test. Data in (b) was log-transformed for graphical presentation after statistical testing; *p < 0.05.
Correlations between plasma and saliva tHTT and mHTT, and clinical symptoms in HTT mutation-carriers
Correlations were analyzed using the PM, HD, and combined PM + HD (gene (+)) cohort, both without (Table 3) and with adjusting for age, CAG repeat length, and sex (Suppl. Table 1). In the PM cohort, salivary tHTT and mHTT were significantly correlated with each other, TMS, Chorea, and DCL scores. In addition, salivary mHTT was also correlated with Timed Up and Go (TUG) score. In the HD cohort, salivary tHTT was associated with TMS and Chorea scores, and salivary mHTT was associated with age and CAG repeat number. In the combined HTT-mutation carrier cohort (PM + HD), salivary mHTT levels were associated with salivary tHTT levels, CAG repeat number, CAP score, PIN score, predicted years to 60% probability of manifest symptom onset, Independence score, TMS, Chorea, DCL, and TUG (Table 3). Similar significant correlations were observed after correcting for age, CAG repeat number, and sex (Suppl. Table 1). Associations between salivary mHTT and salivary tHTT, and TMS, in the PM cohort, and CAP score, predicted years to 60% manifest symptom onset, TMS, DCL in the PM + HD cohort, passed Bonferrori-adjusted p value cut-off scores (Table 3). Significant correlations are presented graphically in Suppl. Fig. 3 (salivary tHTT), and Suppl. Fig. 4 (salivary mHTT).
Total HTT protein isoforms vary in saliva and plasma
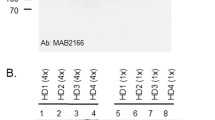
Considering tHTT and mHTT correlations differed between blood and saliva, we hypothesized that these proteins may be uniquely processed in each biofluid. We therefore measured tHTT and mHTT protein levels in saliva and blood from HTT mutation-carriers, using Western Blot. This preliminary qualitative investigation of tHTT (Fig. 3, lanes a–f) and mHTT (Fig. 3, lanes h–m) protein in 600 µg/ml aliquots of blood (Fig. 3a–c,h–j) and saliva (Fig. 3d–f,k–m) from 3 PM participants showed distinct bands in each biofluid.

Total and mutant HTT in blood and saliva from premanifest HD individuals. Fifteen micrograms of blood (a–c,h–j) and saliva (d–f,k–m) were probed with antibodies for total HTT (1:500 4E10; lanes a–f) and mutant HTT (1:500 MW1; lanes h–m) on two NuPAGE 3–8% Tris–Acetate Protein Gels, run simultaneously in the same electrophoresis and transfer system. Blood and saliva samples were matched (participant 1: a,d,h,k; participant 2: b,e,i,l; participant 3: c,f,j,m). Lane g and m show white-light images of pencil markings of the PageRuler™ Unstained Protein Ladder, marked after Ponceau S membrane staining; *indicates a high molecular weight marker detected on Ponceau S staining, which does not correspond to any PageRuler™ Unstained Protein Ladder listed molecular weights.
Discussion
In this study, we have observed significant differences in salivary and plasma mHTT protein levels, but not salivary or plasma tHTT levels, when comparing controls, PM and HD cohorts. Specifically, a significantly greater proportion of PM individuals had detectable salivary and plasma mHTT levels compared to controls. A greater proportion of HD individuals also had detectable salivary mHTT levels compared to controls. The absence of significant different in tHTT in HD compared to controls contrasts with a reported decrease in tHTT in human peripheral blood mononuclear cells, measured by ELISA assay and published by Massai and colleagues28, as well as our previously reported increase in salivary tHTT in manifest HD patients compared to controls, also measured by ELISA assay9. In our previous study, salivary tHTT was positively correlated with UHDRS score and negatively correlated with TFC9, relationships not observed in the current study. However, we did observe significant associations between saliva tHTT levels and other clinical measures: Chorea score, TMS, and DCL. These associations, in addition to correlations between salivary tHTT and mHTT, and salivary mHTT and CAP, PIN and predicted years to manifest onset score in our PM + HD cohort, suggests that these markers are associated with disease progression. Curiously however, while salivary tHTT levels were positively associated with Chorea and TMS in our PM cohort, they were negatively associated in our HD cohort. It is possible that the association in manifest HD patients is influenced by other factors of more severe disease progression. Indeed, differential neurochemical changes have previously been associated with early-disease chorea, compared to late-disease rigidity in HD29. In addition, we have previously reported significant differences in levels of plasma neurofilament light between PM and HD cohorts30, further suggesting a notable neurophysiological shift associated with disease progression. Based on findings from the current study, salivary tHTT levels may increase with motor symptoms, measured here by Chorea score and TMS, in PM individuals, and subsequently decrease with further motor deterioration, or the onset of rigidity, in manifest HD individuals.
Regarding the discrepancy between our two studies, the cohorts used in the previous study and current study did not differ in demographic or disease characteristics, however the two studies did differ in assay methodology, sensitivity and median HD salivary tHTT levels (ELISA (1500 fM) vs SMC (469fM)). Furthermore, the ELISA utilized in our previous study included an antibody which targets a region between amino acids 802–9409, whereas the SMC assay used in the current study targets a proline at amino acid 1220. Previously, an extensive investigation of HTT fragments in a mouse model of HD identified 14 prominent N-terminal fragments ranging from the mutant exon 1 fragment to full length HTT31. It is therefore possible that our previous and current studies have documented two different disease pathologies: an increase in full-length tHTT expression9, countered by the occurrence of possible protein degradation starting from the 3’ region. Alternatively, it is possible that a high concentration of proteolytic enzymes in saliva, contributed by bacteria and oral cavity cells20,32, has lead to substantial degradation of HTT, thereby affecting the observed results. Specifically, such degradation may have influenced our reported findings for salivary tHTT, as a portion of HTT proteins ‘captured’ during the incubation step with the N-terminal 2B7 antibody, may by cleaved in such a way that they lack the epitope for the D7F7 antibody, which binds around amino acid residue 122033. However, previous research has shown that the removal of insoluble material, including bacteria-bound mucins, during saliva sample processing, as well as the the maintenance of samples on ice during handling, and the storage of saliva samples at − 80°C—all of which were performed in this study—preserved the integrity of salivary proteins32. Interestingly, Massai and colleagues, who reported a decrease in tHTT in human peripheral blood mononuclear cells, utilized an antibody which targets amino acids 1844–2131 of the HTT protein28, which is much closer to the 3′ terminal than those antibodies used in either of our reported studies, suggesting that if degradation is responsible for this discrepancy between studies, it is not unique to saliva. Iit is important to note, however, that the antibody used by Massai and colleagues, 4E10, has also been shown to recognize a 1–573 amino acid N-terminal fragment of HTT in a poly-Q dependent manner, suggesting potential reactivity with one or more additional HTT epitopes34. Without the existence of a calibration set of recombinant tHTT proteins of varying fragment lengths, the measure of tHTT protein, which may be cleaved by numerous proteases, remains a relative quantitative assay, and the potential to compare across assay and antibody platforms is limited9,34,35.
The absence of inter-biofluid correlations between plasma and salivary tHTT or mHTT, yet the presence of intra-biofluid correlations between saliva tHTT and mHTT, but not plasma tHTT and mHTT, observed in the current study, supports the likelihood that HTT in each biofluid has a different origin, or that there are biofluid-specific variations in transcriptional or post-translational regulation or aggregation. A 2015 analysis of CSF and plasma, using the same single-molecule counting immunoassay as the current study, similarly found no association between mHTT in the two biofluids7. The three main salivary glands—the sublingual, submandibular and parotid glands—are innervated by the superior and inferior salivary nuclei, located in the brainstem36, which may provide a physiological explanation for the determination of saliva-specific correlations, particularly given that brainstem neurodegeneration has been proposed in HD37. Indeed, it is possible that salivary protein levels have a greater direct association with cortical or subcortical pathophysiology, compared to protein changes in blood. It would be of interest to determine whether salivary tHTT and mHTT levels are associated with those in CSF, or entirely unique. We provide further preliminary evidence for biofluid-specific post-translational modification or processing of blood and salivary tHTT and mHTT, through the presentation of unique tHTT and mHTT bands in a western blot analysis of each biofluid. Interestingly, our preliminary western blot findings, using the 4E10 antibody to detect tHTT, show one band above 200 kDa in saliva, compared to the same band and multiple smaller bands in plasma. When assessed using the polyQ-binding MW1 antibody, only the > 200 kDa band is present in saliva, and only the smaller (≤ 120 kDa) bands are present in plasma. This conflicts with our earlier hypothesized scenario in which proteolytic degradation is high in saliva, and suggests greater proteolytic cleavage in plasma. Considered within the context of our earlier scenario in which cleaved 2B7-captured HTT fragments are not detected by the SMC D7F7 antibody, these 120 kDa HTT fragments, detected in plasma with the amino acid 1844–2131 targeting 4E10 antibody, would similarly not be detected by the SMC assay. As aforementioned, the proteolytic cleavage of HTT, and the lack of a calibration set of recombinant tHTT proteins of varying fragment lengths, is a recognized limitation in assessing HTT protein levels.
This study is not without limitations. In addition to the potential presence of proteolytic enzymes in saliva and/or plasma, our limited sample size and the recording of mHTT below the lower limit of quantification in a number of these samples, restricts the conclusions that we can draw from these findings. The detection of plasma and salivary mHTT in our control cohort must also be addressed, however is not unique to our study. Previous studies have detected mHTT in control blood, and cheek buccal cells, and these studies have suggested that assay interfering factors present in the plasma collection tubes, or off-target background detection in the absence of a target, may be the cause of mHTT detection in controls22,38,39. In addition, while the MW1 antibody is frequently used and validated in HD research, MW1 binds to a non-pathological glutamine length (Q10) and a number of previous studies have suggested that it may bind to wild-type HTT40,41,42. Such lack of specificity may also explain the detection of mHTT in our control cohort. The MW1 antibody is also limited in that it’s binding affinity is affected by CAG repeat length, such that individuals with higher CAG repeat lengths would show greater levels of MW1 binding. We have accounted for the effect of CAG repeat length on MW1 binding by adjusting for this covariate in our correlation analyses, however acknowledge that some variance may still remain.
Our research group is unique in its analysis of HTT protein from whole saliva, and we acknowledge that much work still needs to be done to optimize both the mHTT assay, and the use of this assay in saliva.
Overall, our study presents a compelling argument for the inclusion and analysis of saliva to further the understanding, diagnosis and prognosis of HD. While saliva has been long used as a diagnostic tool for local afflictions which directly affect the oral cavity, such as viral load, drug screening, it has been underappreciated as a vector for CNS-sourced biomarkers of neurodegenerative and psychiatric disorders. We show that mHTT is uniquely processed in saliva, compared to blood, and contend that further investigation into this biofluid will provide new information regarding the development and disease progression of Huntington’s Disease.
Data availability
Anonymized summary data are available from the corresponding author by reasonable formal request from qualified researchers, subject to a data sharing agreement and in compliance with the requirements of the funding bodies and institutions.
References
Wexler, N. S. Venezuelan kindreds reveal that genetic and environmental factors modulate Huntington’s disease age of onset. Proc. Natl. Acad. Sci. USA. 101(10), 3498–3503 (2004).
Andresen, J. M. et al. The relationship between cag repeat length and age of onset differs for Huntington’s disease patients with juvenile onset or adult onset. Ann. Hum. Genet. 71(3), 295–301 (2007).
Andrew, S. E. et al. The relationship between trinucleotide (cag) repeat length and clinical features of Huntington’s disease. Nat. Genet. 4(4), 398–403 (1993).
Arrasate, M. & Finkbeiner, S. Protein aggregates in Huntington’s disease. Exp. Neurol. 238(1), 1–11 (2012).
Cattaneo, E., Zuccato, C. & Tartari, M. Normal huntingtin function: An alternative approach to Huntington’s disease. Nat. Rev. Neurosci. 6(12), 919–930 (2005).
Byrne, L. M. et al. Evaluation of mutant huntingtin and neurofilament proteins as potential markers in Huntington’s disease. Sci. Transl. Med. 10(458), eaat7108 (2018).
Wild, E. J. et al. Quantification of mutant huntingtin protein in cerebrospinal fluid from Huntington’s disease patients. J. Clin. Investig. 125(5), 1979–1986 (2015).
Rodrigues, F. B. et al. Mutant huntingtin and neurofilament light have distinct longitudinal dynamics in Huntington’s disease. Sci. Transl. Med. 12(574), eabc2888 (2020).
Corey-Bloom, J. et al. Salivary levels of total huntingtin are elevated in Huntington’s disease patients. Sci. Rep. 8(1), 1–9 (2018).
Kieburtz, K. et al. Unified Huntington’s disease rating scale: Reliability and consistency. Neurology 11(2), 136–142 (2001).
Sun, W. et al. Huntington’s disease progression: A population modeling approach to characterization using clinical rating scales. J. Clin. Pharmacol. 60(8), 1051–1060 (2020).
Folstein, M. F., Folstein, S. E. & McHugh, P. R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12(3), 189–198 (1975).
Nasreddine, Z. S. et al. The montreal cognitive assessment, moca: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53(4), 695–699 (2005).
Smith, A. Symbol digit modalities test. In A Compendium of Neuropsychological Tests 2nd edn (eds Spreen, O. & Strauss, E.) (Western Psychological Services, 1982).
Craufurd, D., Thompson, J. C. & Snowden, J. S. Behavioral changes in Huntington disease. Cogn. Behav. Neurol. 14(4), 219–226 (2001).
Zigmond, A. S. & Snaith, R. P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 67(6), 361–370 (1983).
Schobel, S. A. et al. Motor, cognitive, and functional declines contribute to a single progressive factor in early hd. Neurology 89(24), 2495–2502 (2017).
Langbehn, D. R., Hayden, M. R., Paulsen, J. S., PREDICT‐HD Investigators. Cag-repeat length and the age of onset in Huntington disease (HD): A review and validation study of statistical approaches. Am. J. Med. Genet. B Neuropsychiatr. Genet. 153(2), 397–408 (2010).
Long, J. D. et al. Validation of a prognostic index for Huntington’s disease. Mov. Disord. 32(2), 256–263 (2017).
Granger, D. A. & Taylor, M. K. Salivary Bioscience: Foundations of Interdisciplinary Saliva Research and Applications (Springer Nature, 2020).
Fodale, V. et al. Quantifying huntingtin protein in human cerebrospinal fluid using a novel polyglutamine length-independent assay. J. Huntingtons Dis. 1–15 (2022) (in Press).
Fodale, V. et al. Validation of ultrasensitive mutant huntingtin detection in human cerebrospinal fluid by single molecule counting immunoassay. J. Huntingtons Dis. 6(4), 349–361 (2017).
Ananbeh, H. et al. Huntingtin co-isolates with small extracellular vesicles from blood plasma of tghd and ki-hd pig models of Huntington’s disease and human blood plasma. Int. J. Mol. Sci. 23(10), 5598 (2022).
Wilkinson, F. et al. Localization of rabbit huntingtin using a new panel of monoclonal antibodies. Mol. Brain Res. 69(1), 10–20 (1999).
Ko, J., Ou, S. & Patterson, P. H. New anti-huntingtin monoclonal antibodies: Implications for huntingtin conformation and its binding proteins. Brain Res. Bull. 56(3–4), 319–329 (2001).
Schadt, E. E., Li, C., Ellis, B. & Wong, W. H. Feature extraction and normalization algorithms for high-density oligonucleotide gene expression array data. J. Cell Biochem. 84(S37), 120–125 (2001).
Välikangas, T., Suomi, T. & Elo, L. L. A systematic evaluation of normalization methods in quantitative label-free proteomics. Brief Bioinform. 19(1), 1–11 (2018).
Massai, L. et al. Development of an elisa assay for the quantification of soluble huntingtin in human blood cells. BMC Biochem. 14(1), 1–9 (2013).
Storey, E. & Beal, M. Neurochemical substrates of rigidity and chorea in Huntington’s disease. Brain 116(5), 1201–1222 (1993).
Parkin, G. M., Corey-Bloom, J., Snell, C., Castleton, J. & Thomas, E. A. Plasma neurofilament light in Huntington’s disease: A marker for disease onset, but not symptom progression. Parkinsonism Relat. Disord. 87, 32–38 (2021).
Landles, C. et al. Proteolysis of mutant huntingtin produces an exon 1 fragment that accumulates as an aggregated protein in neuronal nuclei in Huntington disease. J. Biol. Chem. 285(12), 8808–8823 (2010).
Chevalier, F. et al. Proteomic studies of saliva: A proposal for a standardized handling of clinical samples. Clin. Proteomics. 3(1), 13–21 (2007).
Fischer, D. F. et al. Development of mab-based polyglutamine-dependent and polyglutamine length-independent huntingtin quantification assays with cross-site validation. PLoS ONE 17(4), e0266812 (2022).
Fodale, V. et al. Analysis of mutant and total huntingtin expression in Huntington’s disease murine models. Sci. Rep. 10(1), 1–13 (2020).
Lee, J. W. et al. Fit-for-purpose method development and validation for successful biomarker measurement. Pharm. Res. 23(2), 312–328 (2006).
Proctor, G. B. The physiology of salivary secretion. Periodontol. 70(1), 11–25 (2016).
Rüb, U., Vonsattel, J. P. G., Heinsen, H. & Korf, H.-W. Widespread brainstem neurodegeneration in Huntington’s disease (hd). In The Neuropathology of Huntington’s Disease: Classical Findings, Recent Developments and Correlation to Functional Neuroanatomy Vol. 217 83–90 (Springer, 2015).
Hensman Moss, D. J. et al. Quantification of huntingtin protein species in Huntington’s disease patient leukocytes using optimised electrochemiluminescence immunoassays. PLoS ONE 12(12), e0189891 (2017).
Weiss, A. et al. Mutant huntingtin fragmentation in immune cells tracks Huntington’s disease progression. J. Clin. Investig 122(10), 3731–3736 (2012).
Owens, G. E., New, D. M., West, A. P. Jr. & Bjorkman, P. J. Anti-polyq antibodies recognize a short polyq stretch in both normal and mutant huntingtin exon 1. J. Mol. Biol. 427(15), 2507–2519 (2015).
Klein, F. A. et al. Linear and extended: A common polyglutamine conformation recognized by the three antibodies mw1, 1c2 and 3b5h10. Hum. Mol. Genet. 22(20), 4215–4223 (2013).
Li, P. et al. The structure of a polyq–anti-polyq complex reveals binding according to a linear lattice model. Nat. Struct. Mol. Biol. 14(5), 381–387 (2007).
Acknowledgements
This work was supported the National Institutes of Health (NS111655 to E.A.T.); the UCSD Huntington’s Disease Society of America Center of Excellence; and the UCSD Shiley-Marcos Alzheimer’s Disease Research Center NIH P50 AG005131. These funding sources had no role in study design, conduct, analysis, interpretation or writing of the manuscript, or in the decision to submit the manuscript. We thank Dr. Douglas Macdonald (CHDI Management/CHDI Foundation) for scientific input regarding the HTT assays.
Author information
Authors and Affiliations
Contributions
Research project conceptualization and methodology: J.C.-B., E.A.T.; Data collection: C.S., H.S., A.L., M.D., A.B.; Statistical analysis: G.M.P.; Drafting of manuscript: G.M.P; manuscript review and critique: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Parkin, G.M., Corey-Bloom, J., Snell, C. et al. Salivary Huntingtin protein is uniquely associated with clinical features of Huntington’s disease. Sci Rep 13, 1034 (2023). https://doi.org/10.1038/s41598-023-28019-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-28019-y
- Springer Nature Limited