
Abstract
Kawasaki disease (KD) is an acute systemic immune vasculitis caused by infection, and its etiology and underlying mechanisms are not completely clear. This study aimed to identify differentially expressed genes (DEGs) with diagnostic and treatment potential for KD using bioinformatics analysis. In this study, three KD datasets (GSE68004, GSE73461, GSE18606) were downloaded from the Gene Expression Omnibus (GEO) database. Identification of DEGs between normal and KD whole blood was performed using the GEO2R online tool. Gene ontology and Kyoto Encyclopedia of Genes and Genomes (KEGG) functional enrichment analysis of DEGs was undertaken with Metascape. Analysis and visualization of protein–protein interaction networks (PPI) were carried out with STRING and Cytoscape. Lastly, miRNA-genes regulatory networks were built by Cytoscape to predict the underlying microRNAs (miRNAs) associated with DEGs. Overall, 269 DEGs were identified, including 230 up-regulated and 39 down-regulated genes. The enrichment functions and pathways of DEGs involve regulation of defense response, inflammatory response, response to bacterium, and T cell differentiation. KEGG analysis indicates that the genes were significantly enriched in Neutrophil extracellular trap formation, TNF signaling pathway, Cytokine-cytokine receptor interaction, and Primary immunodeficiency. After combining the results of the protein–protein interaction (PPI) network and CytoHubba, 9 hub genes were selected, including TLR8, ITGAX, HCK, LILRB2, IL1B, FCGR2A, S100A12, SPI1, and CD8A. Based on the DEGs-miRNAs network construction, 3 miRNAs including mir-126-3p, mir-375 and mir-146a-5p were determined to be potential key miRNAs. To summarize, a total of 269 DEGs, 9 hub genes and 3 miRNAs were identified, which could be considered as KD biomarkers. However, further studies are needed to clarify the biological roles of these genes in KD.
Similar content being viewed by others

Introduction
Kawasaki disease (KD) is an acute pediatric self-limiting systemic inflammatory vasculitis that usually affects small and medium-sized blood vessels throughout the body and was first identified by Dr. Kawasaki of Japan in 19671,2. KD is diagnosed mainly by clinical criteria. The diagnosis of a typical KD is based on fever lasting ≥ 5 days with 4 of the 5 main clinical features satisfied (including erythema and dehiscence of the lips, strawberry tongue, erythema of the oral mucosa; bilateral bulbar conjunctival injection without exudation; rash: maculopapular or diffuse erythema; erythema and edema of the hands and feet in the acute phase; and usually unilateral enlarged cervical lymph nodes, > 1.5 cm in diameter). Patients lacking the full clinical features of a typical KD can be considered diagnosed in most cases if a coronary artery abnormality is detected1,3. The cause of KD is uncertain and there is still no specific diagnostic test. Combining the results of several studies, the consensus is that KD is an immune-related disease triggered by infection in genetically susceptible patients4,5,6. Approximately 25% of untreated KD patients will result in a coronary aneurysm or even a life-threatening condition. Although prompt treatment with intravenous immunoglobulin (IVIG) reduces this risk to 3% to 5%, the side effects associated with IVIG should not be underestimated1. However, biomarkers can assist clinicians in characterizing the severity and prognosis of the disease in early diagnosis and intervention. Therefore, studying and discovering the precise molecular mechanisms of KD is essential for developing therapeutic strategies.
Microarray technology and bioinformatics analysis have been broadly applied to screen for genetic alterations at the genomic level and to identify differentially expressed genes (DEGs) and functional pathways involved in the development and progression of KD7,8,9. Yet, it is difficult to obtain reliable results with a single microarray analysis due to its high rate of false positives. Therefore, in this study, to identify DEGs between normal and KD blood samples, 3 mRNA microarray datasets were downloaded from Gene Expression Omnibus (GEO). Subsequently, Gene ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) functional enrichment analysis of DEGs was undertaken with Metascape. Analysis and visualization of protein–protein interaction networks (PPI) were carried out with STRING and Cytoscape. Lastly, miRNA-genes regulatory networks were built by Cytoscape to predict the underlying microRNAs (miRNAs) associated with DEGs. To summarize, a total of 269 DEGs, 9 hub genes and 3 miRNAs were identified, which could be considered as KD biomarkers.
Materials and methods
Microarray data collection
GEO (http://www.ncbi.nlm.nih.gov/geo)10 is a public functional genomics data repository of high throughput gene expression data, chips and microarrays. The GSE6800411 and GSE7346112 datasets generated using the GPL10558 platform(Illumina HumanHT-12 V4.0 expression beadchip), and GSE1860613 generated on the GPL6480 platform (Agilent-014850 Whole Human Genome Microarray 4 × 44 K G4112F) were downloaded from GEO. According to the annotation information in the platform, the probes are transformed into the corresponding gene symbols. Samples in this study were selected untreated or without other control factors that might influence the variables. The GSE68004 dataset contained 89 complete/incomplete KD whole blood samples and 37 control samples; the GSE73461 dataset contained 77 whole blood samples from KD patients without definite bacterial or viral infections and 55 healthy controls; the GSE18606 dataset contained 8 whole blood samples from KD patients without IVIG treatment and 9 controls.
DEGs identification
Determining DEGs between KD and normal blood samples was performed using GEO2R (http://www.ncbi.nlm.nih.gov/geo/geo2r). GEO2R is an interactive web-based tool that allows users to compare two or more datasets in the GEO series to determine DEGs for various experimental situations. The adjusted P-values (adj. P) and Benjamini and Hochberg false discovery rate were used to strike a balance between finding statistically significant genes and limiting false positives. Genes with no corresponding gene symbols in the probe set or with more than one probe set were removed or averaged out separately. |log FC (fold change)|> 1 and adj. P-value < 0.01 were considered statistically significant.
Enrichment analysis of KEGG and GO for DEGs
Metascape (https://metascape.org/gp/index.html#/main/step1)14 is an analytical website which incorporates functional enrichment, interactome analysis, gene annotation and membership search in a comprehensive portal leveraging more than 40 independent knowledge bases. The KEGG is a resource of databases for the clarification of high-level features and effects of biological systems15,16. Gene Ontology (GO) is a premier bioinformatics program for high-quality functional gene annotation based on biological processes (BP), molecular functions (MF), and cellular components (CC)17. Metascape was used to determine the features of DEGs with the screening criteria set to minimum overlap = 3 and minimum richness = 1.5. P < 0.01 was considered statistically significant.
Construction of PPI network and analysis of module
The PPI network was constructed using the Search Tool for the Retrieval of Interacting Genes (STRING; http://string-db.org) (version 11.5)18 online database, and the parameters were set as follows: meaning of network edges: confidence level; minimum required interaction score: medium confidence (0.400). An open-source bioinformatics software platform, Cytoscape (version 3.9.1) is used to visualize molecular interaction networks19. Molecular Complex Detection (MCODE) (version 2.0) is a plug-in for Cytoscape to perform clustering of a given network according to the topology to identify densely connected regions20. Using Cytoscape to map the PPI network and using MCODE to identify the most important modules in the PPI network. The selection criteria were as follows: MCODE scores > 5, node score cut-off = 0.2, degree cut-off = 2, k-score = 2 and Max depth = 100.
Hub genes selection and analysis
The overlap of the top 20 genes based on the algorithms MCC, Maximum Neighborhood Component (MNC), DNMC, Closeness, Degree, Stress, Betweenness, Bottleneck, and Edge Penetration Component (EPC) were identified as hub genes using the cytoHubba plugin. Metascape was employed to forecast the function of hub genes and the screening conditions were set to Min Enrichment = 1.5 and Min overlap = 3. P < 0.01 was considered to be statistically significant.
Evaluation and validation of hub genes
ROC curves and box plots of gene expression were performed using Graphpad Prism software. When the area under the curve (AUC) exceeds 0.7, the gene will be regarded as highly diagnostic for KD. A two-sample t-test was used to compare the gene expression levels of KD and normal samples.
MiRNAs related to hub genes
Mapping of the top 10 hub genes to their corresponding miRNAs was performed using NetworkAnalyst 3.0 (https://www.networkanalyst.ca/)21, an online platform for visualization that facilitates the search for miRNA-gene interactions in gene regulatory networks. Each hub gene was identified as miRNAs with a degree cutoff value = 1.0. Finally, these hub genes and miRNAs were mapped by Cytoscape 3.9.1.
Results
Identification of DEGs in KD
We retrieved three datasets (GSE68004, GSE73461, and GSE18606) from the GEO database which contained the gene expression profiles of KD whole blood samples and healthy controls. See Table 1 for details of these three datasets. The DEGs (1103 in GSE68004, 684 in GSE73461 and 1602 in GSE18606) were identified after normalization of the microarray outcomes. The DEGs in the GSE68004, GSE73461 and GSE18606 datasets included 832 up-regulated and 271 down-regulated genes, 554 up-regulated and 130 down-regulated genes, and 821 up-regulated and 781 down-regulated genes, respectively. DEGs were all identified by comparison of the gene expression profiles of healthy controls and KD whole blood samples. Figure 1 showed the gene expression profiles of the DEGs in the three datasets containing data from the 2 sets of samples.

Volcano plots showing differentially expressed genes (DEGs) between the control and KD groups. (A–C) DEGs of the GSE68004, GSE73461 and GSE18606 datasets are shown, respectively. Red data points indicate up-regulated genes and blue ones indicate down-regulated genes. Genes without any significant differences are in black.
Further screening of these genes was performed and Venn diagrams were drawn representing these genes. As shown in Fig. 2, 269 DEGs were found to be significantly differentially expressed in the 3 groups, of which 230 genes were upregulated and 39 genes were downregulated (Table 2).

Venn diagram displaying the overlapping differentially expressed genes (DEGs) in three datasets searched from Gene Expression Omnibus (GEO). (A, B) illustrate the overlap of up-regulated and down-regulated genes in the GSE68004, GSE73461 and GSE18606 datasets, respectively.
Enrichment analysis of KEGG and GO for DEGs
We performed functional enrichment analysis of up-regulated and down-regulated genes in order to predict the biological functions of DEGs. GO analysis revealed that the upregulated genes were enriched mainly in tertiary granule, secretory granule lumen, regulation of defense response, and inflammatory response (Fig. 3A), while the down-regulated genes were enriched significantly in T cell differentiation, alpha–beta T cell activation, and positive T cell selection (Fig. 3B). KEGG pathway analysis revealed that the up-regulated genes were significantly enriched in Neutrophil extracellular trap formation, Osteoclast differentiation, and Cytokine-cytokine receptor interaction (Fig. 3C), while the down-regulated genes were mainly enriched in Th1 and Th2 cell differentiation and Primary immunodeficiency (Fig. 3D).

Functional enrichment of DEGs. Bar graphs display the results of the top 20 enrichment analyses for up-regulated genes (A, C) and down-regulated genes (B, D). P-value is shown in color.
Construction of PPI network, analysis of module, and identification of hub genes
The analysis of PPI for DEGs was based on the STRING database and the results were visualized with Cytoscape (Fig. 4A). With MCODE, a plug-in for Cytoscape, we determined the most densely connected regions (16 nodes, 64 edges) in the PPI network (Fig. 4B). The top 20 genes were calculated by 8 algorithms of the Cytoscape plugin cytoHubba (Table 3). Subsequently, the top 9 intersecting genes analyzed according to these 8 algorithms were selected as hub genes, which included CD8A, FCGR2A, HCK, IL1B, ITGAX, LILRB2, S100A12, SPI1, and TLR8 (Fig. 4C).

Network construction and module analysis. (A) Construction of a protein–protein interaction network using Cytoscape. The network includes 269 nodes and 869 edges. 2 edges between nodes indicate gene–gene interactions. The node corresponding to each gene is sized and colored according to the degree of interaction. The color scale indicates the change in the degree of each gene from high (blue) to low (white). Closer to the blue node, the higher the degree of connectivity between the 2 nodes. (B) The most densely connected region of the PPI network (16 nodes, 64 edges) was identified using MCODE. (C) 9 hub genes were determined in the densest connected region using the 8 algorithms in cytoHubba. The degree scores are represented in pink color. A darker color means a higher degree score.
Hub genes selection and analysis
The details of symbols, abbreviations, and functions about hub genes are shown in Table 4. Functional enrichment analysis showed that the 9 hub genes were mainly concentrated in biological processes (BP), namely positive regulation of defense response, immune response-regulating signaling pathway, positive regulation of interleukin-6 production and cell activation, as well as two KEGG that are Osteoclast differentiation and Yersinia infection (Fig. 5A–C, Table 5).

Functional enrichment of hub genes (A) Bar graph of GO analyses of hub genes. P-values were indicated by color. The network of enriched terms of hub genes; colors indicated the same cluster-ID (B) and P-value (C).
Evaluation and validation of hub genes
The diagnostic value in KD was determined by the area under the curve of ROC analysis based on the hub genes derived from the previous step. The results showed that the AUC of all hub genes in GSE73461 was greater than 0.8 (Fig. 6A). In the dataset GSE68004, the AUC values of all genes were higher than 0.7 (Fig. 7A). In the dataset GSE18606, all genes had AUC values higher than 0.8 (Fig. 8A). It can be observed that in these datasets, the expression of all hub genes was higher and statistically significant in KD (Figs. 6B, 7B and 8B). Therefore, combining the expression levels of hub genes and ROC results, we identified the above screened hub genes as candidate markers.

Validation of hub genes in the GSE73461 dataset. (A) ROC analysis of hub genes in KD. Different genes are indicated by different colors. (B) Box plot depicting the expression of hub genes in KD and normal samples.

Validation of hub genes in the GSE68004 dataset. (A) ROC analysis of hub genes in KD. Different genes are indicated by different colors. (B) Box plot depicting the expression of hub genes in KD and normal samples.

Validation of hub genes in the GSE18606 dataset. (A) ROC analysis of hub genes in KD. Different genes are indicated by different colors. (B) Box plot depicting the expression of hub genes in KD and normal samples.
Establishment of miRNAs-hub genes regulatory network
MiRNAs play multiple roles in the modulation of gene expression. The miRNAs and hub gene regulatory networks are built using Cytoscape to predict miRNAs targeting hub genes based on the NetworkAnalyst database. In Fig. 9, the 8 hub genes with their corresponding molecules of regulatory miRNAs are shown. One hub gene (IL1B) has 2 target miRNAs (mir-126-3p and miR-375). Among the 3 miRNAs, mir-126-3p was the common target of 3 hub genes (IL1B, LILRB2 and ITGAX), while mir-146a-5p was the common target of 3 hub genes (CD8A, HCK and S100A12).

Network of integrated miRNA-DEGs with 8 hub genes. Green diamonds indicate the 8 hub genes. Gray circles indicate miRNAs with low connection to the hub genes. Dark pink octagons indicate miRNAs with high connection to the hub genes.
Discussion
Whole-genome association studies have completely transformed the complex field of polygenic diseases and contributed to the achievement of several KD susceptibility genes, resulting in new insights into the pathogenesis of the disease. In the present study, we identified 269 DEGs, including 230 up-regulated genes and 39 down-regulated genes. The results of GO functional enrichment showed that these DEGs were enriched mainly in tertiary granule, secretory granule lumen, regulation of defense response and inflammatory response. In the PPI network of DEGs, 9 (TLR8, ITGAX, HCK, LILRB2, IL1B, FCGR2A, S100A12, SPI1 andCD8A) out of 269 genes had high degree of interaction. All the 9 hub genes were up-regulated in patients with KD except for CD8A. The results of GO functional enrichment indicated that these 9 genes were enriched mainly in positive regulation of defense response, immune response-regulating signaling pathway, positive regulation of interleukin-6 production and cell activation, as well as two KEGG that are Osteoclast differentiation and Yersinia infection. Earlier studies have shown that the infectious trigger of KD leads to a massive activation of the immune system, causing the coronary arteries to be in a prolonged self-immune response22. In addition, KD presents with a marked systemic inflammatory response23. It has been shown that IL-6 production is significantly elevated in KD patients, suggesting that there may be an underlying immune susceptibility in KD patients24. Jing et al. suggested that the formation of Neutrophil extracellular trap may alter the biological response of peripheral blood mononuclear cells (PBMC) and affect vascular injury in the KD25. These GO terms and the enrichment results of the KEGG pathway suggest that the DEGs or hub genes detected in the present study may be involvement in KD progression through the approaches described above.
TLR8, a member of the toll-like receptor family, is expressed mainly in myeloid dendritic cells, neutrophils, and monocytes26. It has been shown that the innate immune receptor TLR8 can be targeted by small molecule agents27. It has been shown that TLR8, a marker of macrophage M2, is significantly elevated in the acute phase of KD, suggesting that activated macrophages are a key driver of vasculitis in KD28. In our study, TLR8 acted as an up-regulated gene and therefore we speculated that it could serve as a potential innate immunotherapeutic target for KD. IL1B (Interleukin 1 Beta) is a crucial mediator in the inflammatory response and is important for both hosting responses and defending against pathogens29. It has been shown that IL-1β plays a key role in KD -associated abdominal aortic aneurysms, and the use of IL-1R blockers that inhibit this pathway may be a promising therapeutic target30. In addition, Porritt et al. demonstrated that IL-1β may play a core role in mediating gender-based differences in KD, with important implications for the use of anti-IL-1β therapies for the treatment of male and female KD patients31. S100A12, a granulocyte-derived receptor for advanced glycosylation end products (RAGE) and Toll-like receptor 4 (TLR-4) agonist, has been demonstrated to be upregulated in KD as well as involved in aseptic inflammatory activation of coronary endothelial cells in KD32,33.
ITGAX is a receptor for fibrinogen that mediates cellular interactions during inflammation34. To date, the role of ITGAX in KD is still unknown, and although one study has demonstrated that it is the key gene in KD35, further studies are needed to determine it. Hematopoietic cell kinase (HCK) is a member of the SRC family of cytoplasmic tyrosine kinases (SFKs) that are expressed in cells of the myeloid and B-lymphocyte lineages and may serve as therapeutic targets in immune cells and cancer cells36. Leukocyte immunoglobulin-like receptor subfamily B member 2 (LILRB2, also known as Ig-like transcript 4) is a receptor for class I MHC antigens that identify a broad range of HLAs and could participate in the immune response37. HLA class II has been shown to influence the genetic risk of KD through genetic polymorphisms38, suggesting that LILRB2 may be involved in the genetic susceptibility to KD. FCGR2A (Fc fragment of IgG receptor IIa, also known as CD32) encodes cell surface receptor protein discovered on phagocytes and participates in phagocytic clearance of antigen–antibody complexes39. Earlier studies have identified FCGR2A as a genetic locus associated with KD susceptibility40. Dysregulated B-cell signaling (such as FCGR2A) in genetic risk factors has been shown to increase susceptibility to KD41.
The T-cell surface glycoprotein CD8 alpha chain (CD8A), as an integral membrane glycoprotein, plays an important role in the immune response and has multiple functions in the response against external and internal attacks42. The role of CD8A in KD remains unreported, and interestingly, it was the only down-regulated hub gene in our study, suggesting a possible protective role in the progression of KD. Transcription factor PU.1 (SPI1), is a transcriptional activator that may be specifically involved in the differentiation or activation of macrophages or B cells43. Several bioinformatics studies have identified a correlation between SPI1 and KD35,44, but the exact mechanism remains to be explored.
In our study, the roles of TLR8, S100A12 and IL1B in KD have been validated through numerous previous studies, and they may serve as potential immune targets for the treatment of KD. The roles of ITGAX, HCK, LILRB2 and FCGR2A in KD have not been widely studied, but based on our findings, except for CD8A, they were all hub genes that significantly upregulated in KD and might be used as diagnostic markers to predict disease progression.
MiRNAs are a type of small non-coding RNA that modulates mRNA expression, and they are becoming key genes in a range of cellular processes, including apoptosis, inflammation, and innate immune responses45. Moreover, several studies have shown that miRNAs can be involved in the disease progression of KD46,47,48,49. Ning et al.50 suggested that miR-126-3p might be a good reference miRNA gene in platelets of KD patients. It has been demonstrated that IL-10 reduces cardiovascular inflammation by interacting with pathways such as miR-37551, therefore it is speculated that mir-375 may be involved in KD by protecting against cardiovascular inflammation. A study showed that the genetic polymorphic locus of mir-146a was associated with susceptibility to KD in Chinese children52. Nevertheless, the role of these miRNAs in KD that we have identified still needs to be further explored. In addition, there are still limited studies related to genes and miRNAs in the KD.
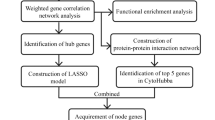
It is evident that gene-miRNA regulatory networks play a key part in the development of KD. In this way, it increases the knowledge of KD identification and contributes to targeted therapeutic management strategies and KD prediction. This study has several limitations. For one, the results of microarray expression profiling were performed with bioinformatics analysis and were not confirmed with basic experiments. Furthermore, the detailed mechanisms of how hub genes and miRNAs regulate KD deficiency were not explored. We have mapped a proposed mechanism for the main results of this study (Fig. 10). Unfortunately, there are currently very few experimental studies and related drug development for these potential biomarkers, making it difficult to explore them in more depth in conjunction with clinical data and experiments, which leaves our hypotheses without strong support. For future work, experimental validation of these findings will be performed in vitro and in vivo. There is also a need to propose effective strategies for in-depth clinical validation, e.g., increasing follow-up time to validate results, using methods including multiple regression models to confirm and increase the specificity and sensitivity of biomarkers, etc.

Hub genes and miRNAs in KD.
Conclusion
To summarize, a total of 269 DEGs, 9 hub genes (TLR8, ITGAX, HCK, LILRB2, IL1B, FCGR2A, CD8A, SPI1 and S100A12) and 3 miRNAs (mir-126-3p, mir-375 and mir-146a-5p) were identified, which could be considered as KD biomarkers. However, further studies are needed to clarify the biological roles of these genes in KD.
Data availability
The datasets generated and/or analyzed during the current study are available in the [GEO] repository, [https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE68004/GSE73461/GSE18606].
References
Sosa, T., Brower, L. & Divanovic, A. Diagnosis and management of Kawasaki disease. JAMA Pediatr. 173(3), 278–279 (2019).
Kawasaki, T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi 16(3), 178–222 (1967).
McCrindle, B. W. et al. Diagnosis, treatment, and long-term management of Kawasaki Disease: A scientific statement for health professionals from the American Heart Association. Circulation 135(17), e927–e999 (2017).
Son, M. B. F. & Newburger, J. W. Kawasaki disease. Pediatr. Rev. 39(2), 78–90 (2018).
Burgner, D. & Harnden, A. Kawasaki disease: What is the epidemiology telling us about the etiology?. Int. J. Infect. Dis. 9(4), 185–194 (2005).
Burns, J. C. The riddle of Kawasaki disease. N. Engl. J. Med. 356(7), 659–661 (2007).
He, L. et al. Identification of differentially expressed genes in Kawasaki disease patients as potential biomarkers for IVIG sensitivity by bioinformatics analysis. Pediatr. Cardiol. 37(6), 1003–1012 (2016).
Rahmati, Y. et al. CASP5 and CR1 as potential biomarkers for Kawasaki disease: An integrated bioinformatics-experimental study. BMC Pediatr. 21(1), 566 (2021).
Rowley, A. H. et al. The transcriptional profile of coronary arteritis in Kawasaki disease. BMC Genom. 16, 1076 (2015).
Edgar, R., Domrachev, M. & Lash, A. E. Gene Expression Omnibus: NCBI gene expression and hybridization array data repository. Nucleic Acids Res. 30(1), 207–210 (2002).
Jaggi, P. et al. Whole blood transcriptional profiles as a prognostic tool in complete and incomplete Kawasaki disease. PLoS ONE 13(5), e0197858 (2018).
Wright, V. J. et al. Diagnosis of Kawasaki disease using a minimal whole-blood gene expression signature. JAMA Pediatr. 172(10), e182293 (2018).
Fury, W. et al. Transcript abundance patterns in Kawasaki disease patients with intravenous immunoglobulin resistance. Hum. Immunol. 71(9), 865–873 (2010).
Zhou, Y. et al. Metascape provides a biologist-oriented resource for the analysis of systems-level datasets. Nat. Commun. 10(1), 1523 (2019).
Kanehisa, M. The KEGG database. Novartis Found Symp, Vol. 247 91–101 (2002) discussion 101–3, 119–28, 244–52.
Kanehisa, M. et al. KEGG: New perspectives on genomes, pathways, diseases and drugs. Nucleic Acids Res. 45(D1), D353–D361 (2017).
Pomaznoy, M., Ha, B. & Peters, B. GOnet: A tool for interactive gene ontology analysis. BMC Bioinform. 19(1), 470 (2018).
Franceschini, A. et al. STRING v9.1: Protein-protein interaction networks, with increased coverage and integration. Nucleic Acids Res. 41(Database issue), D808–D815 (2013).
Smoot, M. E. et al. Cytoscape 2.8: New features for data integration and network visualization. Bioinformatics 27(3), 431–2 (2011).
Bandettini, W. P. et al. MultiContrast Delayed Enhancement (MCODE) improves detection of subendocardial myocardial infarction by late gadolinium enhancement cardiovascular magnetic resonance: A clinical validation study. J. Cardiovasc. Magn. Reson. 14, 83 (2012).
Zhou, G. et al. NetworkAnalyst 3.0: A visual analytics platform for comprehensive gene expression profiling and meta-analysis. Nucleic Acids Res. 47(W1), W234–W241 (2019).
Yeung, R. S. Pathogenesis and treatment of Kawasaki’s disease. Curr. Opin. Rheumatol. 17(5), 617–623 (2005).
Burns, J. C. Kawasaki disease. Adv. Pediatr. 48, 157–177 (2001).
Chen, K. Y. H. et al. Innate immune responses following Kawasaki disease and toxic shock syndrome. PLoS ONE 13(2), e0191830 (2018).
Jing, Y. et al. Neutrophil extracellular trap from Kawasaki disease alter the biologic responses of PBMC. Biosci. Rep. https://doi.org/10.1042/BSR20200928 (2020).
Marques, J. T. & Williams, B. R. Activation of the mammalian immune system by siRNAs. Nat. Biotechnol. 23(11), 1399–1405 (2005).
Sakaniwa, K. & Shimizu, T. Targeting the innate immune receptor TLR8 using small-molecule agents. Acta Crystallogr. D Struct. Biol. 76(Pt 7), 621–629 (2020).
Guo, M. M. et al. Epigenetic regulation of macrophage marker expression profiles in Kawasaki disease. Front. Pediatr. 8, 129 (2020).
Lopez-Castejon, G. & Brough, D. Understanding the mechanism of IL-1beta secretion. Cytokine Growth Factor Rev. 22(4), 189–195 (2011).
Wakita, D. et al. Role of interleukin-1 signaling in a mouse model of Kawasaki disease-associated abdominal aortic aneurysm. Arterioscler. Thromb. Vasc. Biol. 36(5), 886–897 (2016).
Porritt, R. A. et al. Interleukin-1 beta-mediated sex differences in Kawasaki disease vasculitis development and response to treatment. Arterioscler. Thromb. Vasc. Biol. 40(3), 802–818 (2020).
Li, S. C. et al. Serum proteins may facilitate the identification of Kawasaki disease and promote in vitro neutrophil infiltration. Sci. Rep. 10(1), 15645 (2020).
Armaroli, G. et al. Monocyte-derived interleukin-1beta as the driver of S100A12-induced sterile inflammatory activation of human coronary artery endothelial cells: Implications for the pathogenesis of Kawasaki disease. Arthritis Rheumatol. 71(5), 792–804 (2019).
Shelley, C. S. et al. Mapping of the human CD11c (ITGAX) and CD11d (ITGAD) genes demonstrates that they are arranged in tandem separated by no more than 11.5 kb. Genomics 49(2), 334–6 (1998).
Gao, S. et al. Identification of key genes and underlying mechanisms in acute Kawasaki disease based on bioinformatics analysis. Med. Sci. Monit. 27, e930547 (2021).
Poh, A. R., O’Donoghue, R. J. & Ernst, M. Hematopoietic cell kinase (HCK) as a therapeutic target in immune and cancer cells. Oncotarget 6(18), 15752–15771 (2015).
Shiroishi, M. et al. Human inhibitory receptors Ig-like transcript 2 (ILT2) and ILT4 compete with CD8 for MHC class I binding and bind preferentially to HLA-G. Proc. Natl. Acad. Sci. U. S. A. 100(15), 8856–8861 (2003).
Onouchi, Y. et al. A genome-wide association study identifies three new risk loci for Kawasaki disease. Nat. Genet. 44(5), 517–521 (2012).
Gerber, J. S. & Mosser, D. M. Stimulatory and inhibitory signals originating from the macrophage Fcγ receptors. Microbes Infect. 3(2), 131–139 (2001).
Khor, C. C. et al. Genome-wide association study identifies FCGR2A as a susceptibility locus for Kawasaki disease. Nat. Genet. 43(12), 1241–1246 (2011).
Kumrah, R. et al. Immunogenetics of Kawasaki disease. Clin. Rev. Allergy Immunol. 59(1), 122–139 (2020).
Ellmeier, W., Haust, L. & Tschismarov, R. Transcriptional control of CD4 and CD8 coreceptor expression during T cell development. Cell. Mol. Life Sci. 70(23), 4537–4553 (2013).
Verbiest, T. et al. PU.1 downregulation in murine radiation-induced acute myeloid leukaemia (AML): From molecular mechanism to human AML. Carcinogenesis 36(4), 413–9 (2015).
Srivastava, P. et al. Exploration of potential biomarker genes and pathways in Kawasaki disease: An integrated in-silico approach. Front. Genet. 13, 849834 (2022).
Tahamtan, A. et al. Anti-inflammatory MicroRNAs and their potential for inflammatory diseases treatment. Front. Immunol. 9, 1377 (2018).
Chu, M. et al. Bone marrow-derived microRNA-223 works as an endocrine genetic signal in vascular endothelial cells and participates in vascular injury from Kawasaki disease. J. Am. Heart Assoc. https://doi.org/10.1161/JAHA.116.004878 (2017).
Nakaoka, H. et al. MicroRNA-145-5p and microRNA-320a encapsulated in endothelial microparticles contribute to the progression of vasculitis in acute Kawasaki disease. Sci. Rep. 8(1), 1016 (2018).
Liu, C. et al. MicroRNA-197-3p mediates damage to human coronary artery endothelial cells via targeting TIMP3 in Kawasaki disease. Mol. Cell. Biochem. 476(12), 4245–4263 (2021).
Maruyama, D. et al. MicroRNA-223 regulates the development of cardiovascular lesions in LCWE-induced murine Kawasaki disease vasculitis by repressing the NLRP3 inflammasome. Front. Pediatr. 9, 662953 (2021).
Ning, Q. et al. The platelet microRNA profile of Kawasaki disease: identification of novel diagnostic biomarkers. Biomed. Res. Int. 2020, 9061568 (2020).
Goswami, S. K. et al. Management of inflammation in cardiovascular diseases. Pharmacol. Res. 173, 105912 (2021).
Zha, L. et al. Association of miR-146a gene polymorphism at loci rs2910164 G/C, rs57095329 A/G, and rs6864584 T/C with susceptibility to Kawasaki disease in Chinese children. Pediatr. Cardiol. 40(3), 504–512 (2019).
Acknowledgements
We would like to thank Editage (www.editage.cn) for English language editing.
Funding
No funding was available for this work.
Author information
Authors and Affiliations
Contributions
W.H. participated in the design of the study, carried out the study, performed the statistical analysis, and drafted the manuscript. Y.C. reviewed and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cai, Y., Hu, W. Identifying differentially expressed genes and miRNAs in Kawasaki disease by bioinformatics analysis. Sci Rep 12, 21879 (2022). https://doi.org/10.1038/s41598-022-26608-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-26608-x
- Springer Nature Limited