
Abstract
We aim to estimate the prevalence of prediabetes, and diabetes mellitus (DM). We estimated awareness, treatment, plasma glucose control, and associated factors in diabetes, as well as, socioeconomic-related inequality in the prevalence of diabetes and prediabetes. Data for adults aged 35–70 years were obtained from the baseline phase of the Dehgolan prospective cohort study (DehPCS). Diabetes status was determined as fasting plasma glucose (FPG) of ≥ 126 mg/dl and/or taking glucose lowering medication confirmed by a medical practitioner. Prediabetes was considered as 100 ≤ FPG ≤ 125 mg/dl. The relative concentration index (RCI) was used to exhibit socioeconomic inequality in the prevalence of prediabetes and DM. Prevalence of prediabetes and DM, diabetes awareness and treatment, and glycemic control of DM 18.22%, 10.00%, 78.50%, 68.91% and, 28.50%, respectively. Increasing age (p < 0.001), Increasing body mass index (BMI) (p < 0.05), ex-smoker (p < 0.01), family history of diabetes (FHD) (p < 0.001), and comorbidity (p < 0.001) were independent risk factors for DM. Age group of 46–60 (p < 0.05), ex-smoker (p < 0.05), FHD (p < 0.05) were increased chance of awareness. Current smokers (p < 0.05), and higher education increase the chance of glycemic control in DM. Both DM (RCI = − 0.234) and prediabetes (RCI = − 0.122) were concentrated significantly among less-educated participants. DM was concentrated significantly among poor (RCI = − 0.094) people. A significant proportion of DM awareness and treatment can be due to the integration of diabetes into the primary health care system. The high prevalence of prediabetes and diabetes, which is affected by socioeconomic inequality and combined with low levels of glycemic control may place a greater burden on the health system. Therefore, awareness, receiving treatment, and glycemic control in people with diabetes, and the socioeconomic status of people have become increasingly important in the near future.
Similar content being viewed by others

Introduction
Today, diabetes mellitus (DM) is a worldwide public health challenge, imposing a significant burden on socioeconomic development and global public health1,2. International Diabetes Federation (IDF) has estimated that 537 million adults aged 20–79 are living with DM in 2021, and it is expected to rise to 783 million by 2045. In addition, 541 million adults with impaired glucose tolerance (IGT), are at higher risk for DM3.
The Prevalence of diabetes and prediabetes in people over 18 years was estimated at 14.15% and 24.79% respectively in 2021 in Iran. It represents a 45.5% increase in diabetes prevalence compared to 20164. According to the last national survey of risk factors of non-communicable diseases (NCDs), 15.14% of the Iranian population over 25 years old had diabetes in 20214. The number of people with diabetes in Iran is projected to increase to 9.2 million by 2030 if no effective prevention is incorporated5.
Due to the silent nature of diabetes, a significant portion of the affected population is unaware of their DM status6, and many people with diabetes are unaware of their complications due to uncontrolled blood glucose levels7. For example, according to national reports in 2021, the proportion of DM awareness in Iran was 73% and only 31% of people with diabetes in Iran have controlled hyperglycemia4.
Along with economic transition, urbanization, industrialization, and globalization, the rapid increase in diabetes prevalence have been occurred due to changes in socioeconomic status (SES), environmental, and lifestyle factors8. Environmental risk factors for DM are reasonably well established but the impact of SES in relation to DM is not well understood9.
Differences in health between socioeconomic groups are one of the major public health challenges worldwide10. Several literatures provide irrefutable evidence of SES as a determinant in prevalence and control of DM8,10. SES affects individual health behaviors through many aspects, including patient abilities, community or neighborhood support, health-related behaviors, access to care, and the care process11. This can lead to a lack of diabetes-related awareness and willingness to diagnose diabetes, which is important in glucose control in DM12. Undiagnosed diabetes can lead to a sudden adverse outcome, and if not diagnosed for a long time, it can progress into a serious problem in the patient's later life12.
Updating information on the prevalence, control, treatment, and awareness of diabetes and prediabetes is essential for prioritizing and planning health care services and achieving the goals of the World Health Organization (WHO) Action Plan for the Prevention and Control of NCDs in 202513. In addition, measuring health inequalities is helpful in promoting equality and achieving Sustainable Development Goals (SDGs).
To our knowledge, previous studies have estimated the prevalence of diabetes in Iran, but limited studies have reported awareness, treatment, control of diabetes, and SES inequalities using clinical outcomes in addition to the self-reporting data. Therefore, this study aims to (1) describe the prevalence, control, treatment, and awareness of diabetes and prediabetes, (2) determine socioeconomic inequalities in the prevalence of diabetes and prediabetes using the Relative concentration index (RCI) among adults aged 35–70 years participating in the Dehgolan prospective cohort study (DehPCS).
Methods
Study population
The present study utilized enrollment phase data of the DehPCS. As a part of the prospective epidemiological research study in Iran (PERSIAN), DehPCS was conducted to investigate 35–70 years old permanent residents of Dehgolan. PERSIAN covers 18 cohort sits, including a representative sample of the major ethnicity all over Iran. Uniform questionnaires and data collection methods were used at all sites. PERSIAN aimed to follow up participants for the 15-year time period14.
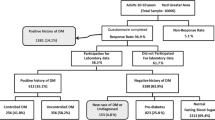
Dehgolan County is a district of Kurdistan province, which is located in the west of Iran. Almost all 9000 residents 35–70 years old have a Kurdish ethnicity. By incorporating simple cluster sampling with a total number of 3996 participants who were enrolled in the study. The response rate of eligible people was 91%. The rationale and detail of the study have previously been published elsewhere15 (Fig. 1).

Flow diagram of participants in Dehgolan Prospective Cohort Study (DehPCS), 2018–2019, who respond to questionnaires and agreed for fasting blood glucose sampling.
Data collection and measurements
A local, trained personnel who spoke native Kurdish collected data in three dimensions including general, medical, and, nutritional information. Questionnaires consisted of demographic, socio-economic, medical/clinical/biological information, lifestyle, personal habit, anthropometry, medication use, and, nutritional status. All eligible participants are invited 1 week earlier to participate in the study. All participants were contacted by call reminder a day before the appointment schedule. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional level and/or national level Medical Research Ethics Committee (MREC) and in line with the 1964 Helsinki declaration and its later amendments.
Upon arrival, the participants are been registered in the online software and received a unique code. In the first step, blood and urine samples were been taken from fasting participants. Height is been also measured at 0.1 cm accuracy with Seca stadiometer. To measure weight, we used Seca scale. Body mass index (BMI) was calculated by dividing weight (kg) by height (cm). Subsequently, based on world health organization guidelines16 BMI was categorized into three groups, normal (≤ 24.9), overweight (≤ 29.9) and, obese (≥ 30.0). Education was categorized as follows: illiterate (zero years of education), 1–6 years of education, 7–12 years of education, and university (more than 12 years of education).
Economic status was defined based on the Wealth index. Wealth index was calculated according to the selected living assets, including having a freezer, washing machine, dishwasher, vacuum cleaner, color TV (no color TV or regular color TV vs. Plasma color Tv), access to internet, motorcycle, car (no access, access to a car with price of < 50 million Tomans, and access to a car with price of > 50 million Tomans), owning a mobile, owning a PC or laptop, international trips in their lifetime. The total wealth score was calculated based on the multiple correspondence analysis (MCA) of assets data17. Then, participants were ranked and divided into three categories of wealth index based on 2 quantiles (cut point), by dividing the range of probability distribution into intervals with an equal probability. The groups were named poor, middle, and rich respectively.
Individuals who smoked more than 100 cigarettes during their lifetime are considered as smokers. However, if someone had smoked during the last month was grouped as current, and if they had not smoked as an ex-smoker. Illicit drug use was defined as using illicit drugs once per week for at least 6 months. Alcohol consumption was defined as drinking approximately 200 ml of beer or 45 ml of liquor, once per week for at least six months. Participants physical activity was measured by self-report of time spent on recreation, work, sport, and other activity during 1 week. The mean 24-h metabolic equivalent task (MET) score was calculated based on the weight, activity type, and time spent on activities. Then, METs were divided into following categories: 24–36.5 (low), 36.6–44.9 (moderate), and ≥ 45 (vigorous)18. Lipid profile was examined after 9–12 h of fasting. Triglyceride (TG), HDL, and LDL-cholesterol were measured through colorimetric and total cholesterol by enzymatic method. Dyslipidemia was determined based on the total cholesterol ≥ 240 (mg/dl), and/ or TG ≥ 200 (mg/dl) and/or LDL ≥ 160 (mg/dl), and/or HDL < 40 (mg/dl), and/or use of medication to treat these conditions19.
Hypertension was measured by a hand-held aneroid sphygmomanometer. After 15 min of rest in a sitting position, blood pressure (BP) was measured twice in each arm with 30 min of time intervals. The average of four systolic and diastolic (SBP & DBP) values were used to determine BP. Those who had SBP ≥ 140 and/or DBP ≥ 90 and/ or use anti-hypertensive medication were considered as hypertensive individuals20.
Diabetes status was determined as abnormal fasting plasma glucose (FPG) and/or current history of taking glucose lowering medication, and/or if was confirmed by a medical practitioner. Prediabetes and diabetes were considered as 100 ≤ FPG ≤ 125 mg/dl and FPG ≥ 126 mg/dl respectively21. Awareness is determined by individual self-reported diabetes among people with diabetes. Patients who received medication and his/her FPG less than 126 mg/dl were considered as controlled FPG.
Statistical analysis
Prevalence of prediabetes, and DM were defined as the number of affected participants divided by the number of all participants. The proportion of the awareness, treatment, and FPG control were also estimated by the available standard method. A 95% confidence interval (CI) were calculated for all estimation. The adjusted logistic regression method was used to investigate the independent relationship of all variables with a p-value less than 0.3 in the univariable analysis. Crude and adjusted odds ratio (OR) with their CI were provided with a significant level of 0.05. RCI and concentration curve (CC) was used to examine the SES-related inequality by years of education and wealth index in the prevalence of prediabetes and diabetes in the study population22. Data were analyzed using STATA software version 16.0 (Stata Corp, College Station, TX, USA).
Ethics approval and consent to participate
The ethical review board at Kurdistan University of Medical Sciences has approved study design and protocol of this study under the code of IR.MUK.REC.1400.149. For experiments involving human participants, informed consent have been obtained.
Results
In total 3996 participants enrolled in the study. 43.74% of participants were male, with a mean age of 48.72 ± 8.91 years. generally, 91.87% of participants were married and, 31.21% were illiterate. 32.3% of participants had BMI ≥ 30 and may have obesity complications. 15.19% were current smokers, 11.34% used illicit drugs, and more than 12% of them were alcohol users. In total, 31.55% of participants reported a family history of diabetes, and 60.11% of them suffered from at least one comorbidity including dyslipidemia (38.61%), hypertension (8.01%), or both (13.49%). The prevalence of dyslipidemia and hypertension among participants were 52.10% and 21.5% respectively (Table 1).
Prevalence, awareness, treatment, FPG control
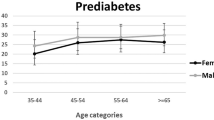
Of all 3996 participants 18.22 (CI 16.99–19.52), and 10.00 (CI 9.09–10.97) were pre diabetic and people with diabetes respectively. The mean and standard deviation of FPG for all samples, females, and males, were 98.31 ± 32.53, 99.26 ± 34.02, and 97.09 ± 30.48 respectively. The proportion of diabetes significantly increased with age in both males and females (p-value for trend < 0.001). The proportion of prediabetes, diabetes, awareness, and FPG control were higher in females than males but, the probability of receiving treatment was lower for females. Diabetes decreased with education years for both males and females (p-value for trend 0.01 and < 0.001 respectively). Women in higher economic classes experienced a lower prevalence of diabetes (p-value for trend = 0.011).
Both diabetes and prediabetes prevalence increased linearly based on the groups formed by the closeness of family relationship (p-value for trend < 0.001). However, the proportion of patients with controlled glycemic level was lower in participants whose familial relationships with people with diabetes were stronger.
Decreasing trend (p-value = 0.009) for diabetes prevalence was seen across the intensity of physical activity but, a sharp increasing trend was seen based on groups formed by comorbidity (p-value for trend < 0.001).
Among all 387 people with diabetes, 303 (78.50%) aware of their condition, 266 (68.73%) take glycemic lowering medication, and 110 (28.72%) were controlled their FPG level (Table 1).
Prediabetes and diabetes associated factors
Although, the crude odds of prediabetes and diabetes were greater in females (OR 1.35, p < 0.001 and OR 1.30, p = 0.016 respectively), adjusted odds were equally distributed among both males and females (Table 2). Age was directly associated with both prediabetes and diabetes (p < 0.001) and education was reversely related to the diabetic and prediabetic patients. Divorced/widowed/single patients were more likely to get diabetes in the crude model.
Results of the adjusted model showed BMI increased odds of diabetes and prediabetes independently of other variables (p < 0.001). Current smoking was reversely associated with prediabetes (p < 0.05), and ex-smoking directly increases the risk of diabetes (p < 0.01) independently of other variables. History of alcohol use had moderately decreased odds of diabetes (p < 0.05). Both pre-diabetes and diabetes independently had a significant dose–response relationship with those who have reported positive family history of diabetes (Table 2). Comorbidity with hypertension and dyslipidemia were increased risk of diabetes (p < 0.001) and pre-diabetes (p < 0.01) in both univariable and multivariable analysis (Table 2).
DM awareness associated factors
Females have more chance to become aware of their diabetes condition (crude OR 1.82, p < 0.001). Age was directly associated with awareness (crude OR 1.03, p = 0.023). A lower chance of awareness was observed in participants with higher education years (crude OR 0.94, p = 0.011). Positive history of diabetes in the family especially in their second-degree family members increased awareness of diabetes condition (p < 0.001).
Multivariable regression results showed that the awareness was higher in the older ages independently of other variables, as the age group of 46–60 showed the strongest relationship with awareness (Adjusted OR 2.55, 95% CI 1.19–5.48). Previously smokers were more likely to be aware of their DM condition than non-smokers were (Adjusted OR 2.91, 95% CI 1.08–7.86). Participants with a positive history of diabetes in their families were more probable to be aware of their DM situation. Participant’s comorbid with hypertension and dyslipidemia were more aware of their diabetes condition, but it was not statistically significant (Table 2).
DM treatment associated factors
Males and females have an equal chance to get DM treatment (p = 0.301). In addition, more older participants have a higher probability of receiving treatment (p = 0.026), and participants with a higher level of physical activity were more likely to get treatment. (p = 0.043).
After adjusting for the effect of covariates in the multivariable regression model, participants more than 60-years-old were about 6 times more likely to receive treatment than those in 35–45 (Adjusted OR 6.08, 95% CI 1.52–24.32). Also, physical activity MET score ≥ 45 (vigorous) significantly decreased the 76% probability of getting DM treatment independently of other variables (Adjusted OR 0.24, 95% CI 0.07–0.82). Being male and of a higher education level increased the chance of receiving treatment, while smoking reduced the likelihood of receiving treatment. However, these relationships were not statistically significant (p > 0.05) (Table 2).
DM control associated factors
In the univariate analysis, the control of glycemic level was equally distributed among different levels of independent variables. However, in the multivariable logistic regression, after adjusting for different covariates, glycemic control was significantly different for gender, education, and smoking status. The odd of diabetes control was 68% lower in male than female participants (OR 0.32, 95% CI 0.14–0.75). There was a significant dose–response relationship between education levels and glycemic control in diabetes patients. It was about 2.4, 4.0, and 4.8 times more than illiterate for primary, high school, and university degrees respectively (OR 2.44, 4.02 and, 4.78 respectively). Ex-smokers and current smokers were more probable to control their glycemic index than non-smokers. It was only statistically significant in current smokers with odds of about 2.5 times higher than non-smokers (OR 2.63, 95 CI 1.06–6.52) (Table 2).
SES-related inequality
The results of socioeconomic-related inequality for the prevalence of prediabetes and diabetes are reported in Table 3. As indicated, diabetes was concentrated among the poorer people (RCI = − 0.094, 95% CI − 0.155 to − 0.033) and people with lower education levels (RCI = − 0.234, 95% CI − 0.293 to − 0.175). We also observed predicates are more prevalent among the poor and among the less-educated individuals (RCI = − 0.122, 95% CI = − 0.170 to − 0.070). However, the results for the prevalence of prediabetes by wealth index are not significant (p-value = 0.509). For prediabetes and diabetes prevalence, education-related inequality was higher than wealth-related inequality (Fig. 2). As indicated in Fig. 2, the CC for the prevalence of diabetes and prediabetes lies on the perfect line; meaning that the higher prevalence of diabetes and prediabetes are more concentrated among the socioeconomically disadvantaged population (less educated and lower income).

Concentration index for prediabetes and diabetes according to the education years (A) and wealth index (B).
Discussion
The prevalence of DM and prediabetes among 3996 participants was 10% and 18%, respectively. About 78% of patients were aware of their disease status and 84.82% were under treatment. However, glycemic control was observed in only 40% of the treatment on people with diabetes. According to the results, the DM prevalence in this study was less than the national estimate of 15.0% in Iran in 202113. Similar studies with the same age groups, in Shahroud (12%)23, Ahvaz (15%)24, and Yazd (24%)25 reported a higher proportion, and Ravansar in Kermanshah (8.19%)6 and Valashahr in Fars (9.19%)26 reported less prevalence of diabetes. Also, this prevalence was still fewer than that of Afghanistan27, and Pakistan28 and higher than that of Bangladesh29 and Nepal30. This may be due to differences in people's age distribution, demographic characteristics, and lifestyles.
The association between smoking and DM or prediabetes was challenging in the current study. Although much evidence has shown an association between smoking, DM, and prediabetes31,32,33, in the present study, after eliminating confounding factors, smoking had only an effect on prediabetes and no significant effect on DM. In the present study, ex-smokers had a higher risk of developing DM compared to non-smokers. In a meta-analysis of prospective studies, the risk of DM after quitting smoking was also observed to steadily decrease and achieve a level of risk compared to those who never smoked33. Conversely, some studies similar to the current study showed quitting smoking might increase the risk of DM33,34. Probably due to weight gain and increased waist circumference after smoking cessation, the risk of DM increased33. There was a protective association between alcohol consumption and a chance of developing DM in this study. Other studies showed some inconsistencies in alcohol consumption and its effect on DM. In the meta-analysis study, low and moderate consumption reduced DM by 28%. In addition, excessive alcohol consumption had no effect on DM incidence. Low and moderate alcohol consumption could improve insulin sensitivity and reduce fasting insulin concentrations and glycosylated hemoglobin35. In contrast, in a cohort study on Korean adults, alcohol consumption ≥ 2 units per day (≥ 16 g/day) significantly increased the risk of DM36, so high alcohol consumption may be considered a risk factor for DM. In this regard, probably due to legal and religious restrictions on alcohol consumption in Iran, consumers are likely to be of low or moderate types. According to the results of previous studies, the diabetes family history is considered as an independent factor of DM and prediabetes. Also, the risk of DM was much higher in people who suffered from hypertension or dyslipidemia37,38. This has also been seen in previous studies.
DM awareness in the present study was 78%, which was almost the same as the national estimate (awareness of 79.6%). It is different in other parts of Iran. For example, DM awareness in Yazd and Kerman was about 97–95%25 while in Ahvaz, it was 40%24 and in the neighboring province (Kermanshah), it was similarly 75%6. In other countries such as China39, the US40, and Malaysia41, it was reported 52.5%, 71.5%, and 65.2%, respectively. Over the past years in Iran, the prevalence of undiagnosed diabetes has decreased from 45.7 to 24.7%42. The results of the present study paradoxically showed DM awareness had an inverse association with higher income levels while in some studies; individuals in higher income families had more awareness of diabetes43,44,45. Other studies in Iran and other countries did not report a significant association between diabetes and awareness44,45,46. Higher-income people may be able to receive health education and services more easily, but in recent years, with the expansion of screening programs of the health system to identify people with diabetes at the primary levels, and by reducing financial barriers, income does not have such an impact on access to primary health services. Similarly, in the present study, the diabetes family history6,47, age6,48 and smoking cessation6 had a direct association with DM awareness. In fact, people with a family history of diabetes show more health protective behaviors, especially weight control behaviors, than those without a family history of diabetes. In addition, with aging due to increased experiences and risk of diabetes, it seems that increasing awareness is logical. Ex-smokers are also more likely to develop DM than non-smokers39, so people may also develop other positive health-related behaviors at the same time as quitting smoking.
In this study, approximately 85% of people with diabetes were under treatment, which was higher than the statistic of 33% in Iran49 in previous years and the rate reported in neighboring provinces (75%)6. Treatment was reported in Malaysia 87%41, in Portugal 80%50, in the UA 71%40 and in villages of China 62%51. Therefore, receiving treatment among people with diabetes seems desirable compared to other studies. Also, based on the results of this research and other studies, treatment increases among age groups of 60 years and older51.
Despite the fact that a significant proportion of patients were treated in this study, only 40% of them controlled their blood sugar, which was almost similar to the national estimate (41.2%)13, and was lower than the rates reported for Portugal (63%)50, and the United States (50%)40 while it was higher than those for Kermanshah (33%)52, the national study in Iran (33%)52, Malaysia (22%)41, and villages of China (22%). In the results of previous studies, the low the proportion of glucose control has been stated as an indicator of inappropriate quality of services provided to people with diabetes52. Women also controlled at diabetes relatively higher rates than men. Studies also showed women were more adherent than men53. In the present study, the chance of diabetes control among ex-smoker was higher than among smokers and non-smokers. However, in other studies, smoking cessation has been associated with significant weight gain and body weight gain after quitting smoking may worsen glycemic control54,55,56. The results of our study are inconsistent with this finding perhaps because people who wish to quit smoking at the same time follow other health-related recommendations and people with diabetes who quit smoking also pay more attention to their blood sugar control and adherence to treatment33.
Finally, inequality analysis showed the prevalence of pre-diabetes and diabetes was significantly more concentrated among people with lower education, and financial levels. Other studies also showed the effect of educational inequality on diabetes1 and in a study, the likelihood of developing diabetes and pre-diabetes among people with low education was twice as high as those with moderate and high education levels whereas it clearly decreased in the higher education group57. Higher education generally seems to lead to better working conditions, higher incomes and better housing, and thus affects a person’s ability to take a more favorable social position. In other words, people with lower education may be exposed to risk factors and susceptible to T2 diabetes compared to their counterparts due to more unfavorable living conditions1,58. Similarly, in other studies, a positive association was observed between diabetes, pre-diabetes, and wealth status59,60,61. Even in a study, it has been noted that undesirable SES early in life are associated with an increased risk of developing pre-diabetes and diabetes in adulthood62.
In terms of socioeconomic inequality, our study indicated that diabetes and prediabetes are more prevalent among less educated people and among people with lower wealth scores. These findings are consistence with the studies conducted in other countries11,63. A study conducted by Al-Hanawi et al. in Saudi Arabia indicated that diabetes prevalence was concentrated among the poor and among people with less education. They also concluded that education-related inequality was higher than income-related inequality64.
It is worth noting that 97% of the participants underwent blood sampling, which was much higher than in other similar studies. However, due to the cross-sectional nature of this study and the unclear temporality of the relationship between the variables, the effect size values should be interpreted with caution. Another limitation of the study was the use of fasting glycemic index as a proxy to assess diabetes control. In this study, due to financial constraints, stronger indicators such as HbA1C were not used.
Conclusion
A significant proportion of DM awareness and treatment can be due to the integration of diabetes in the primary health care system. The high prevalence of prediabetes and diabetes, which is affected by socioeconomic inequality and combined with low levels of glycemic control, may place a more significant burden on the health system. It is worth noting that among all people with diabetes, only 28.50% controlled their FPG level. This means, more than 70% of people were not controlled which may cause more burden of DM related complications in the future. As well as, more than 20% were unaware of their diabetes status and about 31.50% of people with diabetes do not receive any treatment. So, it is necessary to encourage people to have an annual check-up by a health physician, as well as this, periodic check-ups of blood sugar levels in people with diabetes are recommended. Therefore, it is suggested emphasizing education of patients and their physicians on trying to reach the defined goals in diabetes management.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DM:
-
Diabetes Mellitus
- SES:
-
Socioeconomic status
- WHO:
-
World Health Organization
- NCDs:
-
Non communicable diseases
- SDGs:
-
Sustainable Development Goals
- DehPCS:
-
Dehgolan prospective cohort study
- RCI:
-
Relative concentration index
- PERSIAN:
-
Prospective epidemiological research study in Iran
- BMI:
-
Body mass index
- MCA:
-
Multiple correspondence analysis
- MET:
-
Metabolic equivalent task
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- FPG:
-
Fasting plasma glucose
- CI:
-
Confidence interval
- OR:
-
Odds ratio
References
Honnudóttir, V. et al. Social inequality in type 2 diabetes mellitus in the Faroe Islands: A cross-sectional study. Scand. J. Public Health 50, 638 (2021).
Lin, X. et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 10(1), 14790 (2020).
ID Federation. IDF Diabetes Atlas, 10th edn. https://diabetesatlas.org/. (Accessed 28 April 2022) (2021).
National Institute of Health Researches of Iran. Atlas of STEPwise Approach to Noncommunicable Disease (NCD) Risk Factor Surveillance (STEPs) 2021, 1–631 (Spring, 2022).
Javanbakht, M., Mashayekhi, A., Baradaran, H. R., Haghdoost, A. & Afshin, A. Projection of diabetes population size and associated economic burden through 2030 in Iran: Evidence from micro-simulation Markov model and Bayesian meta-analysis. PLoS ONE 10(7), e0132505 (2015).
Safari-Faramani, R. et al. Prevalence, awareness, treatment, control, and the associated factors of diabetes in an Iranian Kurdish population. J. Diabetes Res. 2019, 1–9 (2019).
Hadaegh, F. et al. High prevalence of undiagnosed diabetes and abnormal glucose tolerance in the Iranian urban population: Tehran Lipid and Glucose Study. BMC Public Health 8(1), 1–7 (2008).
Denova-Gutiérrez, E. et al. Asociación entre las inequidades socioeconómicas y la diabetes tipo 2 mediada por la obesidad y factores del estilo de vida en adultos mexicanos: Un enfoque de modelos de ecuaciones estructurales. Salud Pública de México 62(2), 192–202 (2020).
Williams, E. D. et al. Health behaviours, socioeconomic status and diabetes incidence: The Australian Diabetes Obesity and Lifestyle Study (AusDiab). Diabetologia 53(12), 2538–2545 (2010).
Lai, S. et al. Socioeconomic inequalities in the prevalence of chronic diseases and preventive care among adults aged 45 and older in Shaanxi Province. China. BMC Public Health 19(1), 1–12 (2019).
Tatulashvili, S. et al. Socioeconomic inequalities and type 2 diabetes complications: A systematic review. Diabetes Metab. 46(2), 89–99 (2020).
Hasan, M., Tasnim, F., Tariqujjaman, M. & Ahmed, S. Socioeconomic inequalities of undiagnosed diabetes in a resource-poor setting: Insights from the cross-sectional Bangladesh demographic and health survey 2011. Int. J. Environ. Res. Public Health 16(1), 115 (2019).
Khamseh, M. E. et al. Nationwide prevalence of diabetes and prediabetes and associated risk factors among Iranian adults: Analysis of data from PERSIAN cohort study. Diabetes Therapy 12(11), 2921–2938 (2021).
Poustchi, H. et al. Prospective epidemiological research studies in Iran (the PERSIAN cohort study): Rationale, objectives, and design. Am. J. Epidemiol. 187(4), 647–655 (2018).
Moradpour, F. et al. Cohort profile: Dehgolan prospective cohort study (DehPCS) on non-communicable diseases in a Kurdish community in the west of Iran. Epidemiol. Health 43, e2021075 (2021).
World health organization. A Healthy Lifestyle—WHO Recommendations 2010. https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (2022).
Greenacre, M. & Blasius, J. Multiple Correspondence Analysis and Related Methods (Chapman and Hall/CRC, 2006).
Aadahl, M. & Jorgensen, T. Validation of a new self-report instrument for measuring physical activity. Med. Sci. Sports Exerc. 35(7), 1196–1202 (2003).
Lu, Y. et al. Comparison of prevalence, awareness, treatment, and control of cardiovascular risk factors in China and the United States. J. Am. Heart Assoc. 7(3), 7462 (2018).
Chobanian, A. V. et al. Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 42(6), 1206–1252 (2003).
American Diabetes Association. 2 Classification and diagnosis of diabetes: Standards of medical care in diabetes-2021. Diabetes Care 44(Suppl 1), S15–S33 (2021).
O’Donnell, O., O’Neill, S., Van Ourti, T. & Walsh, B. conindex: Estimation of concentration indices. Stata J. 16(1), 112–138 (2016).
Katibeh, M. et al. Prevalence and risk factors of diabetes mellitus in a central district in Islamic Republic of Iran: A population-based study on adults aged 40–80 years. East. Mediterr. Health J. 21(6), 412–419 (2015).
Yazdanpanah, L. et al. Prevalence, awareness and risk factors of diabetes in Ahvaz (South West of Iran). Diabetes Metab. Syndr. 10(2), S114–S118 (2016).
Mirzaei, M., Rahmaninan, M., Mirzaei, M. & Nadjarzadeh, A. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes in Central Iran: Results from Yazd health study. BMC Public Health 20(1), 1–9 (2020).
Akbarzadeh, A. et al. Epidemiology of adult diabetes mellitus and its correlates in pars cohort study in southern Iran. Arch. Iran. Med. 22, 11 (2019).
Akhtar, S. et al. The prevalence of diabetes in Afghanistan: A systematic review and meta-analysis. BMC Public Health 21(1), 1–8 (2021).
Akhtar, S., Nasir, J. A., Abbas, T. & Sarwar, A. Diabetes in Pakistan: A systematic review and meta-analysis. Pak. J. Med. Sci. 35(4), 1173 (2019).
Akhtar, S. et al. Prevalence of diabetes and pre-diabetes in Bangladesh: A systematic review and meta-analysis. BMJ Open 10(9), e036086 (2020).
Gyawali, B. et al. Prevalence of type 2 diabetes in Nepal: A systematic review and meta-analysis from 2000 to 2014. Glob. Health Action 8(1), 29088 (2015).
Aeschbacher, S. et al. Association of smoking and nicotine dependence with pre-diabetes in young and healthy adults. Swiss Med. Wkly. 144, 14019 (2014).
Bucheli, J. R., Manshad, A., Ehrhart, M. D., Camacho, J. & Burge, M. R. Association of passive and active smoking with pre-diabetes risk in a predominantly Hispanic population. J. Investig. Med. 65(2), 328–332 (2017).
Akter, S., Goto, A. & Mizoue, T. Smoking and the risk of type 2 diabetes in Japan: A systematic review and meta-analysis. J. Epidemiol. 27(12), 553–561 (2017).
Willi, C., Bodenmann, P., Ghali, W. A., Faris, P. D. & Cornuz, J. Active smoking and the risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 298(22), 2654–2664 (2007).
Schrieks, I. C., Heil, A. L., Hendriks, H. F., Mukamal, K. J. & Beulens, J. W. The effect of alcohol consumption on insulin sensitivity and glycemic status: A systematic review and meta-analysis of intervention studies. Diabetes Care 38(4), 723–732 (2015).
Baik, I. & Park, S. I. Associations of alcohol consumption and physical activity with lean type 2 diabetes mellitus among Korean adults: A prospective cohort study. PLoS ONE 15(9), e0238641 (2020).
Wang, R. et al. The prevalence of pre-diabetes and diabetes and their associated factors in Northeast China: A cross-sectional study. Sci. Rep. 9(1), 1–8 (2019).
Klen, J., Goričar, K., Janež, A. & Dolžan, V. NLRP3 inflammasome polymorphism and macrovascular complications in type 2 diabetes patients. J. Diabetes Res. 2015, 1 (2015).
Hu, M. et al. Prevalence, awareness and associated risk factors of diabetes among adults in Xi’an, China. Sci. Rep. 7(1), 1–9 (2017).
McDonald, M., Hertz, R. P., Unger, A. N. & Lustik, M. B. Prevalence, awareness, and management of hypertension, dyslipidemia, and diabetes among United States adults aged 65 and older. J. Gerontol. Ser. A 64(2), 256–263 (2009).
Ho, B. et al. Prevalence, awareness, treatment and control of diabetes mellitus among the elderly: The 2011 National Health and Morbidity Survey, Malaysia. Malay. Fam. Phys. 9(3), 12 (2014).
Esteghamati, A. et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005–2011. Diabetes Res. Clin. Pract. 103(2), 319–327 (2014).
Kumar, S. & Agrawal, K. L. A questionnaire-based study of diabetic patients’ awareness and understanding of diabetic retinopathy at a tertiary care hospital in Bihar State. Eur. J. Mol. Clin. Med. 7, 11 (2020).
Le, C., Jun, D., Zhankun, S., Yichun, L. & Jie, T. Socioeconomic differences in diabetes prevalence, awareness, and treatment in rural southwest China. Trop. Med. Int. Health 16(9), 1070–1076 (2011).
Brown, A. F. et al. Socioeconomic position and health among persons with diabetes mellitus: A conceptual framework and review of the literature. Epidemiol. Rev. 26(1), 63–77 (2004).
Khosravi, A., Emamian, M. H., Hashemi, H. & Fotouhi, A. Pre-hypertension and the risk of diabetes mellitus incidence using a marginal structural model in an Iranian prospective cohort study. Epidemiol. Health 40, e2018026 (2018).
Baptiste-Roberts, K. et al. Family history of diabetes, awareness of risk factors, and health behaviors among African Americans. Am. J. Public Health 97(5), 907–912 (2007).
Alanazi, F. K. et al. Knowledge and awareness of diabetes mellitus and its risk factors in Saudi Arabia. Saudi Med. J. 39(10), 981 (2018).
Ebrahimi, M. et al. Social disparities in prevalence, treatment and control of hypertension in Iran: Second National Surveillance of risk factors of noncommunicable diseases, 2006. J. Hypertens. 28(8), 1620–1629 (2010).
Barreto, M. et al. Prevalence, awareness, treatment and control of diabetes in Portugal: Results from the first National Health examination Survey (INSEF 2015). Diabetes Res. Clin. Pract. 140, 271–278 (2018).
Liu, X. et al. Prevalence, awareness, treatment, control of type 2 diabetes mellitus and risk factors in Chinese rural population: The RuralDiab study. Sci. Rep. 6(1), 1–9 (2016).
Moradi, G., Shokri, A., Mohamadi-Bolbanabad, A., Zareie, B. & Piroozi, B. Evaluating the quality of care for patients with type 2 diabetes mellitus based on the HbA1c: A national survey in Iran. Heliyon 7(3), e06485 (2021).
Fadare, J., Olamoyegun, M. & Gbadegesin, B. Medication adherence and direct treatment cost among diabetes patients attending a tertiary healthcare facility in Ogbomosho, Nigeria. Malawi Med. J. 27(2), 65–70 (2015).
Jensen, E. X., Fusch, C., Jaeger, P., Peheim, E. & Horber, F. F. Impact of chronic cigarette smoking on body composition and fuel metabolism. J. Clin. Endocrinol. Metab. 80(7), 2181–2185 (1995).
Iino, K., Iwase, M., Tsutsu, N. & Iida, M. Smoking cessation and glycaemic control in type 2 diabetic patients. Diabetes Obes. Metab. 6(3), 181–186 (2004).
Raum, E. et al. Medication non-adherence and poor glycaemic control in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 97(3), 377–384 (2012).
Dam, K. & Hall, E. O. Childhood experiences pursue adulthood for better and worse: A qualitative study of adults’ experiences after growing up with a severely mentally ill parent in a small-scale society. J. Res. Nurs. 25(6–7), 579–591 (2020).
Agardh, E., Allebeck, P., Hallqvist, J., Moradi, T. & Sidorchuk, A. Type 2 diabetes incidence and socio-economic position: A systematic review and meta-analysis. Int. J. Epidemiol. 40(3), 804–818 (2011).
Maddah, M. Association of diabetes with living area in Iranian women. Int. J. Cardiol. 143(1), 100–102 (2010).
Peykari, N. et al. Socioeconomic inequalities and diabetes: A systematic review from Iran. J. Diabetes Metab. Disord. 14(1), 1–13 (2015).
Safieddine, B. et al. Socioeconomic inequalities in type 2 diabetes in employed individuals, nonworking spouses and pensioners. SSM-Popul. Health 11, 100596 (2020).
Derks, I. P. et al. The association of early life socioeconomic conditions with prediabetes and type 2 diabetes: Results from the Maastricht study. Int. J. Equity Health 16(1), 1–7 (2017).
Ortiz, M. S., Cabieses, B., Oyarte, M. & Repetto, P. Disentangling socioeconomic inequalities of type 2 diabetes mellitus in Chile: A population-based analysis. PLoS ONE 15(9), e0238534 (2020).
Al-Hanawi, M. K., Chirwa, G. C. & Pulok, M. H. Socio-economic inequalities in diabetes prevalence in the Kingdom of Saudi Arabia. Int. J. Health Plann. Manage. 35(1), 233–246 (2020).
Acknowledgements
Special thanks to the central committee who provided their consultancy without any expectations in return. We also wish to acknowledge the assistance provided by the technical and support staff of the DehPCS.
Funding
The Iranian Ministry of Health and Medical Education contributed to funding for the PERSIAN cohort study through Grant No. 700/534.
Author information
Authors and Affiliations
Contributions
Conceptualization: S.R., G.M., Y.M., N.P., B.P. Data curation: F.M., A.S. Formal analysis: F.M., Y.M., G.M., A.S. Funding acquisition: F.M. Writing—original draft: F.M., A.S., G.M. Writing—review & editing: S.R., G.M., Y.M., N.P., B.P.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Moradpour, F., Rezaei, S., Piroozi, B. et al. Prevalence of prediabetes, diabetes, diabetes awareness, treatment, and its socioeconomic inequality in west of Iran. Sci Rep 12, 17892 (2022). https://doi.org/10.1038/s41598-022-22779-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-22779-9
- Springer Nature Limited
This article is cited by
-
Socioeconomic inequalities in type 2 diabetes mellitus: a study based on a population-based survey in Iran
BMC Public Health (2024)
-
Relationship between diabetes health literacy, distress, burnout, social support, complications, self-care behaviors, and quality of life among patients with type 2 diabetes: a path analysis study
Diabetology & Metabolic Syndrome (2024)
-
Evaluation of the knowledge and practice of family physicians in the management of diabetes mellitus type 2 in Iran
BMC Primary Care (2023)
-
The evaluation of the role of diabetes health literacy and health locus of control on quality of life among type 2 diabetes using the Path analysis
Scientific Reports (2023)
-
Evaluation of the diabetes care cascade and compliance with WHO global coverage targets in Iran based on STEPS survey 2021
Scientific Reports (2023)