
Abstract
The aim of this study was to investigate the associations between liver fat content (LFC), sedentary behaviour (SB), physical activity (PA), fitness, diet, body composition, and cardiometabolic risk factors in adults with metabolic syndrome. A total of 44 sedentary adults (mean age 58 [SD 7] years; 25 women) with overweight or obesity participated. LFC was assessed with magnetic resonance spectroscopy and imaging, SB and PA with hip-worn accelerometers (26 [SD 3] days), fitness by maximal bicycle ergometry, body composition by air displacement plethysmography and nutrient intake by 4-day food diaries. LFC was not independently associated with SB, PA or fitness. Adjusted for sex and age, LFC was associated with body fat%, body mass index, waist circumference, triglycerides, alanine aminotransferase, and with insulin resistance markers. There was and inverse association between LFC and daily protein intake, which persisted after further adjusment with body fat%. LFC is positively associated with body adiposity and cardiometabolic risk factors, and inversely with daily protein intake. SB, habitual PA or fitness are not independent modulators of LFC. However, as PA is an essential component of healthy lifestyle, it may contribute to liver health indirectly through its effects on body composition in adults with metabolic syndrome.
Similar content being viewed by others


Introduction
Obesity is associated with an increased risk of developing non-alcoholic fatty liver disease (NAFLD)1. In NAFLD excess triglycerides accumulate in the hepatocytes increasing liver fat content (LFC), which may cause inflammation and damage the liver1. NAFLD is associated with metabolic syndrome (MetS) and is described as the hepatic component of this condition2. MetS is a complex disorder characterized by elevated fasting plasma glucose and triglycerides levels, hypertension, low HDL levels, and a large waist circumference [WC]3, and it increases the risk of cardiovascular diseases and type 2 diabetes4. The current obesity pandemic is estimated to lead to 25% of the global population eventually developing NAFLD, which is identified as one of the growing causes of liver cancer5. NAFLD is usually asymptomatic and becomes apparent when the situation is already severe6. Therefore, early diagnosis and prevention play important roles in the detection and treatment of this disease.
Sedentary behaviour (SB) is associated with unhealthy body composition7,8,9, whereas habitual PA is associated with lowered body fat%, body mass index [BMI] and WC10,11. Previous studies have shown that LFC is positively associated with SB and inversely with PA, and this association is strengthened in a dose-dependent manner12,13,14,15,16,17. However, these studies were based on self-reports, which can overestimate actual SB and PA levels18. Further, in a majority of these studies LFC was determined by ultrasound or fatty liver index, instead of the gold standard LFC assessment methods liver biopsy and magnetic resonance spectroscopy (MRS). To our knowledge, only few studies to date have investigated the associations between accelerometer-measured SB and PA and liver health19,20,21. The duration of accelerometry measurement has generally been only 4–7 days, however, which might not accurately represent habitual activity and behavior over longer periods of time22. Additionally, cardiorespiratory fitness and diet were assessed only in one study19.
Therefore, the primary aim of this study was to comprehensively and simultaneously investigate important lifestyle factors and liver health, measured as LFC. We particularly wanted to examine the associations between LFC and SB and habitual PA in sedentary adults with MetS, who are thus at increased risk of developing metabolic diseases. LFC was quantified with two methods: MRS and magnetic resonance imaging (MRI). In contrast to previous studies with short accelerometer measurements, SB and PA were assessed with accelerometers continuously for one month to get a more comprehensive representation of daily behaviors. We also examined the associations between LFC and fitness, daily nutrient and energy intake, and common markers of cardiometabolic health. Lastly, we also evaluated the correlation and agreement between the two different LFC quantification methods.
Methods
Study design
This study used the baseline data of an intervention trial (Medical and physiological benefits of reduced sitting, ClinicalTrials.gov ID NCT03101228) performed at the Turku PET Centre, Turku, Finland between April 2017 and August 2019. All participants gave written informed consent. The study was conducted according to good clinical practice and the Declaration of Helsinki and approved by the Ethics Committee of the Hospital District of Southwest Finland (16/1810/2017).
Participants
The participants were physically inactive, middle-aged adults with MetS3 who were recruited locally through bulletin boards and newspaper advertisements.The inclusion and exclusion criteria are described in Table 1.
Measurements
Liver fat content
LFC was measured by MRS and MRI, based on two-point Dixon [2PD] method using a Philips 3 Tesla system (Ingenuity TF PET/MR) with a Q-Body coil. Because of the MRI scanner replacement during this study, MRS and MRI quantification of LFC of seven participants were conducted with Siemens Magnetom Skyra fit 3T MRI system (Siemens Healthcare, Erlangen, Germany) with Siemens Body 30 and 18 channel coils, and 32 channel Spine coil. A detailed description of the measurement is presented in the Supplementary Material (S1).
SB and PA measurements
SB and PA were measured for four weeks with validated hip-worn tri-axial accelerometers (UKK AM30, UKK-Institute, Tampere, Finland) and analysis methods. In short, the collected accelerometer data was analyzed in six-second epochs and SB (sitting and lying together), standing, light physical activity (LPA), moderate-to-vigorous physical activity (MVPA), steps, and breaks in SB were defined using validated mean amplitude deviation (MAD)23 and angle for posture estimation (APE) methods24. The following SB and PA variables were calculated: mean daily SB time, mean daily standing time, mean daily LPA time, mean daily MVPA time, and mean daily steps. For a valid data collection, daily wear time of 10–19 h and at least 4 days of valid measurements were required. Daily measurement time exceeding 19 h indicates that the participant has likely slept with the accelerometer and measurement hours exceeding the 19 h per day were substracted from the SB time.
Cardiorespiratory fitness
Maximal oxygen consumption (VO2max) measurements were conducted after the participants had passed a thorough physical examination and electrocardiographical measurements. VO2max was determined by bicycle ergometry (eBike EL Ergometer + CASE v6.7, GE Medical Systems Information Technologies, Inc. Milwaukee, WI, USA) with direct respiratory gas measurements (Vyntus CPX, CareFusion, Yorba Linda, CA, USA). We also determined VO2max per fat free mass (FFM) (ml/min/kgFFM), and maximal load (Wmax). A detailed description of the measurements is included in Supplementary Material (S1).
Whole-body insulin sensitivity and blood sampling
Whole-body insulin-stimulated glucose uptake (M-value) was measured and calculated with the gold standard method hyperinsulinemic-euglycemic clamp, as previously reported25. Venous blood samples were drawn after at least 10 h of fasting. Plasma glucose, plasma insulin, hemoglobin A1c (HbA1c), plasma triglycerides, total cholesterol, LDL, HDL, alanine aminotransferase (ALT), aspartate aminotransferase (AST) and γ-glutamyltransferase (GGT) were determined according to methods described in the Supplementary Material (S1). Homeostatic model assessment of insulin resistance (HOMA-IR) was calculated using the formula: fasting glucose (mmol/l) × fasting insulin (mU/l)/22.5.
Nutrient intake
Nutrient intake was examined by 4-day food diaries (including one weekend day) and analyzed by a nutritionist with a computerized software (AivoDiet 2.2.0.1, Aivo, Turku) utilizing the Finnish Food Composition Database Fineli26. Participants were guided not to change their normal dietary habits during the study.
Body composition, anthropometry, blood pressure and resting heart rate
Participants could choose the measurement time by convenience. Validated27 air displacement plethysmography (the Bod Pod system, COSMED, Inc., Concord, CA, USA) with predicted thoracic gas volume was used to estimate body composition (body fat%, fat mass and fat-free mass) after fasting for at least four hours. Participants were advised not to exercise or take a shower beforehand on the day of the measurement. After emptying the bladder, participants entered the measurement chamber wearing a tight cap and underwear or swimming suit. Body weight, body height, waist circumference, blood pressure and resting heart rate were measured according to details reported in the Supplementary Material (S1).
Statistical methods
The associations between LFC (dependent variable) and SB and PA measures, fitness, health markers and nutrient intake (independent variables) were examined with linear mixed models. Unpaired t-test was first used to compare sexes. All the models were adjusted for age, and because of a significant between-sex difference in LFC values, sex was also included as an explanatory variable in all the analyses (model 1). Body fat% was added to the linear model to adjust for confounding overweight or obesity (model 2). Normal distribution of the residuals was assessed by visual evaluation and Shapiro–Wilk test, and logarithmic transformations were used when necessary to fulfil the normal distribution assumption. Linear regression model, Tukey mean difference test and Bland–Altman analysis were used to analyze the correlation and the agreement between MRS and MRI (2PD); the results are reported in the Supplementary File (S2). Multicollinearity was controlled for with variance inflation factors, which were all below five indicating no multicollinearity issues. Missing data was handled by pairwise deletion. Power calculation for determining the sample size was done for the primary outcome (whole-body insulin sensitivity) of the sedentary behaviour reduction intervention trial (NCT03101228), from which baseline imaging measurements form the data for the current study. MRS-measured LFCs of three participants were missing due to image artifacts and MRS and MRI-measured LFCs of one participant were missing due to technical challenges with the scanner. VO2max measures of two participants were missing because they interrupted the test before reaching exhaustion (knee pain or difficulties in breathing) and the results of one participant were lost due to technical difficulties. Fasting plasma glucose value of one participant and resting heart rate values of two participants were missing due to incomplete documentation. If not otherwise stated, data are expressed as mean and standard deviation (SD), standardized β coefficients and 95% CI values. The level of statistical significance was set at 5% (two-tailed). All analyses were carried out with the JMP pro 13.1 for Windows (SAS Institute Inc., Cary, NC, USA) and with GraphPad Prism version 5.01 for Windows (GraphPad Software, La Jolla California USA).
Results
Characteristics of the participants
Participants’ baseline characteristics are presented by sex in Table 2. Sixty-six percent of the participants were obese (BMI > 30 kg/m2) and 34% were overweight (BMI 25.0 to < 30). Men had significantly higher LFC, AST, HOMA-IR, and fasting insulin levels compared to women, while women had higher body fat% and HDL levels. Women also had slightly longer daily accelerometer wear time, standing time, daily standing%, LPA and LPA% and breaks in SB. On the other hand, men had higher daily SB% and VO2max levels when compared to women.
Associations of body composition with SB and PA
The associations between body fat%, WC, BMI and SB, PA and fitness are presented in Table 3. When adjusted for age and sex, body fat% associated positively with lying time (h/day) and SB time (%/day), and negatively with standing (h/day), daily steps, MVPA, MVPA%, total PA and VO2max. WC associated positively with lying time and SB%, and negatively with standing, standing%, MVPA, MVPA%, total PA, daily steps and breaks in SB. BMI associated positively with lying time, and negatively with standing, MVPA, daily steps, breaks in SB and VO2max.
Associations of LFC with SB and PA
When adjusted for age and sex, LFC was not associated with any of the SB or PA variables (model 1, Table 4). Associations remained non-significant when body fat% was added to the model (model 2, Table 4). The associations of MRI-measured LFC with SB and PA are presented in the Supplementary File (S2).
Associations of LFC with fitness and nutrient intake
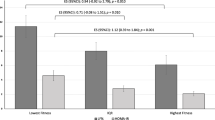
In the sex- and age-adjusted model LFC was not associated with VO2 max (ml/min/kg) (model 1, Table 5), and when body fat% was included in the model, the association remained non-significant (model 2, Table 5). Also, when fitness was expressed as VO2max (ml/min/kgFFM) or Wmax, none of the associations were significant (model 1–2, Table 5). In the sex- and age-adjusted model LFC was not associated with any of the nutrient intake variables expressed as % of daily energy intake (model 1, Table 5). When body fat% was added to the model, all other associations were non-significant except for the association between LFC and protein intake (model 2, Table 5). The associations of MRI-measured LFC with fitness and nutrient intake are presented in the Supplementary File (S2).
Additionally, we tested the associations between LFC (measured by MRS and MRI) and the daily intake of protein, carbohydrates, fat, alcohol, saturated fatty acids (SFA), monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), saccharose and fiber measured in grams. MRS-measured LFC was not associated with any of the nutrient variables, when adjusted for sex and age, nor when further adjusted for body fat % (data not shown). MRI-measured LFC was associated with MUFA (g) (β = 0.35, 95% CI [0.05, 0.64], p = 0.02). However, when body fat % was added to the model, the association turned non-significant (β = 0.22, 95% CI [− 0.007, 0.50], p = 0.13).
Associations of LFC with body adiposity and other health markers
When adjusted for age and sex, LFC associated positively with body fat%, BMI, WC, triglycerides, ALT, fasting insulin, HOMA-IR, M-value and HbA1c (model 1, Table 6). After further adjustment for body fat%, LFC remained positively associated with WC, M-value, HbA1c, triglycerides and ALT, and the association between LFC and GGT turned significant. On the other hand, the associations between LFC and fasting insulin and HOMA-IR turned non-significant (model 2, Table 6). The associations between the MRI-measured LFC with body adiposity and other health markers are presented in the Supplementary File (S2).
Discussion
In the present study, we found that LFC is not associated with accelerometer-measured SB, habitual PA or fitness in sedentary adults with MetS. Additionally, we found that LFC is associated with body fat%, BMI and WC, and also with other health risk markers (insulin resistance, fasting triglycerides and circulating liver enzymes) independent of body adiposity. We also demonstrated that body composition (body fat%, BMI and WC) was positively associated with daily SB and negatively with habitual PA. Thus, our results indicate that body adiposity is a key regulator of LFC, but LFC is also independently clustered with other cardiometabolic risk factors. We also detected that LFC was negatively associated with the energy intake from protein, which might refer that replacing some of the daily carbohydrates and/or fat with protein sources might improve liver health. Our study gives new insights to the associations between LFC and accelerometer-measured SB and PA, fitness and nutrient intake in adults with MetS. Additionally, our study shows the compatibility of MRS and MRI (2PD) for measuring LFC.
Associations of LFC with SB and PA
LFC was not associated with SB, standing or habitual PA performed at different intensities. When adjusted for sex and age, only the association between MRI-measured LFC and daily steps was significant. However, when body fat% was added to the model the association was non-significant, suggesting that the association between LFC and steps is mediated by body adiposity. Although with a larger number of participants, the majority of the previous studies investigating associations between LFC and SB and PA have used self-reports to determine SB and PA. Most have reported a positive association between LFC and SB15,16 and a negative association between LFC and PA12,13,14,17. Additionally, a stronger association between LFC and PA has been shown with increased amount and intensity of PA12,13,14. However, in one previous study the association between LFC and PA was attenuated when WC was added to the model17. SB has also been suggested to be an independent predictor of NAFLD based on the data from the National Health and Nutrition Examination Survey (NHANES) 2007–201628. The NHANES 2007–2016 study also indicated that increasing habitual and transportation-related PA would lower the risk of NAFLD in a dose-dependent manner28. Although the study had a very large nationally representative cohort of US adults, SB was likely underestimated and PA overestimated since SB and PA levels were based on self-reports18.
On the other hand, the few studies with accelerometer-measured PA have shown mixed results. In contrast to our findings, a positive association between the measured SB and MRS-measured liver fat% was found in 98 habitually active young—middle aged adults with or without MetS, when adjusted for age and BMI19. Another study with sixty-six adults found that more time spent in SB was associated with higher liver fat% in individuals at high risk of developing metabolic diseases such as type 2 diabetes20. However, there is also evidence supporting our findings. For example, in adults with overweight or obesity liver fat was not associated with the measured habitual PA or SB21.
Differences in the results might originate from differences in study populations, methods, and genetic variation in fitness levels29. Most of the previous studies determined LFC by ultrasound or fatty liver index, instead of the gold standard assessment methods liver biopsy and MRS, which may affect the results. An important difference in the methods pertains to the variation in data collection time between the studies. In all previous studies the accelerometer-measured PA was collected during 4–7 days, whereas in our study the mean data collection was 26 days. This is likely to provide a more comprehensive representation of daily behaviors compared to short measurement periods. In addition, the placement of the accelerometer can also have an impact on the results. Majority of the previous studies used wrist-worn accelerometers to measure SB and PA19,21, whereas, we used hip-worn accelerometers. With this placement the device is closer to the center of mass of the body, and thus detects more accurately body motion and postural differences30.
Lastly, it seems that the intensity and the duration of PA might be they key factors to reveal any significant associations between LFC and PA. For example, a recent meta-analysis showed that high and moderate levels of PA are associated with a reduced risk of NAFLD, and that the risk is reduced in a dose-dependent manner. The meta-analysis also suggested that PA amount above the recommended minimum of 150 min of moderate- or 75 min of vigorous-intensity activity might be required to achieve a considerable reduction in NAFLD risk31. Thus, the major reason for not finding any associations between LFC and PA in our study might be the inactive and sedentary population that was used. It is possible that there was not enough variation in PA levels in our homogenous study group. Thus, our data suggests that neither SB nor habitual PA is independently associated with LFC in inactive adults with metabolic syndrome, and a higher amount and/or intensity of PA might be needed to improve LFC.
Associations of LFC with fitness and nutrition
When adjusted for sex and age, MRI-measured LFC was significantly associated with VO2max. However, when body fat % was added to the model the associations were attenuated, regardless of the measurement method of LFC. Similar results with same statistical adjustments have been reported previously32. Our finding together with previous evidence suggests that fitness is not independently associated with LFC, and the primary regulator of LFC is the overall adiposity, and thus reducing excess body fat would be the key factor to impact LFC.
We also found that, when adjusted for sex, age and body fat%, MRS- and MRI-measured LFC was negatively associated with daily protein intake (% of total energy intake). This is in line with a recent review33 that suggests that a diet high in protein, particularly that of plant-based origin, and a low content of carbohydrates and sugars would be one strategy to improve LFC and insulin sensitivity.
We did not find any significant associations between LFC and intakes of carbohydrates, sugars or saturated or unsaturated fatty acids. The reason for this could be that there was not enough variation in the nutrient intake in our study participants with overweight and obesity. It has been shown that fat and carbohydrates can have different influence in liver fat accumulation, and the effects may differ based on the type of the macronutrient34,35. Saturated fatty acids and fructose have been found to induce the greatest increases in intrahepatic triglycerides, and on the other hand, unsaturated fatty acids have been found to have beneficial effects on liver health34,35,36. Recent meta-analysis showed that replacing saturated fatty acids with unsaturated fatty acids leads to decrease in liver fat content35. Additionally, previous studies indicate that diets with low carbohydrate content are beneficial for subjects with NAFLD37. Thus, it seems that replacing some of the daily carbohydrates and/or fats with protein sources might associate with healthier LFC in adults at increased risk of cardiometabolic diseases. For summary, previous studies shows that both the quality and quantity of different macronutrients play important role in liver fat accumulation. Nevertheless, it seems that the total daily calories rather than different proportions of macronutrients may be more important factor for the liver fat content34,38.
Associations of LFC with general health markers
In our study, LFC was positively associated with markers of obesity (body fat%, BMI and WC). Similarly, previous studies have also shown a strong association between fatty liver and obesity39,40,41. Moreover, high BMI increases NAFLD risk in a dose-dependent manner40. In the current study LFC was also positively associated with insulin resistance markers such as fasting insulin, M-value, HOMA-IR and HbA1c, when adjusted for sex and age. However, only the associations between LFC and M-value and HbA1c remained significant when body fat% was added to the model. Similar associations between LFC and risk factors related to glucose metabolism have been reported earlier42,43. For example, fatty liver index has been positively associated with insulin resistance, coronary heart disease and atherosclerosis42.
We showed that LFC is positively associated with fasting plasma triglycerides. Fasting triglycerides have also previously been shown to strongly associate with NAFLD, and elevated triglyceride levels in the blood have been indicated as markers of high LFC in adults with or without NAFLD33. Additionally, we found that LFC was positively associated with circulating liver enzymes (ALT, AST and GGT). This was expected, since serum liver enzyme levels are commonly used to detect liver diseases. However, these enzymes are not always elevated in NAFLD44. Diagnosed only with blood sampling, the true prevalence of NAFLD might be significantly underestimated. To conclude, our results build on the existing evidence and support the notion that obesity and other cardiometabolic risk factors (e.g., insulin resistance, elevated blood lipids, and elevated liver enzyme levels) are closely associated with LFC.
Correlation and agreement between MRS and MRI
In the present study we also tested the correlation and agreement between two LFC-quantification methods: MRS and MRI (2PD). Our results show that MRI correlated strongly with MRS (S2, Fig. 1). However, when we tested the agreement between these two methods (S2, Fig. 2), the mean difference was statistically significant. The reason for this is that MRI systematically gave higher (over 2.5 times greater) LFC-values than MRS. Previously liver biopsy has been shown to give over two times greater LFC-values than MR-techniques45. Liver biopsy is the most accurate method to quantify liver fat46, however, it is not always the most feasible method to use due to its invasive nature. Both MRS and MRI have been used to quantify LFC in clinical practice, but MRS has appeared to be a more accurate method when compared to other non-invasive methods47. However, MRS also has some limitations, e.g., LFC can be misestimated due to the small size of the measured liver section, especially in case of heterogenous steatosis. It is also more time-consuming and challencing to perform compared to MRI45. Further studies are warranted to determine which of these two methods (MRS or MRI [2PD]) gives the most accurate results to measure LFC, when compared to liver biopsy. This is important in terms of the correct NAFLD diagnosis, because possible underestimation of LFC with MRS might leave underlying NAFLD undetected.
Strengths and limitations
The major strengths of our study are the methods that we used to quantify liver fat and SB and PA. LFC was measured with two different methods: MRI (2PD) and MRS, which is considered the golden standard method to non-invasively quantify liver fat47. We used validated algorithms and hip-worn accelerometers to measure SB and PA23,24. The placement of the accelerometer may provide more accurate representation of motion and postural differences than wrist-worn accelerometers48 used in previous investigations19,21. Additionally, one of the key strengths is the duration of the accelerometer data collection, which was considerably longer (26 days), compared to previous studies19,20,21, and thus can give more robust estimation of individual habitual PA and SB.
This study also has some limitations. Due to the MRI scanner replacement during the study, MRS and MRI quantification of LFC of seven participants were conducted with a different scanner, which might affect the results. Also, our sample size was relatively small, and power calculation was done only for longitudinal analysis. However, the used methods (MR, accelerometry as well as direct respiratory gas measurements in fitness test) are very sensitive for detecting small variations in the outcomes and therefore can be used with relatively small study samples. Lastly, very intensive studies for both study personnel and study participants were conducted. Additionally, we included only physically inactive sedentary participants. The results might have been different if we had included participants with more variation in their SB and habitual PA. However, previous evidence suggests that the intensity of PA may play an important role, and the amount of habitual PA by itself may not be strong enough stimulus to have a positive effect on LFC. It is also possible that the participants have either underestimated food intake or changed their eating behavior when filling the food diary. However, at the group level food diaries yield reliable information on the intake of energy yielding nutrients. More detailed analyses about the protein sources (animal or plant-based) would also have given more insights into the association between LFC and daily protein intake. However, it was beyond the scope of this study and can thus be considered a limitation.
Conclusions
In this study based on a one-month accelerometer-measurement of SB an PA, LFC was not associated with SB or habitual daily PA in sedentary inactive adults with MetS. However, we found positive associations between LFC and obesity markers (body fat%, BMI, WC), suggesting that weight loss especially from the abdominal area, is likely the primary method to reduce fat in the liver. We also showed that body composition (body fat%, BMI and WC) was positively associated with daily SB and negatively with habitual PA. Thus, SB and habitual PA may not be the main regulators of LFC, but they may indirectly affect liver health through their effects on body composition. Additionally, the negative association between LFC and daily protein intake suggest that replacing some of the carbohydrates and/or fat with protein sources in diet might associate with healthier LFC. Future studies should aim to assess the relationship between LFC and SB, habitual PA, fitness, as well as nutrient intake, in longitudinal and experimental settings, which may show causal relations.
Data availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
References
Sarwar, R., Pierce, N. & Koppe, S. Obesity and nonalcoholic fatty liver disease: Current perspectives. Diabetes Metab. Syndr. Obes. 11, 533–542 (2018).
Yki-Järvinen, H. Non-alcoholic fatty liver disease as a cause and a consequence of metabolic syndrome. Lancet Diabetes Endocrinol. 2(11), 901–910 (2014).
Alberti, K. G. et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 120(16), 1640–1645 (2009).
Nilsson, P. M., Tuomilehto, J. & Rydén, L. The metabolic syndrome—What is it and how should it be managed? Eur. J. Prev. Cardiol. 26(2), 33–46 (2019).
Huang, D. Q., El-Serag, H. B. & Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 18(4), 223–238 (2021).
Friedman, S. L., Neuschwander-Tetri, B. A., Rinella, M. & Sanyal, A. J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 24(7), 908–922 (2018).
Bellettiere, J. et al. Associations of sitting accumulation patterns with cardio-metabolic risk biomarkers in Australian adults. PLoS ONE 12(6), e0180119 (2017).
Heinonen, I. et al. Sedentary behaviours and obesity in adults: The cardiovascular risk in young Finns study. BMJ Open 3(6), 002901. https://doi.org/10.1136/bmjopen-002901 (2013).
Swartz, A. M. et al. Prediction of body fat in older adults by time spent in sedentary behavior. J. Aging Phys. Act. 20(3), 332–344 (2012).
Bradbury, K. E., Guo, W., Cairns, B. J., Armstrong, M. E. G. & Key, T. J. Association between physical activity and body fat percentage, with adjustment for BMI: A large cross-sectional analysis of UK Biobank. BMJ Open 7(3), e011843 (2017).
Cárdenas Fuentes, G. et al. Association of physical activity with body mass index, waist circumference and incidence of obesity in older adults. Eur. J. Public Health 28(5), 944–950 (2018).
Perseghin, G. et al. Habitual physical activity is associated with intrahepatic fat content in humans. Diabetes Care 30(3), 683–688 (2007).
Kistler, K. D. et al. Physical activity recommendations, exercise intensity, and histological severity of nonalcoholic fatty liver disease. Am. J. Gastroenterol. 106(3), 460–468 (2011).
Li, Y. et al. Dose–response association between physical activity and non-alcoholic fatty liver disease: A case–control study in a Chinese population. BMJ Open 9(3), e026854 (2019).
Ryu, S. et al. Relationship of sitting time and physical activity with non-alcoholic fatty liver disease. J. Hepatol. 63(5), 1229–1237 (2015).
Wei, H., Qu, H., Wang, H. & Deng, H. Associations between sitting time and non-alcoholic fatty liver diseases in Chinese male workers: A cross-sectional study. BMJ Open 6(9), e011939 (2016).
Zelber-Sagi, S. et al. Role of leisure-time physical activity in nonalcoholic fatty liver disease: A population-based study. Hepatol. Baltim. Md. 48(6), 1791–1798 (2008).
Sallis, J. F. & Saelens, B. E. Assessment of physical activity by self-report: Status, limitations, and future directions. Rese Q. Exerc. Sport. 71(2 Suppl), 1 (2000).
Bowden Davies, K. A. et al. Physical activity and sedentary time: Association with metabolic health and liver fat. Med. Sci. Sports Exerc. 51(6), 1169–1177 (2019).
Henson, J. et al. Associations of sedentary time with fat distribution in a high-risk population. Med. Sci. Sports Exerc. 47(8), 1727–1734 (2015).
Keating, S. E. et al. Objectively quantified physical activity and sedentary behavior in predicting visceral adiposity and liver fat. J. Obes. 2016, 2719014 (2016).
Sjöros, T. et al. Influence of the duration and timing of data collection on accelerometer-measured physical activity, sedentary time and associated insulin resistance. Int. J. Environ. Res. Public Health 18(9), 4950 (2021).
Vähä-Ypyä, H. et al. Validation of cut-points for evaluating the intensity of physical activity with accelerometry-based mean amplitude deviation (MAD). PLoS ONE 10(8), e0134813 (2015).
Vähä-Ypyä, H., Husu, P., Suni, J., Vasankari, T. & Sievänen, H. Reliable recognition of lying, sitting, and standing with a hip-worn accelerometer. Scand. J. Med. Sci. Sports. 28(3), 1092–1102 (2018).
Garthwaite, T. et al. Standing is associated with insulin sensitivity in adults with metabolic syndrome. J. Sci. Med Sport. 24(12), 1255–1260 (2021).
National Institute for Health and Welfare, Public Health Promotion Unit. Fineli. Finnish Food Composition Database. Release 20. Helsinki 2019. www.fineli.fi.
Fields, D. A., Goran, M. I. & McCrory, M. A. Body-composition assessment via air-displacement plethysmography in adults and children: A review. Am. J. Clin. Nutr. 75(3), 453–467 (2002).
Kim, D., Vazquez-Montesino, L. M., Li, A. A., Cholankeril, G. & Ahmed, A. Inadequate physical activity and sedentary behavior are independent predictors of nonalcoholic fatty liver disease. Hepatol. Baltim. Md. 72(5), 1556–1568 (2020).
Chung, H. C., Keiller, D. R., Roberts, J. D. & Gordon, D. A. Do exercise-associated genes explain phenotypic variance in the three components of fitness? A systematic review & meta-analysis. PLoS ONE 16(10), 1–18 (2021).
Chastin, S. et al. Joint association between accelerometry-measured daily combination of time spent in physical activity, sedentary behaviour and sleep and all-cause mortality: A pooled analysis of six prospective cohorts using compositional analysis. Br. J. Sports Med. 55(22), 1277 (2021).
Qiu, S. et al. Association between physical activity and risk of nonalcoholic fatty liver disease: A meta-analysis. Ther. Adv. Gastroenterol. 10(9), 701–713 (2017).
Church, T. S. et al. Association of cardiorespiratory fitness, body mass index, and waist circumference to nonalcoholic fatty liver disease. Gastroenterol. N. Y. 130(7), 2023–2030 (2006).
De Chiara, F., Ureta Checcllo, C. & Ramón, A. J. High protein diet and metabolic plasticity in non-alcoholic fatty liver disease: Myths and truths. Nutrients 11(12), 2985 (2019).
Hydes, T., Alam, U. & Cuthbertson, D. J. The impact of macronutrient intake on non-alcoholic fatty liver disease (NAFLD): Too much fat, too much carbohydrate, or just too many calories? Front. Nutr. 8, 640557 (2021).
Winters-van Eekelen, E. et al. Effects of dietary macronutrients on liver fat content in adults: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 75(4), 588–601 (2021).
Jensen, T. et al. Fructose and sugar: A major mediator of non-alcoholic fatty liver disease. J. Hepatol. 68(5), 1063–1075 (2018).
Haghighatdoost, F., Salehi-Abargouei, A., Surkan, P. & Azadbakht, L. The effects of low carbohydrate diets on liver function tests in nonalcoholic fatty liver disease: A systematic review and meta-analysis of clinical trials. J. Res. Med. Sci. 21(1), 53 (2016).
Parry, S. A. & Hodson, L. Influence of dietary macronutrients on liver fat accumulation and metabolism. J. Investig. Med. 65(8), 1102–1115 (2017).
Jakobsen, M., Berentzen, T., Sørensen, T. & Overvad, K. Abdominal obesity and fatty liver. Epidemiol. Rev. 29(1), 77–87 (2007).
Li, L. et al. Obesity is an independent risk factor for non-alcoholic fatty liver disease: Evidence from a meta-analysis of 21 cohort studies. Obes. Rev. 17(6), 510–519 (2016).
Riquelme, A. et al. Non-alcoholic fatty liver disease and its association with obesity, insulin resistance and increased serum levels of C-reactive protein in Hispanics. Liver Int. Off. J. Int. Assoc. Study Liver 29(1), 82–88 (2009).
Gastaldelli, A. et al. Fatty liver is associated with insulin resistance, risk of coronary heart disease, and early atherosclerosis in a large European population. Hepatol. Baltim. Md. 49(5), 1537–1544 (2009).
Yki-Järvinen, H. Fat in the liver and insulin resistance. Ann. Med. Hels. 37(5), 347–356 (2005).
Younossi, Z. M. et al. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatol. Baltim. Md. 64(1), 73–84 (2016).
Parente, D. B. et al. Is MR spectroscopy really the best MR-based method for the evaluation of fatty liver in diabetic patients in clinical practice? PLoS ONE 9(11), e112574 (2014).
Berger, D., Desai, V. & Janardhan, S. Con: Liver biopsy remains the gold standard to evaluate fibrosis in patients with nonalcoholic fatty liver disease. Clin. Liver Dis. Malden Mass. 13(4), 114–116 (2019).
Pasanta, D. et al. Magnetic resonance spectroscopy of hepatic fat from fundamental to clinical applications. Diagn. Basel 11(5), 842 (2021).
Yang, C. C. & Hsu, Y. L. A review of accelerometry-based wearable motion detectors for physical activity monitoring. Sensors 10(8), 7772–7788 (2010).
Acknowledgements
This study was conducted within the Centre of Excellence in Cardiovascular and Metabolic Research, supported by the Academy of Finland, the University of Turku, Turku University Hospital, and Åbo Akademi University. The authors thank the staff of Turku PET Centre, University of Turku, and the laboratory personnel in the Turku University Hospital Laboratory for their excellent technical assistance. The study was financially supported by Grants from Academy of Finland, Instrumentarium Science Foundation, the Finnish Cultural Foundation, the Juho Vainio Foundation, the Hospital District of Southwest Finland, the Yrjö Jahnsson Foundation, the Turku University Foundation and the Finnish Diabetes Research Foundation.
Author information
Authors and Affiliations
Contributions
I.H.A., J.K., T.V., V.S., K.L. and T.S. conception and design of the study. S.L., T.S., and T.G., acquisition of data. S.L., T.S., T.G., H.V.Y., E.L., H.S., N.H., M.S., P.K., V.S., E.S. and I.H.A. analysis and interpretation of data. SL drafted the manuscript and all authors edited and revised the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Laine, S., Sjöros, T., Garthwaite, T. et al. Relationship between liver fat content and lifestyle factors in adults with metabolic syndrome. Sci Rep 12, 17428 (2022). https://doi.org/10.1038/s41598-022-22361-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-22361-3
- Springer Nature Limited