
Abstract
Blood pressure variability is an emerging risk factor for Alzheimer’s disease in older adults, independent of average blood pressure levels. Growing evidence suggests increased blood pressure variability is linked to Alzheimer’s disease pathophysiology indexed by cerebrospinal fluid and positron emission tomography markers, but relationships with plasma Alzheimer’s disease markers have not been investigated. In this cross-sectional study of 54 community-dwelling older adults (aged 55–88, mean age 69.9 [8.2 SD]), elevated blood pressure variability over 5 min was associated with lower levels of plasma Aβ1–42 (standardized ß = − 0.36 [95% CI − 0.61, − 0.12]; p = 0.005; adjusted R2 = 0.28) and Aβ1–42: Aβ1–40 ratio (ß = − 0.49 [95% CI − 0.71, − 0.22]; p < 0.001; adjusted R2 = 0.28), and higher levels of total tau (ß = 0.27 [95% CI 0.01, 0.54]; p = 0.04; adjusted R2 = 0.19) and Ptau181:Aβ1–42 ratio (ß = 0.26 [95% CI 0.02, 0.51]; p = 0.04; adjusted R2 = 0.22). Findings suggest higher blood pressure variability is linked to plasma biomarkers of increased Alzheimer’s disease pathophysiology.
Similar content being viewed by others


Introduction
Both high and low blood pressure (BP) are associated with Alzheimer’s disease (AD) dementia risk and pathology1,2, and even small improvements in BP control may have the potential to minimize deleterious health outcomes on a world-wide scale3,4. Beyond modifying average BP levels, there has been recent interest in BP variability (BPV) as a risk factor for dementia, in part due to BP’s highly variable nature and its potential therapeutic implications5,6,7,8. Emerging evidence suggests elevated BPV over the longer term (e.g., over months to years or “visit-to-visit” BPV) and shorter term (e.g., over minutes, days) is associated with cognitive impairment and decline8, incidence and progression of dementia, including AD and vascular dementia7,9,10,11,12, cerebrovascular disease13,14,15, stroke16,17, and AD pathology18, independent of average BP levels8. Further evidence indicates these relationships may be especially pronounced in individuals at increased genetic risk for AD through the apolipoprotein (APOE) e4 allele19,20,21.
Amyloid-beta (Aβ), phosphorylated tau (Ptau), and total tau are well-studied indicators and predictors of AD-related neurodegeneration, even in individuals without cognitive impairment22, and are already being included as endpoints in clinical trials that increasingly focus on preclinical or early stages of AD23. There are several methods available to measure these hallmark AD biomarkers: cerebrospinal fluid (CSF), positron emission tomography (PET), post-mortem evaluation, and most recently, plasma from blood samples. Growing evidence suggests elevated BPV is associated with CSF21, PET20, and postmortem markers15,18 of AD pathology. However, relationships with the newer plasma markers are unknown and could represent a less invasive and lower cost method to characterize AD biomarkers. Additionally, the majority of studies on BPV and markers of AD have used visit-to-visit measures of BPV15,18,20,21, and relationships with continuous, acute BPV are understudied. The present study examined links between short-term BPV (continuously collected over a 5-min resting period) and plasma AD biomarkers in a sample of community-dwelling, independently living older adults.
Results
A total of 54 older adults were included in the present study. Clinical and demographic information about the sample is summarized in Table 1.
Elevated systolic BPV was significantly associated with lower levels of Aβ1–42 (standardized beta (ß) = − 0.36 [95% CI − 0.61, − 0.12]; p = 0.005; adjusted R2 = 0.28) (Fig. 1A), lower ratio of Aβ1–42:Aβ1–40 (ß = − 0.49 [95% CI − 0.71, − 0.22]; p < 0.001; adjusted R2 = 0.28) (Fig. 1B), higher levels of total tau (ß = 0.27 [95% CI 0.01, 0.54]; p = 0.04; adjusted R2 = 0.19) (Fig. 1C), and higher ratio of Ptau181:Aβ1–42 (ß = 0.26 [95% CI 0.02, 0.51]; p = 0.04; adjusted R2 = 0.22) (Fig. 1D), after controlling for age, sex, and APOE e4 carrier status. BPV was not significantly associated with levels of Ptau181 (ß = − 0.009 [95% CI − 0.29, 0.27]; p = 0.95; adjusted R2 = 0.11) (data not shown). Findings with diastolic BPV were similar (see Supplementary Table 1).

Elevated short-term systolic BPV is associated with plasma AD biomarkers in older adults. Scatterplots display the relationship between short-term systolic BPV and (A) Aβ1–42, (B) Aβ1–42: Aβ1–40, (C) total tau and (D) Ptau181: Aβ1–42 plasma AD biomarker levels in older adults. Lines are shaded with 95% CI. Plasma values were adjusted for age, sex, and APOE e4 carrier status. BPV blood pressure variability.
Sensitivity analyses
The majority of findings remained significant when controlling for (1) cerebrovascular disease by Fazekas score/white matter hyperintensity severity, (2) global cognitive ability by DRS-2 scaled total score, (3) years of education, (4) body mass index (BMI), and (5) antihypertensive medication use (see Supplementary Table 2). Findings remained significant after FDR correction for Aβ1–42 (p = 0.01) and Aβ1–42:Aβ1–40 ratio (p = 0.002), and were no longer significant for total tau (p = 0.05) or Ptau181:Aβ1–42 ratio (p = 0.05).
Discussion
Findings suggest elevated BPV over a period of a few minutes is associated with plasma AD biomarker levels in a sample of community-dwelling older adults, independent of average BP levels. Results are consistent with growing evidence that BPV may be a useful marker of vascular dysfunction related to AD5,6,7,8,9,10,15,19,20,21,24,25,26,27,28. Findings add to previous studies on BPV using CSF21 and PET20 AD biomarkers.
Mechanisms underlying BPV remain unclear and fluctuations in BP are common and complex29. BP levels change in the face of environmental, physical, and emotional factors and have an inverse relationship with heart rate variability30, a well-studied marker of cardiovascular and emotional health31. Just as age-related declines in heart-rate variability are thought to reflect diminished vagal tone and autonomic control31,32, BP becomes increasingly variable over time likely due to a combination of physiological factors such as baroreceptor reflex sensitivity and arterial stiffness16,29,30,33,34,35,36,37. Arteries tend to stiffen with age as a result of chronic mechanical stress on arterial walls exerted with each heartbeat38. Arterial stiffening may alter pulse wave dynamics, potentially causing a buildup or otherwise erratic flow of blood and tissue perfusion5,36,39. Disrupted blood flow may be particularly detrimental to organs with high metabolic demand like the brain35,36,38,40,41,42,43,44. The brain’s smaller cerebral arterioles and capillaries may be the most vulnerable, where the majority of nutrient transfer, nutrient influx, and waste clearance takes place across the blood–brain barrier, which could be related to the present study findings. Additionally, disrupted blood flow could be a harbinger of microvascular damage and a large body of evidence suggests BPV is associated with cerebrovascular disease burden on neuroimaging13,14,45 and postmortem evaluation15,18.
Other evidence indicates BPV may be related to endothelial dysfunction27,46, which could underlie the findings with Ptau in the current study. Specifically, a recent rodent study found that loss of nitic oxide due to high dietary salt intake leads to changes in neuronal enzymatic function that promote tau phosphorylation47. Therefore, it is possible that BPV in the present study is associated with Ptau via endothelial nitic oxide deficiency, which is in turn strongly linked with hypertension47.
Prior work on BPV and AD pathophysiology using CSF21 and PET20 found weaker, if any, links with Aβ when compared to findings with Ptau. In contrast, BPV was strongly associated with plasma markers of Aβ1–42 and Aβ1–42:Aβ1–40. It remains unclear whether the discrepancy between BPV relationships with central (e.g., CSF, PET) versus peripheral (plasma) Aβ markers may be related to differences in metabolic factors impacting central versus peripheral Aβ levels. Interestingly, Aβ is cleared in both the brain and in the kidneys, and damage to the kidneys is independently related to elevated BPV48. Additionally, chronic kidney disease may impact clearance of proteins and has been associated with elevated levels of plasma Aβ1–42 and Aβ1–40 as well as plasma Ptau181 and Ptau21749. Therefore, it is possible that plasma/peripheral Aβ may be more impacted by kidney function than central nervous system measures of Aβ, although this remains an open question for future investigation.
It is also true that prior CSF and PET studies used BPV measured over a period of months (e.g., “visit-to-visit” BPV) and the present investigation is the first to examine links between short-term BPV over a period of a few minutes and plasma markers of AD. Thus, it is possible that acute BPV reflects different physiological mechanisms than visit-to-visit measures. For example, short-term BPV is thought to reflect sympathetic nervous system overactivation and peripheral noradrenaline signaling to a greater degree than visit-to-visit measures, which may be of relevance to the relationship between BPV and Aβ levels29,37,48.
Alternatively, neurodegeneration of autonomic centers in the brain could be related to both BP fluctuations and AD pathophysiology28. The cross-sectional nature of the present study limits our ability to assess directionality or potential mechanisms and future studies are needed to elucidate ways in which BPV may be linked with increased dementia risk. Nevertheless, study findings suggest BPV may be related to plasma AD biomarkers in older adults without major neurocognitive disorder, with potential therapeutic implications. A few studies indicate differential class effects of BPV on risk for stroke50,51, independent of traditionally studied average BP levels, but more research is needed. Antihypertensive treatment decisions that consider the variability in BP levels could improve precision-medicine approaches to dementia care52,53.
A strength of the present study is the focus on blood-based AD biomarkers, a promising alternative to more invasive and costly markers of AD pathophysiology (i.e., CSF, PET) that could make their way into a wider range of clinical settings. Relatedly, BPV, whether assessed continuously over a few minutes, via ambulatory monitoring, or at routine clinical visits, is a readily available index of vascular health29 with growing links to dementia risk8,11,54. The present study used acute, continuous BPV and adds to the literature using BPV measured over longer periods. Findings were present even in this sample of community-dwelling older adults, consistent with prior reports that elevated BPV may occur before the onset of major neurocognitive dysfunction24. However, investigating relationships in study samples with more advanced disease may be helpful. There are several limitations worth noting. First, the sample size is relatively small and additional studies with larger sample sizes are needed. Relatedly, it was not possible to assess for potential antihypertensive medication class effects. Second, BP measurements and plasma samples were collected at two sites, USC and UCI, which could introduce measurement error. Additionally, BP fluctuations occur for many reasons, some of which we were not able to control for in the present study (e.g., stimulant intake, medication use, pain, perceived stress). BPV was calculated over a period of a few minutes, consistent with most prior studies on short-term BPV29. However, the study of BPV is an emerging field and there is no current gold standard of time to measure short-term BPV. Finally, the study sample was generally representative of community-dwelling older adults in the local region in terms of cerebrovascular disease55 (e.g., 59.3% had Fazekas scores ≤ 1 suggesting minimal cerebrovascular disease burden, 38.9% had Fazekas scores ≥ 2 suggesting moderate to severe cerebrovascular disease burden), education (mean 16.4 SD 2.5 years [range 9–20 years]), BMI (mean 25.9 SD 5.2), and race/ethnicity (74.1% non-Hispanic White). However, replicating these findings in larger and more heterogeneous cohorts is an important area for future research.
Conclusions
Elevated short-term BPV, independent of average BP levels, in a sample of community-dwelling older adults is related to blood-based markers of Aβ and tau-mediated neurodegeneration. BPV may be a readily accessible but understudied vascular factor associated with AD pathophysiology.
Methods
Participants
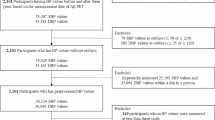
Study participants were drawn from the Vascular Senescence and Cognition Lab at the University of Southern California (USC) and University of California Irvine (UCI), an ongoing research study (n = 126) of vascular contributions to cognitive decline and dementia. Participants were recruited from the community via flyers and related research list-serves at USC and UCI. Inclusion criteria included aged 55–90 and living independently in the greater Los Angeles and Orange County areas. Participants were excluded for history of dementia, stroke, traumatic brain injury, learning disability, or other systemic or neurological disorder known to affect the central nervous system. Additionally, all research participants underwent neuropsychological testing that included the Mattis Dementia Rating Scale-2 (DRS-2)56, a widely used measure of global cognition. Remaining eligible participants were further excluded based on a DRS-2 total score ≤ 126, an established cutoff to rule out major neurocognitive impairment56. The study was approved by the Institutional Review Board at USC and UCI and all participants provided their written informed consent. All methods were performed in accordance with the relevant guidelines and regulations.
Of the total 126 participants enrolled in the ongoing study, 70 did not have valid BPV data and 2 did not have plasma AD biomarker data available. Therefore, 54 older adult participants (aged 55–88) who underwent continuous BP monitoring over a 5-min resting period and venipuncture to determine levels of plasma AD biomarkers were included in the present study.
Measures
BP assessment
BP was collected continuously using a Biopac® BP monitoring device during a 5-min resting period in which participants were in the supine position. Data were processed offline using a custom pipeline scripted in AcqKnowledge® that excluded outliers and instances of noise (e.g., signal dropout due to sensor interference), as described elsewhere25. Intraindividual BPV was calculated as variation independent of mean (VIM), a commonly used measure of BPV uncorrelated with mean BP levels7,24,26,57,58,59. In our study, BPV was not significantly correlated with average BP levels (systolic: r = 0.12, p = 0.40; diastolic: r = 0.28, p = 0.06). VIM was calculated as: VIM = standard deviation (SD)/meanx, where the power x was derived from non-linear curve fitting of BP SD against average BP using the nls package in R Project, as previously described15,24,26,57.
Plasma AD biomarkers assessment
Participants underwent venipuncture after an overnight 12-h fast, and within 1–2 h before BP monitoring. Blood samples were collected in EDTA tubes and used to determine levels of plasma AD biomarkers Aβ1–42, Aβ1–40, Ptau181, and total tau. Ptau181 samples were processed using the assay Simoa® pTau-181 Advantage V2 Kit (Quanterix). Accepted ranges for Ptau181 values were 0–424 pg/mL. Aβ1–42, Aβ1–40, and total tau samples were processed using the assay Simoa® Neurology 3-Plex A Advantage Kit (Quanterix). Accepted ranges were as follows: Aβ1–42 = 0–240 pg/mL, Aβ1–40 = 0–560 pg/mL, total tau = 0–400 pg/mL. Ratios were determined for Ptau181:Aβ1–42 and Aβ1–42:Aβ1–40.
White matter hyperintensity assessment
Nearly all participants (n = 53 out of 54) also underwent T2-fluid attenuated inversion recovery (FLAIR) MRI sequence for the evaluation of white matter lesions, as previously described25. Briefly, the following imaging parameters were used: TR = 10,000 ms; TE = 91 ms; TI = 2500 ms; slice thickness = 5.0 mm; flip angle = 150°; field of view = 220 mm. Fazekas scores60 were visually determined by the same rater, blinded to all other study measures, and used to calculate severity of white matter lesions.
Other measurements
Blood samples from venipuncture were also used to determine APOE e4 carrier status (≥ 1 e4 allele), as previously prescribed61. Genomic DNA was extracted using the PureLink Genomic DNA Mini Kit (Thermo). The isolated DNA concentration was determined using a NanoDrop One (Thermo). DNA was then stored at − 80 °C for long-term storage. Isolated DNA was first diluted to a concentration of 10 mg/μL. PCR reactions were performed in a final volume of 25 μL containing 25 ng DNA, 0.5 μM of both forward and reverse primers (forward: ACGGCTGTCCAAGGAGCTG; reverse: CCCCGGCCTGGTACACTG), and 1× SYBR Green Master Mix (Qiagen) diluted in H2O. For the amplification, a T100 Thermal Cycler (BioRad) was used with the following settings: 95 °C for 10 min; 32 cycles of 94 °C for 20 s, 64 °C for 20 s, and 72 °C for 40 s; followed by 72 °C for 3 min. 15 μL of the DNA PCR product was digested with Hhal-fast enzyme at 37 °C for 15 min. The digested PRC product was added to a 3% agarose gel in 1× borax buffer for gel electrophoresis. The gel was run at 175 V for 25 min and visualized on ChemiDoc (BioRad) with a GelRed 10,000× gel dye. Height (m) and weight (kg) were determined from study screening and used to calculate body mass index (BMI [kg/m2]). Study screening also determined self-reported antihypertensive use and participants were categorized as those taking antihypertensive medication (all classes) vs those who were not. Total DRS-262 raw scores (max score = 144) were converted to age-corrected scaled scores.
Statistical analysis
BPV and plasma AD biomarker outliers that were ± 3 SD from the mean were removed. One participant was excluded (Ptau181:Aβ1–42 was + 3 SD from the mean). Multiple linear regression was used to investigate relationships between BPV and individual plasma AD biomarkers (and their ratios). All models included the potentially confounding variables age, sex, and APOE e4 carrier status. Sensitivity analyses tested the robustness of findings by controlling for (1) Fazekas score, (2) DRS-2 scaled total score, (3) years of education, (4) BMI, and (5) antihypertensive medication use (see Supplementary Materials). These are commonly used covariates in other BPV studies8,14,25 and were entered one at a time into regression models. Systolic BPV findings are reported in the main text and diastolic findings are reported in Supplementary Materials. Multiple comparison corrections using the False Discovery Rate (FDR) method for significant findings was set at p < 0.05. All analyses were 2-sided with significance set at p < 0.05 and were carried out in R Project63.
Data availability
Data are available by request to Daniel Nation.
References
Lane, C. A. et al. Associations between blood pressure across adulthood and late-life brain structure and pathology in the neuroscience substudy of the 1946 British birth cohort (Insight 46): An epidemiological study. Lancet Neurol. 18, 942–952 (2019).
Arvanitakis, Z. et al. Late-life blood pressure association with cerebrovascular and Alzheimer disease pathology. Neurology 91, e517–e525 (2018).
Yaffe, K. Prevention of cognitive impairment with intensive systolic blood pressure control. JAMA 321, 548–549 (2019).
Barnes, D. E. & Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 10, 819–828 (2011).
Nagai, M. et al. Visit-to-visit blood pressure variability and Alzheimer’s disease: Links and risks. J. Alzheimer’s Dis. 59, 515–526 (2017).
Nagai, M., Kato, M. & Dote, K. Visit-to-visit blood pressure variability in mild cognitive impairment: A possible marker of Alzheimer’s disease in the SPRINT study? J. Clin. Hypertens. https://doi.org/10.1111/jch.14388 (2021).
de Heus, R. A. A., Olde Rikkert, M. G. M., Tully, P. J., Lawlor, B. A. & Claassen, J. A. H. R. Blood pressure variability and progression of clinical Alzheimer disease. Hypertension 74, 1172–1180 (2019).
De Heus, R. A. A. et al. Association between blood pressure variability with dementia and cognitive impairment: A systematic review and meta-analysis. Hypertension. https://doi.org/10.1161/HYPERTENSIONAHA.121.17797 (2021).
Lattanzi, S., Luzzi, S., Provinciali, L. & Silvestrini, M. Blood pressure variability predicts cognitive decline in Alzheimer’s disease patients. Neurobiol. Aging 35, 2282–2287 (2014).
Lattanzi, S. et al. Visit-to-visit blood pressure variability in Alzheimer disease. Alzheimer Dis. Assoc. Disord. 28, 347–351 (2014).
Oishi, E. et al. Day-to-day blood pressure variability and risk of dementia in a general Japanese elderly population: The Hisayama study. Circulation 136, 516–525 (2017).
Alpérovitch, A. et al. Blood pressure variability and risk of dementia in an elderly cohort, the three-city study. Alzheimer’s Dement. 10, S330–S337 (2014).
Tully, P. J. et al. Association between blood pressure variability and cerebral small-vessel disease: A systematic review and meta-analysis. J. Am. Heart Assoc. 9, e013841 (2020).
Ma, Y. et al. Blood pressure variability and cerebral small vessel disease: A systematic review and meta-analysis of population-based cohorts. Stroke 51, 82–89 (2020).
Sible, I. J., Bangen, K. J., Blanken, A. E., Ho, J. K. & Nation, D. A. Antemortem visit-to-visit blood pressure variability predicts cerebrovascular lesion burden in autopsy-confirmed Alzheimer’s disease. J. Alzheimers. Dis. 83, 65–75 (2021).
Chang, T. I. et al. Visit-to-visit office blood pressure variability and cardiovascular outcomes in SPRINT (systolic blood pressure intervention trial). Hypertension (Dallas) 70, 751–758 (2017).
Lee, K., Chang, A. Y. W. & Sung, P. Association between Blood Pressure , Blood Pressure Variability , and Post-Stroke Cognitive Impairment (2021).
Ma, Y. et al. Visit-to-visit blood pressure variability, neuropathology, and cognitive decline. Neurology 96, e2812–e2823 (2021).
Sible, I. J. & Nation, D. A. Blood pressure variability and medial temporal atrophy in apolipoprotein 4 carriers. Brain Imaging Behav. 16, 792–801 (2021).
Sible, I. J. & Nation, D. A. Visit-to-visit blood pressure variability and longitudinal tau accumulation in older adults. Hypertension (Dallas) 79, 629–637 (2022).
Sible, I. J. & Nation, D. A. Visit-to-visit blood pressure variability and CSF Alzheimer’s disease biomarkers in cognitively unimpaired and mildly impaired older adults. Neurology 98, e2446 (2022).
Jack, C. R. et al. NIA-AA research framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 14, 535–562 (2018).
Knopman, D. S., Jones, D. T. & Greicius, M. D. Failure to demonstrate efficacy of aducanumab: An analysis of the EMERGE and ENGAGE trials as reported by Biogen, December 2019. Alzheimer’s Dement. 17, 696–701 (2021).
Sible, I. J. & Nation, D. A. Long-term blood pressure variability across the clinical and biomarker spectrum of Alzheimer’s disease. J. Alzheimer’s Dis. 77, 1655–1669 (2020).
Sible, I. J. et al. Selective vulnerability of medial temporal regions to short-term blood pressure variability and cerebral hypoperfusion in older adults. Neuroimage Rep. 2, 100080 (2022).
Sible, I. J. et al. Visit-to-visit blood pressure variability and regional cerebral perfusion decline in older adults. Neurobiol. Aging 105, 57–63 (2021).
Lattanzi, S., Vernieri, F. & Silvestrini, M. Blood pressure variability and neurocognitive functioning. J. Clin. Hypertens. 20, 645–647 (2018).
Kitamura, J. et al. The insular cortex, Alzheimer Disease pathology, and their effects on blood pressure variability. Alzheimer Dis. Assoc. Disord. 34, 282–291 (2020).
Parati, G., Ochoa, J. E., Lombardi, C. & Bilo, G. Assessment and management of blood-pressure variability. Nat. Rev. Cardiol. 10, 143–155 (2013).
Baumert, M. et al. Heart rate variability, blood pressure variability, and baroreflex sensitivity in overtrained athletes. Clin. J. Sport Med. 16, 412–417 (2006).
Thayer, J. F., Åhs, F., Fredrikson, M., Sollers, J. J. & Wager, T. D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 36, 747–756 (2012).
Sturm, V. E. et al. Network architecture underlying basal autonomic outflow: Evidence from frontotemporal dementia. J. Neurosci. 38, 8943–8955 (2018).
Conway, J., Boon, N., Jones, J. V. & Sleight, P. Mechanisms concerned with blood pressure variability throughout the day. Clin. Exp. Hypertens. A7, 153–157 (1985).
Imai, Y. et al. Factors that affect blood pressure variability: A community-based study in Ohasama, Japan. Am. J. Hypertens. 10, 1281–1289 (1997).
Schillaci, G. et al. Relationship between short-term blood pressure variability and large-artery stiffness in human hypertension: Findings from 2 large databases. Hypertension 60, 369–377 (2012).
Tatasciore, A. et al. From short-term blood pressure variability to atherosclerosis: Relative roles of vascular stiffness and endothelial dysfunction. J. Clin. Hypertens. 22, 1218–1227 (2020).
Mancia, G., Di Rienzo, M., Parati, G. & Grassi, G. Sympathetic activity, blood pressure variability and end organ damage in hypertension. J. Hum. Hypertens. 11(Suppl 1), S3–S8 (1997).
Van Popele, N. M. et al. Association between arterial stiffness and atherosclerosis: The Rotterdam study. Stroke 32, 454–460 (2001).
AlGhatrif, M. & Lakatta, E. G. The conundrum of arterial stiffness, elevated blood pressure, and aging. Curr. Hypertens. Rep. 17, 12 (2015).
Vikner, T. et al. Cerebral arterial pulsatility is linked to hippocampal microvascular function and episodic memory in healthy older adults. J. Cereb. Blood Flow Metab. https://doi.org/10.1177/0271678X20980652 (2021).
Zhou, T. L. et al. Blood pressure variability, arterial stiffness, and arterial remodeling the Maastricht study. Hypertension 72, 1002–1010 (2018).
Saji, N., Toba, K. & Sakurai, T. Cerebral small vessel disease and arterial stiffness: Tsunami effect in the brain? Pulse 3, 182–189 (2016).
Winder, N. R., Reeve, E. H. & Walker, A. E. Large artery stiffness and brain health: Insights from animal models. Am. J. Physiol. Heart Circ. Physiol. 320, H424–H431 (2021).
Muhire, G. et al. Arterial stiffness due to carotid calcification disrupts cerebral blood flow regulation and leads to cognitive deficits. J. Am. Heart Assoc. 8, e011630 (2019).
Brickman, A. M. et al. Long-term blood pressure fluctuation and cerebrovascular disease in an elderly cohort. Arch. Neurol. 67, 564–569 (2010).
Eto, M. et al. Reduced endothelial vasomotor function and enhanced neointimal formation after vascular injury in a rat model of blood pressure lability. Hypertens. Res. 26, 991–998 (2003).
Faraco, G. et al. Dietary salt promotes cognitive impairment through tau phosphorylation. Nature 574, 686–690 (2019).
Bilo, G. & Parati, G. Blood pressure variability and kidney disease: Another vicious circle? J. Hypertens. 36, 1019–1021 (2018).
Mielke, M. M. et al. Performance of plasma phosphorylated tau 181 and 217 in the community. Nat. Med. https://doi.org/10.1038/s41591-022-01822-2 (2022).
Webb, A. J., Fischer, U., Mehta, Z. & Rothwell, P. M. Effects of antihypertensive-drug class on interindividual variation in blood pressure and risk of stroke: A systematic review and meta-analysis. Lancet 375, 906–915 (2010).
Rothwell, P. M. et al. Effects of β blockers and calcium-channel blockers on within-individual variability in blood pressure and risk of stroke. Lancet Neurol. 9, 469–480 (2010).
Hoshide, S. Clinical implication of visit-to-visit blood pressure variability. Hypertens. Res. 41, 993–999 (2018).
Kollias, A., Stergiou, G. S., Kyriakoulis, K. G., Bilo, G. & Parati, G. Treating visit-to-visit blood pressure variability to improve prognosis. Hypertension 70, 862–866 (2017).
Yoo, J. E. et al. Blood pressure variability and the risk of dementia: A nationwide cohort study. Hypertension 75, 982–990 (2020).
Smith, E. E. et al. Prevention of stroke in patients with silent cerebrovascular disease: A scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 48, e44–e71 (2017).
Griffiths, S., Sherman, E. M. S. & Strauss, E. Dementia Rating Scale-2. In Encyclopedia of Clinical Neuropsychology (eds Kreutzer, J. S. et al.) 810–811 (Springer, 2011).
Rothwell, P. M. et al. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 375, 895–905 (2010).
Rouch, L. et al. Visit-to-visit blood pressure variability is associated with cognitive decline and incident dementia: The SAGES cohort. Hypertension 76, 1280–1288 (2020).
Xia, Y. et al. Influence of beat-to-beat blood pressure variability on vascular elasticity in hypertensive population. Nature 7, 1–8 (2017).
Fazekas, F., Chawluk, J. B. & Alavi, A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am. J. Neuroradiol. 8, 421–426 (1987).
Kapoor, A. et al. Increased levels of circulating angiogenic cells and signaling proteins in older adults with cerebral small vessel disease. Front. Aging Neurosci. 13, 711784 (2021).
Lucas, J. A. et al. Normative data for the Mattis Dementia Rating Scale. J. Clin. Exp. Neuropsychol. 20, 536–547 (1998).
R Core Team. R: A Language and Environment for Statistical Computing (2018).
Acknowledgements
The authors would like to thank the study participants and their families. The study data collection and data analysis were supported by NIH/NIA Grants (R01AG064228, R01AG060049, P30AG066519, P01AG052350), National Science Foundation grant DGE1418060, and Alzheimer’s Association Grant AARG-17-532905.
Author information
Authors and Affiliations
Contributions
I.J.S. designed and conceptualized the study. I.J.S., B.Y., J.Y.J., J.P.M.A., A.G., A.N., S.D., A.E.B., J.K.H., A.J.M., A.K., and F.S. collected the data. I.J.S. analyzed the data. I.J.S. and D.A.N. interpreted the data. I.J.S. drafted the manuscript for intellectual content. B.Y., J.Y.J., J.P.M.A., Y.L., A.G., A.N., S.D., A.E.B., J.K.H., A.J.M., A.K., F.S., K.E.R., V.E.S., E.H., A.M., and D.A.N. revised the manuscript for intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sible, I.J., Yew, B., Jang, J.Y. et al. Blood pressure variability and plasma Alzheimer’s disease biomarkers in older adults. Sci Rep 12, 17197 (2022). https://doi.org/10.1038/s41598-022-20627-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-20627-4
- Springer Nature Limited