
Abstract
There is an ongoing debate on the implementation of the COVID-19 passport throughout Europe. We sought to build and test a feasible prevention strategy to ensure low SARS-CoV transmission risk in public events. We conducted a non-randomised controlled study. The intervention group obtained a confidential digital certificate of very low capacity for transmitting SARS-CoV-2 and attended socio-cultural events in Girona (Spain) between 1 April and 21 May 2021. The primary care services and a network of pharmacies cooperated in providing the certification. A group of non-attendees was randomly selected from pseudonymised health records as controls. We estimated the incidences of SARS-CoV-2 infection and recorded the challenges in the process. Follow-up was complete for 1351 participants, who were matched with 4050 controls. Mean age of the study population was 31.1 years, and 53% of participants were women. Incidence rates of SARS-CoV infection at 14 days in the group of attendees and non-attendees were 15.9 and 17.7 per 100,000 person-days, respectively; the difference between incidences was − 1.8 (95% CI − 22.8, 19.3). Implementation problems were minor, and 89.2% of respondents to a survey were satisfied with the process. The incidence rate of SARS-CoV-2 infection was not different in the intervention and control groups. These results are in favour of establishing a COVID-19 certificate to attend public events, and connote feasibility of implementation at a population level.
Similar content being viewed by others


Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is considered the most severe pandemic of the twenty-first century thus far. Over 190 million confirmed cases and more than four million of coronavirus disease 2019 (COVID-19)-related deaths accumulated in all continents as of 26 July 2021, according to the World Health Organization1. Such dissemination was mainly driven by the high transmissibility of this virus.
Measures to restrict mobility and social life are effective at controlling this pandemic, but have had grave consequences on the economic and social fabric2, and thus on the population’s wellbeing. Culture, sports, leisure, and catering have been the most affected sectors2. Moreover, confinement has shown an association with an increased incidence of pathologies related to mental health3,4. At the time this study was carried out, Spain was being struck by a fifth wave with a dramatic increase in the incidence of new infections that eventually reached the vulnerable population, despite vaccination coverage of 30–40% that hindered further escalation of hospitalisation rates. Later on, in July 2020, certain countries in Central Europe reinstated lockdown measures or were planning to do so. Some other areas, like Catalonia (Spain) were discussing the implementation of the EU digital COVID certificate, to allow certain social and economic activities without weakening health security. In this regard, mass-gathering events deserved special attention, because of their association with a high risk of SARS-CoV-2 dissemination5,6; this risk was particularly high in sports events and concerts7.
Previous studies indicated that mass-gathering events could be safe in the context of a COVID-19 outbreak if a comprehensive preventive intervention was implemented8,9,10. Such evidence includes a randomised trial that examined a large number of participants and had sufficient statistical power to estimate SARS-CoV-2 transmission risk9. However, these studies examined one (musical) event. Further confirmation and inclusion of various social events, different scenarios of the pandemic, and vaccinated as well as non-vaccinated people would be of interest. Even more, feasibility of implementation of these preventive measures is crucial and thus should be explored. Accordingly, we sought to analyse whether people who attended public events with a certified low risk of transmitting SARS-CoV-2 infection, through a negative result from a rapid antigenic test (up to 36 h previous to the event) or proven immunisation against SARS-CoV-2 (confirmed vaccination, or confirmed recovery from COVID-19) presented a higher rate of detected SARS-CoV-2 infections compared to a group of people who did not attend such events. We also aimed to frame such analysis into an integrated strategy that could be deployed throughout the territory.
Methods
Study design and participants
ObrirGirona was a non-randomised controlled study that compared attendees to social and cultural events (intervention group) with a matched group of non-attendees (as controls). The study involved social and cultural events held in the city of Girona (Catalonia, Spain) between 1 April and 21 May 2021. Participants could choose to have dinner at any of the five participating restaurants (on three weekends) or either of the following two concerts: La Mercè Electrònica, and a concert tribute to health professionals by Manel in La Mirona, Salt (Catalonia, Spain). Although the bar services in the concerts were outdoors, both types of events -concerts and dinner at restaurants- were indoors, we evaluated mainly indoor activities.
Invitation to participate in the group of attendees was voluntary and advertised on mass and social media. Individuals from the general population willing to enter the study had to download the free AOKpass application program (app), to create a digital certificate of very low risk of transmission (VLRT), which had to be validated at a pharmacy.
One of the following requirements was necessary to obtain the digital certificate: proof of recovery from SARS-CoV-2 infection, proof of previous vaccination, or negative antigen test. (1) A positive PCR test result for SARS CoV-2 (from three months before up to 15 days prior to the index date) confirmed previous SARS-CoV-2 infection. This result had to be certified by an authorised clinical analysis laboratory and granted the validity of the digital VLRT pass for three months, starting from the date of analysis; (2) proof of vaccination status against SARS-CoV-2 required a standardised form from the Catalan Institute of Health (ICS-Institut Català de la Salut). This document certified six months of immunisation. If neither of these two documents could be provided (3) a negative antigen test for SARS-CoV-19 had to be performed at the pharmacy, which guaranteed validity of the digital VLRT pass for 36 h.
Exclusion criteria applied to people with COVID-19 symptoms or with a positive PCR test result within 15 days before the event. An anamnesis inquired about possible COVID-19 symptoms, and addressed the need for quarantine, which was mandatory when there had been previous contact with a person with SARS-CoV-2 infection. Participants also had to fill in and sign a responsibility form where they stated lack of COVID-19 symptoms, or recent contact with a person with SARS-CoV-2 infection. If a person had symptoms (fever, persistent cough, shortness of breath, recent anosmia/ageusia, or two of the following: sore throat, runny nose, fatigue, muscle aches, headache, stomachache with vomiting or diarrhoea) no further testing was performed and that person was directed to the healthcare services and followed the corresponding SARS-CoV-2 protocols in force at the time.
Participants received information on the cost of obtaining the VLRT pass, which included the performance of the test when needed and the creation of a certificate (the cost of a test plus the certificate was 8.5€; the cost of the certificate [of vaccination or laboratory analysis] was 2.5€).
The control group of non-attendees was a random selection from the clinical health records of people assigned to the public primary care services who had not attended the event. Data from this sample was pseudonymised and matched with participants in the intervention group by age, sex, postal code, history of previous SARS-CoV-2 infection, vaccination status, and event date.
We calculated the sample size to estimate the difference between two independent proportions using the ARCSIN approximation. Considering an alpha risk of 0.05 and a beta risk < 0.2 in a bilateral contrast, we should require 1260 people in the first group (of attendees) and 3780 in the second (of non-attendees), to detect a statistically significant difference between two proportions, which were expected to be 0.012 in the first group and 0.0030 in the second group. We estimated a 0% of follow-up loss rate. The matching ratio was 1:3. For this calculation, we considered the cumulated incidence observed before the beginning of the study: 300 per 100,000 person-years11 (Supplementary Fig. S1).
The index date was that of the event in both the group of attendees and in the matched group of non-attendees. After data pseudonymisation, follow-up was carried out, through electronic health records from the ICS, and lasted 14 days from index date. No project-specific testing was performed during follow-up.
Variables
We recorded the following variables from the intervention group of attendees: date of birth, sex, symptoms compatible with COVID-19—exclusion criterion—(yes/no), derivation to a COVID-19 primary care manager (yes/no), test type (if performed), test result. We also recorded whether participants presented proof of SARS-CoV-2 vaccination, or a certified report with a PCR test result.
The pseudonymised data from participants in the control group of non-attendees comprised the following variables: age, sex, postal code, history of previous SARS-CoV-2 infection (yes/no), and SARS-CoV-2 vaccination status (vaccinated/unvaccinated).
Data downloading was carried out by the Quality and Safety Unit from the Clinical Management Area of the Primary Care Directorate in ICS Girona. This Unit performed the data pseudonymisation before delivery to the research team, who conducted the analysis.
Outcomes
The main outcome was incident SARS-CoV-2 infection, defined by a positive confirmatory test (rapid antigen test, or PCR) in the first 14 days after the social event. Additionally, we collected information on possible logistical and implementation problems during the process of generating the secure pass for the intervention group (attendees). We also collected the opinion and satisfaction level of a subsample of 149 individuals within the first 468 participants from the intervention group. Three questions about global satisfaction, economic cost, and intention of recommending the process were asked to these people. The level of agreement was classified according to a Likert scale. Respondents could select an answer from the following: totally agree, agree, agree a little, disagree a little, disagree, and totally disagree.
Procedures and circuits
The app AOKpass (developed in partnership with the International Chamber of Commerce—ICC, International SOS, and Société Générale de Surveillance—SGS) is a secure, simple, and unequivocal pass to certify that a person has a VLRT in an access control point (managed by non-healthcare professional). This app ensures data privacy and total control over the use of one’s personal information. For each validated user, the app only sends a hash with the data emitted from a mobile phone; user identification is not possible. Personal data of users who acted as certificate generators were not saved, only their username and password.
Users who wished to attend one of the proposed events within the project went to one of the pharmacy offices across Girona, Salt, Sarrià, and Sant Julià de Ramis (Catalonia, Spain) that volunteered to participate in this study. These pharmacies allocated an individual ventilated extraction space and procured all the mandatory protective and waste collection equipment. The entire procedure was coordinated and monitored by the Official College of Pharmacists of Girona (COFGi). The antigen test used in this study was SARS-CoV-2 Rapid Antigen Test12, which has high sensitivity and specificity13, and analyses nasal swabs -instead of the nasopharyngeal ones- facilitating implementation. Training on all the procedures was carried out by pharmacists and clinical analysts from the COFGi and technical staff from the Blockchain Centre of Catalonia. This program was coordinated by the primary healthcare and the COVID-19 managers in Girona, for referral of positive or suspected cases and later monitoring during the 14 follow-up days.
In the context of the study, access control to the events included reading the AOK pass to certify VLRT, participants had to wear FFP2 masks that could only be removed at the time of drinking or eating in the allocated spaces, no minimum distance was required when attending the events, and the staff working at the events were required to have a negative antigen test for SARS-CoV-2 from the previous 36 hours.
Statistical analysis
Normal continuous quantitative variables were described with the mean and standard deviation, and qualitative variables with percentages. The comparison of participants’ characteristics between groups was performed using student’s t-test and χ2 test for continuous and categorical variables, respectively. We estimated the incidences of SARS-CoV-2 infection at seven and 14 days; and the corresponding 95% confidence intervals (CI) using the Poisson approximation. The comparison of the incidences between groups was carried out using Poisson model. The survival analysis was graphed using Kaplan-Meier curves.
Ethical considerations and data confidentiality
This study has been approved by the Clinical Research Ethics Committee of the IDIAP Jordi Gol, including the waiver of obtaining informed consent for the pseudonymised data from the control group of non-attendees according to current regulations (ethical approval document 21/080-PCV). Informed consent was not required for participants in the group of non-attendees because the information obtained from the clinical health records was pseudonymised. Confidentiality was ensured by a coding system that blocked availability of any possible identifier to the researchers. Participants in the group of attendees received thorough information on the project and were asked to sign an informed consent and a statement of responsibility to participate in it, and provide permission to use their data within the context of the project.
This project was carried out in keeping with The World Medical Association’s Declaration of Helsinki, the Convention on Human Rights and Biomedicine regarding biomedical research (2005), and subsequent updates (Declaration of Helsinki, Fortaleza, Brazil, October 2013), as well as the Regulations 2016/679 of the European Parliament, the Council of 27 April 2017 on Data Protection (RGPD), and the applicable national regulations.
Results
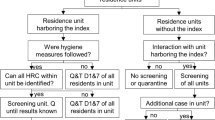
During the study period, 1699 people tried to obtain the VLRT certificate at one of the participating pharmacies. Three of these individuals presented symptoms compatible with COVID-19 and were initially excluded (two of them had a posterior positive test, and one a negative test). Of the remaining ones, 31 (1.8%) had suffered COVID-19 confirmed with a positive PCR test (from three months before up to 15 days prior to the index date), 205 (12.1%) had been vaccinated, and the remaining 1460 underwent antigen testing. Five people within the latter group (undergoing antigen testing) tested positive. These five asymptomatic people, added to the above-mentioned two, who tested positive and had symptoms, amounted to seven individuals with a positive test result. Very low risk of transmission certificates were supplied to 1691 people. Of these, 1384 attended one of the events within the ObrirGirona project. The 14-day follow-up was attained for 1351 participants (97.6%), who were finally included in the analysis (Fig. 1). Even though three random controls (non-attendees) were selected for each person who attended an event, three of the attendees could only be matched to two controls (non-attendees); thus, the final numbers of analysed participants were 1351 people who attended an event (intervention group) and 4050 non-attendees (controls).

Flowchart of participation in the study.
Table 1 compares the participants’ characteristics of both groups and counts the number of attendees per event type. The mean age of the study population was 31.1 years, and 53% of participants were women. Eleven per cent of the attendees reported that they had suffered from COVID-19 at some time since the beginning of the pandemic. Thirteen per cent of attendees had been vaccinated. Participants in both groups were similar regarding these characteristics, as expected when matching. The majority of participants in the intervention group attended the concerts: 86.4% of them; whereas 13.6% of attendees went for dinner at the restaurants.
Incidence of COVID19 during follow-up
The estimated incidences by group at seven and 14 days of follow-up are shown in Table 2. During the first seven days of follow-up, the incidence rate was lower in the intervention group (attendees), even though the difference between groups was not statistically significant.
During 14 days of follow-up, the incidence rate in the intervention group was 15.9 per 100,000 person-days, and the cumulative incidence was 222.1 per 100,000 persons; the corresponding figures in the group of non-attendees were 17.7 and 246.9, respectively. These differences were not statistically significant (as in the analysis with seven days of follow-up). The Kaplan–Meier survival curves are shown in Fig. 2.

Kaplan–Meier survival curves by group during 14 days of follow-up (n = 5401).
Report of the logistical and implementation challenges
Minor implementation problems arose only in 10% of cases, mainly because the users had not downloaded the app, or did not present adequate identification. Technical errors related to the app occurred in less than 0.5% of cases. All problems were readily solved.
Satisfaction survey
A subsample of 148 people participated in a satisfaction questionnaire. Regarding overall satisfaction, 89.2% of respondents agreed or totally agreed with the process of obtaining the digital pass. As for the economic cost, 60.8% of respondents agreed or totally agreed that the cost was reasonable. Only 9.5% disagreed or totally disagreed. Finally, 83.1% of respondents agreed or totally agreed when asked if they would recommend following this process to a friend.
Discussion
The results of our study showed that those people who attended public events with a certified digital pass did not have a higher SARS-CoV-2 infectious rate than a group that did not attend such events. The digital pass certified a negative antigen test result, or immunity against SARS-Cov-2 (confirmed vaccination or recovery from COVID-19). This risk screening strategy was grounded on the coordination of the primary care services and a community pharmacy network to ensure its feasibility and was well received by the participants in the events. Allowing safe social interactions not only would help alleviate the mental burden that lingering social restrictions inflict on the population, but it would also contribute to keeping the local economies open, and to the continuity of the cultural, sports, and catering sectors.
The observed cumulative incidences were similar to those in our area at the time of the study, which ranged from 103 to 362 per 100,000 persons (at 14 days) and had a median value of 309, supporting the validity of our results. Supplementary Fig. S1 shows the incidence of SARS-CoV-2 in our area during the study period14. Our findings also concur with previous reports. The PRIMACOV study8 included 1047 participants, aged 18–59 years, with no COVID-19 diagnosis in the 14 days previous to a concert held in Barcelona (Catalonia), and a negative antigen test result before entering the venue. Of those, 465 were randomly selected to go to the concert and 495 did not attend and comprised the control group. Both groups completed the follow-up visits. Results showed that none of the participants who went to the concert had a positive antigen test for SARS-CoV-2 during follow-up8. Conclusions of an observational subsequent study that included 5000 individuals, to test the preventive measures in a larger population, confirmed the lack of remarkable transmission events during a concert10. A very large randomised trial (SPRING) carried out in France aimed to compare nearly 4500 people assigned to attend an indoor live concert with over 2000 assigned not to attend it, and also found no increase in the SARS-CoV-2 transmission. In this trial, all participants underwent a screening test within the 3 days previous to the event, and around 7% of them had been vaccinated with two doses9. In our study, we used vaccination status and history of previous COVID-19, in addition to rapid antigen testing, to certify immunity against SARS-CoV-2, aiming to examine the available tools.
Rapid antigen tests have a high sensitivity to detect SARS-CoV-2, up to 98.6% when the viral load is high enough to suppose likely infectiousness (which could generally be considered under a cycle threshold of 30 if a PCR was performed)14,15,16. Rapid antigen tests in our study were not necessarily performed right before entering a concert, as in the PRIMACOV, but had a validity of up to 36 h before any event, because we were also aiming to examine the feasibility of implementation at a large scale. This was in line with the SPRING trial, where participants were tested within the 3 days before the event. Further studies to determine the maximum acceptable gap of time from the performance of rapid antigen test until the event would be of interest.
Only a minority of participants presented a certification of vaccination status as proof of immunisation in the digital pass. However, percentages shifted, later on, towards the predominance of fully vaccinated people. The overall effectiveness for the prevention of infection has been estimated at 91% for fully vaccinated people17. Vaccination not only poses a lower risk of SARS-CoV-2 infection, but also attenuates the effects of breakthrough infections17,18,19, which is of paramount importance within the context of a wave.
History of recovery from SARS-CoV-2 infection was the third condition that justified a low risk of SARS-CoV-2 transmission20,21,22. A recent review reported a very low probability of detecting replication-competent virus from samples of people with SARS-CoV-2 infection in cultured cells after 8–15 days from symptom onset20. Within this range, the duration of infectivity was longer in samples from individuals with a more severe illness20. Epidemiological data also reflected these results23.
Another novelty in our study is the type of activities considered to evaluate SARS-CoV-2 transmission. Additional to concerts or other mass-gathering events where participants used the mask, we also included dinners at restaurants, a context in which people are at a relatively close distance without covering their faces while eating. At the time of the study, mask and security distance was mandatory indoors and outdoors, along with adequate ventilation of indoor public spaces, access control of attendees to cultural and leisure activities, use of hand sanitiser at the entrance of indoor public spaces, social distance whenever possible, and control of mobility indoors, amongst a list of preventive measures and indications detailed in Supplementary Table S124,25.
Finally, the most relevant addition concerned the organisational structure. The PRIMACOV study reported the difficulty of testing thousands of people within a few hours before the concert8. Striving to address this question, we considered the type of sample and participation of a pharmacy network. The rapid antigen tests were performed from a nasal swab, which is easier to obtain than the nasopharyngeal swab, and thus facilitated supervised self-administration, which in turn allowed testing for a higher number of individuals in a given period of time. Rapid antigen tests from a self-administered nasal swab under professional supervision have similar sensitivity to those from a nasopharyngeal swab26,27. On the other hand, the adequacy of the spaces where the COVID-19 VLRT certificate could be obtained is important. These spaces needed to meet certain quality and safety requirements, regarding logistics, training and protection of the staff involved, and protection of all participants. Pharmacies are accessible premises spread throughout the territory and thus good candidates to perform the necessary tests and checks to obtain a digital pass, provided they comply with the appropriate quality and safety measures. Participating pharmacies had to allocate a specific space for this purpose that was isolated, separated from the other customer service areas, and with adequate ventilation. Such space was duly cleaned after each sample was taken.
Another key point of the organisation was the technology to frame the certification process in a safe and efficient manner. We used the AOKpass digital app, (developed by the ICC, International SOS, and SGS), to hold a safe, easy-to-use pass that certified a VLRT condition in an access control that could be performed by a non-healthcare professional. The VLRT condition implied vaccination against SARS-CoV-2, recovery from COVID-19, or a negative result in an antigen test. This type of certification would be analogous, or could even be adapted for its use as a certification to travel throughout Europe.
The following limitations should be considered in our study. First, the group of attendees and non-attendees could be different regarding certain variables omitted in the matching. However, we considered the main determinants of SARS-CoV-2 infection and used methodological matching28,29. Second, Howthorne bias is intrinsic to trials: participants are aware that they are part of an experiment and thus certain modification in their behaviour is bound to occur, which has to be considered when applying the results beyond the study context. Finally, compliance with safety measurements might be lower in participants lost to follow-up, which could partly bias the results.
Lifting of restrictions on social contacts resulted in an increase in cases associated to mass gathering events, especially in non-vaccinated populations. Increasing vaccination rates contributed to reducing the severity of infected people, but the more vulnerable were eventually also affected -including those with contraindication for vaccination- due to the high transmission capacity of this virus, which could be noticed in the number of hospitalisations and severe cases30.
We examined the feasibility of the implementation of a certificate that could be obtained through a process that involves the coordination of the primary care services and a network of already-existing pharmacy offices adapted for such purpose. Our study shows that the reopening of social life could be done in a controlled way, using an app to certify the minimised risk of SARS-CoV-2 transmission. Such an approach could benefit the wellbeing of the population, particularly regarding mental health, and help socio-economic sectors like culture, sports, and catering.
Conclusion
Attendance to events that involved social interaction with a certified digital pass was not associated with an increased rate of SARS-CoV-2 infection compared to a control group who did not attend these events. Such certifications stated a negative result in an antigen test or immunity against SARS-CoV-2, through vaccination or recovery from COVID-19. Logistical problems during the process of obtaining the certificate were very infrequent and easy to solve. The users’ overall opinion on the accreditation process was satisfactory or very satisfactory for the vast majority of participants. The implementation of the presented approach is feasible and could allow socio-economic spaces and activities to remain open.
Data availability
The datasets analysed in this study are not publicly available due to legal reasons related to data privacy protection but are available from the corresponding author on reasonable request.
References
World Health Organization. Weekly Operational Update on COVID-19. 1–10.
Moreno-Luna, L., Robina-Ramírez, R., Sánchez, M.S.-O. & Castro-Serrano, J. Tourism and sustainability in times of COVID-19: The case of Spain. Int. J. Environ. Res. Public Health 18, 1–22 (2021).
Gerlach, L. B. et al. The COVID-19 pandemic and mental health symptoms among US adults. J. Gen. Intern. Med. https://doi.org/10.1007/s11606-021-07046-3 (2021).
Garre-Olmo, J. et al. Changes in lifestyle resulting from confinement due to COVID-19 and depressive symptomatology: A cross-sectional a population-based study. Compr. Psychiatry 104, 152214 (2021).
Althouse, B. M. et al. Superspreading events in the transmission dynamics of SARS-CoV-2: Opportunities for interventions and control. PLOS Biol. 18, e3000897 (2020).
DC, A. et al. Clustering and superspreading potential of SARS-CoV-2 infections in Hong Kong. Nat. Med. 26, 1714–1719 (2020).
Centers for Disease Control and Prevention. Considerations for Events and Gatherings|CDC.
Revollo, B. et al. Same-day SARS-CoV-2 antigen test screening in an indoor mass-gathering live music event: A randomised controlled trial. Lancet. Infect. Dis. 21, 1365–1372 (2021).
Delaugerre, C. et al. Prevention of SARS-CoV-2 transmission during a large, live, indoor gathering (SPRING): A non-inferiority, randomised, controlled trial. Lancet. Infect. Dis. 22, 341–348 (2022).
Llibre, J. M., Videla, S., Clotet, B. & Revollo, B. Screening for sars-cov-2 antigen before a live indoor music concert: An observational study. Ann. Intern. Med. 174, 1487–1488 (2021).
Departament de Salut Generalitat de Catalunya. Dades COVID SETMANAL. https://dadescovid.cat/setmanal.
Roche Diagnostics. SARS-CoV-2 Rapid Antigen Test. https://diagnostics.roche.com/global/en/products/params/sars-cov-2-rapid-antigen-test.html#productSpecs.
Roche. Roche to launch SARS-CoV-2 Rapid Antigen Test in countries accepting CE mark, allowing fast triage decisions at point of care. https://www.roche.com/media/releases/med-cor-2020-09-01b.htm.
Gniazdowski, V. et al. Repeat COVID-19 molecular testing: Correlation of SARS-CoV-2 culture with molecular assays and cycle thresholds. Clin. Infect. Dis. 383, 494–496 (2020).
Guglielmi, G. Rapid coronavirus tests: A guide for the perplexed. Nature 590, 202–205 (2021).
Mina, M. J., Peto, T. E., García-Fiñana, M., Semple, M. G. & Buchan, I. E. Clarifying the evidence on SARS-CoV-2 antigen rapid tests in public health responses to COVID-19. Lancet 397, 1425–1427 (2021).
Thompson, M. G. et al. Prevention and attenuation of Covid-19 with the BNT162b2 and mRNA-1273 Vaccines. N. Engl. J. Med. NEJMoa2107058 (2021). https://doi.org/10.1056/NEJMOA2107058.
Baden, L. R. et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 384, 403–416 (2021).
Polack, F. P. et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 383, 2603–2615 (2020).
Rhee, C., Kanjilal, S., Baker, M. & Klompas, M. Duration of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infectivity: When is it safe to discontinue isolation?. Clin. Infect. Dis. 72, 1467–1474 (2021).
Mack, C. D. et al. SARS-CoV-2 transmission risk among national basketball association players, staff, and vendors exposed to individuals with positive test results after COVID-19 recovery during the 2020 regular and postseason. JAMA Intern. Med. 181, 960–966 (2021).
Yang, C. et al. Viral RNA level, serum antibody responses, and transmission risk in recovered COVID-19 patients with recurrent positive SARS-CoV-2 RNA test results: a population-based observational cohort study. Emerg. Microbes Infect. 9, 2368–2378 (2020).
Cheng, H.-Y. et al. Contact tracing assessment of COVID-19 transmission dynamics in Taiwan and risk at different exposure periods before and after symptom onset. JAMA Intern. Med. 180, 1156 (2020).
Departament de Salut Generalitat de Catalunya. RESOLUCIÓ SLT/845/2021, de 26 de març. DOGC. https://dogc.gencat.cat/ca/document-del-dogc/?documentId=896691 (2021).
Departament de Salut Generalitat de Catalunya. RESOLUCIÓ SLT/1088/2021, de 16 d’abril. DOGC. https://dogc.gencat.cat/ca/document-del-dogc/?documentId=896691 (2021).
Klein, J. A. F. et al. Head-to-head performance comparison of self-collected nasal versus professional-collected nasopharyngeal swab for a WHO-listed SARS-CoV-2 antigen-detecting rapid diagnostic test. Med. Microbiol. Immunol. 210, 181–186 (2021).
Lindner, A. K. et al. Head-to-head comparison of SARS-CoV-2 antigen-detecting rapid test with self-collected nasal swab versus professional-collected nasopharyngeal swab. Eur. Respir. J. 57, (2021).
Cousens, S. et al. Alternatives to randomisation in the evaluation of public-health interventions: Statistical analysis and causal inference. J. Epidemiol. Community Health 65, 576–581 (2011).
Bonell, C. P. et al. Alternatives to randomisation in the evaluation of public health interventions: Design challenges and solutions. J. Epidemiol. Community Health 65, 582–587 (2011).
Salut/COVID Data. dades-covid_Salut. https://dadescovid.cat/?lang=eng.
Acknowledgements
We acknowledge the financial support from the European Union ERDF funds -Network for Prevention and Health Promotion in Primary Care, RedIAPP- (grant number RD16/0007/0004) and the Agency for Management of University and Research Grants -AGAUR- (grant number 2017 SGR 1146).Marc Comas-Cufí is a Serra Húnter Fellow.
Author information
Authors and Affiliations
Contributions
R.R., R.N.A., A.P.e., L.A., and Q.S. conceived the project and designed the study. L.A.C., A.P.e., L.A., S.d.C., A.d.A., E.B., A.A., and R.N.A. contributed to the design and organisation of the work. Q.S., S.C., R.M.L., A.P., and M.G.G., were in charge of data collection and management. J.B. and M.C.C. undertook the statistical analyses. R.R. and L.A.C. wrote the initial draft. R.R. and R.N.A. supervised the project. All authors interpreted the data and contributed to the discussion providing important intellectual content, revised the manuscript and approved the final version, and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ramos, R., Alves-Cabratosa, L., Blanch, J. et al. SARS-CoV-2 transmission risk screening for safer social events: a non-randomised controlled study. Sci Rep 12, 12794 (2022). https://doi.org/10.1038/s41598-022-16905-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-16905-w
- Springer Nature Limited