
Abstract
A range of self-report questionnaires were developed to quantify one’s risk-taking (RT) tendency. Exploring people’s perceived risk level associated with negative risk behaviors is essential to develop a better understanding and intervention policies for RT. In the present study, we proposed a 2 × 10-item scale, namely, the general risk-taking questionnaire (GRTQ), to evaluate RT tendency and risk attitude among the general population by measuring people’s engagement in and perceptions toward 10 commonly known risky behaviors. A total of 2984 adults residing in 10 prefectures in Japan (age range = 20–59, 53.12% female) provided valid responses to an online survey. Apart from the factor analysis procedures, multivariate negative binomial regression models have been applied to investigate the relationship between RT engagement and perception. We obtained two identical factors, namely, personal risk and relational risk, for both scales of the GRTQ. Increased levels of RT engagement were found in younger, male, nonmarried, nonparent and urban respondents. Despite an overall negative correlation between RT engagement and perception, our model revealed a weaker linkage in the younger population for relational risk behaviors. Overall, we showed evidence that the GRTQ is an easy-to-administer, valid and reliable measure of RT for future clinical research.
Similar content being viewed by others

Introduction
Behaviors that are known to have possible adverse effects on actors’ health and social and financial status are termed risk behaviors (RBs); examples of conventional RBs include illicit drug use and unsafe sexual behavior. If a person acknowledges the potential negative consequences of an act, despite being uncertain about how likely those negative outcomes would happen, still decides to engage in it, he/she is said to practice (conscious) risk-taking (RT)1,2,3,4. What causes someone to be involved in RT is an interesting research question. However, before investigating the underlying factors, it is necessary for researchers to accurately index the tendency/frequency of someone to commit RT5,6,7,8,9,10,11.
A behavior may be perceived as an RB by one individual but not the other since everyone would have their own subjective judgment on the probabilities of potential consequences and outcomes associated with an act, which is also known as risk perception12. Traditionally, researchers include behavior items that they themselves perceived as RBs in questionnaires, which were then used to assess RT tendency by measuring one’s frequency of engaging in them. These scales might not be truly indexing RT since they were based on a bold assumption that participants and researchers shared the same risk perception1,13,14,15,16. For instance, if participants engaged in a conventional (researcher perceived) RB, such as smoking, because (1) they did not perceive it to be associated with any potential negative consequences at all, then the frequencies of smoking reported would simply reflect the prevalence of a behavior rather than the true (conscious) RT. Apart from this, one’s engagement in it could be that the person (2) believes the undesirable consequence is unlikely to happen, i.e., low level of risk perceived, or (3) does perceive an act as risky but prefers the risk, i.e., a risk-seeking attitude. For these reasons, without an individual’s self-declared risk perception of a behavior, despite the success of finding consistent linkages between engagement in conventional RBs and certain personality traits17, life experiences18, mental health conditions19,20 and sociodemographic factors1, it has been challenging for researchers to interpret the findings.
Another recently challenged assumption is that individuals or groups were categorized as risk-avoiding or risk-seeking along a continuum based on their risk attitude (aka “risk preference”)21,22. Under the stable risk attitude trait assumption, if male respondents were found to have a more “risk-seeking” attitude than females, they would be expected to engage in more RT across all domains, ranging from health (e.g., alcohol abuse) to recreational (e.g., bungee jumping) or relational (e.g., breaking a promise) RT than females. Empirical findings, however, did not support this notion, with conflicting RT tendencies reported within individuals/groups across different behavioral contexts16,23,24,25,26. For example, an individual who is willing to take risks in the relational domain, such as breaking a promise, may not feel comfortable committing actions that put one’s health on risk (e.g., drug abuse). The observations of domain-specific RT highlight the importance of exploring the latent constructs/domains underlying engagement in different RB items.
Additionally, health and risk behavioral research tended to focus highly on the behaviors that were known to bring serious negative consequences (e.g., economic, psychological and health harms) at both the individual and societal levels27,28,29. Common examples include substance use (drug/alcohol)30,31, risky sexual behaviors32, or violence33. Little attention has been given to general RBs, behaviors associated with “seemingly less severe” undesirable outcomes but are commonly perceived as RBs by the general population, such as riding a bicycle with the light off at night, making a dash to train doors, or breaking a promise. These general RB items make a scale’s internal reliability less susceptible to the influence of different sample characteristics, such as age, gender, education levels and cultural backgrounds, because of the low level of specific knowledge or experience required to understand the scenario and context of the RB items. A meta-analysis revealed that the measurement accuracy of the domain-specific risk-taking (DOSPERT) scale was influenced by the different degrees of familiarity respondents had with the contents of the items/situations34. For instance, the Cronbach’s α of the questions in the social domain was lower (lower internal consistency) for students than for nonstudents—probably due to the unfamiliarity of the students with the workplace-related items. Some ethical and financial domains also contained items (e.g., “Taking some questionable deductions on your income tax return.”) that are not general situations/decisions that one has to made across lifespan, and respondents may lack the conceptual and/or experimental knowledge of the items34.
The present study seeks to investigate RT using a novel questionnaire named the general risk-taking questionnaire (GRTQ), which contains general RBs in everyday decision-making and two subscales that measure one’s risk engagement (GRTQ-E) and perception (GRTQ-P). Taking into account that people across the lifespan need to make important decisions under uncertainty and risk, a sample with a broad age range was recruited in the current study. Risk attitudes in the population could be inferred from the relationship between the frequency of engagement and the associated perceived risk. In addition, the associations between engagement in the GRTQ items and other potential explanatory variables, such as age, gender, socioeconomic and other demographic characteristics, were also explored using generalized linear models (GLMs).
Results
Mean score differences across demographic subgroups
Higher mean scores on the GRTQ-E were observed in males than in females (1.43 vs. 1.35, p < 0.001, see Table 1), younger age groups (aged 20–25: 1.50 to aged ≥ 56: 1.29, p < 0.001), and subjects living in predominantly urban areas than in those residing in intermediate areas (1.41 vs. 1.37, p = 0.001). Respondents who were married (1.36 vs. 1.43, p < 0.001) and with children (1.34 vs. 1.42, p < 0.001) reported lower GRTQ-E mean scores than their counterparts.
For the GRTQ-P, females had higher mean scores than males (2.91 vs. 2.82, p < 0.001), and respondents with children associated greater risk to GRTQ items than those who were childless (2.91 vs. 2.83, p < 0.001).
Bivariate correlations between GRTQ-E and GRTQ-P
The correlation between risk engagement and perception could represent a sample’s risk attitude, potentially highlighting how they relate risk with their corresponding behaviors. An identical 2-factor structure, namely, Personal risk and Relational risk, for both the GRTQ-E and GRTQ-P was revealed and confirmed by exploratory and confirmatory factor analysis (details on the development and validity of the GRTQ can be found in the Supplementary Information online). Bivariate correlation analysis revealed that the mean scores of the GRTQ-E were negatively correlated with those of the GRTQ-P for the full scale (τb = − 0.223) and the Personal Risk (τb = − 0.241) and Relational Risk (τb = − 0.183) subscales (see Table 2).
GLM: explanatory variables for the GRTQ-E in personal and relational RBs
Crude associations (controlling for age and gender effects only)
Mean frequency counts of the GRTQ-E Personal Risk and Relational Risk subscales and the incidence rate ratios (IRR: mean ratio of the outcome) of the crude association models on them are presented in Table 3. Three categorical variables were significantly associated with the frequency counts of the GRTQ-E Personal Risk subscale. Male gender (IRR = 1.578, p < 0.001), urban place of residence (IRR = 1.094, p < 0.01) and 12 million yen annual household income (IRR = 1.402, p < 0.01) were all linked with greater GRTQ-E Personal Risk scores. For the GRTQ-E Relational Risk subscale, male gender (IRR = 1.161, p < 0.001) was associated with greater GRTQ-E scores than female gender, and being a parent was found to be linked with a lower level of GRTQ-E (IRR = 0.896, p < 0.01).
Two-dimensional variables, namely, age and GRTQ-P ratings, were significantly negatively associated with the GRTQ-E in both the Personal Risk (age: IRR = 0.979; GRTQ-P Personal Risk: IRR = 0.872) and Relational Risk (age: IRR = 0.984; GRTQ-P Relational Risk: IRR = 0.943) subscales, all ps < 0.001. The IRRs indicated that the rate ratio for engagement in the GRTQ-E Personal Risk and Relational Risk subscales would be expected to decrease by a factor of 0.979 and 0.984 per year increase in age and decrease by a factor of 0.872 and 0.943 per score increase in the GRTQ-P, respectively.
Multivariate models (all independent variables mutually adjusted)
Multivariate negative binomial regressions revealed that all explanatory variables of the GRTQ-E discovered in crude association models for both subscales remained significant when all independent variables were mutually adjusted (see Table 4). Men had a greater GRTQ-E score on both subscales (Personal Risk: IRR = 1.339, Relational Risk: IRR = 1.178; both ps < 0.001). Living in predominantly urban areas (IRR = 1.088, p = 0.007) and with an annual household income of > 12 m yen (IRR = 1.355, p = 0.017) remained associated with a higher engagement in the GRTQ-E Personal Risk subscale. Being a parent remained linked with a lower GRTQ-E on the Relational Risk subscale (IRR = 0.916, p = 0.042). Age was significantly negatively associated with the GRTQ-E in both the Personal Risk and Relational Risk subscales (age: IRR = 0.983 and 0.983, respectively; both ps < 0.001). Notably, the GRTQ-P ratings not only remained negatively related to the GRTQ-E but also had even lower IRRs for both subscales when socioeconomic, education and demographic factors and interaction effects were controlled for (Personal Risk: IRR = 0.869, Relational Risk: IRR = 0.932; both ps < 0.001).
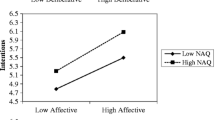
Interaction effects of the three most significant explanatory variables, namely, age, gender, and the GRTQ-P ratings, were examined. Age was found to exacerbate the negative effect of the GRTQ-P on the GRTQ-E frequency for the Relational Risk subscale (IRR = 0.997, p < 0.001). Simple slopes analysis indicated that the negative association between the GRTQ-P and GRTQ-E for the Relational Risk subscale strengthened with aging, with a steeper slope in the older group (Fig. 1; younger (age = 29.25, mean age—1 SD): B = − 0.03, z = − 4.12; middle (40.21): B = − 0.06, z = -11.09; older (51.16, mean + 1 SD): B = − 0.09, z = − 11.05; all ps < 0.001).

Follow-up simple slopes analysis for the interactions between age and the GRTQ-P Relational Risk ratings on the GRTQ-E Relational Risk scores. The shaded region depicts the 95% confidence level interval for the beta estimates.
Discussion
The present study explored RT in a sample with a broad age range from 20 to 59 years using a novel general risk-taking questionnaire—the GRTQ. Although a few efforts to measure risk attitudes or the prevalence of risk behaviors have been made in previous studies, our study is the first to address both risk perception and actual behavioral engagement with clear evidence supporting its validity. Higher mean scores on the GRTQ-E were found in groups known to engage in more RT: male1,35,36, younger27,37,38, nonmarried39,40, nonparent41, and urban areas residing42,43,44,45 compared to their counterparts.
Gender and age differences were observed in both subscales of the GRTQ-E in our GLM results, with males and younger age associated with more engagement in both personal and relational RBs. These results have been frequently reported in previous literature in which risk perception was not measured, and it was concluded that males and younger respondents were more “risk-seeking” and more prone to RT1,46,47. However, considering the negative correlations between the GRTQ-P and GRTQ-E on both subscales, they were indeed less “risk averse”. Interestingly, the significant interaction between age and the GRTQ-P further implied that the effect of perception on engagement in the Relational Risk subscale was weaker in younger adults, confirming their stronger risk tolerance level, particularly for relational RBs. Such risk context- and gender-specific effects of age on risk preference might explain why previous RT literature, with different RBs and gender ratios in samples, reported conflicting age effects on risk tolerance (negative:48,49,50, positive:51).
In addition, the above findings better explained why younger participants engaged in more RT in general. First, they associated the lowest riskiness with the RB items. The negative consequences of relational RT perceived by younger adults could be less severe (less dreadful) than older adults because of the less valuable/well-established relationships they have with friends/families/colleagues, leading to a lower risk perception52. The differences in risk perception could also be explained by the concept of affect heuristics, which suggested that negative (positive) emotion would lead to over- (under) estimation of risk53. People of younger age are likely to have fewer experiences of unexpected negative consequences that induce strong negative feelings from relational RT. As a result, they might have perceived themselves to be familiar with the potential consequences associated with it and attached fewer negative feelings to relational RT, leading to an underestimation of risk for RBs in this context. The opposite idea could be applied to older people and have resulted in negative emotions associated with relational RBs, which led to an overestimation of their risk. This might also serve as a potential explanation for the effect of age on relational risk attitudes.
Second, younger adults had the lowest tendencies to avoid both personal and relational risks, which could originate from the differences in self-efficacy. Previous research has shown that people who are very competent in decision-making tend to see more opportunities, rather than threats, in a risky choice54. Younger adults might have higher self-efficacy and therefore engage in more RT. Combined with the dual-process theory, which suggested that younger individuals and those with higher self-efficacy might have adopted a more heuristic, rather than analytic, decision-making approach, leading to a less “rational” behavioral outcome (more RT)55,56,57,58. Finally, different risk attitudes and perceptions could be driven by hormonal59, cognitive60, neurological61, sociocultural62 and genetic63 factors, which should not be overlooked.
The study is limited by its lack of respondents aged below 20 and above 59. In addition, as part of a nationwide online survey, the applicability of the GRTQ across cultures needs to be further examined. Due to the cross-sectional nature of our data, we could not differentiate whether the differences found across age groups were caused by aging, period, or cohort effects50,64,65. Further investigations applying the GRTQ in longitudinal or cohort studies would help develop a deeper understanding of the effect of age, as well as its interaction with gender, on personal and relational RT. The psychometric validity of the GRTQ could be enhanced by comparing scale scores with widely established RT-related measures, including scales such as the Zuckerman Sensation Seeking Scale66 and the Self-Efficacy Scale67, behavioral tasks such as the Balloon Analog Risk Task9 and Columbia Card Task68, genotypic data63 and hormonal measures such as testosterone and cortisol59.
An individual’s decision making in everyday risk behaviors could lead to personal and public safety issues. The present study revealed that engagement in RBs was negatively correlated with the perceived level of risk people associated with the behaviors and that such linkage was weaker in the younger population (“less risk averse”). Strategies for the prevention and intervention of RBs may include education programs that emphasize their negative outcomes in the general population, with an extra focus on the objective likelihood of adverse consequences to reduce the associated safety issues among the young populations. In addition, we demonstrate the utility of a novel RT measure, the GRTQ, through its stable factor structure and measurement invariance across gender and age groups, making it a useful tool to investigate the aging, period or cohort effects when applied to longitudinal studies and the associations between RT and neurobiological, sociocultural, cognitive, or physiological measures among patients with psychiatric disorders and the general population.
Methods
Participants
The current study is part of an anonymous and cross-sectional online study about risk engagement and perception. A total of 3417 participants were randomly sampled from the registrants of iBRIDGE, a Japanese survey research company, between September and November 2020, stratified by geographical location (10 Japanese prefectures), age range and gender. This study was approved by the Ethics Committee of the University of Tokyo (No. 20-172). All procedures performed in this study were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Online informed consent was obtained from all participants.
The analyses included 2984 adults who provided valid responses to the questionnaires. The mean age was 40.21 years (SD = 10.95), with 53.12% female, 50.47% married and 40.28% having child(ren) (see Supplementary Table S1 online). For the geographic locations, prefectures were categorized into predominantly urban, intermediate and predominantly rural areas based on the regional typology established by the Organisation for Economic Co-operation and Development69, with 46.35% and 45.88% of participants residing in predominantly urban and intermediate areas, respectively. Based on the contents of the self-indicated educational categories, education attainment was coded according to the International Standard Classification of Education (ISCED)70, resulting in a mean ISCED level of 4.57 (SD = 1.46), which was comparable to the general population in Japan stratified by age groups (p > 0.05)71.
Of these participants, 100 randomly selected respondents were readministered the online survey one month later to test the reliability of the scale, of which 99 provided valid responses.
The general risk-taking questionnaire (GRTQ)
The sources of the initial 19 items for the GRTQ are listed in Table 5. RB items that are widely experienced or familiar across broad sample characteristics were selected from the YRBS (Japanese Version, 2011)72 and the Risk-taking Behavior Scale for Undergraduates (RIBS-U)73. To examine the dimensionality of RT, the selected items cover a range of previously discovered RB domains, including social, health, traffic, and financial items. With the aim of choosing items that would be likely to be perceived as RBs by our respondents, the majority of our items were taken from the RIBS-U considering that all items, retained or not in the final scale, were nominated by Japanese undergraduates as RBs at the early development stage of the RIBS-U. The final RIBS-U is a 12-item Japanese RT engagement scale that contains two subscales (factors discovered), namely, personal and social risk, with good construct validity and test–retest reliability. Another three items, which are more general health RBs, were selected from the YRBS considered the benefits of including them on an RT scale, as discussed above, and the unchanged prevalence of them over the ten years (from 2001 to 2011) despite a general trend of decrease among most of the other YRBS items.
The GRTQ contains two types of questions for all items, Engagement (-E) and Perception (-P). Following the RIBS-U scale, the GRTQ-E scale asked participants, “How frequent do you normally engage in the following behaviors? Please indicate the most appropriate option for each of the behavioral items.” 4-Likert response options include “Never”, “Seldom”, “Some of the time” and “Most of the time” (Ranged 1–4, greater score indicates more frequent engagement of each risk item). The GRTQ-P scale began with the question "To what extent do you think that the following behaviors are risky considered the possible adverse effect on the actor's health, social and financial status, etc.? “. Response options are “Not at all risky”, “Slightly risky”, “Moderately risky”, and “Very risky”, again, scored as 1, 2, 3, and 4, respectively.
Statistical analysis
Generalized linear models to explore variables associated with GRTQ-E
Based on the obtained dimensionality, we estimated two separate generalized linear models (GLMs) for each outcome of interest (frequency counts of the GRTQ-E for items loaded onto each factor). We first examined crude associations between the independent (GRTQ-P ratings, socioeconomic and demographic variables) and outcome variables (frequency counts of the GRTQ-E for the extracted factors) while adjusting only for gender and age effects. Then, final multivariate models, which allow all potential explanatory variables to mutually adjust, were performed. To estimate the potential moderating effect of age and gender on the GRTQ-P’s impact on GRTQ-E frequency, we added the interaction terms of age × GRTQ-P, gender × GRTQ-P, and age × gender × GRTQ-P to the final multiple regression models.
Relationships between the GRTQ-E and independent variables are indicated by the incidence rate ratios (IRR: mean ratio of the outcome) from negative binomial regressions74. Negative binomial regressions were chosen because of the overdispersion (i.e., model variance exceeds the mean) observed in the response variables, which were nonnegative integer responses that approximated a Poisson distribution75,76,77,78,79. IRR and unstandardized regression coefficients of the GLM models were estimated via the “mfx” (v1.2-2)80 and “MASS” (v 7.3-53)81 packages, respectively, implemented in R. The p-values reported in GLM analysis were not multiple testing corrected.
Significant interactions revealed from the GLM were tested and interpreted by simple slopes analysis (SSA), which considers the regression of the explanatory variable on the outcome measure for low (mean − 1 SD), average (the mean), and high (mean + 1 SD) levels of the moderating variable82,83. Consequently, the nature of the interaction effect was visualized and interpreted by plotting and comparing the slopes in terms of their significance and the values and directions of the unstandardized regression coefficients (B)82. SSA was performed using the “interactions” package (v1.1.3)84 implemented in R.
Data availability
The data are available after revision approval from the ethical review board at The University of Tokyo. Please ask the corresponding author if needed.
References
Byrnes, J. P., Miller, D. C. & Schafer, W. D. Gender differences in risk taking: A meta-analysis. Psychol. Bull. 125, 367–383 (1999).
de Groot, K. & Thurik, R. Disentangling risk and uncertainty: When risk-taking measures are not about risk. Front. Psychol. 9, 2194 (2018).
Holton, G. A. Defining risk. Financ. Anal. J. 60, 19–25 (2004).
Leigh, B. C. Peril, chance, adventure: Concepts of risk, alcohol use and risky behavior in young adults. Addiction 94, 371–383 (1999).
Ahmed, S. U. nAch, risk-taking propensity, locus of control and entrepreneurship. Pers. Individ. Differ. 6, 781–782 (1985).
Arnett, J. J. Sensation seeking, aggressiveness, and adolescent reckless behavior. Pers. Individ. Differ. 20, 693–702 (1996).
Centers for Disease Control and Prevention. Youth Risk Behavior Survey Questionnaire. www.cdc.gov/yrbs (2019).
Dohmen, T., Falk, A., Huffman, D., Sunde, U. & Schupp, J. Individual risk attitudes: New evidence from a large, representative, experimentally validated survey. (2005).
Lejuez, C. W. et al. Evaluation of a behavioral measure of risk taking: The balloon analogue risk task (BART). J. Exp. Psychol. Appl. 8, 75–84 (2002).
Rivalan, M., Ahmed, S. H. & Dellu-Hagedorn, F. Risk-prone individuals prefer the wrong options on a rat version of the Iowa Gambling Task. Biol. Psychiat. 66, 743–749 (2009).
Schwartz, A. et al. Risk perception and risk attitudes in Tokyo: A report of the first administration of DOSPERT+M in Japan. Judgment and Decision Making vol. 8 https://sjdm.org/journal/13/131001/jdm131001.pdf (2013).
Tversky, A. & Kahneman, D. Advances in prospect theory: Cumulative representation of uncertainty. J. Risk Uncertain. 5, 297–323 (1992).
Arnett, J. The young and the reckless: Adolescent reckless behavior. Curr. Dir. Psychol. Sci. 4, 67–70 (1995).
Gibbons, F. X. & Gerrard, M. Predicting young adults’ health risk behavior. J. Pers. Soc. Psychol. 69, 505–517 (1995).
Stanford, M. S., Greve, K. W., Boudreaux, J. K., Mathias, C. W. & Brumbelow, J. L. Impulsiveness and risk-taking behavior: Comparison of high-school and college students using the Barratt Impulsiveness Scale. Pers. Individ. Differ. 21, 1073–1075 (1996).
Weber, E. U., Blais, A. R. & Betz, N. E. A domain-specific risk-attitude scale: Measuring risk perceptions and risk behaviors. J. Behav. Decis. Mak. 15, 263–290 (2002).
Gupta, R., Derevensky, J. L. & Ellenbogen, S. Personality characteristics and risk-taking tendencies among adolescent gamblers. Psychol. Assoc. 38, 201–213 (2006).
Anderson, L. Edgework. Symb. Interact. 29, 577–584 (2006).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR). (American Psychiatric Association, 2000).
Reddy, L. F. et al. Impulsivity and risk taking in bipolar disorder and schizophrenia. Neuropsychopharmacology 39, 456–463 (2014).
Allport, F. H. & Allport, G. W. Personality traits: Their classification and measurement. J. Abnormal Psychol. Soc. Psychol. 16, 6–40 (1921).
Eysenck, H. J. & Eysenck, M. W. Personality and Individual Differences. Personality and Individual Differences (Springer, 1985). https://doi.org/10.1007/978-1-4613-2413-3.
Blais, A. & Weber, E. U. A domain-specific risk-taking (DOSPERT) scale for adult populations. Judgm. Decis. Mak. 1, 33–47 (2006).
Nicholson, N., Soane, E., Fenton-O’Creevy, M. & Willman, P. Personality and domain-specific risk taking. J. Risk Res. 8, 157–176 (2005).
Schoemaker, P. J. H. Are risk-attitudes related across domains and response modes?. Manage. Sci. 36, 1451–1463 (1990).
Slovic, P., Fischhoff, B. & Lichtenstein, S. The Psychometric Study of Risk Perception. in Risk Evaluation and Management 3–24 (Springer US, 1986). https://doi.org/10.1007/978-1-4613-2103-3_1.
Duell, N. et al. Age patterns in risk taking across the world. J. Youth Adolesc. 47, 1052–1072 (2018).
Hansen, E. B. & Breivik, G. Sensation seeking as a predictor of positive and negative risk behaviour among adolescents. Pers. Individ. Differ. 30, 627–640 (2001).
Keough, K. A., Zimbardo, P. G. & Boyd, J. N. Who’s smoking, drinking, and using drugs? Time perspective as a predictor of substance use. Basic Appl. Soc. Psychol. 21, 149–164 (1999).
Klein, W., Geaghan, T. & MacDonald, T. Unplanned sexual activity as a consequence of alcohol use: A prospective study of risk perceptions and alcohol use among college freshmen. J. Am. Coll. Health 56, 317–323 (2007).
Widom, C. S. & Hiller-Sturmhöfel, S. Alcohol abuse as a risk factor for and consequence of child abuse. Alcohol Res. Health 25, 52–57 (2001).
Ramrakha, S., Caspi, A., Dickson, N., Moffitt, T. E. & Paul, C. Psychiatric disorders and risky sexual behaviour in young adulthood: Cross sectional study in birth cohort. BMJ 321, 263–266 (2000).
Krug, E. G., Mercy, J. A., Dahlberg, L. L. & Zwi, A. B. The world report on violence and health. Lancet 360, 1083–1088 (2002).
Shou, Y. & Olney, J. Assessing a domain-specific risk-taking construct: A meta-analysis of reliability of the DOSPERT scale. Judgm. Decis. Mak. 15, 112–134 (2020).
Charness, G. & Gneezy, U. Strong evidence for gender differences in risk taking. J. Econ. Behav. Organ. 83, 50–58 (2012).
Friedl, A., Pondorfer, A. & Schmidt, U. Gender differences in social risk taking. J. Econ. Psychol. 77, 102182 (2020).
Deakin, J., Aitken, M., Robbins, T. & Sahakian, B. J. Risk taking during decision-making in normal volunteers changes with age. J. Int. Neuropsychol. Soc. 10, 590–598 (2004).
Turner, C. & McClure, R. Age and gender differences in risk-taking behaviour as an explanation for high incidence of motor vehicle crashes as a driver in young males. Inj. Control Saf. Promot. 10, 123–130 (2003).
Whitlock, G., Norton, R., Clark, T., Jackson, R. & MacMahon, S. Motor vehicle driver injury and marital status: A cohort study with prospective and retrospective driver injuries. Inj. Prev. 10, 33–36 (2004).
Wyke, S. & Ford, G. Competing explanations for associations between marital status and health. Soc. Sci. Med. 34, 523–532 (1992).
Görlitz, K. & Tamm, M. Parenthood, risk attitudes and risky behavior. J. Econ. Psychol. 79, 102189 (2020).
Dodoo, F.N.-A., Zulu, E. M. & Ezeh, A. C. Urban–rural differences in the socioeconomic deprivation–Sexual behavior link in Kenya. Soc. Sci. Med. 64, 1019–1031 (2007).
Flisher, A. J. & Chalton, D. O. Urbanisation and adolescent risk behaviour. S. Afr. Med. J. 91, 243–249 (2001).
Strebel, P., Kuhn, L. & Yach, D. Determinants of cigarette smoking in the black township population of Cape Town. J. Epidemiol. Commun. Health 43, 209–213 (1989).
Steyn, N. P., Senekal, M., Brtis, S. & Nel, J. Urban and rural differences in dietary intake, weight status and nutrition knowledge of black female students. Asia Pac. J. Clin. Nutr. 9, 53–59 (2000).
Bener, A. et al. Gender and age differences in risk taking behaviour in road traffic crashes. Adv. Transp. Stud. Int. J. Sect. B 31, 53 (2013).
Miller, T. R., Spicer, R. S. & Lestina, D. C. Who is driving when unrestrained children and teenagers are hurt?. Accid. Anal. Prev. 30, 839–849 (1998).
Morin, R. A. & Suarez, A. F. Risk aversion revisited. J. Financ. 38, 1201–1216 (1983).
Yao, R., Hanna, S. D. & Lindamood, S. Changes in financial risk tolerance, 1983–2001. Financ. Serv. Rev. 13, 249–266 (2004).
Yao, R., Sharpe, D. L. & Wang, F. Decomposing the age effect on risk tolerance. J. Socio-Econ. 40, 879–887 (2011).
Guiso, L., Jappelli, T. & Terlizzese, D. Income risk, borrowing constraints, and portfolio choice. Am. Econ. Rev. 86, 158–172 (1996).
Beyth-Marom, R., Austin, L., Fischhoff, B., Palmgren, C. & Jacobs-Quadrel, M. Perceived consequences of risky behaviors: Adults and adolescents. Dev. Psychol. 29, 549–563 (1993).
Wang, M., Keller, C. & Siegrist, M. The less you know, the more you are afraid of-a survey on risk perceptions of investment products. J. Behav. Finance 12, 9–19 (2011).
Krueger, N. & Dickson, P. R. How believing in ourselves increases risk taking: Perceived self-efficacy and opportunity recognition. Decis. Sci. 25, 385–400 (1994).
Boyer, T. W. The development of risk-taking: A multi-perspective review. Dev. Rev. 26, 291–345 (2006).
Gerrard, M., Gibbons, F. X., Houlihan, A. E., Stock, M. L. & Pomery, E. A. A dual-process approach to health risk decision making: The prototype willingness model. Dev. Rev. 28, 29–61 (2008).
Sloman, S. A. The empirical case for two systems of reasoning. Psychol. Bull. 119, 3–22 (1996).
Stanovich, K. E. The Robot’s Rebellion: Finding Meaning in the Age of Darwin. The Robot’s Rebellion (University of Chicago Press, 2004). https://doi.org/10.7208/chicago/9780226771199.001.0001.
Mehta, P. H., Welker, K. M., Zilioli, S. & Carré, J. M. Testosterone and cortisol jointly modulate risk-taking. Psychoneuroendocrinology 56, 88–99 (2015).
Schonberg, T., Fox, C. R. & Poldrack, R. A. Mind the gap: Bridging economic and naturalistic risk-taking with cognitive neuroscience. Trends Cogn. Sci. 15, 11–19 (2011).
Shulman, E. P. et al. The dual systems model: Review, reappraisal, and reaffirmation. Dev. Cogn. Neurosci. 17, 103–117 (2016).
Zinn, J. O. Towards a better understanding of risk-taking: Key concepts, dimensions and perspectives. Health Risk Soc. 17, 99–114 (2015).
Strawbridge, R. J. et al. Genome-wide analysis of self-reported risk-taking behaviour and cross-disorder genetic correlations in the UK Biobank cohort. Transl. Psychiatry 8, 39 (2018).
Bossaerts, P. & Murawski, C. Decision neuroscience: Why we become more cautious with age. Curr. Biol. 26, R495–R497 (2016).
Fienberg, S. E. & Mason, W. M. Specification and implementation of age, period and cohort models. Cohort Anal. Soc. Res. https://doi.org/10.1007/978-1-4613-8536-3_3 (1985).
Zuckerman, M. Dimensions of sensation seeking. J. Consult. Clin. Psychol. 36, 45–52 (1971).
Sherer, M. et al. The self-efficacy scale: Construction and validation. Psychol. Rep. 51, 663–671 (1982).
Figner, B., Mackinlay, R. J., Wilkening, F. & Weber, E. U. Affective and deliberative processes in risky choice: Age differences in risk taking in the columbia card task. J. Exp. Psychol. Learn. Mem. Cogn. 35, 709–730 (2009).
OECD. OECD Territorial Reviews: Japan 2016. (2016). https://doi.org/10.1787/9789264250543-en.
International Standard Classification of Education (ISCED) 2011. International Standard Classification of Education (ISCED) 2011 (UNESCO Institute for Statistics, 2012). https://doi.org/10.15220/978-92-9189-123-8-en.
Statistics Bureau of Japan. The 2010 Population Census of Japan. https://www.e-stat.go.jp/en (2014).
Nozu, Y. Japan Youth Risk Behavior Survey (JYRBS 2011)-Tsukuba Health Education (THE) Study. https://www.yumpu.com/en/document/read/52616061/japan-youth-risk-behavior-survey-jyrbs-2011 (2012).
Oshio, A. Development and validation of a Risk-taking Behavior Scale for Undergraduates (RIBS-U). Bull. Grad. School Educ. Hum. Dev. Nagoya Univ. (Psychol. Hum. Dev. Sci.) 48, 257–265 (2001).
Piza, E. L. Using Poisson and Negative Binomial Regression Models to Measure the Influence of Risk on Crime Incident Counts. (2012).
Cox, D. R. Some remarks on overdispersion. Biometrika 70, 269–274 (1983).
Gardner, W., Mulvey, E. P. & Shaw, E. C. Regression analyses of counts and rates: Poisson, overdispersed poisson, and negative binomial models. Psychol. Bull. 118, 392–404 (1995).
Lawless, J. F. Regression methods for poisson process data. J. Am. Stat. Assoc. 82, 808–815 (1987).
Long, J. S. Regression Models for Categorical and Limited Dependent Variables. Regression Models for Categorical and Limited Dependent Variables (Sage Publications, 1997).
Walters, G. D., Frederick, A. A. & Schlauch, C. Postdicting arrests for proactive and reactive aggression with the PICTS proactive and reactive composite scales. J. Interpers. Violence 22, 1415–1430 (2007).
Fernihough, A. mfx: Marginal Effects, Odds Ratios and Incidence Rate Ratios for GLMs. (2014).
Venables, W. N. & Ripley, B. D. Random and Mixed Effects 271–300 (Springer, 2002). https://doi.org/10.1007/978-0-387-21706-2_10.
Aiken, L., West, S. & Reno, R. Multiple Regression: Testing and Interpreting Interactions (Sage Publications, 1991).
Cohen, J., Cohen, P., West, S. G. & Aiken, L. S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences (Routledge, 2002).
Long, J. A. interactions: Comprehensive, User-Friendly Toolkit for Probing Interactions. (2019).
Funding
The funding was provided by Japan Society for the Promotion of Science (Grant No. JP22H05212), Center for Integrative Science of Human Behavior, University of Tokyo, International Research Center for Neurointelligence, University of Tokyo.
Author information
Authors and Affiliations
Contributions
Study conception and design, Data analysis and interpretation: W.H.C.L., C.Y.F., S.K.; Data Acquisition: S.Y.; Writing: W.H.C.L., C.Y.F., S.K.; Revision: W.H.C.L., S.Y., C.Y.F., S.K.; Project supervision: S.K.; Final approval of the version to be published: All authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Law, W.H.C., Yoshino, S., Fong, C.Y. et al. Younger adults tolerate more relational risks in everyday life as revealed by the general risk-taking questionnaire. Sci Rep 12, 12184 (2022). https://doi.org/10.1038/s41598-022-16438-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-16438-2
- Springer Nature Limited