
Abstract
Gastric cancer (GC) is the fifth most frequent malignancy worldwide and the third leading cause of cancer-associated mortality. The study’s goal was to construct a predictive model and nomograms to predict the survival of GC patients. This historical cohort study assessed 733 patients who underwent treatments for GC. The univariate and multivariable Cox proportional hazard (CPH) survival analyses were applied to identify the factors related to overall survival (OS). A dynamic nomogram was developed as a graphical representation of the CPH regression model. The internal validation of the nomogram was evaluated by Harrell’s concordance index (C-index) and time-dependent AUC. The results of the multivariable Cox model revealed that the age of patients, body mass index (BMI), grade of tumor, and depth of tumor elevate the mortality hazard of gastric cancer patients (P < 0.05). The built nomogram had a discriminatory performance, with a C-index of 0.64 (CI 0.61, 0.67). We constructed and validated an original predictive nomogram for OS in patients with GC. Furthermore, nomograms may help predict the individual risk of OS in patients treated for GC.
Similar content being viewed by others


Introduction
Gastric cancer (GC) is one of the most common malignancies, with high incidence and mortality rates, and ranks as the fifth most frequent cancer and the third leading cause of cancer-related deaths globally1. The cancer is most commonly diagnosed in men among five countries (Bhutan, China, Kyrgyzstan, Mongolia, and Vietnam)2. Despite the fact that the incidence of GC has reduced during the past decades in European countries, the prognosis stays poor3. Also, the 5-year overall survival rate for GC patients is approximately 25 percent in the West4. Though the incidence of GC has decreased in Western countries in recent decades, its incidence has remained high in some Eastern countries (e.g., China, Japan, and Korea). Basis on the cancer registry of Turkey, GC may be the 5th most common malignancy in both men and women5. countries, two-thirds of new cases of stomach cancer are recorded, and survival is still low in both developed and developing countries6.
The incidence is approximately 7300 cases per year among the Iranian population, which is the most common cancer in men7. Moreover, mortality from GC can be the first leading factor of death due to cancer in both sexes8. However, the incidence of the disease was higher in men than in women9. Considering the low rate of 5-year survival of GC patients, identification and control of predictive factors remain the essential prevention methods10.
Notwithstanding these technologies and therapeutic strategies have progressed over the last several decades, but GC patients’ survival and risk factors remain unsatisfactory. It is crucial to recognize prognostic factors for those patients.
According to various statistical analyses, many researches have been performed to evaluate the prognosis factor on the survival of patients with GC10,11. Those methods incorporate several variables to predict a particular endpoint using traditional statistical methods (e.g., logistic or CPH regression models)12,13. Other studies have surveyed machine learning methods, which are a branch of artificial intelligence (AI) and computer science, on GC data14,15,16,17. Almazat et al. applied the Kaplan–Meier method to estimate overall survival in patients with GC18. The Cox and Frailty models of survival analysis were used and then compared with C-index13. Other researchers have presented nomograms, which are the graphical representation to intuitive perception of clinicians in Colorectal cancer (CRC) and GC patients11,19,20. A nomogram, a simple graphical visualization combining and quantifying all independent prognostic factors, plays an increasingly vital role in medical sciences and clinical studies21. Moreover, nomograms play a significant role in improving prognostic accuracy by combining all independent prognostic factors and quantifying their risks22,23. Nomogram, can be considered as a predictive statistical model for individual patients, reveals benefits than the conventional staging systems in predicting the outcomes of long-term survival in patients24. To the best of our knowledge, this study was the first survey on the predictive model regarding to nomogram presentation and OS for GC in Iran.
The objective of this study was to establish a CPH regression model to explore prognostic factors for OS in patients who underwent D2 radical gastric cancer surgery. Then, a more dynamic nomogram was constructed to predict overall survival based on a relatively large historical cohort of patients with GC.
Materials and methods
Patients and data sources
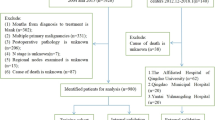
The demographical and clinicopathological characteristics of 733 GC patients were extracted from a tertiary University-Hospital of Iran, Taleghani Hospital in Tehran, between 2013 and 2020. This research complies with the principles of the Helsinki Declaration. We obtained the patients’ informed consent to be allowed to use their medical information. The methods were carried out in accordance with the relevant guidelines and regulations. The Ethics Committee of Iran University of Medical Sciences approved the study (Ethical code: IR.IUMS.REC.1399.122).
Demographic and clinical variables
Survival time, based on months elapsed from the cancer diagnosis until death, was considered the outcome variable. The demographical and clinical variables, including sex, marital status, smoking status, body mass index (BMI), family history, type of treatment, grade of tumour, depth of tumour, number of involved lymph nodes were predictors. The patients’ survival status was collected based on alive or dead.
Statistical analysis
The continuous variables were described as mean ± SD. Also, the frequency and percentage of categorical variables were reported. Missing data were imputed by fully conditional specification25. The Kaplan–Meier was used in order to estimate the survival function. We applied a univariable CPH model to explore the relationship between a patient’s survival and explanatory variables. The selected variables with P < 0.2 in the univariable analysis were subjected to multivariable regression modelling. Then, the nomogram was illustrated according to the multivariable CPH model. At last, C-index, as a global index for validating the predictive ability of a survival model, and time-dependent area under the roc curve were calculated to assess the internal validation. Also, internal calibration using bootstrap resampling was assessed by plotting the predicted probabilities from the model versus actual survival probabilities. The analysis was perform using the SPSS 23 and Stata 11. The survival, DynNom, rms, and hdnom packages in R 4.1.0 software were used to create a dynamic nomogram and to perform validation and calibration. Additionally, decision curve analysis (DCA) was applied with the function of “dcurves”. When the net benefit of a model is greater than curing in both all and none group of patients, the model can be considered as a clinical utility. The decision curve model can be compared with serious cases that curing all patients or none. If a model has acceptable level of advantage in a wide range of clinically reasonable preferences, the model or test can be advised.
Results
The study population consisted of 733 confirmed patients with GC who underwent treatment. The median of follow-up time is 9.55 months (IQR = 4–19.13, range 0.1–84). The mean ± SD age of patients was 59.49 ± 13.47 years, with ranges from 14 to 89 years. 932 (69.1%) of patients were male, and 417 (30.9%) were female. Six hundred ninety-nine (51.8%) patients were censored, and 643 (47.7%) of patients died at the end of follow-up. Other demographic and pathological characteristics of GC patients are given in Table 1. Also, the table revealed factors related to survival rate according to the univariable CPH regression model.
The results showed that age of diagnosing, BMI, family history, type of treatment, grade of tumour, and depth of tumour were significant in the univariable CPH model (P < 0.05).
Figure 1 revealed the Kaplan–meier according to American Joint Committee on Cancer (AJCC) staging, which the number at risks were listed below.

Kaplan–Meier survival curves by American joint committee on cancer staging, along with the number at risks in gastric cancer patients.
The results of the multivariable CPH were presented in Table 2. Variables that had P < 0.2 in the univariable analysis were candidates for the multivariable regression analysis. The table showed that age of diagnosis, BMI, grade of the tumour, and depth of tumour are significant in the multivariable CPH model (P < 0.05).
The result showed that for every 10 years of increasing the age, the hazard rate increases by 10% (HR = 1.01, P value < 0.05). The HR in patients with the overweight range was 46% less the than normal group (HR = 54%, P < 0.05); however, obese patients had higher HR than normal weight, which is non-significant (HR = 1.2, P = 0.518).
Also, the hazard ratio in patients who underwent chemotherapy, radiotherapy, and immunotherapy, presented as other treatments in the table, is 33% more than the people who had surgery; however, the type of treatment was non-significant (HR = 1.33, P = 0.057). Moreover, HR of tumour grade in patients with undifferentiated tumour grade was 57% more than people with well grade (HR = 1.57, P < 0.05). When the depth of the tumour deteriorated, the HR was soared significantly in GC patients. Thus, the higher the tumour depth, the higher HR (P < 0.05).
The results of the multivariable CPH model were presented as a nomogram in Fig. 2. The probability of survival for a GC patient can be predicted at a specific time point using this nomogram. The patient’s characteristics have been plotted on each variable axis. To predict the survival probability of a patient, a vertical line is drawn from the patient’s characteristics value to the top points scale. In this way, the number of points that were assigned by that variable value is determined. Then, the points from each variable value are summed. Finally, the sum on the total points is vertically projected onto the bottom axis, and a personalized probability survival time is obtained. Figure 3 shows the image of a web-based nomogram which is accessible in the https://nbshiny.shinyapps.io/GastricDynNom/. This is very simple-to-use web-based nomogram for convenient application, which can aid personalized treatment and clinical decision-making. This dynamic nomogram considers the sliders for covariates variable, bounded on the observed ranges, and drop-down boxes for categorical ones.

Predictive nomogram for survival in Gastric cancer patients.

Web-based survival rate calculator (Dynamic Nomogram (shinyapps.io)) to predict the survival of GC patients; Two patients who are 77 years old, no surgery, no family history, PT3 and 25 ≤ BMI < 30, but have different grade, well (black line) and poorly (blue line), according to the web survival rate calculator.
Internal validation and calibration
The internal validation was checked using C-Index and time-dependent AUC at evaluation time points. The C-index was calculated as 0.64 (CI 0.61, 0.67) also, we validate the performance of the CPH model with bootstrap resampling every year from the first year to the sixth year. In addition to, the C-index of the presented model, 0.64, was slightly less that of the AJCC clinical staging 0.68. The time-dependent AUC at 1, 2-, 3-, 4-, 5- and 6-years follow-up have been presented in Fig. 4A. Based on DCA, if the threshold probability be > 0.45, the developed nomogram is superior in predicting survival in all of the patients (Fig. 4B). In addition, the internal calibration using bootstrap resampling was assessed by plotting the predicted probabilities from the model versus actual survival probabilities. In this way, the samples were split into ten risk groups, and the survival probabilities at 1 and 2 years were obtained and summarized as calibration plots in Fig. 4C.

(A) Time-dependent AUC summary at evaluation time points. (B) Decision curve analysis. (C) Internal calibration using bootstrap resampling at 1 year and 2 years.
Discussion
This study provided a significant contribution through the use of a historical cohort of patients with GC who were treated in Iran from 2009 to 2020. As far as is known, this is the first study of nomogram in GC patients of Iranian population, known as a user-friendly clinical tool with an acceptable sample size and long-term follow up. In our study, we applied a web-based nomogram that can be used to predict the survival probability. The multivariable CPH model presented that age of diagnosing, BMI, family history, type of treatment, grade of tumour, and depth of tumour were statistically significant. Furthermore, we construct a nomogram to predict OS, which could provide individualized estimates of potential survival and aid individualized management decisions for GC. The C-index, calculated as 0.64 (CI 0.61, 0.67), was applied to evaluate the model internal validation, and found that the prognostic model has high accuracy. The C-index of 0.68 in AJCC clinical staging surpass the C-index of the presented model. Moreover, the time-dependent AUC was obtained to validate the performance of model, which was more than 60% for 1-, 3-, and 5-year of survival.
Nomogram is a precise and useful clinical tool that can help clinicians predict the probability of an outcome event, that is, survival time. A variety of nomograms have been built to predict the therapeutic benefits, the postoperative survival rate in patients with GC26,27,28. Mu et al. predicted the long-term survival of 421 GC patients, who underwent D2 radical lymphadenectomy, using survival model and establish a nomogram27. They calculated C-index of the model that was 0.76 for internal verification. Their significant factors were tumour staging, location of tumour, BMI, neural and vessel invasion. In our investigation, the age, grade of tumour and depth of tumour were considered as the main factor in multivariable CPH; also, the C-index was calculated 0.64. A study was done by Han et al. to predict survival after D2 gastrectomy for GC patients29. The C-index for OS was 0.69, and also, they established a nomogram predicting 5- and 10-year overall survival after D2 gastrectomy for gastric cancer. Also, another gastric cancer study multivariable Fine and Gray regression model to predict disease-specific mortality (DSM) that considered competing risks30. The goal of the study was to progress the first pre-treatment gastric cancer nomogram for predicting DSM that represented a acceptable discrimination in the new nomogram. Their result showed that the newly advanced nomogram perfectly predicted DSM, which can be used for patient advising in medical practice. In this study, their C-index of the model was 0.887 as well as the AJCC clinical staging 0.794. However, in our study the C-index of our model, equal to 0.64, was slightly less that of the AJCC clinical staging 0.68.
Here, we constructed a nomogram to predict the survival rate in GC patients. According to previous studies, a C-index > 0.6 indicated that the built model had an acceptance accuracy29,31,32. The value of this index was consistent with our study. In general, a few studies have applied AUC to predict the OS26,28,33. The AUC values of ROC were more than 60% for 1-, 3-, and 5-year of survival, which are compatible with our study. In addition, DCA was drawn to evaluate the clinical application value of the nomogram28,30,31,32,34. Lu et al. used a nomogram to predict recurrence-free survival and the advantages of adjuvant chemotherapy after radical resection in high stage GC patients31. They applied CPH model to identify predictive factors for RFS; moreover, established a novel nomogram for GC after radical resection.
Our multivariable CPH regression model discovered that age of diagnosis, BMI, grade of the tumour and tumour depth were independent risk factors in GC. Most of the previous studies focused on independent variables associated with GC and found that tumour depth, differentiation grade, size, and lymphatic invasion were closely associated with patients’ survival35,36. Lu et al. reported age, differentiation, tumour size, number of examined lymph nodes, pT stage, pN stage, and adjuvant chemotherapy as associated with GC31. They showed that the hazard ratio increased with age, which means that, the older patients get, the higher the hazard. Similarly, our study found that age and pT stage were significant in the CPH model. In our multivariable CPH regression model, the groups with 25 ≤ BMI < 30 had significantly higher than the group with a BMI ≤ 18.5 cm, suggesting that the BMI was a powerful predictor in patients with GC. The built nomogram finally corroborated that the BMI was one of the main risk factors in predicting survival of GC patients27,32. Regarding the grade of tumour, most previous studies reported that the tumour grade was a main predictor for patients with GC14,15,22,26,27,29,31. Similarly, our study found the grade of tumour can be a strong predictor in patients with GC. That means the worse the tumor grade, the greater the hazard ratio.
Study limitation
The key strength of this study is the long-term follow-up period. The second strength of the study is to use web-based nomogram that any expert can calculate the overall survival probability. Also, we had several limitations. First, some variables, such as Helicobacter pylori infection status, location of tumour, demarcation line of tumour lesion, tumour markers, nutritional status, and Charlson Comorbidity Index, may also be potential risk factors in patients with GC and need to be incorporated into our model. Second, statistical analysis was performed using internal validation. It is suggested that in future studies, external validation can be performed using another test dataset. Third, the key limitation of the present survey was the small number of sample size in a center that recommend to larger sample size in similar studies. Forth limitation is to collect some variables, such as BMI and age in the form of continuous instead of categorical variable37.
Conclusion
We successfully established a novel nomogram using patient data from the GC database in Taleghani University-Hospital. Furthermore, the age at diagnosing, BMI, tumour grade, depth of tumour made a significant contribution in predicting OS of patients with GC.
Abbreviations
- AI:
-
Artificial intelligence
- AJCC:
-
American Joint Committee on Cancer
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- C-index:
-
Concordance index
- CI:
-
Confidence interval
- CRC:
-
Colorectal cancer
- CPH:
-
Cox proportional hazard
- DCA:
-
Decision curve analysis
- DSM:
-
Disease-specific mortality
- GC:
-
Gastric cancer
- HR:
-
Hazard ratio
- IQR:
-
Interquartile range
- OS:
-
Overall survival
- RFS:
-
Recurrence-free survival
- ROC:
-
Receiver operating characteristic
- SD:
-
Standard deviation
References
Díaz del Arco, C. et al. Are Borrmann’s types of advanced gastric cancer distinct clinicopathological and molecular entities? A western study. Cancers 13(12), 3081 (2021).
Stojanovic, M. M., Rancic, N. K., Andjelkovic Apostolovic, M. R., Ignjatovic, A. M. & Ilic, M. V. Trends of stomach cancer in Central Serbia. Medicina 57(7), 665 (2021).
Dassen, A. E. et al. Gastric cancer: Decreasing incidence but stable survival in the Netherlands. Acta Oncol. 53(1), 138–142 (2014).
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2016. Cancer J. Clin. 66(1), 7–30 (2016).
Yaprak, G., Tataroglu, D., Dogan, B. & Pekyurek, M. Prognostic factors for survival in patients with gastric cancer: Single-centre experience. Northern Clin. Istanbul 7(2), 146 (2020).
Ferlay, J. et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 144(8), 1941–1953 (2019).
Safari, M., Mahjub, H., Esmaeili, H., Sadighi, S., & Roshanaei, G. Estimating the treatment effect in patients with gastric cancer in the presence of Noncompliance. Gastroenterology and Hepatology from Bed to Bench. 2021.
Maroufizadeh, S., Hajizadeh, E., Baghestani, A. R. & Fatemi, S. R. Multivariate analysis of prognostic factors in gastric cancer patients using additive hazards regression models. Asian Pac. J. Cancer Prev. 12(7), 1697–1702 (2011).
Farmanfarma, K. K., Mahdavifar, N., Hassanipour, S. & Salehiniya, H. Epidemiologic study of gastric cancer in Iran: A systematic review. Clin. Exp. Gastroenterol. 13, 511 (2020).
Talebi, A. et al. Survival analysis in gastric cancer: A multi-center study among Iranian patients. BMC Surg. 20(1), 1–8 (2020).
Borumandnia, N. et al. Nomogram to predict the overall survival of colorectal cancer patients: A multicenter national study. Int. J. Environ. Res. Public Health 18(15), 7734 (2021).
Xu, W. et al. Prediction model of tumor regression grade for advanced gastric cancer after preoperative chemotherapy. Front. Oncol. 11, 25 (2021).
Faradmal, J., Talebi, A., Rezaianzadeh, A. & Mahjub, H. Survival analysis of breast cancer patients using cox and frailty models. J. Res. Health Sci. 12(2), 127–130 (2012).
Nilsaz-Dezfouli, H., Abu-Bakar, M. R., Arasan, J., Adam, M. B. & Pourhoseingholi, M. A. Improving gastric cancer outcome prediction using single time-point artificial neural network models. Cancer Inform. 16, 1176935116686062 (2017).
Niu, P.-H., Zhao, L.-L., Wu, H.-L., Zhao, D.-B. & Chen, Y.-T. Artificial intelligence in gastric cancer: Application and future perspectives. World J. Gastroenterol. 26(36), 5408 (2020).
Zhou, C. et al. A machine learning-based predictor for the identification of the recurrence of patients with gastric cancer after operation. Sci. Rep. 11(1), 1–7 (2021).
Zhu, S.-L., Dong, J., Zhang, C., Huang, Y.-B. & Pan, W. Application of machine learning in the diagnosis of gastric cancer based on noninvasive characteristics. PLoS ONE 15(12), 0244869 (2020).
Almazar, A. E., Penfield, J. D., Saito, Y. A. & Talley, N. J. Survival times of patients with Menetrier’s disease and risk of gastric cancer. Clin. Gastroenterol. Hepatol. 19(4), 707–712 (2021).
Liang, X., et al. Development of a clinical nomogram for prediction of response to neoadjuvant chemotherapy in patients with advanced gastric cancer. 2021.
Zhou, X. et al. A novel nomogram for predicting survival of patients with poorly differentiated gastric adenocarcinoma. Transl. Cancer Res. 10(2), 886–898 (2021).
Jalali, A., Alvarez-Iglesias, A., Roshan, D. & Newell, J. Visualising statistical models using dynamic nomograms. PLoS One 14(11), e0225253 (2019).
Kawai, K. et al. Nomogram predicting survival after recurrence in patients with stage I to III colon cancer: A nationwide multicenter study. Dis. Colon Rectum 61(9), 1053–1062 (2018).
Song, K. Y., Park, Y. G., Jeon, H. M. & Park, C. H. A nomogram for predicting individual survival of patients with gastric cancer who underwent radical surgery with extended lymph node dissection. Gastr. Cancer 17(2), 287–293 (2014).
Li, L. et al. Development and validation of a prognostic nomogram based on the systemic immune-inflammation index for resectable gallbladder cancer to predict survival and chemotherapy benefit. Front. Oncol. 11, 2392 (2021).
Liu, Y. & De, A. Multiple imputation by fully conditional specification for dealing with missing data in a large epidemiologic study. Int. J. Stat. Med. Res. 4(3), 287 (2015).
Gao, Z. et al. A nomogram for prediction of stage III/IV gastric cancer outcome after surgery: A multicenter population-based study. Cancer Med. 9(15), 5490–5499 (2020).
Mu, G.-C. et al. Application value of nomogram and prognostic factors of gastric cancer patients who underwent D2 radical lymphadenectomy. BMC Gastroenterol. 19(1), 1–8 (2019).
Wang, J. et al. Nomogram-based prediction of survival in unresectable or metastatic gastric cancer patients with good performance status who received first-line chemotherapy. Ann. Transl. Med. 8, 6 (2020).
Han, D.-S. et al. Nomogram predicting long-term survival after d2 gastrectomy for gastric cancer. J. Clin. Oncol. 30(31), 3834–3840 (2012).
Bando, E. et al. Development and validation of a pretreatment nomogram to predict overall survival in gastric cancer. Cancer Med. 9(16), 5708–5718 (2020).
Lu, J. et al. Development and external validation of a nomogram to predict recurrence-free survival after R0 resection for stage II/III gastric cancer: An international multicenter study. Front. Oncol. 10, 25 (2020).
Yin, Q. H. et al. A Nomogram based on preoperative clinical bio-indicators to predict 5-year survivals for patients with gastric cancer after radical gastrectomy. Cancer Manage. Res. 12, 3995 (2020).
Chen, J. et al. A clinical model to predict distant metastasis in patients with superficial gastric cancer with negative lymph node metastasis and a survival analysis for patients with metastasis. Cancer Med. 10(3), 944–955 (2021).
Luo, J. et al. Prognostic value and nomograms of proximal margin distance in gastric cancer with radical distal gastrectomy. Chin. J. Cancer Res. 32(2), 186 (2020).
Fang, W.-L. et al. The risk factors of lymph node metastasis in early gastric cancer. Pathol. Oncol. Res. 21(4), 941–946 (2015).
Yang, H.-J. et al. Predictors of lymph node metastasis in patients with non-curative endoscopic resection of early gastric cancer. Surg. Endosc. 29(5), 1145–1155 (2015).
Frank, E. H. Regression Modeling Strategies with Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis (Springer, 2015).
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, A.T. and N.B.; methodology, A.T. and N.B.; software, N.B., A.T.; formal analysis, N.B. and A.T.; investigation, A.T.; resources, A.T.; responsible for data collection, M.A.P.; data curation, A.T.; N.B.; and S.A.; writing-original draft preparation, A.T., N.B.; writing-review and editing, A.T., N.B., S.A., H.D., S.A.P.T.; visualization, N.B. and A.T.; supervision, A.T., N.B., S.A., H.D.; All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Talebi, A., Borumandnia, N., Doosti, H. et al. Development of web-based dynamic nomogram to predict survival in patients with gastric cancer: a population-based study. Sci Rep 12, 4580 (2022). https://doi.org/10.1038/s41598-022-08465-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-08465-w
- Springer Nature Limited