
Abstract
Although female infants may have an early life biological advantage over males, gendered treatment can alter health outcomes. Ecuador has an unusually high ratio of male to female infant mortality, but gender norms have been reported to favor boys. This analysis of baseline data from the Lulun Project, a randomized controlled trial conducted in rural Andean communities of Ecuador, investigates the roles of sex and gender in undernutrition among infants 6 to 9 months of age. Twenty-four-hour recall frequencies were used to assess dietary intake. Food outcome models were analyzed as prevalence ratios calculated using a binomial distribution with a log link or robust Poisson regression. Linear regression was used to analyze the continuous growth outcome length-for-age z score. Socioeconomic and health history variables were comparable between male and female infants. Boys were more often fed liquids other than breastmilk within their first 3 days of life (17.1% vs. 5.2%, P = 0.026). Compared with girls, boys were less likely to be fed eggs by 33% (95% CI 0.46, 0.96), cheese, yogurt, or other milk products by 40% (95% CI 0.39, 0.92), yellow fruit by 44% (95% CI 0.33, 0.97), water by 37% (95% CI 0.45, 0.88), thin porridge by 29% (95% CI 0.56, 0.92), and tea without milk by 67% (95% CI 0.11, 0.99). Prevalence of boys with an adequate dietary diversity score (≥ 4) was reduced by 27% relative to girls (95% CI 0.54, 0.99). Males fared worse in length-for-age z scores (− 2.16 vs. − 1.56, P = 0.000), weight-for-age z scores (− 0.86 vs. − 0.33, P = 0.002), prevalence of stunting (50.6% vs. 23.4%, P = 0.000), and plasma concentrations of dimethylglycine (1.25 vs. 1.65 µg/mL, P = 0.021). After adjusting for demographic, caregiver perceptions of appetite, and biological factors, length-for-age z score for a male child was 0.62 units lower than for a female (95% CI − 0.98, − 0.26). Male infants were shown to receive lower quality complementary foods and have worse anthropometric measures than female infants.
Trial registration clinicaltrials.gov, NCT02446873. Registered February 28, 2015, https://clinicaltrials.gov/ct2/show/NCT02446873.
Similar content being viewed by others

Introduction
From infancy through early childhood, across a variety of contexts and health outcomes, females have been observed to have a biological advantage over males1,2,3,4,5. In 2012, the global infant mortality sex ratio (the ratio of male to female mortality) was 1.13 (90% uncertainty interval, 1.12–1.15), indicating 13% more infant deaths among males than females worldwide6. A recent systematic review and meta-analysis finds that this pattern extends to undernutrition; boys under age 5 are more likely to experience wasting, stunting, and underweight than girls7. However, these results are context dependent. Girls’ early life advantage is predicated upon equal treatment. In contexts where boys are valued over girls and given greater access to health care and nutrition, the biological female advantage may be diminished or even reversed8.
Although in many contexts, males are expected to have higher rates of morbidity and mortality, extremely high mortality sex ratios may indicate excess male deaths (i.e., more deaths than would be expected by biological factors alone). Ecuador, with an unusually high ratio of male to female infant mortality of 1.32, may have a greater-than-expected degree of male disadvantage in survival5, which may imply a gendered behavioral effect. This difference would be significant because gender inequality that favors men has been identified as a key factor impacting Ecuador’s standing on the Human Development Index9. Moreover, in traditional gender-based practices in highland indigenous communities in Ecuador, lactation and weaning practices favored boys10. Given these opposing trends, it is unclear whether, in this context, one would expect differences in breastfeeding and complementary feeding, which contribute to infant survival, to favor boys or girls.
From March to December 2015, the Lulun Project, a randomized controlled trial (RCT), was conducted in rural Andean communities in Ecuador to examine the effects of egg consumption early in the complementary feeding period on nutritional outcomes11. At baseline, we observed greater prevalence of undernutrition among male infants. To better understand this observation, the objective of the present study was to investigate the roles of both sex (biological attributes) and gender (social constructs)12 in undernutrition. The latter refers to not only how individuals identify themselves but also how boys and girls (including infants) are treated by others. We tested whether differences in breastfeeding and complementary feeding practices exist, as well as their relation to biological markers and growth outcomes. Given reports of gender inequality in Ecuador as well as its outlying infant mortality sex ratio, we hypothesized that gendered differences in breastfeeding and complementary feeding were likely to exist.
Throughout this report, we attempt to thoughtfully use the terms sex and/or gender in accord with the Sex and Gender Equity in Research (SAGER) guidelines12. In practice, even with careful consideration, these terms may prove difficult if not impossible to disentangle. Often, outcomes may be a mixture of both biological effects of sex combined with social and behavioral impacts of gender13. In this report, when focusing on biological factors (e.g., report of biomarkers), we use the term sex. When discussing factors that imply a behavioral or social component (e.g., complementary feeding behaviors or practices), we use the term gender. In doing so, we do not intend to convey a strict separation; indeed, we acknowledge that in many cases they are inseparable. When considering both biological along with social and behavioral factors, we use the combined term, sex/gender (however, we do not intend for this to suggest that the terms are interchangeable). We acknowledge, as have previous authors, definitions of sex and gender are evolving as science in this area grows13.
Methods
Study sample
This study employs baseline data collected for the Lulun Project, an RCT that investigated nutritional outcomes in children after an intervention that promoted greater consumption of eggs11. The study took place in 5 rural parishes of Cotopaxi Province, Ecuador. This region has a large indigenous population; according to National Census Data, approximately one-fifth (22%) of Cotopaxi’s population of 409,205 persons self-identified as indigenous compared to 7% nationally14. Approval for the study was obtained from ethical oversight committees at the Universidad San Francisco de Quito, Washington University in St. Louis, and the Pan American Health Organization. All mothers or primary caregivers provided written informed consent prior to data collection. All research was performed in accordance with the Declaration of Helsinki.
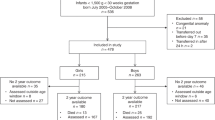
Study design and recruitment methods have been described in detail previously11,15. Eligibility requirements for infants included good health, born singleton, and aged 6 to 9 months at the time of recruitment. Exclusion criteria included congenital heart condition, severe acute malnutrition, and egg allergy. Potential eligible mother or other caregiver-infant pairs were transported to data collection sites. Of the initial 179 pairs assessed for eligibility, 4 did not meet eligibility criteria. An additional 9 caregivers declined for reasons such as moving from the area, concerns regarding blood draws, or other reasons. This analysis is based on 166 mother or other caregiver-infant pairs who enrolled in the study and completed baseline questionnaires. Biomarker data is available for 142 infants.
Study variables
Mothers or other caregivers provided socioeconomic, demographic, breastfeeding status, child dietary intake, and morbidity information via an administered survey. Foods commonly consumed in the area were determined through formative research16,17. Twenty-four-hour recall frequencies were used to assess dietary intake and to assign a dietary diversity score18. Morbidities were assessed through 7-day recall, focusing on conditions prevalent in the area, including diarrheal and respiratory symptoms, as well as fever, skin rash, persistent cough, congestion or runny nose, panting, wheezing, or difficulty breathing, and toothache or teething.
Biomarkers
Plasma concentrations of nutrient biomarkers, including choline, betaine, dimethylglycine (DMG), vitamin B12, linoleic acid (LA; 18:2n-6), α-linolenic acid (ALA; 18:3n-3), and docosahexaenoic acid (DHA) were analyzed. Specimen processing and laboratory methods have been described previously19. In brief, nutrient concentrations for choline, betaine, DMG, LA, ALA, and DHA were determined by modified liquid chromatography-tandem mass spectrometry (LC–MS/MS) methods. For vitamin B12 concentrations, chemiluminescent competitive immunoassay was used (IMMULITE 1000 Analyzer; Diagnostic Products).
Growth outcomes
International standardized protocols were used to guide measurement of anthropometric data20. As previously described by Iannotti et al. (2017), study enumerators participated in 3-day training and validation exercises. Enumerator pairs each took measurements of child length to the nearest 1 mm using a Seca 417 portable infantometer. If measures differed by 5 mm or more, a third measurement was made, and the result was averaged with the closest measure. A Seca Model 874 Electronic Digital Scale, with mother/child tare feature to the nearest 0.01, was used to measure weight. If the two measures taken differed by 0.05 kg or more, a third measure was made, and the results averaged. Measures were converted to z scores for length-for-age (LAZ), weight-for-age (WAZ), weight-for-length (WLZ), and BMI (BMIz)11. Stunting is defined as length-for-age z score (LAZ) < − 220.
Statistical methods
Tables were generated to estimate associations between the exposure groups of interest (girls and boys) and possible confounders and then to compare responses to food frequency questionnaires across the groups. For bivariate statistics, probability values were obtained with a Fisher's exact test for categorical variables and two-sample t test for continuous variables. When unequal variances were detected, a two-sample t test with unequal variances was used. For continuous variables, when deviations from normality were detected, results were rechecked with a two-sample Wilcoxon rank-sum test.
Food outcome models (dichotomous outcomes) were analyzed as prevalence ratios calculated using a binomial distribution with a log link or robust Poisson regression when a model failed to converge21. We first fit an unadjusted model including only child’s gender, then adjusted for child’s age, mother’s age and education. We used the Benjamini–Hochberg method with a false discovery rate threshold of 0.20 to adjust for multiple comparisons across individual food items22.
Linear regression was used to analyze our continuous growth outcome LAZ. We first fit an unadjusted model including only child’s sex/gender. In our adjusted model, we included demographic variables (child’s sex/gender, age, and firstborn status, and maternal age and education), breastfeeding and complementary feeding variables (fed something other than breast milk within the first three days, child’s appetite, and dietary diversity score ≥ 4), and biomarkers (choline, betaine, DMG, vitamin B12, ALA, and DHA). We did not include the biomarker LA because of a high correlation (r = 0.878) with ALA. We tested for a sex/gender and vitamin B12 interaction, added to the adjusted model. We conducted diagnostic and residual analysis on the adjusted model. Problematic multicollinearity was not detected based on variance inflation factors (VIF); VIFs were < 2 for all variables. A Breusch-Pagan/Cook-Weisberg test for heteroskedasticity was nonsignificant (P = 0.179). Residuals were assessed graphically and appear reasonably normally distributed. Influential cases were examined using Cook’s distance; no observations were identified as influential. All analyses were performed using STATA software (version 14.2; StataCorp), and P-values ≤ 0.050 were considered statistically significant.
Ethics approval and consent to participate
Approval for the study was obtained from ethical oversight committees at the Universidad San Francisco de Quito, Washington University in St. Louis, and the Pan American Health Organization. All mothers or primary caregivers provided written informed consent prior to data collection.
Results
Of the 166 children included in the study, 54% were male. No statistically significant differences were observed between groups in terms of child age or percent firstborn (Table 1). The groups were similar regarding maternal characteristics, including maternal age, teenage mother, years of education completed, maternal employment outside the home, and type of caregiver reporting. No statistically significant differences were observed regarding household or socioeconomic factors, including number of household members, types of crops grown, livestock owned, participation in the government’s conditional cash transfer program, use of an improved water source, treated water, flush toilet, and gas or electric cooking fuel.
We compared the groups for differences in health characteristics (Supplemental Table 1). No statistically significant differences were observed in 6-month histories of health service visits (to public hospitals or health centers, private clinics, or others). Similarly, no statistically significant differences were found in 6-month use of supplements or other nutrition products (iron, vitamin A, multivitamins or minerals, or food rations). The two groups were similar in report of 7-day histories of fever, diarrhea, blood in stool, skin rash, constant cough, congestion/runny nose, panting/wheezing/difficulty breathing, bruising, scrapes, or cuts, toothache/teething, and receipt of oral rehydration salts.
A similar proportion of infant boys and girls were ever breastfed, breastfed within 1 h of birth, fed colostrum, received practical support or advice to start breastfeeding, breastfed yesterday, and who the decision-maker was for what the child should and should not be fed (Table 2). But boys were reported 3 times more often than girls to have been fed something other than breast milk within their first 3 days of life. Differences were also noted in caregiver’s assessment of the child’s appetite, with poor appetite reported nearly 5 times less frequently for boys than girls.
The prevalence ratios of boys receiving the same food items within the last 24 h as compared to girls are reported in Table 3. In all cases, when a statistically significant difference was detected, it favored receipt of the item by girls. In adjusted models, prevalence of receiving the following food items were reduced for boys relative to girls: by 33% for eggs, 40% for cheese, yogurt, or other milk products, 37% for water, 29% for thin porridge, 67% for tea without milk, and 44% for yellow fruit. Prevalence of boys receiving a dietary diversity score of ≥ 4 was reduced by 27% relative to girls. These results remained significant after applying the Benjamini–Hochberg procedure with a 0.20 false discovery rate level. No statistically significant differences were detected among other food items.
With regard to anthropometric measures LAZ and WAZ, males fared significantly worse than females; LAZ for males was 38% lower than that of females, while WAZ was nearly 3 times lower (Table 4). Likewise, prevalence of stunting among males was more than double that of females. Other anthropometric measures—WLZ and BMIZ—show a similar pattern (higher values for females than males), although the differences were not statistically significant. Prevalences of underweight and wasting were low in this sample, and no statistically significant differences between groups were detected. Plasma concentrations of DMG for males were 24% lower than that of females. No significant differences were noted for other biomarkers, including choline, betaine, ratio betaine to choline, vitamin B12, LA, ALA, Ratio LA to ALA, and DHA.
Based on our unadjusted model, LAZ for a male child is 0.63 units lower than for a female (95% confidence interval [CI] − 0.97, − 0.29; Table 5). After controlling for other variables in the model, LAZ for a male child is 0.62 units lower than for a female (95% CI − 0.98, − 0.26). For each unit increase in caregiver’s assessment of child’s appetite, LAZ increases by 0.38 (95% CI 0.05, 0.71). For each unit increase in vitamin B12, LAZ decreases by 0.002 (95% CI − 0.003, − 0.001). Other variables in the model showed no statistically significant relationship with LAZ. Added to our adjusted model, we found that an interaction between sex/gender and vitamin B12 was significant (P = 0.008). A graph of the joint effects with selected values for vitamin B12 is provided in Supplemental Fig. 1. For males, as vitamin B12 increases, LAZ decreases; however, for females, level of vitamin B12 has no association with LAZ. Prevalence ratios for unadjusted and adjusted models of the growth outcome stunting calculated using robust Poisson regression are presented in Supplemental Table 2.
Discussion
Among infants ages 6 to 9 months of age, males were at greater risk for stunting than females after adjusting for demographic, caregiver perceptions of appetite, and biological factors. Vitamin B12 showed a statistically significant negative association with LAZ. In terms of potential risk factors, this analysis shows that caregivers reported a healthy appetite among a higher proportion of boys compared to girls, but boys had lower odds of receiving certain complementary foods and dietary diversity compared to girls. These findings are consistent with the evidence that shows a biological health advantage for females; however, these results also suggest a gendered behavioral effect that favors girls. This is important to consider, as these results suggest a greater degree of vulnerability in male infants in this population.
Our findings of significantly worse growth outcomes for male infants align with the literature that reports a female advantage across a variety of health outcomes. Obstetrical complications, such as umbilical cord abnormalities, gestational diabetes, and delivery by cesarean section, are more common among male pregnancies than female1,2,4. Newborn males fare worse in susceptibility to birth trauma, intrauterine hypoxia and birth asphyxia, prematurity, respiratory distress syndrome, neonatal tetanus, congenital anomalies, intestinal infections, and lower respiratory infections5. Male children also appear to be more strongly affected by environmental exposures such as lead and pesticides, as well as by exposures resulting from maternal behaviors such alcohol or opioid use3. Although more research is needed to help elucidate the mechanisms underlying these outcomes, evolutionary theories of fitness suggest males face a trade-off between immunity and musculoskeletal maintenance, related to the major costs of immune response23. However, in a study examining the impact of immune function on growth among Amazonian forager-horticulturalists, investigators did not observe consistent differences between male and female children24. Others have explored evidence of sex-specific life history strategies, with females exhibiting greater growth canalization, as well as survivorship effects in the aftermath of unequal treatment in early life25.
When children receive equal treatment, female advantage is generally expected. When there are gendered differences in treatment, this trend may be either heightened, diminished, or even reversed depending on which gender is favored and to what degree. Thus, although female advantage may be the norm, it is highly context dependent. Alkema et al. (2014) identified 17 countries in 1990 with higher-than-expected under-5 mortality sex ratios and 5 countries in 2012: Guinea-Bissau, Kazakhstan, Mongolia, Uganda, and Uzbekistan. Similarly, a report by the United Nations Population Division (2011) identified twenty countries, including Ecuador, with excessively high infant mortality sex ratios (indicative of greater-than-expected male mortality)5. Excess female mortality has been reported in 10 countries based on outlying under-5 mortality sex ratios: Afghanistan, Bahrain, Bangladesh, China, Egypt, India, Iran, Jordan, Nepal, and Pakistan6. In India, the country with the highest excess female infant mortality rate in 20126, nutritional disadvantage may play a role. An analysis of data from India’s National Family Health Survey (2005–2006) found that higher mortality risk among girls was associated with gendered differences in breastfeeding and complementary feeding; specifically, girls received less breast milk and less fresh milk than boys8.
We examined whether worse growth outcomes observed among male than female infants in Ecuador are related to gendered differences in breastfeeding or complementary feeding practices. Our results show a consistent pattern of gendered differences. Anthropological research conducted in Ecuador has reported that boys receive better treatment than girls during lactation and weaning, largely because of traditional beliefs that boys should be strong, while breastfeeding girls will convey undesirable male characteristics10. We found that boys were more often fed something other than breast milk within their first 3 days of life, as opposed to the recommended practice of exclusive breastfeeding for the first 6 months26. This could negatively impact infant health through increased immune challenge as the result of early exposure to contaminated liquids. Additionally, early supplementation negatively impacts breastmilk production, duration and exclusivity of breastfeeding, and the infant’s microbiome27. Boys were less likely to receive nutritious food items such as eggs, dairy products, and yellow fruits. However, boys were also less likely to receive water, thin porridge, or tea without milk, which are items of poor nutritional value. Boys were less likely to receive a score ≥ 4 for dietary diversity; this finding is significant because consumption of foods from 4 or more of the 7 constructed food groups is indicative of better quality diets regardless of breastfeeding status18.
Caretakers’ assessments of infants’ appetites were a statistically significant predictor of LAZ; perception of stronger appetite was associated with greater LAZ. Additionally, we noted gendered differences in caretakers’ perception of infants’ appetite, with poor appetite rarely noted for boys. Caretakers’ greater concern for poor appetite among girls may have led them to offer a wider variety of complementary foods, a potential explanation for the gendered differences observed here. Similarly, mothers in an indigenous village in Guatemala reported that infant boys were hungrier and less satisfied with breastfeeding alone, leading to earlier complementary feeding. While growth patterns initially favored female infants, sex differences declined in the second year of life, a pattern the authors attributed to gendered cultural perceptions around feeding28. In an Andean population of Peru, similar results were seen, with female infants initially showing better growth in height-for-age z scores at baseline, while differences by sex were not statistically significant at 6-month follow-up29. In Ecuador, additional research is needed to explore this result and track outcomes over time.
Among the biomarkers tested, only DMG showed a statistically significant difference by sex. Females had significantly higher DMG than males in this study. However, DMG was not a significant predictor of our growth outcome, LAZ. It is unclear whether DMG levels would be expected to differ by sex at this age. Vitamin B12 was identified as a significant predictor of LAZ. While seemingly counterintuitive, higher levels of vitamin B12 were associated with lower LAZ. However, for LAZ, the significant interaction between vitamin B12 and sex/gender indicated this association was specific to males but not females. To our knowledge, this is a novel finding, requiring additional research to verify and explain this result. Both DMG and vitamin B12 are components of the one-carbon metabolism cycle, impacting health and disease through their role in physiological processes including biosynthesis, amino acid homeostasis, epigenetic maintenance, and redox defense30.
Limitations
This study was observational and not designed a priori to test sex and gender factors on nutrition outcomes in these infants. Several factors may have impacted growth outcomes but were not tested in this analysis. Birth weight and gestational age at birth were not collected because they may not be accurately remembered or may be unknown11. Intergenerational effects on linear growth have been well documented31,32, but we do not have maternal anthropometric measurements. We did not account for maternal nutritional status during pregnancy and breastfeeding nor recurrent infections in infants, which are reported to be proximal determinants of stunting33. We utilized baseline data to avoid the intervention effects of the RCT, but longitudinal data would be preferable; it is unclear if biomarkers and complementary feeding would be expected to predict growth outcomes at the same time point, rather than future growth. Additionally, we lack qualitative data which could have helped us understand the cultural beliefs underlying feeding practices.
Conclusions
This analysis demonstrates that male infants in this Andean population fare significantly worse than females, both in terms of anthropometric growth outcomes and receipt of healthy complementary foods. That is, unlike earlier studies that showed that gendered differences in infant feeding favored boys, we found that those practices seem to favor girls, leaving boys at a double disadvantage. While further research is needed to confirm and explain this difference, this paper highlights the enhanced vulnerability of male infants in this study area. Moving forward, studies are needed to determine sex-specific ranges for biomarkers by age, and both biological mechanisms leading to different outcomes based on sex and differences based on social and cultural behaviors revolving around gender, which may impact nutritional outcomes, should be explored.
Data availability
The data analyzed for this study are publicly available at Synapse, https://www.synapse.org/#!Synapse:syn21595086/files/.
Abbreviations
- ALA:
-
Alpha-linolenic acid
- BMIz:
-
Body mass index z score
- DHA:
-
Docosahexaenoic acid
- DMG:
-
Dimethylglycine
- LA:
-
Linoleic acid
- LAZ:
-
Length-for-age z score
- LC–MS/MS:
-
Modified liquid chromatography-tandem mass spectrometry
- RCT:
-
Randomized Controlled Trial
- SAGER:
-
Sex and Gender Equity in Research
- VIF:
-
Variance inflation factor
- WAZ:
-
Weight-for-age z score
- WLZ:
-
Weight-for-length z score
References
Aibar, L., Puertas, A., Valverde, M., Carrillo, M. P. & Montoya, F. Fetal sex and perinatal outcomes. J. Perinat. Med. 40, 271–276. https://doi.org/10.1515/jpm-2011-0137 (2012).
Di Renzo, G. C., Rosati, A., Sarti, R. D., Cruciani, L. & Cutuli, A. M. Does fetal sex affect pregnancy outcome?. Gend. Med. 4, 19–30. https://doi.org/10.1016/s1550-8579(07)80004-0 (2007).
DiPietro, J. A. & Voegtline, K. M. The gestational foundation of sex differences in development and vulnerability. Neuroscience 342, 4–20. https://doi.org/10.1016/j.neuroscience.2015.07.068 (2017).
Sheiner, E. et al. Gender does matter in perinatal medicine. Fetal. Diagn. Ther. 19, 366–369. https://doi.org/10.1159/000077967 (2004).
United Nations, Department of Economic and Social Affairs, Population Division. Sex Differentials in Childhood Mortality. (2011).
Alkema, L., Chao, F., You, D., Pedersen, J. & Sawyer, C. C. National, regional, and global sex ratios of infant, child, and under-5 mortality and identification of countries with outlying ratios: a systematic assessment. Lancet Glob. Health 2, e521–e530. https://doi.org/10.1016/s2214-109x(14)70280-3 (2014).
Thurstans, S. et al. Boys are more likely to be undernourished than girls: a systematic review and meta-analysis of sex differences in undernutrition. BMJ Glob. Health 5, 1–10. https://doi.org/10.1136/bmjgh-2020-004030 (2020).
Fledderjohann, J. et al. Do girls have a nutritional disadvantage compared with boys? Statistical models of breastfeeding and food consumption inequalities among Indian siblings. PLoS ONE 9, e107172. https://doi.org/10.1371/journal.pone.0107172 (2014).
UN Women. Americas and the Caribbean, Ecuador, https://lac.unwomen.org/en/donde-estamos/ecuador (n.d.).
Novotny, R. in Alimentacion, salud y estado nutricional del niño preescolar en la Sierra Ecuatoriana (eds L. McKee & S. Arguello) 271–308 (Editorial Abya-Yala, 1988).
Iannotti, L. L. et al. Eggs in early complementary feeding and child growth: a randomized controlled trial. Pediatrics https://doi.org/10.1542/peds.2016-3459 (2017).
Heidari, S., Babor, T. F., De Castro, P., Tort, S. & Curno, M. Sex and Gender Equity in Research: rationale for the SAGER guidelines and recommended use. Res. Integr. Peer Rev. 1, 2. https://doi.org/10.1186/s41073-016-0007-6 (2016).
Canadian Institutes of Health Research. What a difference sex and gender make: a gender, sex and health research casebook. (Ottowa, Canada, 2012).
Instituto Nacional de Estadísticas y Censos (INEC). Censo de Población y Vivienda 2010, http://www.ecuadorencifras.gob.ec/censo‐de‐poblacion‐y‐vivienda/ (2010).
Gallegos-Riofrío, C. A. et al. The Lulun Project’s social marketing strategy in a trial to introduce eggs during complementary feeding in Ecuador. Matern. Child Nutr. 14 Suppl 3, e12700. https://doi.org/10.1111/mcn.12700 (2018).
Arimond, M. et al. Simple food group diversity indicators predict micronutrient adequacy of women’s diets in 5 diverse, resource-poor settings. J. Nutr. 140, 2059s–2069s. https://doi.org/10.3945/jn.110.123414 (2010).
Gallegos CA, F. W., Waters W. . Assessment of the food situation of the population of Ecuador [In Spanish]. . (Quito, Ecuador: Secretaria Nacional de Planificacion y Desarrollo (SENPLADES), 2010).
World Health Organization. Indicators for assessing infant and young child feeding practices. (2008).
Iannotti, L. L. et al. Eggs early in complementary feeding increase choline pathway biomarkers and DHA: a randomized controlled trial in Ecuador. Am. J. Clin. Nutr. 106, 1482–1489. https://doi.org/10.3945/ajcn.117.160515 (2017).
World Health Organization. Child growth standards, https://www.who.int/childgrowth/standards/en/ (2017).
Petersen, M. R. & Deddens, J. A. A comparison of two methods for estimating prevalence ratios. BMC Med. Res. Methodol. 8, 9. https://doi.org/10.1186/1471-2288-8-9 (2008).
Glickman, M. E., Rao, S. R. & Schultz, M. R. False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. J. Clin. Epidemiol. 67, 850–857. https://doi.org/10.1016/j.jclinepi.2014.03.012 (2014).
Campbell, B. C., Lukas, W. D. & Campbell, K. L. in Reproductive Ecology and Human Evolution (ed P. T. Ellison) Ch. 7, 160–164 (Transaction Publishers, 2011).
Urlacher, S. S. et al. Tradeoffs between immune function and childhood growth among Amazonian forager-horticulturalists. Proc. Natl. Acad. Sci. U S A 115, E3914-e3921. https://doi.org/10.1073/pnas.1717522115 (2018).
Decaro, J. A., Decaro, E. & Worthman, C. M. Sex differences in child nutritional and immunological status 5–9 years post contact in fringe highland Papua New Guinea. Am. J. Hum. Biol. 22, 657–666. https://doi.org/10.1002/ajhb.21062 (2010).
World Health Organization. Infant and young child feeding, https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding#:~:text=WHO%20and%20UNICEF%20recommend%3A,years%20of%20age%20or%20beyond. (2020).
Walker, M. Formula supplementation of breastfed infants: helpful or hazardous?. ICAN Infant Child Adolescent Nutr. 7, 198–207. https://doi.org/10.1177/1941406415591208 (2015).
Tumilowicz, A., Habicht, J. P., Pelto, G. & Pelletier, D. L. Gender perceptions predict sex differences in growth patterns of indigenous Guatemalan infants and young children. Am. J. Clin. Nutr. 102, 1249–1258. https://doi.org/10.3945/ajcn.114.100776 (2015).
Hoke, M. K. Economic activity and patterns of infant growth in a high altitude district of Peru. Am. J. Hum. Biol. https://doi.org/10.1002/ajhb.23038 (2017).
Ducker, G. S. & Rabinowitz, J. D. One-carbon metabolism in health and disease. Cell Metab 25, 27–42. https://doi.org/10.1016/j.cmet.2016.08.009 (2017).
Martorell, R. & Zongrone, A. Intergenerational influences on child growth and undernutrition. Paediatr. Perinat. Epidemiol. 26(Suppl 1), 302–314. https://doi.org/10.1111/j.1365-3016.2012.01298.x (2012).
de Onis, M. & Branca, F. Childhood stunting: a global perspective. Matern. Child Nutr. 12(Suppl 1), 12–26. https://doi.org/10.1111/mcn.12231 (2016).
Prendergast, A. J. & Humphrey, J. H. The stunting syndrome in developing countries. Paediatr. Int. Child Health 34, 250–265. https://doi.org/10.1179/2046905514y.0000000158 (2014).
Funding
All phases of the Lulun RCT were supported by The Mathile Institute for the Advancement of Human Nutrition. Bill & Melinda Gates Foundation provided additional funding for some of the biomarker analyses.
Author information
Authors and Affiliations
Contributions
All authors have fulfilled all conditions required for authorship. L.L.I., C.P.S., C.K.L., W.F.W., and C.A.G.R. designed the research. C.A.G.R. and W.F.W. conducted the research. E.C.E. analyzed and interpreted the data and wrote the manuscript. L.L.I., C.A.G.R., W.F.W., C.K.L., and C.P.S. substantively revised the article. All authors have approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Evers, E.C., Waters, W.F., Gallegos-Riofrío, C.A. et al. A sex- and gender-based analysis of factors associated with linear growth in infants in Ecuadorian Andes. Sci Rep 12, 3292 (2022). https://doi.org/10.1038/s41598-022-06806-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-06806-3
- Springer Nature Limited