
Abstract
Bladder cancer (BCa) patients are diagnosed by cytology and cystoscopy. However, these diagnostic tests bear some limitations. We sought for reliable biomarkers to better determine BCa extension. Prostate-specific membrane antigen (PSMA) appears to fulfill this requirement in prostate cancer but its role in BCa has not been established yet. We then analyzed 87 bladder tissue samples from 74 patients assessing PSMA expression by immunohistochemistry. The median PSMA expression, exclusively found in tumor neovasculature, in terms of H-score significantly differed between non-tumor samples and tumor samples (p = 0.00288) showing a higher neovasculature-related PSMA expression. No differences were observed in relation to tumor type, grade and stage. BCa neovasculature-related PSMA overexpression may be useful in defining the degree of extension of the neoplasm. In addition, testing PSMA expression by immunohistochemistry may hold theranostic implications both considering anti-angiogenesis agents and radio-labelled PSMA ligands for intracavitary radionuclide therapy. In our opinion, BCa neovasculature-related PSMA overexpression may be considered an apt target for anti-angiogenesis and radionuclide treatment in BCa, once the evaluation of tumor-retention time for the appropriateness of long half-life therapeutic PSMA ligands as radionuclide treatment will be performed.
Similar content being viewed by others

Introduction
Bladder cancer (BCa) is the 10th most common form of cancer worldwide, with 549,000 new cases estimated and 200,000 deaths1. Despite urothelial BCa has been reported to be 3 times more common in men, many studies conclude that women have poorer prognosis2.
The excess risk in men has been hypothesized to be driven by higher exposure to carcinogens (cigarette smoking, occupation, chemical and water contaminants), whereas the reasons for poorer survival in women is not clear2.
The most common type of BCa is urothelial carcinoma, and approximately 75% of cases are non–muscle invasive (NMIBC) at diagnosis. Generally, NMIBC has a favorable prognosis and is diagnosed and treated with trans-urethral endoscopic resection, followed by intravesical therapy if the risk of recurrence of NMIBC or progression to muscle-invasive bladder cancer (MIBC) is high3. Cytology and cystoscopy are the conventionally used techniques for BCa diagnosis and monitoring but these have some limitations. The former has low sensitivity for low grade and low stage tumors, the latter has high specificity but it is invasive, therefore new diagnostic biomarkers would be desirable.
MIBC is found in about 25% of patients at the time of diagnosis, and these are conventionally treated by means of radical cystectomy (RC) and lymph node dissection4. The presence of nodal metastases, found in 20% to 25% of patients at the time of RC, is an important indicator for poor outcome along with pathologic tumor stage5. However, up to 37% of patients with locally-advanced BCa and absent nodal involvement (i.e. T stage > pT2 and pN0) develop distant metastases6. Thus, biological markers able to predict prognosis in this subset are still needed.
Prostate-specific membrane antigen (PSMA) is a non-soluble type 2 integral membrane protein with carboxypeptidase activity, expressed on the apical surface of endothelial cells. The expression of this antigen is not fully prostate-specific as it is also expressed in tumor-associated neovasculature of several solid malignancies7,8,9. It is known that PSMA plays a functional role in prostate cancer progression10, but its role in BCa progression is not well established yet.
PSMA has been validated as a target for PET imaging of prostate cancer, at primary staging and biochemical recurrence11,12. For human the most frequent used PET imaging PSMA ligand is the low-weight urea-based PSMA inhibitor Glu-NH-CO–NH-Lys(Ahx)-HBED-CC labelled with 68Gallium (68 Ga-PSMA-11). Like the PSMA monoclonal antibody used for immunostaining in our study (i.e. SP29), 68 Ga-PSMA-11 binds to a C-terminal epitope of the large extra-membrane domain of PSMA. How much the degree of uptake of 68 Ga-PSMA-11 uptake in BCa significantly correlates with PSMA expression in the different BCa lesions and stage of the disease has to be demonstrated yet.
The aim of the present study was to assess whether PSMA expression could represent a useful marker for BCa diagnosis and to establish whether its expression could be an apt target for anti- angiogenesis and/or radionuclide treatment in BCa.
Results
The analysis of PSMA expression was feasible in the overall series of tumor and non tumor samples (healthy tissues, hyperplasia, dysplasia). We observed PSMA expression only in the tumor neovasculature; in particular PSMA positivity in the tumors was observed in the tumor neovasculature, while in the non tumor tissue it was expressed in the neovasculature of dysplastic area and in some cases it was observed in ulcerated area. Eighteen samples (20.7%) were classified as non tumor samples of whom 11 (12.6%) were healthy bladder tissue, 3 (3.4%) were hyperplasia and 4 (4.6%) were dysplastic tissue. Sixty-nine (79.3%) were tumor samples (Table 1).
Out of the 69 tumor samples 7 were in situ carcinomas, 39 were papillary carcinomas of whom 5 had infiltrating morphological features, and 23 were infiltrating tumors. These 23 samples were further classified by the pathologist in: 1 adenocarcinoma of the bladder, 2 small cell carcinomas, 2 squamous cell carcinomas, 1 clear cell urothelial carcinoma (glycogen rich), 1 sarcomatoid carcinoma, 2 poorly differentiated urothelial carcinomas, 1 urothelial carcinoma with glandular differentiation, 10 conventional urothelial carcinomas and 3 large nested urothelial carcinomas.
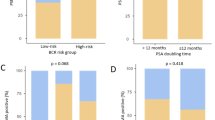
The median PSMA expression in terms of H-score in the overall series was 210 (range 0–300) (Table 1). In Fig. 1, we present the data distribution in terms of PSMA H-score of non tumor (no. 18) and tumor samples (no. 69).

Data distribution in terms of PSMA H-score of non tumor (no. 18) and tumor samples (no. 69).
The median PSMA expression in terms of H-score significantly differed between non tumor and tumor samples (p = 0.00288) (Table 1), that showed higher PSMA expression in the tumor neovasculature. We observed higher expression of PSMA in papillary tumors than in urothelial infiltrating tumors, although the difference was not statistically significant (Table 1). No differences were observed for PSMA expression in relation to grade and stage.
In Fig. 2, we reported PSMA expression of a benign lesion and in different tumor samples at different stages, where only neovasculature-related PSMA expression was demonstrated (Fig. 2A–D). Figure 2D shows PSMA expression with a strong immunoreactivity of a high grade solid papillary carcinoma from a 78-year-old patient with high-grade urothelial carcinoma. Figure 3 reports the 68 Ga-PSMA-11 PET/CT of this patient.

Representative images of PSMA immunohistochemical stainings (40X magnification). (A) Chronic erosive cystitis negative for PSMA expression; (B) weak PSMA expression of transitional cells in a in situ lesion; (C) low grade papillary carcinoma showing a weak PSMA expression; (D) strong immunoreactivity of a high grade papillary carcinoma.

78-year-old patient with high-grade urothelial carcinoma. (A) and (B) Transaxial 68 Ga-PSMA-11 PET/CT fused and 68 Ga-PSMA-11 PET-only images showing focal high PSMA uptake at the site of the primary BCa (left bladder wall); (C) Transaxial contrast-enhanced CT image showing primary BCa enhancing lesion; (D) Maximum Intensity Projection (MIP) image of 68 Ga-PSMA-11 distribution in the pelvic area.
Discussion
The clinical management of patients with BCa is normally based on cytology and cystoscopy. These techniques are not 100% accurate in the diagnosis, localization and discriminating between low- and high-risk patients, indicating the need for companion biomarkers to be used in BCa clinical practice, even more they could serve as therapeutic target. Several molecular tests have been proposed and among them Fluorescence in situ hybridization (UroVysion, Abbott, Vysis) obtained FDA approval for the diagnosis and monitoring of BCa patients13. However, its use requires specialized personnel for the analysis and appropriate laboratory equipment. For these reasons, it is not feasible in all the laboratories and the search of new biomarkers is still ongoing.
Despite in vitro and in vivo studies have demonstrated PSMA expression in various malignant and benign tumors as promising biomarker, its role in BCa diagnosis and evolution has yet to be confirmed10,14,15. In fact, several studies reported that differences in PSMA expression in terms of cellular or tissue localization may depend on the type of antibody and platform used and sample analyzed. It has also been reported that other healthy and benign tissues different from prostate cancers display PSMA apical and cytoplasmic positivity, and PSMA expression is also observed in the neovasculature9,16,17. In the bladder, we demonstrated that PSMA is expressed exclusively in the neoformed vessels of carcinoma, even in in situ tumors, and it showed a weak expression in the vasculature of inflammatory/erosive benign lesions (chronic and erosive cystitis). These results are in accordance with literature data showing that PSMA is a marker of tumor associated neo-angiogenesis. These data could be useful in BCa diagnosis and could acquire even more importance in considering new therapeutic strategies, such as anti-angiogenesis agents and radio-labelled PSMA ligands.
Despite no differences have been observed on PSMA expression exclusively found in tumor neovasculature, in relation to tumor type, grade and stage, we found that PSMA expression, in terms of H-score was different between non tumor samples and tumor samples, reflecting the presence of a neoplasm. In addition, the high PSMA expression observed in the papillary tumors is in accordance with the fact that they are frequently accompanied by abundant fibrovascular supporting stroma. Moreover, the exuberant PSMA-positive neovascularization could be explained by the role of the gene FGFR3 and its mutations at the level of BCa cells, an indirect marker of tumor aggression implicated in the neo-angiogenesis process18,19.
We are aware of the retrospective nature of the study and of the limited number of analyzed cases, but this explorative work could thus form the basis for future research to assess the real diagnostic and prognostic value of PSMA on enlarged case series of samples of BCa.
Based on an immunohistochemical study showing PSMA expression in urothelial BCa, some authors hypothesized that PSMA expression in adenocarcinoma of the urinary bladder can be demonstrated in vivo using 68 Ga-PSMA-11PET/CT19. Both 18F-FDG and 68 Ga-PSMA-11 PET/CT were performed in a single patient, which showed PSMA expression both at the site of the primary BCa and in metastatic lymph nodes20. Similarly, in a 78-year-old patient with high-grade urothelial carcinoma (Fig. 3) we could observe high 68 Ga-PSMA-11 primary tumor uptake by PET, corresponding to high PSMA tumor expression on immunohistochemistry (Fig. 2D). These anecdotical experiences may suggest a role for 68 Ga-PSMA-11 PET/CT for in vivo detection of primary and metastatic BCa. Still, the high renal excretion and bladder accumulation of all 68 Ga-labeled PSMA ligands of clinical use greatly hamper primary urothelial detection due to the very low tumor neovasculature PSMA uptake compared to the considerable urinary PSMA activity background. The increasing, but still limited availability of 18F-labeled PSMA ligands with negligible urinary excretion such as 18F-PSMA-1007 and, more recently 18F-AlF-PSMA-11, provide better accuracy in the visualization of bladder wall lesions along with metastatic disease, where present. Thus, the in vivo confirmation of tumor neo-angiogenesis through 18F-PSMA-1007 PET could allow for more accurate pre-operative staging and lesion characterization.
In the clinical scenario of metastatic BCa patients, the verification of PSMA-expressing BCa lesions by either 68 Ga-PSMA or 18F-PSMA PET imaging would allow for the evaluation of eligibility for anti-angiogenic agents and PSMA radionuclide therapy. In this specific context, 68 Ga-PSMA-11 urinary excretion would not impede visualization of PSMA-avid metastatic disease. About PSMA radionuclide therapy, established PSMA theranostic tandems such as PSMA I&T and PSMA-617 (labeled with 68 Ga for diagnostic imaging and 177Lu for delivering targeted radiation therapy) could be investigated in BCa with future studies both as an alternative to maintenance endovesical treatments of superficial BCa and as a supplementary therapeutic option for metastatic BCa patients. We demonstrated by immunohistochemistry the presence of PSMA in the neovasculature of BCa and demonstrated positive targeting of PET-labeled PSMA ligand. In future the evaluation of tumor-retention time is needed to assess the appropriateness of long half-life therapeutic PSMA ligands as radionuclide treatment for BCa.
Methods
Case series
This retrospective study included BCa patients followed up at the Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (Italy) between 2009 and 2020.
Seventy-four patients were enrolled in the study and 87 BCa samples were analyzed. The study protocol was reviewed and approved by the Area Vasta Romagna Ethics Committee. Patients’ median age was 73 years (range 40–93). All diagnostic procedures and pathology analyses were carried out in accordance with the relevant guidelines and regulations, and written informed consent was obtained from all study participants. The histology and grading of 87 lesions were established by an expert pathologist at our hospital in accordance with the International Society of Urological Pathology (ISUP) Consensus Conference guidelines 421.
Immunohistochemistry
Immunostaining for PSMA expression was performed, as already described in our previous paper10, using the Ventana Benchmark Ultra staining system (Ventana Medical Systems, Tucson, AZ, USA) with Optiview DAB Detection Kit (Ventana Medical Systems). Tissue sections were incubated for 32 min with ready-to-use anti-PSMA antibody (SP29 Spring Bioscience, Pleasanton, CA, USA). Sections were automatically counterstained with hematoxylin II (Ventana Medical Systems). PCa and breast cancer tissues were used as positive and negative controls, respectively, in all of the experiments. Biomarker expression was quantified as the percentage of immunopositive tumor cells with membrane staining. Non-malignant tissue around the tumor, when present, was also evaluated for PSMA expression. Staining intensity (i.e. 0 absent, 1 weak, 2 moderate, 3 strong) was assessed to calculate the H-score, defined as the product of the percentage of the immunopositive tumor cells and the staining intensity. All samples were evaluated by 2 independent observers. Disagreement of > 10% positive cells was resolved by consensus after joint review using a multihead microscope.
Statistical analysis
Descriptive statistics are reported as median values and ranges. The normality of data distribution was assessed by Shapiro Wilk test. Since the data were not distributed in a normal way, the relationship between median PSMA expression values and pathology-based categories was evaluated by Mann–Whitney nonparametric test. All p-values were based on two-sided testing and values lower than 0.05 were considered statistically significant. Statistical analyses were performed using SAS statistical software version 14 (SAS Inc., Cary, NC, United States of America).
References
Bray, F. et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. https://doi.org/10.3322/caac.21492 (2018).
Radkiewicz, C. et al. Sex differences in urothelial bladder cancer survival. Clin. Genitourin. Cancer 18, 26-34.e6 (2020).
Kamat, A. M. et al. Bladder cancer. Lancet 388, 2796–2810 (2016).
Heck, M. M. et al. Molecular lymph node staging for bladder cancer patients undergoing radical cystectomy with pelvic lymph node dissection. Urol. Oncol. Semin. Orig. Investig. 38(639), e11-639.e19 (2020).
Hautmann, R. E., de Petriconi, R. C., Pfeiffer, C. & Volkmer, B. G. Radical cystectomy for urothelial carcinoma of the bladder without neoadjuvant or adjuvant therapy: long-term results in 1100 patients. Eur. Urol. 61, 1039–1047 (2012).
Madersbacher, S. et al. Radical cystectomy for bladder cancer today—a homogeneous series without neoadjuvant therapy. J. Clin. Oncol. 21, 690–696 (2003).
Heitkötter, B. et al. Expression of PSMA in tumor neovasculature of high grade sarcomas including synovial sarcoma, rhabdomyosarcoma, undifferentiated sarcoma and MPNST. Oncotarget 8, 4268–4276 (2017).
Schmidt, L. H. et al. Prostate specific membrane antigen (PSMA) expression in non-small cell lung cancer. PLoS ONE 12, e0186280 (2017).
S S Chang 1, V E Reuter, W D Heston, N H Bander, L S Grauer, P. B. G. Five different anti-prostate-specific membrane antigen (PSMA) antibodies confirm PSMA expression in tumor-associated neovasculature.
Bravaccini, S. et al. PSMA expression: a potential ally for the pathologist in prostate cancer diagnosis. Sci. Rep. 8, 4254 (2018).
Hope., T. ASCO 2020: Accuracy of 68Ga-PSMA-11 for Pelvic Nodal Metastasis Detection Prior to Radical Prostatectomy and Pelvic Lymph Node Dissection.
FDA approves first PSMA-targeted PET imaging drug for men with prostate cancer. News release. FDA. December 1, 2020. Accessed December 1, 2020. https://bit.ly/2Vo5esv.
Bravaccini, S. et al. Combining cytology, TRAP assay, and FISH analysis for the detection of bladder cancer in symptomatic patients. Ann. Oncol. 22, 2294–2298 (2011).
Ross, T., Ahmed, K., Raison, N., Challacombe, B. & Dasgupta, P. Clarifying the PSA grey zone: The management of patients with a borderline PSA. Int. J. Clin. Pract. 70, 950–959 (2016).
Ezenwa, E. V. et al. The value of percentage free prostate specific antigen (PSA) in the detection of prostate cancer among patients with intermediate levels of total PSA (4.0–10.0 ng/mL) in Nigeria. Arab. J. Urol. 10, 394–400 (2012).
Sam S Chang. Overview of prostate-specific membrane antigen.
Mhawech-Fauceglia, P. et al. Prostate-specific membrane antigen (PSMA) protein expression in normal and neoplastic tissues and its sensitivity and specificity in prostate adenocarcinoma: an immunohistochemical study using multiple tumour tissue microarray technique. Histopathology 50, 472–483 (2007).
Billerey, C. et al. Frequent FGFR3 mutations in papillary non-invasive bladder (pTa) tumors. Am. J. Pathol. https://doi.org/10.1016/S0002-9440(10)64665-2 (2001).
Guancial, E. A. et al. FGFR3 expression in primary and metastatic urothelial carcinoma of the bladder. Cancer Med. https://doi.org/10.1002/cam4.262 (2014).
Roy, S. G. et al. In vivo demonstration of PSMA expression in adenocarcinoma urinary bladder using 68Ga-PSMA 11 PET/CT. Clin. Nucl. Med. 42, 542–543 (2017).
Van Leenders, G. J. L. H. et al. The 2019 international society of urological pathology (ISUP) consensus conference on grading of prostatic carcinoma. Am. J. Surg. Pathol. https://doi.org/10.1097/PAS.0000000000001497 (2020).
Author information
Authors and Affiliations
Contributions
G.P., M.P. designed the study; M.M.T. performed the methodology and acquired the data, S.R. and M.M.T. analyzed and interpreted the data, G.P., F.M., M.C., M.M.T., S.B., S.R. wrote the manuscript, S.B., M.P., G.P., supervised the study. All authors provided final approval to publish and agree to be accountable for all aspects of the manuscript.
Corresponding author
Ethics declarations
Competing interests
Ugo De Giorgi received advisory board or consultant fees from Merck Sharp & Dohme, Bristol Myers Squibb, Janssen, Astellas, Sanofi, Bayer, Pfizer, Ipsen, Novartis, Pharmamar and Institutional research grant from Astrazeneca, Sanofi, Roche. All other authors have no conflicts of interest to declare.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tumedei, M.M., Ravaioli, S., Matteucci, F. et al. Spotlight on PSMA as a new theranostic biomarker for bladder cancer. Sci Rep 11, 9777 (2021). https://doi.org/10.1038/s41598-021-89160-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-89160-0
- Springer Nature Limited