
Abstract
Several studies have documented the burden and risk factors associated with diarrhoea in low and middle-income countries (LMIC). To the best of our knowledge, the contextual and compositional factors associated with diarrhoea across LMIC were poorly operationalized, explored and understood in these studies. We investigated multilevel risk factors associated with diarrhoea among under-five children in LMIC. We analysed diarrhoea-related information of 796,150 under-five children (Level 1) nested within 63,378 neighbourhoods (Level 2) from 57 LMIC (Level 3) using the latest data from cross-sectional and nationally representative Demographic Health Survey conducted between 2010 and 2018. We used multivariable hierarchical Bayesian logistic regression models for data analysis. The overall prevalence of diarrhoea was 14.4% (95% confidence interval 14.2–14.7) ranging from 3.8% in Armenia to 31.4% in Yemen. The odds of diarrhoea was highest among male children, infants, having small birth weights, households in poorer wealth quintiles, children whose mothers had only primary education, and children who had no access to media. Children from neighbourhoods with high illiteracy [adjusted odds ratio (aOR) = 1.07, 95% credible interval (CrI) 1.04–1.10] rates were more likely to have diarrhoea. At the country-level, the odds of diarrhoea nearly doubled (aOR = 1.88, 95% CrI 1.23–2.83) and tripled (aOR = 2.66, 95% CrI 1.65–3.89) among children from countries with middle and lowest human development index respectively. Diarrhoea remains a major health challenge among under-five children in most LMIC. We identified diverse individual-level, community-level and national-level factors associated with the development of diarrhoea among under-five children in these countries and disentangled the associated contextual risk factors from the compositional risk factors. Our findings underscore the need to revitalize existing policies on child and maternal health and implement interventions to prevent diarrhoea at the individual-, community- and societal-levels. The current study showed how the drive to the attainment of SDGs 1, 2, 4, 6 and 10 will enhance the attainment of SDG 3.
Similar content being viewed by others


Introduction
Despite killing over 2000 children every day—more than AIDS, malaria, and measles combined, diarrhoea received less attention from child health programmers and funders compared with other child killer diseases1,2. In 2015, there were an estimated 2.3 billion diarrhoea-related illnesses of which 1.3 million deaths occurred globally with about half a million diarrhoea-related deaths among under-five children annually3,4. Under-five mortality is a core indicator of the overall wellbeing of a society and a measure of the progress made by societies in healthcare system and management5,6. In 2015, there were nearly 6 million under-five mortalities including 45% neonatal deaths7 of which about 90% were in sub-Saharan Africa and South Asia8. The disproportionate ratio of 73.1–5.3 under-five deaths per 1000 live births in the low-income countries and high-income countries respectively is a source of concern9. Effective interventions such as prevention and control of childhood diseases, enhanced health care programmes, effective and efficient provision and utilization of health care facilities including adequate and timely immunization and vaccination are very essential to reduce under-five mortalities5,6.
Although remarkable progress has been reported in the reduction of under-five mortality and morbidities globally8,10,11,12, childhood diarrhoea remains major public, clinical and social health challenges in the Low- and Middle-Income Countries (LMIC)3. There have been differences but a close ranking of diarrhoea burden among these countries in the literature. While Gill et al. reported that diarrhoea disease is the 9th leading cause of death globally but 4th among children under-5 years13, the ranks were 8th and 5th respectively in a Global Burden of Disease (GBD) study14. About nine of every annual global diarrhoea-related deaths among under-five children occurs in Sub-Saharan Africa and South Asia3,15. Worse still, the survivors of diarrhoea are faced with a long-time higher risk of growth faltering, ill health, stunting, and cognitive impairment16,17.
Diarrhoea diseases have continued to cause monumental morbidity and mortality in developing countries3. With a reported 15% of global deaths among children under-5 years attributable to diarrhoea4,10,11,15, it remains one of the topmost children killers in LMIC8,10,12,18,19,20,21. The findings of Mokomane et al. corroborated the GBD and WHO assertions that acute diarrhoea disease is one of the topmost causes of global morbidity and mortality particularly among young children in resource-constrained countries17. The burden of diarrhoea is much higher in LMIC than in the high-income countries10,14,22,23 with worst hits in the South Asia and sub-Saharan Africa regions, both having 52% of all the burden24. This is quite plausible as these regions constitute the majority of LMIC. Also, researchers were unanimous that diarrhoea is caused by a diverse range of aetiological agents, inclusive of bacterial enteritis which is very common in LMIC16,17,25.
Global efforts have been made to strengthen health systems in every country to offer interventions that could prevent diarrhoea and save the lives of several millions of children. Among several efforts to combat diarrhoea is the pronouncement of the Sustainable Development Goal (SDG)-3 which focused on ensuring healthy lives and promoting the well-being of all, with specific target 3.2 to end preventable deaths of children under 5 years of age by 2030, and drastic reduction of neonatal and under-five mortalities to at least as low as 12 and 25 per 1000 live births respectively in all countries26. Also, a study coordinated by WHO and UNICEF, developed the Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea27. The group established plans to reduce the severe incidence and deaths due to diarrhoea in children by 202514. Several other national and local interventions have been made in different countries to alter the tides in diarrhoea10,18. The central aim of these interventions is to increase life expectancy with a reduction in widespread diseases associated with early mortality6.
These efforts notwithstanding, the incidence of diarrhoea and diarrhoea-related under-five mortality remains a major challenge in most LMIC. It is worth noting that although improvements in the standard of living, advances in sanitation, water treatment and food safety awareness have brought about a reduction in the total global deaths due to diarrhoea, the morbidity from diarrhoea have remained exceptionally high and has accounted for substantial economic and societal losses17. Of greater concern is that there may be a rebound in the upsurge of diarrhoea-associated mortality in the nearest future due to increasing diarrhoea-related morbidity, urbanization, global warming and climate change17,28,29. Besides, prolonged episodes of diarrhoea have been linked to significant comorbidities and has put children at risk of a vicious cycle of diarrhoea and malnutrition30.
There is, therefore, an urgent need to assess the risk factors central to most LMIC as a critical step in the potential reworking of intervention strategies to reduce the incidence of diarrhoea among under-five children. Literature is replete with the fact that WASH factors (presence of a domesticated animal in the house, having animal shed in proximity to the household, use of cow dung in household and open field defecation), maternal age and education, household wealth quintile, child age, sex, birth weight, birth order, household wealth quintile and location of the resident are associated with the experience of diarrhoea among under-five children10,17,20,31,32. These studies have established a pathway between the factors and diarrhoea diseases. This study, therefore, reported the prevalence of diarrhoea among under-5 year children in 57 LMIC. The study also identified the individual-specific factors, neighbourhood factors and country-level factors that affect the occurrence of diarrhoea among under-five children in the 57 LMIC using hierarchical Bayesian logistic regression models.
Methods
Study design and data
The cross-sectional and nationally representative Demographic and Health Surveys (DHS) data collected during household surveys across most LMIC were used for this study. We extracted and pooled the latest recoded “children data” from the DHS that collected information on diarrhoea, conducted between 2010 and 2018 and available in the DHS data domain by March 2019. Only 57 LMIC met these criteria and were included in this study. The DHS uses a multi-stage, stratified sampling design with households as the sampling unit33,34. However, due to differences in the administrative levels in different countries, the number of sampling stages differed. Country-specific sampling methodologies are available at dhsprogram.com and in the country-specific reports35,36,37. Sampling weights were computed and provided alongside the data from each country by DHS and were applied to our analysis. The sampling weights were based on the multi-stage sampling procedures to ensure representation of the general population. All the DHS questionnaires were standardized and implemented across all countries with similar interviewer training, supervision, and implementation protocols.
Data source
The secondary data used for this study is available on request from the owners of the data at https://www.dhsprogram.com/data/dataset_admin/login_main.cfm.
Dependent variable
Our dependent variable is diarrhoea. Firstly, women were asked to name all births they had within 5 years before the survey dates. They were then asked if any of the children had at least an episode of diarrhoea within 2 weeks preceding the survey date. The response is binary with children who had diarrhoea coded as “1” and “0” otherwise.
Independent variables
We used three categories of explanatory variables.
Individual-level factors
Sex of the children (male versus female), children age (< 12 months (infants) and 12–59 months), household head sex (male or female), mothers’ age (15–24, 25–34, 35–49 years), mothers’ highest education (none, primary, secondary or higher); marital status (never, currently or formerly married), employment status (currently employed or not), access to media (yes or no), sources of drinking water (improved or unimproved), toilet type (improved or unimproved), house building material (improved or unimproved), cooking fuel (clean or unclean), weight at birth (average+, small or very small birth weight), and birth order (1, 2, 3 and 4+). These variables have been linked with diarrhoea in the literature10,17,20,31,32. We used the DHS wealth index as a proxy indicator for socioeconomic status. The methods used in computing the DHS wealth index have been described in the literature38 as depicted in Fig. 1.

The hierarchical structure of the source data (Authors’ drawings using World Map39).
Neighbourhood-level factors
In this study, the terms “neighbourhood” and “community”, were used to describe clustering of children within the same geographical living environment6,40,41. Neighbours are the children that share the same Primary Sample Unit (PSU) within the DHS data. The PSUs were identified using the most recent census in each country where DHS was carried out40,42. The neighbourhood-level factors included in the current study are the place of residence (rural or urban), neighbourhood poverty-, illiteracy- and unemployment levels as illustrated in Fig. 1. The neighbourhood poverty-, illiteracy- and unemployment levels were computed as the proportion of children from households in the lowest two wealth quintiles, children whose mother has no former education and children whose mother was unemployed respectively within each country as of the survey time. We categorized these neighbourhood factors into two levels (low and high) each using the 50th percentile cut-off to allow for non-linear effects and offer useful results for policy decisions. Similar procedures have been used in previous studies40,42.
Country-level factors
We retrieved the country-level data from the human index reports published by the United Nations database43,44. The Human Development Index (HDI) was created by the United Nations to emphasize “that people and their capabilities should be the ultimate criteria for assessing the development of a country, not economic growth alone”45. The HDI summarizes the average achievement of countries in three key dimensions of human development: “a long and healthy life, access to knowledge and a decent standard of living”45. We categorized the countries into the lowest, middle and highest HDI as shown in Fig. 1. We also explored other country-level factors such as country’s rural area percentages (a measure of the proportion of a countries population that resides in rural areas), multidimensional poverty index (a measure of acute multidimensional poverty) and intensity of deprivation (a measure of the average percentage of deprivation experienced by people in multidimensional poverty)43,44,45. These variables were used for the descriptive statistics but were excluded from the regression models as they correlated with HDI.
Analytical procedures
We used descriptive statistics to show the distribution of the children by country and by the dependent and independent variables in percentages. Chi-square test of association was used to determine the significance of the association between the independent variables and diarrhoea (Table 1). For the country-level data, we applied sampling weights (SW) provided by the DHS to adjust for unequal cluster sizes, stratifications and to ensure that our findings adequately represent the target population for each country. However, for the pooled data, we computed and applied country-women weights (CWW) to the analysis to reflect the differences in population sizes of the women in each country. The CWW is the product of SW and country-specific weights (CSW). We computed the CSW as the number of sampled women aged 15–49 years divided by the population of women aged 15–49 years for each country. While the number of sampled women is available in the dataset, we obtained the population of each country from United Nations population prospects46. We checked multicollinearity among the independent variables using the “colin” command in Stata version 16. The command provided the variance inflation factor (VIF). All variables with VIF > 2.5 were removed from the regression analysis as literature has shown concerns about VIF > 2.547. Statistical significance was set to 0.05. All analysis was conducted in Stata version 16.
Modelling approaches
The multivariable multilevel logistic regression models were used to identify if an association exists between the individual, community contextual factors and national compositional factors and diarrhoea. Using all the 3-level model for binary response specified above, with children i who had diarrhoea (at level 1), from a neighbourhood j (at level 2), and living in a country k (at level 3) as shown in Fig. 1, we identified, constructed and assessed five models to arrive at a robust model that will help identify risk factors of diarrhoea considering the multi-level structure of the data. The models are based on a hierarchical logistic regression model with mixed outcomes consisting of the fixed and random parts as shown in Eq. (1).
The probability that a child \(i\) of neighbourhood \(j\) from country \(k\) had diarrhoea is denoted by \({\pi }_{ijk}\). The “logit” is the logistic function computed as \(logit\left({\pi }_{ijk}\right)=log\left(\frac{{\pi }_{ijk}}{1-{\pi }_{ijk}}\right)\), \({\beta }_{0}\) is the intercept, \({\beta }_{p}\) is the regression coefficient for the \(p\) parameters, \({X}_{pijk}\) are the covariates, \({U}_{0jk}\) is the random components due collectively to all children from neighbourhood \(j\) of country \(k\) while \({V}_{0k}\) is the random components due collectively to all children from country \(k\). The mixed model enables detailed exploration of variation in variables between higher-level units (contextual heterogeneity).
We developed five distinct models to enable a detailed assessment of different combinations of factors to select the most robust model that could identify the contextual and compositional risk factors of diarrhoea. This was aimed at modelling the compositional factors and contextual factors separately and collectively, with reference to the distinct multi-level structure of the data used for the analysis. The first model was the null model (Model I) to assess the variation due to the neighbourhood and country-specific random effects without any explanatory variable. It decomposed the magnitude of variance that existed between country and neighbourhood levels. The second model (Model II) included only the individual-level variables conditional on the neighbourhood and country-specific random effects. The third model (Model III) included only the neighbourhood level variables conditional on the neighbourhood and country-specific random effects. The fourth model (Model IV) examined the country-level variables conditional on the neighbourhood and country-specific random effects, while the final model (Model V), estimated the odds of individual, neighbourhood and country-level variables conditional on the neighbourhood and country-specific random effects. All the models were executed using the multilevel regression model of the MLwinN software, version 3.03 embedded in Stata version 1548. Parameters were estimated using the Bayesian Markov Chain Monte Carlo (MCMC) procedures49 with the following specifications: distribution: binomial; link: logit, burning: 5000, chain: 50,000 and refresh: 500.
Fixed effects (measures of association)
We reported the results of the fixed effects (measures of association) as the odds ratios (ORs) with their 95% credible intervals (CrIs). Rather than the usual 95% confidence intervals (95% CI) obtained in the frequentist approaches, the Bayesian statistical inference allowed us to summarize probability distributions for measures of association alongside the 95% CrI. The 95% credible interval is simply interpretable as “the 95% probability that the population parameter takes a value in a particular range”.
Random effects (measures of variation)
In addition to the fixed effects, we also measured the likely effects of the factors considered across the three different levels using the Intraclass Correlation (ICC) and median odds ratio (MOR). The ICC is the measure of the similarity among children living in the same neighbourhood and within the same country. The ICC is a measure of clustering of odds of having diarrhoea in the same neighbourhood and the same country. We calculated the ICC using the linear threshold, which is the latent variable method50. Adopting the methods recommended by Larsen et. al. on neighbourhood effects51, we reported the random effects in terms of the odds. The MORs are the measures of the variance of the odds ratio in higher levels (neighbourhood and country levels) and it estimates the probability of having diarrhoea that can be attributed to any of the neighbourhood and country factors. If MOR = 1, there is no neighbourhood or country variance. Conversely, the higher the MOR, the more significant are the contextual effects for understanding the probability of developing diarrhoea. A similar approach has been used in similar settings in the literature52,53.
Ethics approval and consent to participate
This study was based on an analysis of secondary data with all identifier information removed. The Institutional Review Board (IRB) of Inner City Fund (ICF) International Macro at Fairfax, Virginia in the USA reviewed and approved the MEASURE Demographic and Health Surveys Project Phase III. The 2010–2018 DHS’s are categorized under that approval. The Institutional Review Board (IRB) of Inner City Fund (ICF) International Macro complied with the United States Department of Health and Human Services Services guidelines and requirements for the “Protection of Human Subjects” (45 CFR 46). All protocols were carried out in accordance with relevant guidelines and regulations on confidentiality, benevolence, non-maleficience and informed consent. All study participants gave written informed consent before participation and all information was collected confidentially. DHS Program has remained consistent with confidentiality and informed consent over the years. ICF Macro ensures compliance with the U.S. Department of Health and Human Services regulations for the respect of human subjects. The authors sought and obtained express approval to use the data from ICF Macro with Accession number 140625. No further approval was required for this study. The data owners can be contacted at thedhsprogram@gmail.com and data can be found at https://www.dhsprogram.com/data/dataset_admin/login_main.cfm. Further documentations on ethical issues relating to the surveys are available at http://dhsprogram.com.
Patient and public involvement
No patients were involved in the design or dissemination of this analysis.
Results
Sample characteristics
In Table 1, we present the distribution of under-five children studied and the weighted prevalence of diarrhoea by the countries, the regions of the world, year of data collection, and the numbers of neighbourhoods per each country. The median number of neighbourhoods per country sampled was 555, ranging from 252 in Comoros to 28,321 in India.
Measurement of the prevalence of Diarrhoea, special and common cause variations
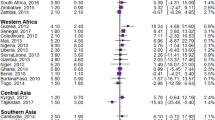
As shown in Table 1, Figs. 2 and 3, we found a wide variation in the prevalence of diarrhoea across the countries. The overall prevalence of diarrhoea was 14.4% (95% confidence interval (CI) 14.2–14.7%) ranging from 3.8% (95% CI 2.9–4.7%) in Armenia to 31.4% (95% CI 30.7–32.1%] in Yemen. Considering the regions of the world, the lowest prevalence was found in South Europe (6.1%, 95% CI 5.2–7.0%) while the highest was in Western Asia at 21.8%. The funnel plot in Fig. 3 showed that only 10(17.5%) countries within the 99% control limits, indicating common-cause variation. Twenty-two (38.6%) countries were above the upper control limit and 25 (43.9%) countries were below the lower control limit, indicating special-cause variation (Fig. 3).

Prevalence of diarrhoea by countries (DHS 2010–2018).

Funnel plot showing common- and special-cause variations in the prevalence of diarrhoea in LMIC (DHS 2010–2018).
Children individual-level, neighbourhood-level and country-level characteristics
The descriptive statistics by selected individual level, neighbourhood level and country-level characteristics are listed in Table 2. About a fifth (21%) of the children were infants, about half were males (51%) and most of their mothers were aged 25–34 years (52%). A third (32%) of the mothers had no formal education and 43% had at least secondary education while only 17% belong to households in the richest wealth quintiles. Most of the mothers were currently employed (59%) and 81% were from male-headed households. Most (79%) of the children had drinking water from improved sources, only 45% had access to improved toilet types, 72% are from households that use unclean (biomass) cooking gas and only 10% are from a household whose floor, roof and wall materials are all improved.
On the neighbourhood-level factors, 66% of the children lived in rural areas, 49% from communities with high poverty rate, 50% and 57% were from communities with high illiteracy rate, and high unemployment rate respectively. Three-fifths (59%) of the children are from countries with a high level of intensity of deprivation and 44%, 42% and 14% from countries with the lowest, middle and high HDI respectively. All the variables considered at the individual-, neighbourhood- and county-levels were significantly associated with diarrhoea in a Chi-square test and the bivariate logistic regression models between each of the explanatory variables and diarrhoea. Hence, all the variables were candidates in the multivariable models.
Measures of associations (fixed effects) of having Diarrhoea
Table 3 presents the outputs of each of the different models explored in this study. In the fully adjusted model (Model V) wherein we controlled for the effects of the individual-, neighbourhood- and country-level factors, children age, children sex, mothers educational attainment, mothers age, employment status, media access, sources of drinking water, toilet type, marital status, housing material, cooking fuel type, weight at birth, birth order, place of residence (rural or urban), neighbourhood poverty-, illiteracy- and unemployment rates, as well as HDI were significantly associated with odds of diarrhoea.
The adjusted odds of diarrhoea was 29% higher among infants than those aged 12–59 months (adjusted odds ratio (aOR) = 1.29, 95% CrI 1.26–1.31). Male children were more likely to have diarrhoea (aOR = 1.11, 95% CrI 1.09–1.12). The odds of diarrhoea was also higher among children whose mothers were aged 15–24 and 25–34 years compared with children whose mothers were aged 35–49 years (15–24: aOR = 1.70; 95% CrI 1.65–1.75 and 25–34: aOR = 1.235; 95% CrI 1.20–1.25). The odds of diarrhoea was significantly less likely among children with no maternal education than the children whose mothers have at least secondary education (aOR = 0.95; 95% CrI 0.92–0.97). Children from households in the poorest wealth quintiles were 23% more likely to have diarrhoea than those from households in the uppermost wealth quintiles (aOR = 1.23, 95% CrI 1.18–1.27). Children whose mothers were unemployed had higher (9%) odds of diarrhoea (aOR = 1.09; 95% CrI 1.07–1.11). Inaccessibility to media increased the odds of diarrhoea by 4% (aOR = 1.04; 95% CrI 1.02–1.06). The odds of diarrhoea was 37% and 18% higher among children who had very small (aOR = 1.37; 95% CrI 1.32–1.42) and small (aOR = 1.18; 95% CrI 1.16–1.21) birth weight respectively than those that had average or bigger birth weights. The odds of diarrhoea was 5% higher in rural areas than in urban areas (aOR 1.05; 95% CrI 1.03–1.08). Children from neighbourhoods with high illiteracy (aOR = 1.07, 95% CrI 1.04–1.10) rates were more likely to have diarrhoea than those from neighbourhoods with low illiteracy rate. At the country-level, the odds of diarrhoea nearly doubled (aOR = 1.88, 95% CrI 1.23–2.83) and tripled (aOR = 2.66, 95% CrI 1.65–3.89) among children from countries with middle and lowest HDI respectively compared with those from highest HDI countries.
Measures of variations (random effects) of having Diarrhoea
Model I (the null model), showed that there was a significant variation in the odds of developing diarrhoea across the countries (σ2 = 0.30, 95% CrI 0.21–0.44) and across the neighbourhoods (σ2 = 0.51, 95% CrI 0.49–0.53). On the assessment of the intra-country and intra-neighbourhood correlation coefficient, 7.4% and 19.8% of the variance in odds of having diarrhoea could be attributed to the country- and neighbourhood-level factors, respectively. The median odds ratio (MOR) in the nested model (Model V) confirmed evidence of neighbourhood (1.57) and societal contextual (1.97) phenomena shaping the distribution of diarrhoea among under-five children as shown in Table 3. Model V revealed significant variation in the odds of developing diarrhoea across both the neighbourhoods (σ2 = 0.50, 95% CrI 0.49–0.52) and the countries (σ2 = 0.22, 95% CrI 0.15–0.33). Going by Model V, 6% of all variability in having diarrhoea was explained by the countries from which the children live compared with 22% explained by their neighbourhood differences.
Discussion
Using the information provided by parents and guardians of 796,150 under-five children from 57 LMIC, we explored the factors associated with the experience of at least one episode of diarrhoea within 2 weeks preceding the survey dates in each of the countries. The proportion of children who experienced diarrhoea varied widely across the 57 countries from 4% in Armenia to 29% in Afghanistan. Our major finding is that factors that predispose children to diarrhoea are diverse and complex. The factors are made up of individual cum household, neighbourhood and country-level factors. These characteristics formed distinct blocks of compositional and contextual factors associated with diarrhoea. The compositional factors include being an infant, males, from female-headed households, mother aged < 35 years, mother had primary education, unemployed, mother never married, from a household in the lower wealth quintiles, and no media access to be at higher odds of diarrhoea. Other significant compositional factors include drinking water from unimproved sources, uses unimproved toilet types, small weight at birth, high birth orders. The contextual factors are residing in rural areas, from communities with high poverty, illiteracy and unemployment rates and from countries with the lowest and middle HDI.
We found diarrhoea episodes to be commoner among infants than the older under-five children. This is consistent with existing findings in the literature1,17,23,31,32,54 and could be attributed to more fragile anatomy of infants as well as the exclusiveness of breastfeeding14. Particular attention should be paid to the prevention of diarrhoea among infants as the higher cases among them has been linked with higher fatalities than among the older children55. We also found higher odds of having diarrhoea among male children compared with their female counterparts. Similar differences have been identified in the literature23 but at variance to the findings of Tetteh et al. that diarrhoea was higher among female children56.
The odds of having diarrhoea reduced with increments in mothers’ age. The odds were higher among children whose mothers were aged 15–24 years and 25–34 years compared with those born to women aged 35–49 years. Similar findings have been reported in the literature57,58. These differences may not be unconnected with the fact that teenage and young adult motherhood comes with its challenges including neglect, limited resources and the likelihood of contracting diseases by both the young mothers and their children59. Also, it is not unlikely that older mothers are more experienced in preventing diarrhoea among under-five children. Therefore, age-specific intervention could be designed to prioritise the younger mothers.
Educational attainment among mothers has been associated with childhood diseases including diarrhoea60. Our findings generally suggested that children from mothers with limited educational attainment are more likely to have diarrhoea as corroborated in the literature10,30,32,57,60,61. The differences were more distinct among children whose mothers had only primary and those that had secondary or higher education. This is a clear indication that other factors interact with women education in the likelihood of children having diarrhoea. Education alone may be insufficient in preventing diarrhoea, factors such as household wealth status, access to media, hygiene and sanitation, good water, rural–urban residential, women age etc. are also important in the prevention of diarrhoea. For instance, higher educational attainment is associated with a better awareness of health education including knowledge and guidelines on sanitation, hygiene, feeding and weaning practices etc60.
The wealth status of the households to which the children belong appeared to have played a dominant and consistent role in whether a child experience diarrhoea or not across the LMIC studied. Our findings are in agreement with earlier reports31,60,61. There were linear increments in the odds of having diarrhoea from those in households in the poorest wealth quintile compared to those in the richest wealth quintile. The likelihood of diarrhoea was generally 23% higher among children from households in the poorest wealth quintiles than those in the richest wealth quintile. The role of wealth, or at least purchasing power, in the knowledge and utilization of health care services, and by extension, in health outcomes, have been documented62. Fagbamigbe et al. reported that women from a household in higher wealth quintiles have a higher likelihood of health care utilization in Nigeria62. Wealth is a vital tool in gaining access to media, good sanitation and hygiene, clean cooking fuel etc. To prevent diarrhoea in LMIC, there is a need to enhance the means of livelihood and alleviate poverty among mothers generally since most people in these countries currently live below $2 per day43. Livelihood enhancement and poverty alleviation strategies could include employments and better education.
In the current study, we identified access to improved sources of drinking water, use of improved toilet types, use of improved housing materials (floor, wall and roof) and use of clean cooking fuel in households to have lowered the odds of diarrhoea in LMIC. As noted by Fagbamigbe et al., poor hygiene and sanitation including the use of unimproved toilets and water sources have a direct pathway to diarrhoea20. We could not assess the effect of “use of soap for hand hand-washing before meals and meals preparation” in this study because the information was not available for most countries. Nonetheless, our result is corroborated with findings from other studies, where diarrhoea have been linked with hygiene, water and sanitation1,10,54,60,63,64. Adequate practice and maintenance of good sanitation, hygiene etc. can reduce the risk of diarrhoea. Efforts should be made to enhance the knowledge and capacity of women and households, in general, to maintain good sanitation and hygiene in addition to the use of improved housing materials and access to safe drinking water.
Health promotion and education on the prevention of diarrhoea are often disseminated through media such as radio, television and newspaper. Access to media on diarrhoea prevention has an indirect link to diarrhoea occurrences. Media access improves knowledge about diarrhoea, which in turn enhances preventive and management practices65. We identified that the children whose mothers had no access to at least one of these media sources had higher odds of developing diarrhoea. This finding is consistent with what has been reported in the literature22,66. However, access to media could be limited by educational attainment, household wealth status and availability of social infrastructures such as electricity which is lacking in most households and communities across the LMIC. Besides media, there may be a need to reach the mothers directly through local postnatal providers and peer education.
Also, children with low birth weights had higher odds of developing diarrhoea compared with those that normal birth weights as reported by Bado et al.54. Greater attention should be paid to the health needs and challenges of children with low birth weights to reduce their chances of developing diarrhoea and other childhood diseases. Children with low birth weight are more susceptible to morbidities and mortality. Therefore, it has a causal pathway to diarrhoea. Using birth order as a proxy for the current family size, we found that the odds of having diarrhoea increased consistently with the increase in the birth order of the children. The prevalence rose from 8 to 18% to 32% among those with 2nd, 3rd and 4th or higher birth orders respectively compared with the children who were first births. Similar findings that diarrhoea is commoner among children in large households have been reported1,61. This is plausible as larger households can overstretch the limited resources at their disposals. More so, larger family size has been reported to be commoner among households in lower wealth quintiles67. This further corroborates our finding on the association between poverty and diarrhoea.
On the contextual factors, we found higher odds of diarrhoea in the rural area compared with the urban areas as reported previously66,68 but at variance with an Ethiopian study which reported higher odds in urban areas10. Also, children from communities with high deprivations in terms of high poverty, illiteracy and unemployment rates had a higher likelihood of experiencing diarrhoea episode compared with the other children from advantaged communities10,69. These contradictions could be ascribed to the specifics of each rural and urban areas. For instance, Kenya has a large slum within its capital city, Nairobi. Diarrhoea experience in such slums with high population density within urban areas could be higher than in rural areas with better and cleaner natural sources70,71.
In a similar pattern, children from countries with the lowest and middle HDI have higher odds of having diarrhoea than those from countries with the highest HDI. Of all the factors considered in this study, countries’ HDI levels presented the highest odds of diarrhoea. While the odds of diarrhoea nearly doubled among children from countries in the middle HDI, it nearly tripled among those from countries having the lowest HDI. This clearly showed that there are country-level contextual factors and other compositional factors that predispose children to diarrhoea. Our finding aligns with previous findings of Mokomane et al. and Ahs et al.17,22.
Our findings provide evidence of wide variations in the development of diarrhoea within and across the LMIC. The dis-advantaged communities (those with a high rate of unemployment, illiteracy, poverty) and countries (those lowest human capital development index) are the worst hit by diarrhoea. Efforts should be made to increase the overall well-being of every community as children from more deprived communities, irrespective of the differences in their compositional factors, all have higher odds of having diarrhoea than their peers from better-off communities. Enhancing the development of LMIC in all spheres will sustain human progress, reduce vulnerabilities and build resilience. As pointed out in earlier reports, there are needs for efficient and effective interventions to guide strategies to target risk factors unique to communities and countries14. The implications of the findings of this study for clinical practices is that clinical practices alone may be insufficient in reducing diarrhoea incidences. Besides adequate platform to manage diarrhoea cases clinically, mothers’ and community-level characteristics should be considered in designing strategies to reduce diarrhoea episodes among children. The identified contextual and compositional factors in this study are “modifiable” as far as diarrhoea preventive interventions are concerned. Through appropriate intervention, the factors could be explored as a means of reducing the occurrence of diarrhoea among under-five children in LMIC.
Study limitation
The data used for this study relied on mothers and guardians/caregivers recall of diarrhoea episodes among their under-five children. This might have introduced a recall bias through underreporting or over-reporting of the cases. However, DHS has incorporated check and control mechanisms to ensure the accuracy of data collected across the countries. Therefore, the recall bias posed no threat to the reliability of our estimates. The cross-sectional nature of the data prevented causal inferences. Nonetheless, the associations established with the risk factors is suitable to design intervention strategies. Also, the secondary nature of the data has limited our choice of community-level independent factors but we were able to generate quality community-level variables to identify the contextual factors. Besides, we have used only quantitative data, availability of qualitative data could have helped dissected the contextual and compositional factors better. These limitations could be addressed by collecting primary data that includes both quantitative and qualitative data. The use of nationally representative data with proven data reliability and integrity have given credence to the reliability of our findings. The strength of our study lies in its ability to pool the diarrhoea experience of about three-quarters of a million children from 57 countries to arrive at our estimates and conclusions.
Conclusion
Diarrhoea remains a major problem in most LMIC studied. We identified diverse individual-level, community-level and national-level factors associated with the development of diarrhoea among under-five children in these countries. In all, we found the highest odds of diarrhoea among the poorest children from the less-advantaged communities within countries with the lowest human development index. Thus, there is a need to reduce the incidence and prevalence of diarrhoea among under-5 year children to forestall a possible/likely rebound in the upsurge of diarrhoea-associated mortality in the nearest future.
Recommendations
There is a need to reinforce diarrhoea prevention and control program at all levels-community, national and global—across the low and middle-income countries to reduce the chances of an under-five child developing diarrhoea. In particular, interventions should include community-level health education and promotion on ways to avert diarrhoea incidences are the best measures to reduce its occurrences. Poverty alleviation through gainful employment and better education among women remains the gateway to necessary information on strategies to guide against diarrhoea. To achieve a meaningful reduction in the prevalence of diarrhoea, there may be a need to involve community and religion leaders to influence communal behaviour and practices that could enhance overall community sanitation.
Data availability
The data supporting this article is available at http://dhsprogram.com on request from the owners of the data.
Abbreviations
- CI:
-
Confidence interval
- CrI:
-
Credible interval
- CSW:
-
Country specific weights
- CWW:
-
Country-women weights
- DHS:
-
Demographic and health survey
- GBD:
-
Global burden of disease
- HDI:
-
Human development index
- ICC:
-
Intraclass correlation
- ICF:
-
Inner city fund
- IRB:
-
Institutional Review Board
- LMIC:
-
Low- and middle-income countries
- MCMC:
-
Markov chain Monte Carlo
- MOR:
-
Median odds ratio
- PSU:
-
Primary sample unit
- SES:
-
Socioeconomic status
- SDGs:
-
Sustainable development goals
- SW:
-
Sampling weights
- UNICEF:
-
United Nations International Children’s Emergency Fund
- VIF:
-
Variance inflation factor
- WHO:
-
World Health Organization
References
Tambe, A. B., Nzefa, L. D. & Nicoline, N. A. Childhood diarrhea determinants in Sub-Saharan Africa: A cross sectional study of Tiko-Cameroon. Challenges 6, 229–243 (2015).
CDC. Diarrhea: Common Illness, Global Killer. Global Diarrhea Burden|Global Water, Sanitation and Hygiene|Healthy Water. 2019. p. 1. https://www.cdc.gov/healthywater/global/diarrhea-burden.html.
Kotloff, K. L. The burden and etiology of diarrheal illness in developing countries. Pediatr. Clin. NA 64, 799–814. https://doi.org/10.1016/j.pcl.2017.03.006 (2017).
GBD (2015) Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1545–1602 (2016).
Abir, T., Agho, K. E. & Page, A. N. Risk factors for under-5 mortality: Evidence from Bangladesh demographic and health survey, 2004–2011. BMJ Open 5(1), e006722. https://doi.org/10.1136/bmjopen-2014-006722 (2015).
Yaya, S., Uthman, O. A., Okonofua, F. & Bishwajit, G. Decomposing the rural-urban gap in the factors of under-five mortality in sub-Saharan Africa? Evidence from 35 countries. BMC Public Health 19(1), 1–10 (2019).
Liu, L. et al. Global, regional, and national causes of under-5 mortality in 2000–2015: An updated systematic analysis with implications for the sustainable development goals. Lancet 388(10063), 3027–3035. https://doi.org/10.1016/s0140-6736(16)31593-8 (2016).
World Health Organization. Children: Reducing mortality fact sheet. 2017. http://www.who.int/mediacentre/factsheets/fs178/en/.
World Health Organization. Global Health Observatory (GHO) data under-five mortality. 2019. https://www.who.int/gho/child_health/mortality/mortality_under_five_text/en/.
Alebel, A. et al. Prevalence and determinants of diarrhea among under-five children in Ethiopia: A systematic review and meta-analysis. PLoS One 13(6), e0199684. https://doi.org/10.1371/journal.pone.0199684 (2018).
Lomazzi, M., Borisch, B. & Laaser, U. The millennium development goals: Experiences, achievements and what’s next?. Glob. Action 7(1), 23695 (2014).
Liu, L. et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 385(9966), 430–440. https://doi.org/10.1016/s0140-6736(16)31593-8 (2015).
Gill, C. J., Thea, D. M. & Hibberd, P. Diarrhoeal disease trends in the GBD 2015 study: Optimism tempered by scepticism. Lancet Infect. Dis. 17(9), 884–885 (2017).
GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018;18(11):1211–28. https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(18)30362-1/fulltext.
GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1459–1544 (2016).
Kotloff, K. L., Nataro, J. P. & Blackwelder, W. C. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multi- center Study, GEMS): A prospective, case-control study. Lancet 382, 209–222 (2013).
Mokomane, M., Kasvosve, I., de Melo, E., Pernica, J. M. & Goldfarb, D. M. The global problem of childhood diarrhoeal diseases: Emerging strategies in prevention and management. Ther. Adv. Infect. Dis. 5(1), 29–43 (2018).
Carvajal-vélez, L. et al. Diarrhea management in children under five in sub-Saharan Africa: Does the source of care matter? A countdown analysis. BMC Public Health 16(830), 1–14 (2016).
Akinyemi, I. A., Fagbamigbe, A. F., Omoluabi, E., Agunbiade, O. M. & Adebayo, S. O. Diarrhoea management practices and child health outcomes in Nigeria: Sub-national analysis. Adv. Integr. Med. 5(1), 15–22 (2018).
Fagbamigbe, A. F., Morakinyo, O. M., & Abatta, E. Analysis of regional variations in influence of household and environmental characteristics on prevalence of diarrhoea among under-five children in Nigeria. Ann. Med. Health Sci. Res. 2017;7(119–130):119–30. http://www.amhsr.org/archive/amhsr-volume-7-issue-3-may-2017.html.
GBD Diarrhoeal Diseases Collaborators. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 17(9), 909–948 (2017).
Ahs, J. W., Tao, W., Löfgren, J., & Forsberg, B. C. Diarrhoeal diseases in low- and middle-income countries: Incidence, prevention and management. Open Infect. Dis. J. 2010;4(123):113–24. https://pdfs.semanticscholar.org/0096/6b7bb3a3a78dd597e987a81cc8cb6a12b518.pdf.
Walker, F. C. L., Rudan, I., Liu, L., Nair, H., Theodoratou, E., Bhutta, Z. A, et al. Global burden of childhood pneumonia and diarrhoea. Lancet. 2013;381(9875):1405–16. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)60222-6/fulltext.
UNICEF. Diarrhoeal disease, Current status and progress. 2015. http://data.unicef.org/topic/child-health/diarrhoeal-disease/.
Pernica, J. M., Steenhoff, A. P. & Welch, H. Correlation of clinical outcomes with multiplex molecular testing of stool from children admitted to hospital with gastroenteritis in Botswana. J. Pediatr. Infect. Dis. Soc. 5, 312–318 (2016).
United Nations. Sustainable Development Goals (SDG). Washington, DC; 2015. http://www.un.org/sustainabledevelopment/sustainable-development-goals/.
Chopra, M., Mason, E. & Borrazzo, J. Ending of preventable deaths from pneumonia and diarrhoea: An achievable goal. Lancet 381, 1499–1506 (2013).
Baker, T. Burden of community diarrhoea in developing countries. Lancet Glob. Health 4(1), e25 (2016).
DeBoer, M. D. et al. Early childhood growth failure and the developmental origins of adult disease: Do enteric infections and malnutrition increase risk for the metabolic syndrome?. Nutr. Rev. 70(11), 642–653. https://doi.org/10.1111/j.1753-4887.2012.00543.x (2012).
Moore, S. R. et al. Prolonged episodes of acute diarrhea reduce growth and increase risk of persistent diarrhea in children. Gastroenterology 139(4), 1156–1164 (2010).
Kattula, D., Francis, M. R., Kulinkina, A., Sarkar, R., Mohan, V. R., Babji, S., et al. Environmental predictors of diarrhoeal infection for rural and urban communities in south India in children and adults. Epidemiol Infect. 2015;1–12. http://www.cmcwtrl.in/publications/Epidemiology-Infection.pdf.
Getachew, A., Guadu, T., Tadie, A., Gizaw, Z., Gebrehiwot, M., Cherkos, D. H., et al. Diarrhea prevalence and sociodemographic factors among under-five children in rural areas of North Gondar Zone, Northwest Ethiopia. Int. J. Pediatr. 2018;2018:1–8. https://www.hindawi.com/journals/ijpedi/2018/6031594/.
Croft, T. N., Marshall, A. M. J., & Allen, C. K. Guide to DHS Statistics [Internet]. 2018. https://dhsprogram.com/pubs/pdf/DHSG1/Guide_to_DHS_Statistics_DHS-7.pdf.
ICF International. Demographic and health survey: Sampling and household listing manual. Calverton; 2012. https://www.dhsprogram.com/pubs/pdf/DHSM4/DHS6_Sampling_Manual_Sept2012_DHSM4.pdf.
ICF International Inc. Uganda Demographic and Health Survey 2011 (UBOS, 2012).
National Bureau of Statistics Tanzania and ICF-Macro. Tanzania Demographic and Health Survey 2010. National Bureau of Statistics Dar es Salaam, Tanzania ICF Macro Calverton, Maryland, USA. 2011. pp. 1–482.
National Population Commission [Nigeria] and ICF International. Nigeria Demographic and Health Survey 2013. Abuja, Nigeria; 2014.
Vyass, S. & Kumaranayake, L. Constructing socioeconomic status indexes: How to use principal component analysis. Health Policy Plan. 21(6), 459–468 (2006).
Max, A. World Map Blank and Printable [Internet]. 2021. p. 1–1. https://worldmapblank.com/.
Fagbamigbe, A. F., Kandala, N. B. & Uthman, O. A. Severe acute malnutrition among under-five children in low- and middle-income countries: A hierarchical analysis of associated risk factors. Nutrition 2020(75–76), 110768 (2020).
Sambala, E. Z. et al. Mind the Gap: What explains the education-related inequality in missed opportunities for vaccination in sub-Saharan Africa? Compositional and structural characteristics. Hum. Vaccines Immunother. 14(10), 2365–2372. https://doi.org/10.1080/21645515.2018.1460985 (2018).
Morhason-Bello, I. O., Fagbamigbe, A. F., Kareem, Y. O. & Ojengbede, O. A. Economic status, a salient motivator for medicalisation of FGM in sub-Saharan Africa: Myth or reality from 13 national demographic health surveys. SSM Popul. Health 11, 100602. https://doi.org/10.1016/j.ssmph.2020.100602 (2020).
United Nations Development Programme. The 2018 Global Multidimensional Poverty Index (MPI) | Human Development Reports [Internet]. Human Development Report. 2018. p. 1. http://hdr.undp.org/en/2018-MPI.
United Nations. World Urbanization Prospects-Population Division-United Nations. 2018. p. 1. https://population.un.org/wup/Download/.
United Nations Development Programme. Human Development Data (1990–2017): Human Development Reports. Human Dev.Reports. 2018. http://hdr.undp.org/en/data.
United Nations. World Population Prospects-Population Division-United Nations. 2021. p. 1. https://population.un.org/wpp/Download/Standard/Population/.
Curtis, S. M. K. & Ghosh, S. K. A bayesian approach to multicollinearity and the simultaneous selection and clustering of predictors in linear regression. J. Stat. Theory Pract. 5(4), 715–735 (2011).
Charlton, C., Rasbash, J., Browne, W. J., Healy, M., & Cameron, B. MLwiN Version 3.03. Bristol; 2018. http://www.bristol.ac.uk/cmm/software/mlwin/refs.html.
Browne, W. J. MCMC Estimation in MLwiN v3.03. Bristol; 2019. http://www.bristol.ac.uk/cmm/software/mlwin/refs.html.
Snijders, T. A. B, & Bosker, R. J. Multilevel analysis : An introduction to basic and advanced multilevel modeling. 2nd ed. Sage; 2012. pp. 1–354. https://www.stats.ox.ac.uk/~snijders/mlbook.htm.
Larsen, K. & Merlo, J. Appropriate assessment of neighborhood effects on individual health: integrating random and fixed effects in multilevel logistic regression. Am. J. Epidemiol. 161(1), 81–88 (2005).
Uthman, O. A. et al. Does it really matter where you live? A multilevel analysis of factors associated with missed opportunities for vaccination in sub-Saharan Africa. Hum. Vaccin Immunother. 14(10), 2397–2404. https://doi.org/10.1080/21645515.2018.1504524 (2018).
Uthman, O. A. Influence of socioeconomic position and gender on current cigarette smoking among people living with HIV in sub-Saharan Africa: Disentangling context from composition. 2016; http://wrap.warwick.ac.uk/81344.
Bado, A. R., Susuman, A. S. & Nebie, E. I. Trends and risk factors for childhood diarrhea in sub-Saharan countries (1990–2013): Assessing the neighborhood inequalities. Glob. Health Action 9, 30166 (2016).
UNICEF. Diarrhoeal disease-UNICEF DATA. 2018. https://data.unicef.org/topic/child-health/diarrhoeal-disease/.
Tetteh, J., Takramah, W. K., Ayanore, M. A., Adoliba Ayanore, A., Bisung, E., & Alamu, J. Trends for diarrhea morbidity in the Jasikan District of Ghana: Estimates from district level Diarrhea Surveillance Data, 2012–2016. J. Trop. Med. 2018;2018:1–10. https://www.hindawi.com/journals/jtm/2018/4863607/.
Connell, B. J. O., Quinn, M. A., & Scheuerman, P. Risk factors of diarrheal disease among children in the East African countries of Burundi, Rwanda and Tanzania. Glob. J. Med. Publ. Health. 2017;6(1):1–7. www.gjmedph.com.
Walker, F. C. L., Perin, J., Aryee, M. J., Boschi-Pinto, C. & Black, R. E. Diarrhea incidence in low- and middle-income countries in 1990 and 2010: A systematic review. BMC Public Health 12(1), 220. https://doi.org/10.1186/1471-2458-12-220 (2012).
Fagbamigbe, A. F., Afolabi, R. F. & Yusuf, O. B. Trend analysis of teenage pregnancy in Nigeria (1961–2013): How effective is the contraceptive use campaign?. Int. J. Public. Health Sci. 8(2), 21–31 (2019).
Gebru, T., Taha, M. & Kassahun, W. Risk factors of diarrhoeal disease in under-five children among health extension model and non-model families in Sheko district rural community, Southwest Ethiopia: Comparative cross-sectional study. BMC Public Health 14(1), 395. https://doi.org/10.1186/1471-2458-14-395 (2014).
Woldu, W., Bitew, B. D. & Gizaw, Z. Socioeconomic factors associated with diarrheal diseases among under-five children of the nomadic population in northeast Ethiopia. Trop. Med. Health 44(1), 40. https://doi.org/10.1186/s41182-016-0040-7 (2016).
Fagbamigbe, A. F. et al. The Nigeria wealth distribution and health seeking behaviour : Evidence from the 2012 national HIV/AIDS and reproductive health survey. Health Econ. Rev. 5(5), e1-10 (2015).
Oloruntoba, E. O., Folarin, T. B. & Ayede, A. I. Hygiene and sanitation risk factors of diarrhoeal disease among under-five children in Ibadan, Nigeria. Afr. Health Sci. 14(4), 1001–1011 (2014).
Menon, J., Musonda, V. & Glazebrook, C. Perception of care in Zambian women attending community antenatal clinics. Educ. Res. 1(9), 356–362 (2010).
Alam, Z., Higuchi, M., Abul, M., Sarker, B. & Hamajima, N. Mass media exposure and childhood diarrhea: A secondary analysis of the 2011 Bangladesh Demographic and Health Survey.. Nagoya J. Med. Sci. 81(1), 31–40 (2019).
Fufa, K. W., Gebremedhin, G. B., Gebregergs, G. B., & Mokonnon, M. T. Assessment of poor home management practice of diarrhea and associated factors among caregivers of under-five years children in urban and rural residents of Doba Woreda, Ethiopia: Comparative cross-sectional study. Int. J. Pediatr. 2019;2019:1–12. https://www.hindawi.com/journals/ijpedi/2019/8345245/.
Meyer, D. F. & Nishimwe-niyimbanira, R. Daniel Francois Meyer & Rachel Nishimwe-Niyimbanira. Afr. Popul. Stud. 30(2), 2283–2295 (2016).
Mshida, H. A, Kassim, N., Kimanya, M. E., & Mpolya, E. Influence of water, sanitation, and hygiene practices on common infections among under-five children in Longido and Monduli Districts of Arusha, Tanzania. J. Environ. Public Health. 2017;2017:1–8. https://www.hindawi.com/journals/jeph/2017/9235168/.
Musonda, C., Siziya, S., Kwangu, M., & Mulenga, D. Factors associated with diarrheal diseases in under-five children: A case control study at arthur davison children’s hospital in Ndola, Zambia. Asian Pac. J. Health Sci. 2017;4(3):228–34. www.apjhs.com.
Mutua, M. K., Kimani-murage, E., & Ettarh, R. R. Childhood vaccination in informal urban settlements in Nairobi, Kenya: Who gets vaccinated?; 2011.
Fagbamigbe, A. F., Kandala, N. B. & Uthman, A. O. Demystifying the factors associated with rural–urban gaps in severe acute malnutrition among under-five children in low- and middle-income countries: A decomposition analysis. Sci. Rep. 10(11172), 1–15. https://doi.org/10.1038/s41598-020-67570-w (2020).
Acknowledgements
The authors are grateful to ICF Macro, USA, for granting the authors the request to use the DHS data. We appreciate the logistic supports provided by the consortium for advanced research and training in Africa (CARTA) to AFF in the course of writing this paper.
Funding
The authors received no funding for this study.
Author information
Authors and Affiliations
Contributions
A.F.F. conceptualised, designed the study, curated and analysed data and produced the vizualizations. All authors (A.F.F., O.A.U. and L.I.) contributed to literature search, figures, data interpretation, writing of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fagbamigbe, A.F., Uthman, A.O. & Ibisomi, L. Hierarchical disentanglement of contextual from compositional risk factors of diarrhoea among under-five children in low- and middle-income countries. Sci Rep 11, 8564 (2021). https://doi.org/10.1038/s41598-021-87889-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-87889-2
- Springer Nature Limited
This article is cited by
-
2-week prevalence and associated factors of fever, diarrhea, and coexisting fever and diarrhea among children aged 6–23 months in rural Hunan Province
Scientific Reports (2024)
-
Statistical Analysis of Factors Associated with Diarrhea in Yemeni Children under Five: Insights from the 2022–2023 Multiple Indicator Cluster Survey
Journal of Epidemiology and Global Health (2024)
-
Impact of ignoring sampling design in the prediction of binary health outcomes through logistic regression: evidence from Malawi demographic and health survey under-five mortality data; 2000-2016
BMC Public Health (2023)
-
Bayesian multilevel logistic regression models: a case study applied to the results of two questionnaires administered to university students
Computational Statistics (2023)
-
Factors contributing to household wealth inequality in under-five deaths in low- and middle-income countries: decomposition analysis
BMC Public Health (2022)