
Abstract
Emerging evidences have shown the utility of saliva for the detection of SARS-CoV-2 by PCR as alternative to nasopharyngeal swab (NPS). However, conflicting results have been reported regarding viral loads between NPS and saliva. We conducted a study to compare the viral loads between NPS and saliva in 42 COVID-19 patients. Viral loads were estimated by the cycle threshold (Ct) values. SARS-CoV-2 was detected in 34 (81%) using NPS with median Ct value of 27.4, and 38 (90%) using saliva with median Ct value of 28.9 (P = 0.79). Kendall’s W was 0.82, showing a high degree of agreement, indicating equivalent viral loads in NPS and saliva. After symptom onset, the Ct values of both NPS and saliva continued to increase over time, with no substantial difference. Self-collected saliva has a detection sensitivity comparable to that of NPS and is a useful diagnostic tool with mitigating uncomfortable process and the risk of aerosol transmission to healthcare workers.
Similar content being viewed by others


Introduction
Rapid and accurate diagnosis of coronavirus disease 2019 (COVID-19) is critical for containing outbreaks that may overwhelm healthcare systems. Although the detection of SARS-CoV-2 nucleic acids from nasopharyngeal swabs (NPS) is considered a gold standard in the diagnosis, self-collected saliva has been reported to have several advantages1. Specifically, self-collection reduces the risk of viral exposure for the healthcare worker and causes less discomfort for the patients. However, although emerging evidences have shown the utility of saliva as an alternative to NPS2,3,4,5,6, conflicting results have been reported regarding SARS-CoV-2 viral loads between NPS and saliva. Wyllie et al. showed that the viral load was higher in saliva than NPS7, while William et al. has reported results to the contrary6. We recently reported that the viral load was equivalent between saliva and NPS samples in large number of asymptomatic persons8. Herein, we conducted a study to compare the viral loads in paired samples (saliva and NPS) from symptomatic patients who were admitted for COVID-19.
Results
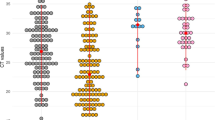
17 female (40%) and 25 male (60%) patients participated in the study. Median age of the patients was 73 years-old (range 27 to 93) and specimens were obtained at a median of 6 days (range 1–12) after symptom onset. SARS-CoV-2 was detected in NPS and saliva in 81% (34/42) and 90% (38/42) of the patients, respectively (Table 1). The cycle threshold (Ct) values using the N2 primers/probe were not significantly different between NPS and saliva, with median [IQR] of 27.4 [21.3, 35.6] and 28.9 [23.1, 33.6], respectively (Wilcoxon’s signed rank P = 0.79, Fig. 1A). Kendall’s W was 0.82, showing a high degree of agreement. Additionally, the Ct values of both NPS and saliva continued to increase over time, with no substantial difference (Fig. 1C). There were cases of both NPS and saliva that became undetermined only three days after the onset of symptoms. Similar results were obtained from N1 primers/probe; the Ct values using the N1 primers/probe were equivalent between NPS and saliva, with median [IQR] of 31.0 [24.2, 39.5] and 33.1 [27.3, 37.3], respectively (Wilcoxon’s signed rank P = 0.24, Fig. 1B). Kendall’s W was 0.83, showing a high degree of agreement. Changes in Ct values of both NPS and saliva were not different over time (Fig. 1D).

Viral loads of SARS-CoV-2 between nasopharyngeal swab and saliva specimens. (A,B) Scatter plots of Ct values using N2 (A) or N1 (B) primer and probe between NPS and saliva specimens taken from 42 COVID-19 patients. (C,D) Scatter plots of Ct values using N2 (C) or N1 (D) primer and probe primer against days from symptom onset. Median spline curves are also drawn using “qsreg” function with the default parameters in R.
Discussion
In this study in symptomatic inpatients with COVID-19, SARS-CoV-2 was detected in saliva in 90% of the patients compared to 81% in NPS, with equivalent viral loads in the two specimens. Although there have been conflicting results reported to date6,7, our study was designed to have significant advantages over previous studies; the number of patients was relatively large, paired samples were simultaneously collected, and qRT-PCR was performed at an independent central laboratory. In our study, viral loads were roughly estimated by the Ct values. Our results demonstrate that self-collected saliva is a useful alternative to NPS for the diagnosis of COVID-19. Furthermore, we recently reported equivalent sensitivity and specificity of qRT-PCR using saliva and NPS, again with equivalent viral loads in a large number of asymptomatic individuals in the setting of mass-screening8. Taken together, self-collected saliva provides highly accurate results and should be considered as an easier and cost-efficient alternative for the detection of SARS-CoV-2 in both symptomatic and asymptomatic individuals.
In summary, self-collected saliva is a useful alternative to NPS as a specimen for detecting SARS-CoV-2 nucleic acids. The methodology of self-collection carries significant logistical and cost advantages over NPS by mitigating the risk of aerosol transmission to healthcare workers and obviating the need for full protective suits.
Methods
Forty-two patients diagnosed with COVID-19 by positive qRT-PCR of NPS were enrolled in this study. Paired NPS and saliva samples were simultaneously collected from all patients upon hospital admission between June 12, 2020 and August 6, 2020. This study was approved by the Institutional Ethics Board (Hokkaido University Hospital Division of Clinical Research Administration Number: 020-0116) and informed consent was obtained from all patients. All the procedures are carried out according to relevant guidelines. qRT-PCR was performed at a central laboratory (SRL, Tokyo, Japan). Self-collected saliva was diluted fourfold with phosphate buffered saline and centrifuged at 2000 × g for 5 min to remove cells and debris. RNA was extracted from 200 µL of the supernatant or nasopharyngeal swab samples using QIAsymphony DSP Virus/Pathogen kit and QIAamp Viral RNA Mini Kit (QIAGEN, Hilden, Germany). qRT-PCR tests were performed, according to the manual by the National Institute of Infectious Diseases (NIID, https://www.niid.go.jp/niid/images/epi/corona/2019-nCoVmanual20200217-en.pdf). Briefly, 5uL of the extracted RNA was used to perform one step qRT-PCR using Thunderbird Probe One-step qRT-PCR Kit (Toyobo, Osaka, Japan) and 7500 Real-time PCR Systems (Thermo Fisher Scientific, Waltham, USA). The Ct values were obtained by using N1 primers (N_Sarbeco_F1, N_Sarbeco_R1) with N1 probe (N_Sarbeco_P1) and by using N2 primers (NIID_2019-nCOV_N_F2, NIID_2019-nCOV_N_R2) with N2 probe (NIID_2019-nCOV_N_P2), as described9.
Ct values of qRT-PCR using NPS and saliva were expressed as scatter plots with Kendall's coefficient of concordance W as nonparametric intraclass correlation coefficient. Scatter plots of Ct values and days from symptom onset for each type of specimen were also provided to examine the relationship between disease course and viral load. To find the longitudinal trends, we performed a median spline regression using “qsreg” function with the default parameters in R. Statistical analysis was conducted by R 4.0.2. All analyzed data were distributed in Supplement.
References
Wang, W. et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 323, 1843–1844. https://doi.org/10.1001/jama.2020.3786 (2020).
To, K. K. et al. Consistent detection of 2019 novel coronavirus in saliva. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciaa149 (2020).
Azzi, L. et al. Saliva is a reliable tool to detect SARS-CoV-2. J. Infect. 81, e45–e50. https://doi.org/10.1016/j.jinf.2020.04.005 (2020).
Tu, Y. P. et al. Swabs collected by patients or health care workers for SARS-CoV-2 testing. N. Engl. J. Med. 383, 494–496. https://doi.org/10.1056/NEJMc2016321 (2020).
Iwasaki, S. et al. Comparison of SARS-CoV-2 detection in nasopharyngeal swab and saliva. J. Infect. 81, e145–e147. https://doi.org/10.1016/j.jinf.2020.05.071 (2020).
Williams, E., Bond, K., Zhang, B., Putland, M. & Williamson, D. A. Saliva as a noninvasive specimen for detection of SARS-CoV-2. J. Clin. Microbiol. 58, https://doi.org/10.1128/JCM.00776-20 (2020).
Wyllie, A. L. et al. Saliva or nasopharyngeal swab specimens for detection of SARS-CoV-2. N. Engl. J. Med. 383, 1283–1286. https://doi.org/10.1056/NEJMc2016359 (2020).
Yokota, I. et al. Mass screening of asymptomatic persons for SARS-CoV-2 using saliva. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciaa1388 (2020).
Nagura-Ikeda, M. et al. Clinical evaluation of self-collected saliva by RT-qPCR, direct RT-qPCR, RT-LAMP, and a rapid antigen test to diagnose COVID-19. J. Clin. Microbiol. https://doi.org/10.1128/JCM.01438-20 (2020).
Acknowledgements
This study was funded by Health, Labour and Welfare Policy Research Grants 20HA2002.
Author information
Authors and Affiliations
Contributions
I.Y., T.T., designed study and wrote paper; T.H., P.Y.S., S.K., A.N., K.T.; collected samples; S.F., M.N., designed study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yokota, I., Hattori, T., Shane, P.Y. et al. Equivalent SARS-CoV-2 viral loads by PCR between nasopharyngeal swab and saliva in symptomatic patients. Sci Rep 11, 4500 (2021). https://doi.org/10.1038/s41598-021-84059-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-84059-2
- Springer Nature Limited