
Abstract
This retrospective cohort study aimed to investigate the effects of neonatal oxygen care and retinopathy of prematurity (ROP) treatment on ROP-related ocular and neurological prognoses. We included premature infants treated for ROP at a tertiary referral center between January 2006 and December 2019. Demographic and clinical data were collected from electronic medical records. Odds ratios (ORs) of oxygen care- and ROP treatment-related factors were calculated for ocular and neurological comorbidities 3 years after ROP treatment, after adjusting for potential confounders. ROP requiring treatment was detected in 171 eyes (88 infants). Laser treatment for ROP (OR = 4.73, 95% confidence interval [CI] 1.64–13.63) and duration of invasive ventilation (OR = 1.02, 95% CI 1.00–1.03) were associated with an increase in ocular comorbidities, along with a history of neonatal seizure (OR = 28.29, 95% CI 5.80–137.95) and chorioamnionitis (OR = 32.13, 95% CI 5.47–188.74). No oxygen care- or ROP treatment-related factors showed significant odds for neurological comorbidities. Shorter duration of invasive oxygen supply during neonatal care (less than 49 days) and anti-vascular endothelial growth factor injection as the primary treatment for ROP are less likely to cause ocular comorbidities. No association was identified between ROP treatment modalities and the risk of neurological comorbidities.
Similar content being viewed by others


Introduction
Retinopathy of prematurity (ROP), a leading cause of childhood blindness, is a proliferative retinal vascular disease exclusive to premature infants1. The primary treatment of ROP is gradually changing from laser photocoagulation 2 to anti-vascular endothelial growth factor (VEGF) injection3, although neurodevelopmental and systemic outcomes are still under investigation4. In recent studies, ROP treatment-related ocular and systemic outcomes of these infants, including neurodevelopmental impairments, were comparable between different ROP treatment modalities5,6,7,8. However, the effects of changes in perinatal risk and neonatal oxygen care have not been comprehensively investigated in tandem with the change in primary treatment of ROP.
The survival rate among extremely premature infants (less than 28 weeks gestation) is increasing9. Concurrently, the rate of multiple births from artificial/assisted fertilization has increased10 and the rate of age-dependent pregnancy complications is also increasing11. Consequently, the pattern of perinatal risk factors has changed over time12,13. Changes in perinatal factors, including neonatal care in prematurity, may affect ophthalmic and systemic outcomes of these infants, not limited by ROP treatment factors.
In neonatal care, the optimal approach to oxygen management remains unclear. Lower oxygen saturation levels increase the risk of mortality, while higher targets are associated with increased rate of oxidative stress14. Presently, ventilator-related strategies aim for lower oxygen targets and higher arterial carbon dioxide levels15,16. A correlation was found between prematurity, oxygen levels, and ROP risk17,18,19. However, little is known about the impact of changing trends in oxygen therapy on ROP-related prognoses.
To determine which factor related to neonatal oxygen care and ROP treatment, is significant to ROP-related ocular and neurological outcomes, we retrospectively investigated demographic and clinical data in infants treated for ROP over a 14-year period and evaluated possible associations.
Results
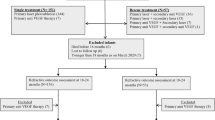
A total of 786 premature infants were screened for ROP, and type 1 ROP requiring treatment was diagnosed in 118 infants, with an overall incidence of 15%. Thirty infants were excluded due to ineligibility (17 for incomplete follow-up and 13 for missing data) and a total of 171 eyes (88 infants) were included in the analyses. The mean follow-up period was 46.6 ± 10.3 months.
Baseline clinical characteristics of ROP infants are provided in Table 1. The average gestational age (GA) was 28.1 ± 2.9 weeks and the mean postmenstrual age (PMA) at treatment was 38.85 ± 7.4 weeks. The average birthweight of premature infants was 1186 ± 475 g. ROP were treated most frequently for stage 3 (59%) following by aggressive posterior ROP (APROP) (26%). Among ROP classification, stage 3 at zone 2 with plus disease was most common (51%). Primary treatment of ROP was laser photocoagulation in 50 eyes (30%) and anti-VEGF injection in 121 eyes (71%). The type of anti-VEGF agent used was ranibizumab in 108 eyes (63%), while bevacizumab in 13 eyes (7.6%). The recurrence rate was significantly higher in anti-VEGF treated eyes (28%) compared to laser-treated eyes (9%, P = 0.003), and there was no significant difference between anti-VEGF agents (12% for bevacizumab vs. 16% ranibizumab, P = 0.13). Additional treatment modalities involved laser (26%), anti-VEGF injection (18%), and scleral buckling (3%). No cases progressed beyond stage 3 ROP after primary treatment, except for one case with stage 4 ROP requiring surgical intervention after laser treatment. In addition, all eyes that required additional laser or anti-VEGF injection for ROP reactivation did not progress to advanced stages and eventually achieved full vascularization of healthy retina.
Perinatal risk factors detected prior to ROP treatment were described in Table 2. Preterm premature rupture of the membranes was most common (27%) of maternal- and birth-related complications, followed by multiple pregnancy (18%). Among systemic comorbidities, intraventricular hemorrhage was noted most frequent (31%), followed by sepsis (9.1%). Neonatal care-related factors were summarized in Table 2. Invasive ventilation was applied in 82 infants for 42 ± 39.4 days, non-invasive ventilation in 65 infants for 11.1 ± 24.1 days, and oxygen supplementation in 84 infants for 54.1 ± 39.1 days.
Table 3 presents ocular and neurological outcomes 3 years after ROP treatment. Strabismus operation rate (15%) was higher than other ocular comorbidities. The incidence of epilepsy or neonatal seizure was assessed in 5.8%, cerebral palsy in 4.1%, and neurodevelopmental delay, evaluated with the Denver II test in 3.5%.
Risk factors for ocular comorbidities 3 years after ROP treatment
Supplementary Table S1 displays the unadjusted ORs (95% CI) in univariable regression analyses for ocular comorbidities 3 years after ROP treatment. Final multivariable regression model after adjusting confounding variables is presented in Table 4. Laser (vs. injection) treatment for ROP had five-fold-increased odds (odds ratio [OR] = 4.732, 95% CI 1.64–13.63) of ocular comorbidities. Longer duration of invasive ventilation (OR = 1.016, 95% CI 1.00–1.03) increased odds of ocular comorbidities with a history of neonatal seizure (OR = 28.292, 95% CI 5.80–137.95), and presence of chorioamnionitis (OR = 32.133, 95% CI 5.47–188.74). APROP was a possible risk factor for poor eye-related outcomes in the univariable analysis but was not included in the final model of multivariable analysis. Low-risk ROP (zone 2 stage 2 with plus) was not associated with a decreased odds of ocular comorbidities.
Analysis of the optimal cut-off for the duration of invasive ventilation, using criterion based on Youden’s index, identified an optical cut-off value of 49 days (Fig. 1). This threshold value in invasive ventilation duration predicts occurrence of ocular comorbidity with 58% sensitivity, 79% specificity, and all with an area-under-the-curve performance of 71%. Additional binary logistic regression modeling of outcomes according to this duration threshold yields statistically significant associations with ocular outcomes (invasive ventilation ≥ 49 days: OR 5.132 for ocular comorbidity, 95% CI 2.44‒10.79; P < 0.001).

Receiver operating characteristic curve and the Youden’s index to determine the optimal cut-off threshold of invasive ventilation duration that increases the risk of ocular comorbidity.
Risk factors for neurological comorbidities 3 years after ROP treatment
Supplementary Table S2 displays the unadjusted ORs (95% CI) in univariable regression analyses for neurological comorbidities 3 years after ROP treatment. Final multivariable regression model after adjusting confounding variables is presented in Table 5. The increased odds of treatment modality of ROP (injection vs. laser) for neurological comorbidities was not significant. While bevacizumab had increased odds of neurological comorbidities compared to ranibizumab, this association was excluded in the final regression model. Any factor related with neonatal oxygen care showed no significant odds of neurological comorbidities.
Higher birthweight (OR = 0.998, 95% CI 0.99–1.00) showed decreased odds of neurological comorbidities. Longer duration of incubator-based care (OR = 1.010, 95% CI 1.00–1.02), a history of intraventricular hemorrhage (OR = 3.836, 95% CI 1.03–14.24), neonatal seizure (OR = 3.836, 95% CI 1.03–14.24), and hydrocephalus requiring shunt placement (OR = 16.102, 95% CI 2.94–88.16) had significantly increased odds of neurological comorbidities. Neither low-risk ROP nor APROP appeared to be associated with neurological comorbidities.
Discussion
This study shows that less invasive oxygen therapy may result in more favorable ROP-related ocular outcomes in conjunction with primary anti-VEGF therapy for ROP. In addition, a history of chorioamnionitis or neonatal seizure was associated with ocular comorbidities. The choice of ROP treatment (anti-VEGF injection or laser photocoagulation) and anti-VEGF agent (bevacizumab or ranibizumab) appears to have no significant effect on ocular or neurological outcomes, including neurodevelopment.
Among the factors related to neonatal care, the duration of invasive ventilation was associated with an increased risk of long-term ocular comorbidities, whereas ROP severity at the time of treatment did not show a significant association. This result suggests that prolonged invasive ventilation may adversely affect the post-treatment course of ROP. Additionally, the length of incubator care was associated with more common neurological comorbidities. For optimal treatment outcomes in premature infants, our study results indicate that comprehensive multidisciplinary management involving neonatologists, pediatric neurologists, and ophthalmologists is necessary.
Overall, infants who recently received ROP treatment were more frequently associated with artificial/assisted pregnancies. This finding is likely accounted for by increasing maternal age, advances in assisted fertilization techniques, and an increasing frequency of artificial/assisted fertilization. Among maternal- and birth-related factors, the presence of maternal chorioamnionitis was a strong independent risk factor for ROP-associated ocular comorbidities. With improved survival rates of extremely premature neonates, the risk of systemic comorbidities has also increased. Importantly, a history of neonatal seizure was associated with an increase of ocular comorbidities. Therefore, infants with a history of maternal chorioamnionitis or neonatal seizure might require careful screening for ophthalmic comorbidities. As expected, a history of neonatal seizure or brain shunt operation for hydrocephalus was a risk factor for neurological comorbidities, along with a lower birthweight.
Chorioamnionitis has been previously associated with retinal and subretinal vasculopathy. In addition to antenatal and postnatal inflammation, circulatory instability and oxygen satuation fluctuations following inflammation may affect retinal perfusion20,21. Prolonged antenatal action of proinflammatory cytokines, major mediator of chorioamnionitis, have been shown to cause delay in retinal vasculature growth, thinning of the choroid, and long-term morphological alterations of the retina22. Our findings provide real-world evidence that maternal chorioamionitis is a risk factor for ocular comorbidities. While neonatal seizures are often associated with retinal hemorrhages, they have not been shown to actually cause retinal hemorrhages23,24. However, acute symptomatic seizures can occur due to hypoxic-ischemic encephalopathy, acquired structural brain lesions, metabolic disturbances, or systemic infections, which may cause vascular instability and prolonged inflammation that may affect retinal development25.
In this study, anti-VEGF injection, compared to laser photocoagulation, was associated with a lower incidence of ocular comorbidities. This difference was most apparent in the number of cases undergoing strabismus surgery that may indicate errors in neurodevelopment as suggested from the pivotal ETROP trials26. However, this is likely to be the result of differences in the age and follow-up between the two groups, warranting caution when interpreting the results. The primary method of ROP treatment (whether laser or injection) was not associated with long-term neurologic prognosis, including neurodevelopmental status assessed by the Denver II Developmental Screening Test. The effects of the anti-VEGF agent type (bevacizumab or ranibizumab) were not significant at risk for neurological comorbidity (including delayed neurological development). This is noteworthy because the potential risk for neurodevelopmental delay caused by systemic absorption of intravitreal anti-VEGF is the main cause of concern regarding widespread use in premature infants. When accounting for comprehensive pediatric evaluations and in depth review of medical records, no increased risk stemming from the use of anti-VEGF therapy was shown over laser treatment. Further research is required to confirm the systemic effects of anti-VEGF agents.
In the present study, we noted a significant proportion of infants of GA > 32 weeks treated for ROP in the recent period, which is atypical for infants within this age-group to progress to treatment-requiring ROP. There were no periodic changes in the PMA at treatment, suggesting a faster ROP progression rate among infants of higher GA and indicating that careful observation of neonates may be warranted during the critical PMA window (37–39 weeks).
Recently, interventions appeared to be delivered at an earlier disease stage (ROP classification of zone 2 stage 2 with plus disease), although this difference was not significant. This finding might be due to the simplification of the treatment process from laser photocoagulation to anti-VEGF injection, which might have allowed ophthalmologists greater ease in recommending interventions to eligible neonates with ROP. Furthermore, higher retreatment rates were observed among eyes treated with anti-VEGF. This may be explained by the pharmacokinetics of these anti-VEGF agents and the fact that a higher proportion of eyes were treated with injection for zone 1 disease and APROP27.
The limitations of this study include its retrospective nature, lack of a control group, and a homogenous sample, which involved a single ethnic group from a well-developed country with easy access to healthcare. Additionally, we could not account for target levels of oxygen therapy due to the retrospective nature of this study. Instead, the application rate and duration of each oxygen therapy modality were used as variables to consider. Because this study was not a randomized controlled trial, we cannot exclude the possibility of confounding bias caused by heterogeneous and time-varying underlying systemic conditions. Therefore, our presentation of possible associations should be considered with caution, and not be interpreted as a cause-and-effect relationship. Furthermore, although variance inflation factor of all independent variables has been evaluated, collinearity between variables may limit our interpretations.
However, this study was conducted on a relatively large number of treated ROP eyes (N = 171) over a 14-year period at a large tertiary medical center with an average follow-up period greater than 3 years. Considering the paucity of treated ROP cases that considered the neonatal management and the difficulty of regular follow-up with infants, our study results do have clinical importance.
Taking into account the contextual changes in perinatal risk and neonatal care, we have identified some important modifiable factors that may affect the long-term ocular and neurological prognosis of premature infants treated for ROP. In conclusion, shorter application of invasive ventilation during neonatal intensive care unit (NICU) care (less than 49 days) and ROP treatment via anti-VEGF injection have emerged as controllable factors that might improve ophthalmic prognosis among neonates treated for ROP. We were unable to confirm previous concerns regarding a potentially harmful association between anti-VEGF injection or injection drugs and neurological outcomes, in this clinical context.
Methods
This retrospective study was conducted at Gangnam Severance Hospital, a tertiary referral-based hospital affiliated with Yonsei University College of Medicine. At this hospital, neonates receive care from a multidisciplinary team, including neonatologists, ophthalmologists, anesthesiologists, and other pediatric specialists. Infants requiring ROP treatment were treated at NICUs. This study was based on data extracted from electronic medical records.
Consecutive infants who were treated for type 1 ROP between January 2006 and December 2019 and followed up at least 3 years were included. Neonates were screened for ROP if they met one or more of the following criteria: GA < 32 weeks, birthweight < 1500 g, or unstable clinical course determined by the primary neonatologist based on the applicable protocol at our institution. All ophthalmic examinations were performed by qualified pediatric retinal specialists using the 2005 International Classification of Retinopathy of Prematurity28; treatment was indicated for infants diagnosed with type 1 ROP, according to the same criteria as used in a previous study2. We further categorized a low-risk ROP type as zone 2 stage 2 ROP with plus disease to determine any possible subtle differences in disease progression and outcomes.
First-line treatment for ROP was chosen after discussion with the infants’ guardians and was performed by pediatric retinal specialists. Although varied due to the specialist’s preference, treatment period, and disease severity, the overall treatment decision could be broadly categorized according to the widening availability of different modalities. Prior to the introduction of anti-VEGF injections for ROP treatment, laser photocoagulation was the treatment of choice. The reporting of reliable safety data regarding anti-VEGF use in neonatal infants has made the injection the primary choice for ROP treatment, especially in less severe cases. In addition, the primary anti-VEGF choice switched from bevacizumab (0.50 mg/0.02 mL, off-label Avastin; Genentech, San Francisco, CA, USA) to ranibizumab (0.20 mg/0.02 mL, off-label Lucentis; Novartis, Basel, Switzerland), after ranibizumab has been shown to have faster systemic clearance and is theoretically safer for use in neonates.
Laser photocoagulation was performed under general anesthesia, using an indirect diode laser system with a 30-diopter (D) hand-held aspheric lens following scleral depression, with power settings adjusted to achieve a pale white burn of the retina. The laser was applied to the avascular area. For intravitreal anti-VEGF injection, either bevacizumab or ranibizumab was injected into the diseased eye under sedation and topical anesthesia. The use of these off-label anti-VEGF agents for treating ROP was approved by the Institutional Review Board. Infants were re-examined the following day and every week thereafter to monitor disease progression. Reappearance of plus disease or progression of ROP stage despite adequate treatment were defined as recurrence. As required, experienced retinal specialists performed additional procedures such as injection, laser, or surgery, including vitrectomy or scleral buckling.
Clinical characteristics of interest included GA, birthweight, ROP-related factors (incidence, severity, treatment age, and modality), and other perinatal factors such as maternal- or birth-related complications, neonatal care (oxygen care type/duration, number of re-intubations, admission duration/re-admission), and systemic comorbidities detected prior to ROP treatment. Invasive ventilation was defined as infants with endotracheal intubation or mechanical ventilation, non-invasive ventilation as infants with face or nasal masks, and oxygen supplementation as infants with oxygen hoods. Target oxygen saturation levels are between 90 and 95% for preterm neonates, while mature infants (GA > 34 weeks) with decreased risk for ROP have a higher target of 97%. The use and duration of each category oxygen were individually tailed in the NICU by trained healthcare professionals; this information is saved to the electronic health records of these infants, and we documented these factors for assessment in this study.
Adverse systemic outcomes were determined through a complete review of patients’ medical records, which included comprehensive examination of follow-up data provided by pediatric specialists; any diagnoses added by the primary pediatrician after ROP treatment were included as systemic comorbidities. Neurological examinations were performed immediately after discharge from the NICU and the Denver II Developmental Screening Test was routinely performed at regular follow-up intervals in the pediatrics department, and those who failed in two or more items of the test were suspected of having neurodevelopmental delay. Ocular comorbidities included any ROP-related ophthalmologic abnormalities (e.g. macular dragging, foveal hypoplasia, optic atrophy, strabismus, late vitreous hemorrhage, cataract, glaucoma, or retinal detachment) that can result in poor visual prognosis detected during ophthalmologic follow-up.
Main outcomes
The primary outcomes were possible associations between methods of oxygen care and ROP treatment with ROP-related ocular and neurological comorbidities, after adjusting for potential confounders.
Statistical analysis
Sample size of 84 cases was calculated with type 1 error probability of 0.05 and power of 80%. We performed statistical analyses using the Statistical Package for the Social Sciences software (version 22.0; IBM, Armonk, NY, USA). Listwise deletion was used method in handling missing data. The Kolmogorov–Smirnov test was used to analyze the distribution of the data. Chi-squared tests for categorical variables were used to compare the groups. Logistic regression analysis (backward selection, using the likelihood ratio method) was performed to assess risk factors for ocular and neurological outcomes. Factors with P < 0.10 in the univariable logistic regression analysis were included in a multivariable logistic regression model. Optimal cut-off thresholds were analyzed using criterion based on Youden’s index, which maximizes the sum of sensitivity and specificity and also maximizes concordance (RStudio version 1.4.1106; R version 4.0.4; Boston, MA, USA). All data are presented as means (standard deviations) for continuous variables or numbers with percentages for categorical variables. P < 0.05 were considered statistically significant.
Ethics information
Ethical approval was obtained from the Institutional Review Board of Gangnam Severance Hospital (No. 3-2019-0332). Informed consent for treatment was obtained from the patients’ parents or guardians, and the need for consent to be involved in this study was waived due to the retrospective nature of the study. The study adhered to the tenets of the Declaration of Helsinki.
Data availability
Anonymized participant data are available upon reasonable request from Dr EY. Choi. However, data reuse is not permitted.
References
Blencowe, H., Lawn, J. E., Vazquez, T., Fielder, A. & Gilbert, C. Preterm-associated visual impairment and estimates of retinopathy of prematurity at regional and global levels for 2010. Pediatr. Res. 74, 35–49. https://doi.org/10.1038/pr.2013.205 (2013).
Good, W. V., Early Treatment for Retinopathy of Prematurity Cooperative, G. Final results of the Early Treatment for Retinopathy of Prematurity (ETROP) randomized trial. Trans. Am. Ophthalmol. Soc. 102, 233–248 (2004) (discussion 248–250).
Mintz-Hittner, H. A., Kennedy, K. A. & Chuang, A. Z. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N. Engl. J. Med. 364, 603–615 (2011).
Stahl, A. et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): An open-label randomised controlled trial. Lancet 394, 1551–1559 (2019).
Fan, Y. Y. et al. Neurodevelopmental outcomes after intravitreal bevacizumab therapy for retinopathy of prematurity: A prospective case–control study. Ophthalmology 126, 1567–1577. https://doi.org/10.1016/j.ophtha.2019.03.048 (2019).
Rodriguez, S. H. et al. Neurodevelopmental outcomes comparing bevacizumab to laser for type 1 ROP. Ophthalm. Surg. Lasers Imaging Retina 50, 337–343. https://doi.org/10.3928/23258160-20190605-01 (2019).
Natarajan, G. et al. Neurodevelopmental outcomes of preterm infants with retinopathy of prematurity by treatment. Pediatrics https://doi.org/10.1542/peds.2018-3537 (2019).
Kang, H. G., Kim, T. Y., Han, J. & Han, S.-H. Refractive outcomes of 4-year-old children after intravitreal anti-vascular endothelial growth factor versus laser photocoagulation for retinopathy of prematurity. Korean J. Ophthalmol. 33, 272–278 (2019).
Myrhaug, H. T., Brurberg, K. G., Hov, L. & Markestad, T. Survival and impairment of extremely premature infants: A meta-analysis. Pediatrics https://doi.org/10.1542/peds.2018-0933 (2019).
Kushnir, V. A., Barad, D. H., Albertini, D. F., Darmon, S. K. & Gleicher, N. Systematic review of worldwide trends in assisted reproductive technology 2004–2013. Reprod. Biol. Endocrinol. 15, 6. https://doi.org/10.1186/s12958-016-0225-2 (2017).
Lean, S. C., Derricott, H., Jones, R. L. & Heazell, A. E. P. Advanced maternal age and adverse pregnancy outcomes: A systematic review and meta-analysis. PLoS ONE 12, e0186287. https://doi.org/10.1371/journal.pone.0186287 (2017).
Bell, R. et al. Changing patterns of perinatal death, 1982–2000: A retrospective cohort study. Arch. Dis. Child Fetal Neonatal Ed. 89, F531-536. https://doi.org/10.1136/adc.2003.038414 (2004).
Kultursay, N. et al. The change of perinatal mortality over three decades in a reference centre in the Aegean Region: Neonatal mortality has decreased but foetal mortality remains unchanged. Balkan. Med. J. 34, 553–558. https://doi.org/10.4274/balkanmedj.2016.0870 (2017).
Kayton, A., Timoney, P., Vargo, L. & Perez, J. A. A review of oxygen physiology and appropriate management of oxygen levels in premature neonates. Adv. Neonatal Care 18, 98–104. https://doi.org/10.1097/ANC.0000000000000434 (2018).
Kumar, P. & Kiran, P. S. Changing trends in the management of respiratory distress syndrome (RDS). Indian J. Pediatr. 71, 49–54. https://doi.org/10.1007/bf02725656 (2004).
Bhandari, V. Noninvasive respiratory support in the preterm infant. Clin. Perinatol. 39, 497–511. https://doi.org/10.1016/j.clp.2012.06.008 (2012).
Chow, L., Wright, K., Sola, A., Group, C. O. A. S. Can changes in clinical practice decrease the incidence of severe retinopathy of prematurity in very low birth weight infants?. Pediatrics 111, 339–345 (2003).
Flynn, J. T. et al. A cohort study of transcutaneous oxygen tension and the incidence and severity of retinopathy of prematurity. N. Engl. J. Med. 326, 1050–1054. https://doi.org/10.1056/NEJM199204163261603 (1992).
Tin, W., Milligan, D. W., Pennefather, P. & Hey, E. Pulse oximetry, severe retinopathy, and outcome at one year in babies of less than 28 weeks gestation. Arch. Dis. Child Fetal Neonatal. Ed. 84, F106-110. https://doi.org/10.1136/fn.84.2.f106 (2001).
Villamor-Martinez, E. et al. Chorioamnionitis as a risk factor for retinopathy of prematurity: An updated systematic review and meta-analysis. PLoS ONE 13, e0205838. https://doi.org/10.1371/journal.pone.0205838 (2018).
Lundgren, P. et al. Aggressive posterior retinopathy of prematurity is associated with multiple infectious episodes and thrombocytopenia. Neonatology 111, 79–85. https://doi.org/10.1159/000448161 (2017).
Beaudry-Richard, A. et al. Antenatal IL-1-dependent inflammation persists postnatally and causes retinal and sub-retinal vasculopathy in progeny. Sci. Rep. 8, 11875. https://doi.org/10.1038/s41598-018-30087-4 (2018).
Aryan, H. E., Ghosheh, F. R., Jandial, R. & Levy, M. L. Retinal hemorrhage and pediatric brain injury: Etiology and review of the literature. J. Clin. Neurosci. 12, 624–631. https://doi.org/10.1016/j.jocn.2005.05.005 (2005).
Sandramouli, S., Robinson, R., Tsaloumas, M. & Willshaw, H. E. Retinal haemorrhages and convulsions. Arch. Dis. Child. 76, 449–451. https://doi.org/10.1136/adc.76.5.449 (1997).
Glass, H. C. et al. Contemporary profile of seizures in neonates: A prospective cohort study. J. Pediatr. 174, 98-103.e101. https://doi.org/10.1016/j.jpeds.2016.03.035 (2016).
Vander Veen, D. K. et al. Prevalence and course of strabismus through age 6 years in participants of the Early Treatment for Retinopathy of Prematurity randomized trial. J. Aapos. 15, 536–540. https://doi.org/10.1016/j.jaapos.2011.07.017 (2011).
Kang, H. G. et al. Intravitreal ranibizumab versus laser photocoagulation for retinopathy of prematurity: Efficacy, anatomical outcomes and safety. Br. J. Ophthalmol. 103, 1332–1336. https://doi.org/10.1136/bjophthalmol-2018-312272 (2019).
International Committee for the Classification of Retinopathy of P. The international classification of retinopathy of prematurity revisited. Arch. Ophthalmol. 123, 991–999. https://doi.org/10.1001/archopht.123.7.991 (2005).
Funding
This work was supported by the Yonsei Graduate Students' Association and funded by the Graduate School of Yonsei University.
Author information
Authors and Affiliations
Contributions
H.G.K. and E.Y.C. conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. H.C., M.K., C.S.L., and S.M.L. coordinated and supervised data collection, and critically reviewed the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kang, H.G., Choi, E.Y., Cho, H. et al. Oxygen care and treatment of retinopathy of prematurity in ocular and neurological prognosis. Sci Rep 12, 341 (2022). https://doi.org/10.1038/s41598-021-04221-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-04221-8
- Springer Nature Limited