
Abstract
Pediatric tuberculosis (TB) remains a major global health problem. Improved pediatric diagnostics using readily available biosources are urgently needed. We used liquid chromatography-mass spectrometry to analyze plasma metabolite profiles of Indian children with active TB (n = 16) and age- and sex-matched, Mycobacterium tuberculosis-exposed but uninfected household contacts (n = 32). Metabolomic data were integrated with whole blood transcriptomic data for each participant at diagnosis and throughout treatment for drug-susceptible TB. A decision tree algorithm identified 3 metabolites that correctly identified TB status at distinct times during treatment. N-acetylneuraminate achieved an area under the receiver operating characteristic curve (AUC) of 0.66 at diagnosis. Quinolinate achieved an AUC of 0.77 after 1 month of treatment, and pyridoxate achieved an AUC of 0.87 after successful treatment completion. A set of 4 metabolites (gamma-glutamylalanine, gamma-glutamylglycine, glutamine, and pyridoxate) identified treatment response with an AUC of 0.86. Pathway enrichment analyses of these metabolites and corresponding transcriptional data correlated N-acetylneuraminate with immunoregulatory interactions between lymphoid and non-lymphoid cells, and correlated pyridoxate with p53-regulated metabolic genes and mitochondrial translation. Our findings shed new light on metabolic dysregulation in children with TB and pave the way for new diagnostic and treatment response markers in pediatric TB.
Similar content being viewed by others

Introduction
The World Health Organization estimates incident tuberculosis (TB) occurs in 1.1 million children annually, representing > 200,000 deaths and 11% of global burden1. India ranks first in pediatric TB cases among 22 high-burden countries2. Since young children with pulmonary TB generally cannot cough effectively, microbiological confirmation of Mycobacterium tuberculosis (MTB) infection is established in only 15–50% of cases2,3, and often only after invasive sample collection4. Although rapid molecular tests have improved sensitivity over smear microscopy, their sensitivity in children remains < 70% compared with culture5,6,7. Furthermore, neither tuberculin skin tests (TST) nor interferon-gamma release assays (IGRA) can distinguish active disease from latent TB infection (LTBI)8,9. As a result, TB treatment is often prescribed empirically based on clinical findings and medical history. This inevitably over-diagnoses some children with associated toxicity and costs10.
Despite these diagnostic challenges, TB induces profound changes in whole-body energy and protein metabolism that can be identified in blood11,12,13,14,15,16,17,18,19,20,21. Such testing could also potentially identify extrapulmonary TB without invasive sampling of pleural or cerebrospinal fluid22,23,24 and improve assessments of treatment response25,26,27. Limited data are available, however, on the metabolic changes affecting children with TB12,13, and it is unknown whether the same differences described in other populations and body compartments will be relevant for blood-based diagnosis of pediatric TB or that the same metabolites will characterize treatment response among children. To characterize TB-associated metabolic dysregulation and assess potential blood-based biomarkers of TB and treatment response in children, we performed a longitudinal case–control study of Indian children with confirmed TB and uninfected household contacts.
Material and methods
Study design and sample selection
The Cohort for TB Research by the Indo-US Medical Partnership (CTRIUMPH) is a 5-year prospective observational study of adults and children with TB and the household contacts of participants with pulmonary TB28. The current analysis represents a nested case–control study in CTRIUMPH for which the methods have been described previously29. CTRIUMPH participants recruited at one of the sites, Byramjee Jeejeebhoy Government Medical College (BJGMC) in Pune, India with confirmed TB who were under 15 years of age were identified as cases, all of whom were successfully treated without clinical or microbiological relapse within 1 year of treatment completion. All participants received standardized therapy according to local standard of care in the public sector at the time of treatment (2015–2016). This included a thrice weekly fixed-dose drug combination of isoniazid, rifampin, pyrazinamide along with ethambutol. All drugs were dosed according to weight. All participants received all four drugs for the first two months of treatment, followed by a weight-based fixed dose combination of isoniazid and rifampin for the remainder of therapy (Table S1). Cases were each age- and sex-matched with two children who were household contacts of pulmonary TB patients (controls). Controls were considered eligible for this study if at the time of enrollment they had a negative symptom screen for TB, negative chest radiography, and both negative TST (< 5 mm induration) and IGRA (measured by QuantiFERON Gold In-Tube according to manufacturer’s instructions). Plasma was collected longitudinally from all cases at the time of treatment initiation, after 1 month of treatment, and at treatment completion at 6 months. Controls had plasma collected at enrollment and again at 4–6 months and 12 months, with repeat assessments at each time point for both active TB and LTBI, defined as positive by either TST or IGRA. Controls with new LTBI had the month of test conversion registered for analysis (Table S2).
Quantitative metabolomic analysis
Samples were processed at Metabolon, Inc. (Durham, North Carolina) using the automated MicroLab STAR system from Hamilton Company and quality-control analyses were performed as described previously30,31. Briefly, several recovery internal standards were added prior to the first step in the extraction process for QC purposes. Samples were placed briefly on a TurboVap (Zymark) to remove the organic solvent. The sample extracts were stored overnight under nitrogen before preparation for analysis by ultrahigh performance liquid chromatography-tandem mass spectroscopy (UPLC-MS/MS). All methods utilized a Waters ACQUITY ultra-performance liquid chromatography (UPLC) and a Thermo Scientific Q-Exactive high resolution/accurate mass spectrometer interfaced with a heated electrospray ionization (HESI-II) source and Orbitrap mass analyzer operated at 35,000 mass resolution. The sample extract was dried and reconstituted in solvents compatible with each of the four methods particularly, to (1) optimize for more hydrophilic compounds, (2) analyze acidic positive ion conditions, (3) operate at an overall higher organic content, and (4) optimize basic negative ions. Each reconstitution solvent employed fixed concentration standards to ensure injection and chromatographic consistency. MS analysis alternated between MS and data-dependent MSn scans using dynamic exclusion. The scan range varied slightly between methods but covered 70–1000 m/z. Raw data were extracted, peak-identified, and QC-processed using Metabolon’s hardware and software as described previously32. Compounds were identified by comparison to Metabolon library entries of purified standards or recurrent unknown entities.
Transcriptomic data
Previous research in this cohort performed RNA-seq on longitudinal whole blood samples collected in PAXgene tubes29. Transcriptional signatures were identified for pediatric TB diagnosis and response to successful TB treatment with data publicly available from NCBI (accession code PRJNA588242). For this study, transcriptomic and metabolomic analyses used samples from the same participants and time points.
Statistical analysis
Data were analyzed in R (https://cran.r-project.org). Differences in mean log2-transformed abundance between study groups were assessed by two-sample t-tests. ANOVA contrasts identified metabolites that differed significantly between groups and sample collection times. Data with p-values < 0.05 were considered significantly different. Exploratory analysis included visual inspection of volcano and principal component plots and construction of Venn diagrams of differentially abundant metabolites (DAMs, p < 0.05) across comparison groups. Log2-transformed metabolite abundance was Z-score-normalized between study groups and heatmaps were created with hierarchical clustering by Euclidean distance using ggplot233. Random forest analysis was employed to estimate how well each metabolite correctly classified each sample and decision tree classification was performed to detect the minimum number of features required to separate groups with maximum accuracy using the rpart package34. Classification model performance was measured by receiver operator characteristic (ROC) curve analysis. Overall accuracy was estimated by area under the ROC curve (AUC).
We have previously defined the molecular degree of perturbation (MDP) as a metric that compares mRNA transcript expression or metabolite abundance to the mean of expression or abundance in the reference group35,36. The accumulated standard deviation of all metabolites > 2 absolute standard deviations from the reference were calculated using the MDP package37. MDPs were correlated with age by Spearman correlation test and MDP was compared by sex using Mann–Whitney tests. Enrichment analysis was performed to correlate metabolomic and transcriptomic data using a hypergeometric test for the main categories of metabolic compounds using the Clusterprofile38 and Reactome Pathway Analysis packages39. Hierarchical cluster analysis was performed using a log2-transformed expression matrix to visualize patterns by study group, with a second heatmap made to cluster metabolite expression levels against the increase of MDP measurement within each group36.
Integrated pathway analysis correlated metabolite abundance with transcript abundance expressed by protein-coding gene for each participant at each time point. Associations with p < 0.05 and Pearson coefficients > 0.7 were plotted to assess the extent to which DAMs were correlated with relevant mRNA transcripts. Multi-omics factor analysis (MOFA) was employed to determine the degree to which metabolite abundance and mRNA expression variables changed together, as assessed by shared variance using the MOFA package40. Variables with shared variance were represented as latent factors based on a common variable model. Finally, each factor underwent over-representation analysis to determine the extent to which latent factors represented distinct canonical Reactome pathways.
Ethics statement
This CTRIUMPH study was approved by the Institutional Review Boards of Byramjee Jeejeebhoy Government Medical College (BJGMC) and the Johns Hopkins University School of Medicine, and all experiments were performed in accordance with institutional guidelines and regulations. All participants < 18 years old had written informed consent provided by their legal guardians. Written assent for participation was provided by participants who were 8 to < 18 years old.
Results
Study participants
Among the 141 pediatric CTRIUMPH participants recruited at BJGMC, 16 (11.3%) children had TB confirmed by positive culture (6), Xpert MTB/RIF (6), or tissue histopathology consistent with TB (7, not mutually exclusive). None were HIV-infected. The median age of these 16 children was 9.5 years (interquartile range 7–14 years), 8 (50%) were female, and eight had extrapulmonary disease (six lymph node, two meningitis, one dermatologic, Table S1). Of 32 selected controls without LTBI upon enrollment, 13 (40.6%) developed incident LTBI and none developed active TB during the 12-month follow-up period. These participants provided 121 plasma samples for analysis (Table S2).
TB-associated changes in metabolites
To study TB-associated metabolic dysregulation, we first compared plasma metabolite abundance among cases to abundance among controls at the time of enrollment. A total of 217 metabolites were identified across all samples, the full results of which are available in the supplementary materials (Table S3). Fifty seven DAMs were identified between enrollment samples (month 0) from cases and controls with p < 0.05 (Fig. 1A,B, Table 1). Of these, 29 DAMs were also differentially abundant between controls and cases mid-treatment (month 1) and between controls and cases at treatment completion (month 6), indicating continued metabolic abnormalities throughout treatment (Fig. 1B and Table 2). Additionally, 9 metabolites differentiated cases from controls at baseline (month 0), but were not differentially abundant between controls and cases after treatment (month 6). This included higher levels of 1-stearoyl-2-oleoyl-GPC (18:0/18:1), glutamate, and N-acetylneuraminate in cases compared to controls and lower levels of 1-(1-enyl-palmitoyl)-2-arachidonoyl-GPC, 1-(1-enyl-palmitoyl)-2-linoleoyl-GPC, aconitate [cis or trans], hydroxyproline, p-cresol sulfate, and prolylhydroxyproline in cases compared to controls. After evaluating heatmaps of differential abundance (Fig. 1C), decision tree analysis found that a single metabolite, N-acetylneuraminate, performed the best, with a log2-transformed abundance value < 20.76, achieving an AUC of 0.66 (Fig. 1D,E).

Differences in plasma metabolites between children with tuberculosis and healthy controls. (A) A volcano plot depicts the log2-fold change in metabolite abundance (x-axis) and the –log10 p-value (y-axis) for each metabolite between children with tuberculosis (“Cases”) and healthy controls at baseline. Positive and negative fold-change differences are depicted on the right and left sides of the graph, respectively. (B) A Venn diagram depicts the number of significantly differentially abundant metabolites for each comparison, including differences between controls and children with tuberculosis (cases) pre-treatment (baseline), mid-treatment (Month 1), and post-treatment (Month 6). (C) A hierarchical cluster analysis was employed to assess overall metabolite abundance between cases and controls. Data were log2-transformed and normalized by row Z-score. (D) A conditional decision tree was used to discriminate cases at the time of TB diagnosis from controls at study enrollment. The single best metabolite to differentiate cases and controls was N-acetylneuraminate. (E) Receiver operator characteristic (ROC) curve analysis demonstrating the sensitivity, specificity, and area under the curve (AUC) of N-acetylneuraminate to discriminate participants by TB status.
Response to TB treatment
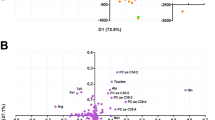
Analysis of treatment response among cases compared metabolite abundance in pre-treatment (month 0), mid-treatment samples (month 1), and post-treatment samples (month 6), with heatmaps demonstrating distinct clustering but some misclassification (Fig. 2A,B). Multiparametric ROC curve analysis found 15 metabolites with differential abundance over the course of treatment (Fig. 2C). Four metabolites (catechol sulfate, dimethylglycine, glycochenodeoxycholate, and trigonelline (N’-methylnicotinate)) differentiated pre-treatment from mid-treatment samples at 1 month with an AUC of 0.88. Ten metabolites (dihomolinoleate (20:2n6), glycochenodeoxycholate, linoleate (18:2n6), linolenate (18:3n3 or 3n6), nicotinamide, oleate/vaccenate (18:1), phenyllactate (PLA), pyridoxate, quinolinate, and trigonelline (N'-methylnicotinate)) differentiated mid-treatment (month 1) from post-treatment (month 6) with an AUC of 0.95, and 4 metabolites (gamma-glutamylalanine, gamma-glutamylglycine, glutamine, and pyridoxate) differentiated pre-treatment from post-treatment samples with an AUC of 0.86 (Fig. 2D).

Plasma metabolic dysregulation during the treatment of TB in children. Differentially expressed metabolites between pre-treatment (month 0), mid-treatment (month 1), and post-treatment (month 6) samples collected from children with tuberculosis. (A) The volcano plots demonstrate the fold difference in metabolite abundance between study groups on the x-axis and the -log10 p-value of each difference on the y-axis. Extreme values on the x-axis indicate greater differences in abundance and the highest − log10 p-value represents the most significantly altered metabolite. The figures represent the differential abundance of metabolites between treatment months 0 and 1 (top), 0 and 6 (middle), and 1 and 6 (bottom). (B) Heatmaps of Z-score normalized metabolite plasma concentrations for the metabolites that were significantly differentially abundant between study groups. (C) Receiver Operator Characteristics (ROC) curve analysis for the combination of significantly differentially abundant metabolites differentiating children with TB at each time point during treatment. (D) The Venn diagram demonstrates the number of significantly differentially abundant metabolites across comparisons based on months of treatment.
Conditional decision tree analysis identified three distinct metabolites that best classified patients with TB at different times during treatment compared to controls at enrolment: N-acetylneuraminate, quinolinate, and pyridoxate (Figure S2). In addition to the characteristics of N-acetylneuraminate described above, quinolinate was found to have an AUC of 0.77 (threshold log2-transformed abundance of < 18.07) for identification of TB following 1 month of treatment compared to controls at baseline, and pyridoxate was found to have an AUC of 0.87 (threshold log2-transformed abundance of < 19.21) for identification of TB at the completion of 6 months of treatment compared to controls at baseline. Although it maintained good discriminating ability, pyridoxate was not one of the DAMs between cases and controls at baseline (p = 0.076) or between cases later in treatment and controls at baseline (pre-treatment vs. end of treatment p = 0.009, mid-treatment vs. end of treatment p = 0.016).
Molecular degree of perturbation (MDP) is independent of participant age or sex
MDP was calculated for each sample to investigate overall differences in metabolite concentrations compared to baseline control samples. Plasma metabolites from TB cases at month 1 of treatment (orange) were the most perturbed, followed by the TB cases at baseline (green, Fig. 3A,B). MDP was not different by sex for any study group (Fig. 3C), but increasing MDP was significantly correlated with increasing age among cases at baseline (r = 0.519, p = 0.041, Fig. 3D). While study groups demonstrated significant differences according to MDP, this was poorly correlated with metabolic variance among individual participants within study groups, indicating poor representation of metabolite abundance in these children by MDP alone (Figure S1).

Molecular degree of perturbation among children with tuberculosis during treatment and uninfected controls, by participant age and sex. (A) Histograms show the single sample molecular degree of perturbation (MDP) score values for controls at baseline (blue), cases before treatment (green), cases after 1 month of treatment (orange), and TB cases after 6 months of treatment (dark yellow). (B) Out of these groups, MDP was significantly higher among cases before treatment (green) and cases after 1 month of treatment (orange) than among controls. MDP was not significantly different between cases after treatment (yellow) and controls (blue). (C) MDP was not significantly different by sex in any study group. (D) MDP was positively correlated with increasing age of participant among cases before treatment, but not among other study groups.
Integrated analysis of metabolomic and transcriptomic data
Three metabolites (N-acetylneuraminate, quinolinate, and pyridoxate) identified by decision tree analysis were correlated with mRNA transcription data to assess the extent to which metabolite abundance increased with increased gene transcription (positive correlation, Fig. 4A) or decreased with increased gene transcription (negative correlation). In total, 22 transcripts demonstrated strong correlation with N-acetylneuraminate, (1 positively correlated and 21 negatively correlated). The top positive and negatively correlated genes for N-acetylneuraminate were osteoclast-associated receptor (OSCAR) and CLYBL, respectively. Transcripts positively correlated with N-acetylneuraminate at the time of TB diagnosis were significantly represented among the pathway involving lymphoid immunoregulatory interactions (Fig. 4B). Similarly, 72 transcripts demonstrated strong correlation with quinolinate (12 positive and 60 negative correlations) and 22 transcripts with pyridoxate (18 positive and 4 negative correlations). The genes positively correlated with quinolinate did not adhere to any specific pathway, but those correlated with pyridoxate were significantly represented in the TP53-regulated metabolic pathway and in mitochondrial translation (elongation, termination, and translation). Transcripts with negative correlation with these metabolites did not cluster with any specific pathways.

Integration of metabolomics and transcriptomics data reveals a complex and multifaceted immune response to TB. (A) Correlation network based on gene expression values in TB cases. Highlighted genes were found to correlate with N-acetylneuraminate, quinolinate and pyridoxate with p-value < 0.05 and absolute value of R > 0.7. (B) List of pathways associated with genes found to be positively and negatively correlated with the above-mentioned 3 metabolites.
Multi‐omics factor analysis (MOFA) of metabolomic and transcriptomic data
Integrated metabolomic and transcriptomic analysis by MOFA was applied to 54 paired samples from the same participants and collection times (Fig. 5A). MOFA recognized 5 latent factors (LF), of which LF1, LF2, and LF4 correlated more strongly with the transcriptome, whereas LF3 correlated with the metabolome (Fig. 5B). Transcriptomics and metabolomics loadings revealed that LF1–5 captured several known important genes related to immune response pathways, including leukocyte immunoglobulin-like receptors (LILR), olfactory receptor 52K2, NADH-ubiquinone oxidoreductase chain 4 (MT-ND4), and heat shock protein 90α (Hsp90α) encoded genes. Similarly, several important metabolites were identified, including sphingolipids, 3-methylhistidine (3-MH), quinolinate, and palmitoyl sphingomyelin (Fig. 5C). Over-representation analysis of each LF found eukaryotic translation elongation, metabolism of proteins, immune system, and gene expression pathways most significantly represented within the 5 latent factors.

Downstream Multi‐Omics Factor Analysis (MOFA) disentangles the variability between metabolomics and transcriptomics data. The fitted MOFA model assessed the proportion of variance explained by each factor in each data modality. (A) Study overview and data types. Data modalities are shown in different rows (d = number of features) and samples (n) in columns. (B) The proportion of total variance (R2) explained by individual factors for each assay. (C) Absolute loadings of the top features of Factors 1 to 5 in the metabolomics (left panel) and transcriptomics (right panel) data.
Discussion
In order to improve the management and outcomes of pediatric TB, better diagnostic tools are desperately needed. In 2014, an NIH expert panel developed a blueprint of diagnostic biomarkers for pediatric TB7. According to the panel, such a biomarker could be obtained without invasive testing, like a blood test, and would work independent of age, nutrition, and HIV status. In this study, we performed an integrated blood-based metabolomic and transcriptomic analysis of children with and without TB to identify such a biomarker to indicate TB diagnosis and treatment response. We identified 57 DAMs between cases and controls, 29 of which remained differentially abundant throughout treatment, and 9 of which were differentially abundant before treatment, but did not remain differentially abundant throughout treatment. A single metabolite, N-acetylneuraminate, identified TB with an AUC of 0.66, while another metabolite, quinolinate, discriminated mid-treatment TB samples from control samples (AUC 0.77), and a third, pyridoxate, best discriminated post-treatment samples from control samples (AUC 0.87). The combination of 4 metabolites classified pre-treatment from post-treatment samples with an AUC of 0.86. Integrative analysis associated N-acetylneuraminate with mRNA transcription in the lymphoid immunoregulatory and neutrophil degranulation pathways. Finally, MOFA confirmed a significant additional contribution of immunomodulatory gene transcription along with sphingolipids, histidine metabolites, and cofactor and vitamin metabolites.
This study is unique in its metabolomic profiling of children with confirmed TB (rather than clinically diagnosed TB), as well as the use of decision tree analysis and integration of metabolomic with transcriptomic data to identify the most high-yield tests for both diagnosis and response to antitubercular treatment.
TB affects multiple host metabolic pathways, including metabolism of nitric oxide14, amino acids such as tryptophan15,17,18,25,41, glucose17, and lipids, including sphingomyelins, ceramides, eicosanoids, and phosphotidylcholines13,16,42. This study found potential diagnostic utility of N-acetyleneuraminate, the main sialic acid in human and mammalian cells, as well as a a nutrient and cell surface component of many pathogenic bacteria43,44. This molecule has previously been reported in higher abundance among TB patients, but not as a single marker for the diagnosis of TB18. Similarly, we found quinolinate to be the best marker to differentiate TB mid-treatment from controls. Quinolinate is a byproduct of the kynurenine pathway responsible for tryptophan catabolism, and is primarily derived from microglia and macrophages. Tryptophan metabolism has been associated with both pulmonary and extrapulmonary TB, as well as with HIV coinfection, which, like pediatric TB, is more frequently associated with extrapulmonary disease22,24. In addition, quinolinate levels are increased in a range of bacterial and viral infections45,46, as the inflammatory cytokines IFN-γ and TNF-α shuttle tryptophan from serotonin towards the kynurenine pathway47. We found quinolinate to differentiate mid-treatment cases from controls with an AUC of 0.77, which is lower than published data finding quinolinate to identify TB at the time of diagnosis (AUC = 0.84)16. This may reflect changes in inflammation and metabolism during the early phase of treatment, as quinolinate rose mid-treatment before falling at the end of treatment in our data (Table S3). Finally, pyridoxate was the metabolite that best differentiated cases following treatment completion from controls with an AUC of 0.87. Pyridoxate, a breakdown product of B6, is a potential biomarker for TB due to its role in human cellular immunity and the ability of MTB to consume host B620. This suggests that the differential abundance between TB patients post-treatment and controls may reflect resolving infection, although follow-up studies are needed to confirm this hypothesis.
This is not the first attempt to combine metabolites into a diagnostic signature for TB. Previous studies have achieved AUC values of 0.86–0.99 among adults, including 0.84 among people with HIV16,25,42. Pediatric studies are less common, however, with one study achieving AUC values between 0.76–0.81 using a variety of techniques, and another achieving an AUC of 0.98, representing better sensitivity of metabolomic signatures in this population than smear microscopy, Xpert MTB/RIF, or urine lipoarabinomannan testing12,13. The simplest metabolic biomarker we identified for TB, N-acetyleneuraminate, achieved an AUC of 0.66, which, while lower than values achieved in studies of adults with TB, is similar to the AUC of urine lipoarabinomannan (LAM) in children (AUC 0.67) and better than that of LAM among children without advanced HIV (AUC 0.46)48. Our data also found that the combination of 4 metabolites (gamma-glutamylalanine, gamma-glutamylglycine, glutamine, and pyridoxate) identified an initial treatment response with an AUC of 0.86, which—if confirmed in other studies including patients who fail treatment—represents improvement over smear and culture conversion to predict durable cure, which have only 24% and 40% sensitivity, respectively49. Previous studies have identified metabolomic signatures of treatment response, including one study identifying a 4 metabolite signature with 86.2% sensitivity, 85.2% specificity and an AUC of 0.9127, and another study finding changes of 5 metabolites during treatment50. These specific metabolites were not significantly different between pre- and post-treatment samples in our study, demonstrating the need to replicate diagnostic accuracy studies in special populations, such as children, before they are broadly employed.
The integrative analysis in this study did not support the addition of MDP to metabolomic assessment to improve diagnostic yield. Nevertheless, it did confirm the correlation of TB-induced metabolic dysregulation with lymphoid and non-lymphoid immunoregulation, as well as with mitochondrial translation. MOFA found strong correlations with transcriptomic and metabolomic data. In our previous work, we have defined transcriptional signatures of pediatric TB and treatment response, achieving AUCs for diagnosis of 0.57–0.90 and AUCs for treatment response of 0.50–0.90 in external datasets29. This suggests that there is room to improve diagnostic accuracy of metabolic assessments by incorporating multiple modalities, as in the current work.
This study has several limitations. While we have focused on an assessment of children with confirmed TB, these results may not be generalizable to adults, who represent the majority of TB patients worldwide. Similarly, TB has a well-known interaction with HIV coinfection, which was not assessed in this study population. While this study was designed to assess metabolic changes among children with confirmed TB, it is important to consider that the majority of children, particularly infants, treated for TB do not have confirmed disease. The choice to study children with confirmed TB likely raised the median age of study participants compared to clinically diagnosed pediatric TB patients2,3. Each of these may have contributed to distinct metabolic changes identified in our study population compared to other study populations.
In this single-site study of children with confirmed TB and exposed, uninfected household contacts of TB patients, we identified N-acetylneuraminate, quinolinate, and pyridoxate as candidate biomarkers for TB disease activity in children. The combination of 4 metabolites (gamma-glutamylalanine, gamma-glutamylglycine, glutamine, and pyridoxate) accurately identified treatment response. Integration of metabolomic and trancriptomic data from the same patients confirmed the involvement of several inflammatory pathways and improved interpretation of these biomarkers. Future validation studies will be needed to confirm these findings among other pediatric populations, including those coinfected with HIV. If successful, these tools may assist in the development of novel host-directed therapies for TB, as well as the use of predictors of treatment response to help shorten TB treatment. This would be particularly helpful for drug-resistant TB and for extrapulmonary TB, for which repeat microbiological assessment is often not possible during treatment.
Data availability
Data supporting the findings of this study are available within the article and its supplementary files, or are available from the authors upon request. Transcriptomics data analyzed in this manuscript are available from the NCBI sequence read archive (accession code PRJNA588242).
References
WHO. Global Tuberculosis Report 2019 297 (World Health Organization, Geneva, 2019).
Dodd, P. J., Gardiner, E., Coghlan, R. & Seddon, J. A. Burden of childhood tuberculosis in 22 high-burden countries: A mathematical modelling study. Lancet Glob. Health 2, e453–e459 (2014).
Graham, S. M. et al. Clinical case definitions for classification of intrathoracic tuberculosis in children: An update. Clin. Infect. Dis. 61(Suppl 3), S179–S187 (2015).
Zar, H. J., Hanslo, D., Apolles, P., Swingler, G. & Hussey, G. Induced sputum versus gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: A prospective study. Lancet (London, England) 365, 130–134 (2005).
Zar, H. J., Connell, T. G. & Nicol, M. Diagnosis of pulmonary tuberculosis in children: New advances. Expert Rev. Anti. Infect. Ther. 8, 277–288 (2010).
Nicol, M. P. & Zar, H. J. New specimens and laboratory diagnostics for childhood pulmonary TB: Progress and prospects. Paediatr. Respir. Rev. 12, 16–21 (2011).
Nicol, M. P. et al. A blueprint to address research gaps in the development of biomarkers for pediatric tuberculosis. Clin. Infect. Dis. 61(Suppl 3), S164–S172 (2015).
Little, K. M., Pai, M. & Dowdy, D. W. Costs and consequences of using interferon-gamma release assays for the diagnosis of active tuberculosis in India. PLoS ONE 10, e0124525 (2014).
Machingaidze, S. et al. The utility of an interferon gamma release assay for diagnosis of latent tuberculosis infection and disease in children: A systematic review and meta-analysis. Pediatr. Infect. Dis. J. 30, 694–700 (2011).
Cuevas, L. E. et al. Evaluation of tuberculosis diagnostics in children: 2. Methodological issues for conducting and reporting research evaluations of tuberculosis diagnostics for intrathoracic tuberculosis in children. Consensus from an expert panel. J. Infect. Dis. 205(Suppl 2), S209–S215 (2012).
Macallan, D. C. et al. Whole body protein metabolism in human pulmonary tuberculosis and undernutrition: Evidence for anabolic block in tuberculosis. Clin. Sci. (Lond. Engl. 1979) 94, 321–331 (1998).
Sun, L. et al. Utility of novel plasma metabolic markers in the diagnosis of pediatric tuberculosis: A classification and regression tree analysis approach. J. Proteome Res. 15, 3118–3125 (2016).
Andreas, N. J. et al. Performance of metabonomic serum analysis for diagnostics in paediatric tuberculosis. Sci. Rep. 10, 7302 (2020).
Butov, D. O., Kuzhko, M., Butova, T. & Stepanenko, G. Changes in nitric oxide synthase and nitrite and nitrate serum levels in patients with or without multidrug-resistant tuberculosis undergoing the intensive phase of antituberculosis therapy. Int. J. Mycobacteriol. 5(Suppl 1), S154–S155 (2016).
Zhou, A. et al. Application of (1)h NMR spectroscopy-based metabolomics to sera of tuberculosis patients. J. Proteome Res. 12, 4642–4649 (2013).
Feng, S. et al. Analysis of serum metabolic profile by ultra-performance liquid chromatography-mass spectrometry for biomarkers discovery: Application in a pilot study to discriminate patients with tuberculosis. Chin. Med. J. 128, 159–168 (2015).
Zhou, A. et al. Metabolomics specificity of tuberculosis plasma revealed by (1)H NMR spectroscopy. Tuberculosis (Edinburgh, Scotland) 95, 294–302 (2015).
Weiner, J. 3rd. et al. Biomarkers of inflammation, immunosuppression and stress with active disease are revealed by metabolomic profiling of tuberculosis patients. PLoS ONE 7, e40221 (2012).
Frediani, J. K. et al. Plasma metabolomics in human pulmonary tuberculosis disease: a pilot study. PLoS ONE 9, e108854 (2014).
Huang, H. et al. Plasma metabolites Xanthine, 4-pyridoxate, and d-glutamic acid as novel potential biomarkers for pulmonary tuberculosis. Clin. Chim.. Acta 498, 135–142 (2019).
Collins, J. M. et al. High-resolution plasma metabolomics analysis to detect Mycobacterium tuberculosis-associated metabolites that distinguish active pulmonary tuberculosis in humans. PLoS ONE 13, e0205398 (2018).
Che, N. et al. Integrated semi-targeted metabolomics analysis reveals distinct metabolic dysregulation in pleural effusion caused by tuberculosis and malignancy. Clin. Chim. Acta 477, 81–88 (2018).
Mason, S., Reinecke, C. J. & Solomons, R. Cerebrospinal fluid amino acid profiling of pediatric cases with tuberculous meningitis. Front. Neurosci. 11, 534 (2017).
van Laarhoven, A. et al. Cerebral tryptophan metabolism and outcome of tuberculous meningitis: An observational cohort study. Lancet. Infect. Dis 18, 526–535 (2018).
Henegar, C., Behets, F., Vanden Driessche, K., Tabala, M. & Van Rie, A. Impact of HIV on clinical presentation and outcomes of tuberculosis treatment at primary care level. Int. J. Tubercul. Lung Dis. 17, 1411–1413 (2013).
Luies, L., Reenen, M. V., Ronacher, K., Walzl, G. & Loots, D. T. Predicting tuberculosis treatment outcome using metabolomics. Biomark. Med. 11, 1057–1067 (2017).
Yi, W. J. et al. l-Histidine, arachidonic acid, biliverdin, and l-cysteine-glutathione disulfide as potential biomarkers for cured pulmonary tuberculosis. Biomed. Pharmacother 116, 108980 (2019).
Gupte, A. et al. Cohort for tuberculosis research by the Indo-US medical partnership (CTRIUMPH): Protocol for a multicentric prospective observational study. BMJ Open 6, e010542 (2016).
Tornheim, J. A. et al. Transcriptomic profiles of confirmed pediatric tuberculosis patients and household contacts identifies active tuberculosis, infection, and treatment response among indian children. J. Infect. Dis. 221, 1647–1658 (2020).
Evans, A. M., DeHaven, C. D., Barrett, T., Mitchell, M. & Milgram, E. Integrated, nontargeted ultrahigh performance liquid chromatography/electrospray ionization tandem mass spectrometry platform for the identification and relative quantification of the small-molecule complement of biological systems. Anal. Chem. 81, 6656–6667 (2009).
Dutta, N. K. et al. Inhibiting the stringent response blocks Mycobacterium tuberculosis entry into quiescence and reduces persistence. Sci. Adv. 5, 2104 (2019).
Dehaven, C. D., Evans, A. M., Dai, H. & Lawton, K. A. Organization of GC/MS and LC/MS metabolomics data into chemical libraries. J. Cheminform. 2, 9 (2010).
Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Springer, Berlin, 2016).
Breiman, L. Random forests. Mach. Learn. 2001, 5–32 (2001).
Prada-Medina, C. A. et al. Systems immunology of diabetes-tuberculosis comorbidity reveals signatures of disease complications. Sci. Rep. 7, 1999 (2017).
Oliveira-de-Souza, D. et al. Molecular degree of perturbation of plasma inflammatory markers associated with tuberculosis reveals distinct disease profiles between Indian and Chinese populations. Sci. Rep. 9, 8002 (2019).
Lever M, Russo P, Nakaya H. mdp: Molecular Degree of Perturbation calculates scores for transcriptome data samples based on their perturbation from controls., 2019.
Yu, G., Wang, L. G., Han, Y. & He, Q. Y. clusterProfiler: An R package for comparing biological themes among gene clusters. OMICS 16, 284–287 (2012).
Yu, G. & He, Q. Y. ReactomePA: An R/Bioconductor package for reactome pathway analysis and visualization. Mol. BioSyst. 12, 477–479 (2016).
Argelaguet, R. et al. Multi-omics factor analysis-a framework for unsupervised integration of multi-omics data sets. Mol. Syst. Biol. 14, e8124 (2018).
Cho, Y. et al. Identification of serum biomarkers for active pulmonary tuberculosis using a targeted metabolomics approach. Sci. Rep. 10, 3825 (2020).
Lau, S. K. et al. Metabolomic profiling of plasma from patients with tuberculosis by use of untargeted mass spectrometry reveals novel biomarkers for diagnosis. J. Clin. Microbiol. 53, 3750–3759 (2015).
Severi, E., Hood, D. W. & Thomas, G. H. Sialic acid utilization by bacterial pathogens. Microbiology (Read. Engl.) 153, 2817–2822 (2007).
Vimr, E. R., Kalivoda, K. A., Deszo, E. L. & Steenbergen, S. M. Diversity of microbial sialic acid metabolism. Microbiol. Mol. Biol. Rev. MMBR 68, 132–153 (2004).
Severino, P. C., Muller Gdo, A., Vandresen-Filho, S. & Tasca, C. I. Cell signaling in NMDA preconditioning and neuroprotection in convulsions induced by quinolinic acid. Life Sci. 89, 570–576 (2011).
Stone, T. W. Endogenous neurotoxins from tryptophan. Toxicon 39, 61–73 (2001).
Guillemin, G. J. Quinolinic acid, the inescapable neurotoxin. FEBS J. 279, 1356–1365 (2012).
LaCourse, S. M. et al. Stool Xpert MTB/RIF and urine lipoarabinomannan for the diagnosis of tuberculosis in hospitalized HIV-infected children. AIDS (Lond. Engl.) 32, 69–78 (2018).
Horne, D. J. et al. Sputum monitoring during tuberculosis treatment for predicting outcome: Systematic review and meta-analysis. Lancet. Infect. Dis 10, 387–394 (2010).
Che, N. et al. Decreased serum 5-oxoproline in TB patients is associated with pathological damage of the lung. Clin. Chim. Acta 423, 5–9 (2013).
Acknowledgements
We would like to acknowledge Metabolon Inc. for generation of the metabolomics data. We would like to thank all the CTRIUMPH participants and study staff.
Funding
This publication was made possible by support from the Johns Hopkins University Center for AIDS Research (NIH P30AI094189). CTRIUMPH was supported by the NIH/DBT RePORT India Consortium with funding in whole or in part from the Government of India’s (GOI) Department ofBiotechnology (DBT), the Indian Council of Medical Research (ICMR), the United States National Institutes of Health (NIH), National Institute of Allergy and Infectious Diseases (NIAID), Office of AIDS Research (OAR), and distributed in part by CRDF Global. ND was supported by a Scholar Grant for Faculty Development and Institute for Clinical and Translational Research (UL1 TR 001079) and Nexus Biomarkers and Diagnostic. ND, AG, and PK were supported by a supplement from the AIDS Clinical Trials Group (UM1 AI68636-12). AG, NG, VM, is also supported by NIAID/NIH under award number UM1AI069465. PK was supported by NIH/NIAID (K24AI143447). ND and PK were supported by the U.S. Civilian Research & Development Foundation distributed by CRDF Global. JAT was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health (NIH NIAID grants K23AI135102 and R21AI122922), the NIH/Fogarty Global Health Fellows Program Consortium (R25TW009340), and the Johns Hopkins University School of Medicine Clinician Scientist Career Development Award. The contents of this publication are solely the responsibility of the authors and do not represent the official views of the DBT, the ICMR, the NIH, or CRDF Global. Any mention of trade names, commercial projects, or organizations does not imply endorsement by any of the sponsoring organizations. The funding sources had no role in the study design, data collection, data analysis, data interpretation or writing of the report.
Author information
Authors and Affiliations
Contributions
Conceived the studies: N.D., J.T., A.G., B.A., P.K. Developed the methodology: N.D., J.T., K.F., M.P., R.T., A.K., C.V., V.K., N.P., S.Y., A.K., A.G., N.G., V.M., A.G., B.A., P.K. Provided data and analysis: N.D., J.T., K.F., M.P., R.T., A.K., C.V., V.K., N.P., S.Y., A.K., A.G., N.G., V.M., A.G., B.A., P.K. Wrote the manuscript, which was edited by all authors: N.D., J.T., K.Y., A.G., B.A., P.K.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dutta, N.K., Tornheim, J.A., Fukutani, K.F. et al. Integration of metabolomics and transcriptomics reveals novel biomarkers in the blood for tuberculosis diagnosis in children. Sci Rep 10, 19527 (2020). https://doi.org/10.1038/s41598-020-75513-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-75513-8
- Springer Nature Limited