
Abstract
Cardiovascular diseases (CVD) are responsible for the majority of deaths in Brazil and worldwide, and constitute an important share of non-transmissible diseases. The objective of this study is to analyze the mortality trends of the three main CVD in Brazil and its geographic regions: acute myocardial infarction, stroke, and heart failure. Data predictions until 2030 were also carried out. An ecological study is presented herein, with data for the period 2001–2015. Mortality from these diseases was evaluated by annual trends, and grouped in five-year intervals for the predictions until 2030. All data are publicly available. Acute myocardial infarction was the leading isolated cause of death. Brazilian trends revealed a decrease in the three diseases, with different patterns across geographic regions. The Southeast, South, and Midwest regions presented reductions for the three diseases. The predictions indicated higher rates for men. There was also a reduction in the risk of death from these diseases for Brazil and, despite the different mortality patterns for the three diseases, the Southeast region presents, primarily, lower predicted rates than the other regions. The assessment of trends and predictions for the three main CVD in Brazil revealed general decreasing trends with differences across the geographic regions.
Similar content being viewed by others


Introduction
According to the World Health Organization (WHO), non-transmissible diseases are responsible for 71% of deaths in the world1 and 74% in Brazil2. Non-transmissible diseases include chronic respiratory diseases, cancers, diabetes, mental conditions, and diseases of the circulatory system (also referred to as cardiovascular diseases—CVD)1, which are responsible for the majority of disabilities3 and deaths worldwide3,4. In Brazil, CVD cause 28% of deaths2, among which ischemic heart diseases are highlighted as the leading cause, followed by stroke3,5,6. Together, these categories account for 1/3 of global deaths7.
The risk factors for these diseases include the consumption of tobacco2,8,9,10,11,12, arterial hypertension2,5,6,9,12,13,14,15, inadequate diet5, sedentarism, excessive consumption of alcohol, environmental pollution1,2,5,9, the presence of metabolic alterations16, high cholesterol3,15,17, diabetes6,8,9,11,13, and overweight and obesity2,8,9,11,14,15. Regarding the moderate consumption of alcohol, some findings have suggested lower chances of developing CVD, but no causal conclusions were drawn13.
Risk factors can also be classified according to CVD, where dyslipidemia, consumption of tobacco, and diabetes are more associated with ischemic heart diseases. Cerebrovascular diseases are more associated with hypertension18 and modifiable factors related to arteriosclerosis19.
The assessment of these risk factors is very important6, along with analysis of health determinants and social iniquities8. Nevertheless, health promotion and prevention actions are also essential, along with the monitoring of trends and their dynamics throughout the years20,21. This identifies the regions with higher potential mortality risks due to CVD, and helps plan public policies more effectively. In this context, the objective of this study is to analyze the mortality trends due to the primary CVD (acute myocardial infarction, stroke, and heart failure) in Brazil and its geographic regions, and carry out data predictions until 2030.
Methods
Study design
An ecological study is presented herein, with mortality data for the period 2001–2015. The proportion of deaths for each category of Chapter IX of the 10th revision of International Classification of Diseases (ICD) was calculated to determine the primary three CVD. For men and women, the main three CVD were: acute myocardial infarction (I21)—AMI, stroke not specified as haemorrhage or infarction (I64), and heart failure (I50).
After calculations of the main CVD in the period, annual death data, per sex, geographic region, and age groups were obtained from the website of the Department of Statistics of the Brazilian Unified Health System (DATASUS), which originated from the Mortality Information System (SIM). All data are publicly available. Trend assessment employed these data, and for the calculation of predictions, data were grouped in five-year intervals until 2030.
Population data are provided by the Brazilian Institute of Geography and Statistics (IBGE). Census data and inter-census projections were utilized, up to 2012. For the period 2013–2030, population projections were employed, also available from IBGE. Data were selected per age group, for each geographic region, year, and sex. Eighteen age groups were evaluated (five-year intervals), ranging from 0–4 years old to 80–85 years old, with the last age group covering the deaths of people over the age of 85.
In this study, it was calculated the standardized rates for the standard world population. These rates considered a population denominator of 100,000 inhabitants, according to Segi22. The rate standardization method is used to correct the effect of different age structures in the analysis performed for different populations. Thus, it enables the comparison of the mortality for the studied diseases in different populations and periods. Even if the populations of each region present different age structures.
Despite improvements in the quality of Brazilian data in recent decades, with broader coverage of SIM and a decrease in the percentage of ill-defined deaths23,24,25, there are differences in data quality across the regions24. Data correction26 is therefore required for a better estimation23,24,27. This study applies a correction to improve the reliability of data, based on a method available at the DATASUS website28. According to this method, redistribution of data by sex and age were employed for the correction procedure, along with adjustments regarding the completeness of death records. The difference in percentage terms was calculated in relation to the number of deaths notified to SIM. These data, however, are only available from Chapter IX of ICD-10 and enable the formulation of the correction factor for the ICD factor28.
The correction factor calculated for Chapter IX (diseases of the circulatory system) considered each age group, sex, and geographic region, and was applied to data of each selected ICD, respecting the correspondence with age group, geographic region, period, and sex. The factor was calculated for the period 2001–2013, according to the equation: 1 + [(redistributed deaths – notified deaths to SIM)/notified deaths to SIM]. Due to the unavailability of data for the period 2014–2015, the 2013 data correction factor was applied28.
The corrected number of deaths was obtained by multiplying the correction factor by the number of deaths for each of the three ICD-10 categories, for the most common CVD, using the equation: Nº of corrected deaths = Nº of deaths per ICD category x correction factor for ICD chapter.
Trend analysis
Trend analysis used annual data, from 2001 to 2015, and the software Joinpoint Regression Program29. Analysis of significant variations in the trend curve utilized the annual percentage change (APC), considered for a statistic significance of p < 0.05, which determines the existence of increasing or decreasing rates throughout time. Cases with no statistical significance were treated as “stable”. The number of significant changes in the trend curve indicates the number of joinpoints. This assessment employed the simplest model that justified the changes in slope.
Predictions
Data prediction considered the addition of annual data for the years constituting each of the five-year intervals (2001–2005; 2006–2010; 2011–2015), with prediction for the subsequent five-year intervals (2016–2020; 2021–2025; 2026–2030), obtaining a mean rate for the quinquennial periods. We use standardized rates per 100,000 inhabitants. The procedure used the statistical package Nordpred, in R software, version 2.8.1, compatible with the aforementioned data packages.
The change occurring between the last observed period (2011–2015) and the last predicted period (2026–2030) was also assessed, according to the changes in death risks for the considered diseases and modifications in the structure and size of population, according to the equation proposed by Möller et al.30: Δtot = Δrisk + Δpop = (Nfff—Nooo) = (Nfff—Noff) + (Noff—Nooo).
Where ∆tot is the total variation; ∆risk is the variation due to changes in the risk of death for the evaluated disease; ∆pop is the variation due to changes in population structure and size; Nfff is the number of predicted cases for the last predicted period; Nooo is the number of deaths in the last observed period; Noff is the number of deaths in the last predicted period, maintaining the rates of the last observed period, and Nfff – Nooo is the annual change in the number of deaths.
Results
Between the years of 2001 and 2015, a total of 2,438,218 deaths were registered in men and 2,209,247 in women due to CVD. This amount represents, respectively, 25.90% and 31.54% of the overall deaths in Brazil for the period, which establishes these diseases as the main causes of deaths in the country.
The three CVD with the higher percentages of deaths were identified, for the same period, as AMI (27.04% in men and 20.75% in women), stroke (13.61% in men and 14.51% in women), and heart failure (8.13% in men and 9.60% in women). AMI is the single disease that caused the most deaths in the country, adding 7% to the total of deaths in the country for men and 6.54% for women.
Trends
Trend analysis in Brazil is presented in Table 1. For AMI, decreasing trends were identified for men, with APC = -1.7(-2.1;-1.3), and women with APC = -2.2(-2.6;-1.8). Regarding geographic regions, among women, there were reductions for the Southeast, South, and Midwest regions. The North presented stability. For the Northeast, there was a joinpoint in 2006 and another in 2010, with the first period showing increasing rates APC1 = 1.8(0.1;3.5), followed by two stable periods. For men, the North region presented stability. For the Southeast, South, and Midwest regions, reductions were identified. For the Northeast, two joinpoints occurred, in 2006 and 2010, with a stable period, followed by a reduction APC2 = -1.5(-2.5;-0.5) and an increase APC3 = 1.7(1.3;2.2).
For stroke in Brazil, there was a reduction in men, APC = -5.3(-5.7;-4.9), and women, APC = -5.8(-6.3;-5.3). Regarding geographic regions, there were decreases for all regions, for men and women, with no joinpoints.
For heart failure, Brazil presented a reduction for men and women, respectively APC = -5.0(-5.6;-4.5) and APC = -5.5(-6.0;-4.9). Considering geographic regions, reductions were identified for the North, Southeast, and Midwest regions, for both sexes. The Northeast presented a joinpoint for men and women, in 2011, with an initial decreasing period with APC1 = -8.0(-9.1;-6.9) for women and APC1 = -7.3(-8.4;-6.1) for men, followed by stable periods for both sexes.
Predictions
Tables 2, 3 and 4 presents the corrected number of deaths, divided into age groups (0–19, 20–39, 40–59, and over 60 years old), along with the crude and adjusted rates considering the standard world population for the three primary cardiovascular diseases in Brazil and its geographic regions for the five-year intervals observed (2001–2005; 2006–2010; 2011–2015) and predicted (2016–2020; 2021–2025; 2026–2030).
The predictions indicate a reduction in Brazilian rates, for the three studied diseases, for men and women. The geographic regions, however, present different patterns. For AMI, the South and Southeast presented a more pronounced reduction and lowest rates for the predicted periods, for men and women. For stroke, the lowest rates occurred for the Southeast and Midwest, for the observed and predicted periods, for men and women. For heart failure, among men, the lowest predicted rates occurred in the Southeast and Midwest, and for women, the lowest rates occurred in the Midwest and Northeast.
The ratio between the rates of men and women is always higher than one, except for the prediction of the period 2026–2030 for the Midwest region, where the female rate is higher. Among the cardiovascular diseases studied, AMI presents the most significant difference between men and women, surpassing the 2:1 ratio in different regions and periods.
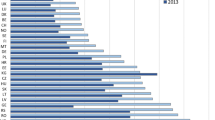
Another assessment carried out from the predictions is the change in the risk of death by the studied diseases in comparison with changes in population structure and size. Comparison of periods 2011–2015 and 2026–2030 revealed, for Brazilian data, a reduction in the absolute number of deaths due to stroke, and increases for AMI and heart failure for men and women. For the three diseases, there was a reduction in the risk of falling ill from each evaluated disease. The increase verified for AMI and heart failure was justified by changes in population structure and size (Fig. 1).

Change in death risk and the in structure and size of population, between the last observed period (2011–2015) and the last predicted period (2026–2030).
For the geographic regions, Fig. 1 depicts an increase in the death risk due to stroke in men of the South region. Also, there was a slight increase in the death risk due to AMI in women of the North region. For the remaining regions, there were reductions in the risk of falling ill due to all the CVD studied, with changes in the number of deaths justified by changes in population structure and size.
Discussion
The study of mortality trends for the main CVD enabled the identification of reductions in the Brazilian rates for the three evaluated diseases. This reduction was also evidenced by other CVD studies that employed different methods31,32,33,34,35 and corroborated by studies that applied joinpoint assessment36,37.
The predictions indicated a decreasing risk of death due to these diseases in Brazil, for the predicted data. Concerning geographic regions, varied patterns were verified among the diseases, with better perspectives of reduction for the regions with higher socioeconomic levels31,35,38. This could be related to factors such as social development, risk behavior, access and coverage of the health system in each region35,39,40, as Brazil has continental dimensions and evident regional inequalities39,41,42. Another important result was the higher mortality in men, which has also been reported by other studies24,32,35.
Despite the decrease in rates, an increase is expected in the number of deaths due to AMI and heart failure. This finding is explained by the aging process of the Brazilian population, with older age groups being more affected by these diseases4,5,8,21. In this way, although decreasing rates were identified, this process implies in the necessity of a better structure of health systems to address the situation34, especially in more critical regions, with worse access to healthcare34. Therefore, population aging has generated several demands towards the health system, considering the necessities of reducing the burden of the disease and promoting healthy aging32,33,36,39,43.
Regarding stroke, a reduction was observed in the rates and in the number of deaths. This could be due to the evolution of the fight against modifiable risk factors for this disease and improvements in treatment. Scientific literature indicates a similar result with developed countries, where better conditions exist for prevention and treatment3,43. However, similar results were also found amongst African countries12.
Another important finding is that mortality due to ischemic heart diseases surpassed that of cerebrovascular diseases in Brazil in recent decades. Other studies report similar results in Brazil for 1980–201218 and 1990–201619, associated with broader access to diagnosis and treatment of systemic arterial hypertension, the primary risk factor for cerebrovascular diseases18. Nevertheless, cerebrovascular diseases cause a significant impact on populations. It is estimated that, in 2015, approximately 9 million first-time brain accidents occurred in the world7 with 5.5 million deaths in 2016, while 116.4 million people recovered with side-effects in the same year19.
This study also identified AMI as the single disease that caused the most deaths in Brazil, in men and women. This disease is also the primary cause of death in the world and the main cause of health loss (except for Sub-Saharan Africa). In 2015, the estimative was 7.3 million heart attacks, with 100.6 million people living with arterial heart diseases7.
Despite being the single leading cause of deaths in Brazil, decreasing mortality trends were identified for AMI during the studied period, except for the Northeast region for men, where there were 2 joinpoints, with a increasing period after 2010. The Southeast, South, and Midwest regions presented reductions in rates for men and women. This finding is probably associated with a better structure of the health system in these regions and better access to healthcare32. Data from 2012 show that important health coverage indicators are better in these three regions, with a higher number of medical appointments per inhabitant, higher proportion of the population covered by health plans, and higher proportion of people that had a medical consultation in the previous 12 months. Resource indicators must also be mentioned, such as a higher number of hospital beds per inhabitant, and higher average expense per hospitalization44.
Heart failure must also be highlighted as the disease with the highest number of deaths among those under 20 years of age, possibly associated with congenital heart issues. The adverse effects of heart failure include morbidity and costs of treatment and hospitalizations, as well as difficult recovery19,45.
When analyzing regional differences in CVD mortality in Brazil, the three primary cardiovascular diseases present reductions for the Midwest region. However, it is expected that female rates surpass male rates for the Midwest region regarding heart failure, in the predicted period 2026–2030. Decreasing trends were revealed for the rates of the South and Southeast regions, for the three main CVD studied herein, which has already been reported by scientific literature31,32,35,38. These results can be explained by better conditions for the diagnosis and treatment in these geographic regions, which concentrate the highest gross domestic products and human development indices of the country and imply in better survival conditions35,46.
Besides, the Southeast and Suth regions present a better healthcare structure for the attention to chronic diseases. These regions present the highest life expectancies within Brazil, with healthier lifestyles, besides being the wealthiest. These factors reflect differences in the access and quality of health services across geographic regions38,47. The North and Northeast regions face additional difficulties such as poverty, lack of good quality education, and unplanned urbanization, which can negatively impact cardiovascular health, leading to unfair distribution of income, resources, and power3,35. These conditions can be associated with the increasing period identified for AMI in the Northeast, among men, after 2010.
The North and Northeast regions present the highest predicted rates for the three diseases studied. The different Brazilian regions experience different stages of the epidemiological transition, and more impoverished areas face more challenges to control and prevent non-transmissible chronic diseases35,47.
In this context, the WHO established a global action plan (2013–2020) with priorities directed to the prevention and control of non-transmissible chronic diseases. The priorities outlined include the reduction of risk factors, promotion of health, and mapping of areas with the occurrence of these diseases. Social, economic, behavioral, and politic determinants must be known to guide the public policies and measures aimed at preventing and controling these diseases20.
Nevertheless, more stringent objectives were stipulated during a 2015 meeting that involved several countries, with the creation of the “Sustainable Development Goals – SCG”, based on the development objectives of the millennium. One of the goals established is directed to health and wellbeing, which is to reduce 1/3 of non-transmissible diseases through prevention and treatment, while also promoting mental health and wellness48. These global goals were established to reduce the impact of these diseases, but it is also fundamental to control and reduce the exposure to risk factors throughout the years. These diseases are better confronted when lifestyle habits are improved, with reductions in the consumption of sugar and alcohol47. A higher exposure to risk factors can cause an increase in future rates8,9,42.
Other authors have remarked on the importance of a healthy diet, emphasizing its impact on the health and prevention of CVD15,34,49. Some of the unhealthy habits that cause CVD include the high consumption of sodium, trans fats, cholesterol, and salt, along with the low consumption of fiber, fruit, vegetables, nuts, seeds3,12,15,17,49, and omega 3@@@49. In contrast, the presence of flavonoids in the diet presents an inversely proportional association with cardiovascular disease mortality50.
In Brazil, reduction of the exposure to CVD risk factors has occurred through the control of hypertension, diabetes, dyslipidemias, obesity2,20,35,38,42 and tobacco prevention32,34,38,42. The country has promoted better access to the medical treatment of these conditions and has been stimulating the practice of more healthy lifestyles, which include physical activity and campaigns against tobacco, through public policies2,20,35. The broader access to the medical treatment of hypertension, diabetes, and dyslipidemias started in 2004 with the creation of the “popular pharmacy” program, aimed at the universalization of access to medicines51. The program was extended and experienced changes related to financing and destination of funds52. Despite the good results obtained, a better access to treatment is not sufficient, on its own, to guarantee adhesion. Activities directed to the promotion of health and education of the population are also necessary.
Regarding the control and prevention of tobacco use, Brazil has promoted legislative and educative measures. In this context, the actions of the National Agency of Sanitary Vigilance (ANVISA) are crucial to promote better health, regulations, control, and inspection of products related to tobacco. In 1999, within ANVISA, the administration of tobacco-derived products was created, and, throughout the following years, different regulations were elaborated to restrict the advertising and use of such products53.
Besides the measures related to control the consumption of tobacco, the Federal Government launched the Health Academy Program in 2011 to promote the practice of physical activity, healthy eating habits, and positive changes in lifestyle. Within the program, primary attention plays a vital role in health promotion and prevention activities54 and stimulates healthy habits in the population. However, there are still no studies that confirm the results of this program concerning CVD.
The strengthening of public policies for the prevention, treatment, and vigilance of CVD must carefully consider regional differences. Studies focusing on the trends and predictions of mortality rates enables actions to be planned and redirected. These studies support planning efforts and the creation of new health policies, along with the assessment and improvement of existing policies guided to the promotion and prevention of health33,43,47,55 and best allocation of health-destined funds47.
A limitation of this study, which is inherent to ecological studies, is the impossibility of establishing causal inferences due to the use of aggregate data. In this context, the level of regional data coverage and completeness of SIM could have influenced the results of trends. Also, data from the ICD-10 chapter (diseases of the circulatory system) was employed for the calculation of the correction factor, as there are no data corrected by category for ICD-10 in DATASUS. However, this limitation is minimized because this study considers the three diseases with the highest mortalities and takes into account separation by sex and age group, which provides a more trustworthy correction factor.
In conclusion, the assessment of trends and predictions for the three main CVD in Brazil revealed general decreasing trends. This national decrease, however, includes differences across the geographic regions. Regions with higher purchase power present better perspectives for the reduction of mortality in future studies. In this sense, governmental policies must be strengthened, especially regarding the control of modifiable risk factors, focusing on reaching the goals stipulated by WHO and SDG.
References
WHO. Noncommunicable diseases (NCDS) and mental health: challenges and solutions. 333, 1, 22 (2014).
WHO. Brazil NCD 2018 WHO. Noncommunicable dis ctry profiles. https://www.who.int/nmh/countries/bra_en.pdf?ua=1 (2019).
Thomas, H. et al. Global Atlas of Cardiovascular Disease 2000–2016: the path to prevention and control. Glob. Heart. 13(3), 143–163. https://doi.org/10.1016/j.gheart.2018.09.511 (2018).
GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159), 1736–1788. https://doi.org/10.1016/S0140-6736(18)32203-7 (2018).
Moran, A. E., Roth, G. A., Narula, J. & Mensah, G. A. 1990–2010 Global cardiovascular disease Atlas. Glob. Heart. 9(1), 3–16. https://doi.org/10.1016/j.gheart.2014.03.1220 (2014).
Mokdad, A. H. et al. Global, regional, national, and subnational big data to inform health equity research: perspectives from the Global Burden of Disease Study 2017. Ethn Dis. 29(Suppl 1), 159–172. https://doi.org/10.18865/ed.29.S1.159 (2019).
American College of Cardiology. "Cardiovascular disease causes one-third of deaths worldwide: 'Alarming trends' for countries in all stages of development." ScienceDaily.www.sciencedaily.com/releases/2017/05/170517143625.htm (2020).
Wilkins, E. et al. European cardiovascular disease statistics 2017 (European Heart Network, Brussels, 2017).
Prabhakaran, D. et al. The changing patterns of cardiovascular diseases and their risk factors in the states of India: the Global Burden of Disease Study 1990–2016. Lancet Glob. Health 6(12), e1339–e1351. https://doi.org/10.1016/S2214-109X(18)30407-8 (2018).
Villela, L. M., Gomes, F. E. & Meléndez, J. G. V. Tendência da mortalidadepordoençascardiovasculares, isquêmicas do coração e cerebrovasculares. Rev enferm UFPE online 8(9), 3134–3141. https://doi.org/10.5205/reuol.5960-55386-1-ED.0809201423 (2014).
Roth, G. A. et al. Estimates of global and regional premature cardiovascular mortality in 2025. Circulation 132(13), 1270–1271. https://doi.org/10.1161/CIRCULATIONAHA.115.016021 (2015).
The Institute for Health Metrics and Evaluation (IHME). Burden of diabetes and cardiovascular diseases in Africa. 1990–2015. W Univ Washingt (Cvd)(2015).
Massa, K. H. C., Duarte, Y. A. O. & ChiavegattoFilho, A. D. P. Analysis of the prevalence of cardiovascular diseases and associated factors among the elderly, 2000–2010. Ciênc. saúdecoletiva 24(1), 105–114. https://doi.org/10.1590/1413-81232018241.02072017 (2019).
Nascimento, B. R. et al. Cardiovascular disease epidemiology in portuguese speaking countries: data from the global burden of disease, 1990 to 2016. Arq. Bras. Cardiol. 110(6), 500–511. https://doi.org/10.5935/abc.20180098 (2018).
Tehrani-Banihashemi, A. et al. Burden of cardiovascular diseases in the eastern mediterranean region, 1990–2015: findings from the Global Burden of Disease 2015 study. Int J Public Health 63, 137–149. https://doi.org/10.1007/s00038-017-1012-3 (2018).
Hamer, M. & Stamatakis, E. Metabolically healthy obesity and risk of all-cause and cardiovascular disease mortality. J. Clin. Endocrinol. Metab. 97(7), 2482–2488. https://doi.org/10.1210/jc.2011-3475 (2012).
Hayward, R. H. Cardiovascular disease in the aged. Postgrad. Med. 45(6), 203–208. https://doi.org/10.1080/00325481.1969.11697179 (2016).
Mansur, A. P. & Favarato, D. Trends in mortality rate from cardiovascular disease in Brazil, 1980–2012. Arq. Bras. Cardiol. 107(1), 20–25. https://doi.org/10.5935/abc.20160077 (2016).
GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 18, 439–458. https://doi.org/10.1016/S1474-4422(19)30034-1 (2019).
World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. https://apps.who.int/iris/handle/10665/94384 (2013).
Roth, G. A. et al. Demographic and epidemiologic drivers of global cardiovascular mortality. N. Engl. J. Med. 372(14), 1333–1341. https://doi.org/10.1056/NEJMoa1406656 (2015).
Segi, M. Cancer Mortality for Selected Sites in 24 Countries (1950–57) (Department of Public Health, Tohoku University of Medicine, Sendai, Japan, 1960).
De Lima, E. E. C. & Queiroz, B. L. Aevolução do sistema de registro de mortalidade no Brasil: Mudanças no perfil de mortalidade, cobertura do registro de óbitos e as causas mal definidas de morte. Cadernos de SaudePublica 30(8), 1721–1730. https://doi.org/10.1590/0102-311X00131113 (2014).
Queiroz, B. L., Freire, F. H. M. A., Gonzaga, M. R. & De Lima, E. E. C. Estimativas do grau de cobertura e da mortalidadeadulta (45q15) para as unidades da federação no Brasil entre 1980 e 2010. RevistaBrasileira de Epidemiologia 20, 21–33. https://doi.org/10.1590/1980-5497201700050003 (2017).
Lotufo, P. A. The pace of reduction of cardiovascular mortality in Brazil (1990 to 2017) is slowing down. Sao Paulo Med. J. 137(1), 3–5. https://doi.org/10.1590/1516-3180.2018.1371090219 (2019).
Bierrenbach, A. L. et al. Redistribution of heart failure deaths using two methods: Linkage of hospital records with death certificate data and multiple causes of death data. Cadernos de SaudePublica 35(5), 1–10. https://doi.org/10.1590/0102-311X00135617 (2019).
Schmertmann, C. P. & Gonzaga, M. R. Bayesian estimation of age-specific mortality and life expectancy for small areas with defective vital records. Demography 55(4), 1363–1388. https://doi.org/10.1007/s13524-018-0695-2 (2018).
Santos, C. A. & Souza, D. L. B. Melanoma mortality in Brazil: trends and projections (1998–2032). Cienc e SaudeColetiva. 24(4), 1551–1561. https://doi.org/10.1590/1413-81232018244.13932017 (2019).
National Cancer Institute. Surveillance research program. Methods and tools. Joinpoint trend analysis software [computer program]. Version 4.0, USA. p. 4 (2019).
Møller, B. et al. Prediction of cancer incidence in the nordic countries up to the year 2020. Eur J Cancer Prev. pp S1–S96 (2002).
Guimarães, R. M. et al. Regional differences in cardiovascular mortality transition in Brazil, 1980 to 2012. RevistaPanamericana de SaludPublica Pan Am J Public Health 37(2), 83–89 (2015).
Brant, L. C. C. et al. Variações e diferenciais da mortalidadepordoença cardiovascular no Brasil e emseusestados, em 1990 e 2015: Estimativas do EstudoCarga Global de Doença. RevistaBrasileira de Epidemiologia 20, 116–128. https://doi.org/10.1590/1980-5497201700050010 (2017).
De Souza, M. D. F. M., Malta, D. C., França, E. B. & Barreto, M. L. Changes in health and disease in Brazil and its states in the 30 years since the unified healthcare system (SUS) was created. Ciencia e SaudeColetiva 23(6), 1737–1750. https://doi.org/10.1590/1413-81232018236.04822018 (2018).
Ribeiro, A. L. P. et al. Cardiovascular health in Brazil trends and perspectives. Circulation 133(4), 422–433. https://doi.org/10.1161/CIRCULATIONAHA.114.008727 (2016).
Baptista, E. A. & Queiroz, B. L. The relation between cardiovascular mortality and development: a study of small areas in Brazil, 2001–2015. Demogr. Res. 41(51), 1437–1452. https://doi.org/10.4054/DEMRES.2019.41.51 (2019).
Lloyd-Sherlock, P., Ebrahim, S., Martinez, R., McKee, M. & Ordunez, P. Reducing the cardiovascular disease burden for people of all ages in the Americas region: analysis of mortality data, 2000–15. Lancet Glob. Health 7(5), e604–e612. https://doi.org/10.1016/S2214-109X(19)30069-5 (2019).
Lotufo, P. A. Trends in cardiovascular diseases and heart disease death rates among adults aged 45–64: Brazil, 2000–2017. Sao Paulo Med. J. 137(3), 213–215. https://doi.org/10.1590/1516-3180.2019.1373.220719 (2019).
Baptista, E. A. & Queiroz, B. L. Spatial analysis of mortality by cardiovascular disease in the adult population: a study for Brazilian micro-regions between 1996 and 2015. Spat. Demogr. 7(1), 83–101. https://doi.org/10.1007/s40980-019-00050-6 (2019).
Baptista, E. A., Queiroz, B. L. & Rigotti, J. I. R. Decomposition of mortality rates from cardiovascular disease in the adult population: a study for Brazilian micro-regions between 1996 and 2015. RevistaBrasileira de Estudos de Populacao https://doi.org/10.20947/S102-3098a0050 (2018).
Rasella, D., Harhay, M. O., Pamponet, M. L., Aquino, R. & Barreto, M. L. Impact of primary health care on mortality from heart and cerebrovascular diseases in Brazil: a nationwide analysis of longitudinal data. BMJ (Online) 349(July), 1–10. https://doi.org/10.1136/bmj.g4014 (2014).
Lotufo, P. A., Fernandes, T. G., Bando, D. H., Alencar, A. P. & Benseñor, I. M. Income and heart disease mortality trends in Sao Paulo, Brazil, 1996 to 2010. Int. J. Cardiol. 167(6), 2820–2823. https://doi.org/10.1016/j.ijcard.2012.07.006 (2013).
Borges, G. M. A transição da saúde no Brasil: Variaçõesregionais e divergência/convergêncianamortalidade. Cadernos de SaudePublica 33(8), 1–15. https://doi.org/10.1590/0102-311X00080316 (2017).
Lopez, A. D. & Adair, T. Is the long-term decline in cardiovascular-disease mortality in high-income countries over? Evidence from national vital statistics net. Int. J. Epidemiol. 48(6), 1815–1823. https://doi.org/10.1093/ije/dyz143 (2019).
RIPSA – RedeInteragencial de Informações para a saúde. Indicadores e Dados Básicos - Brasil – 2012, IDB-2012.1–9 (2020).
Čelutkienė, J. et al. Challenges of treating acute heart failure in patients with chronic obstructive pulmonary disease. Card Fail. Rev. 3(1), 56–61. https://doi.org/10.15420/cfr.2016:23:2 (2017).
InstitutoBrasileiro de Geografia e Estatística (IBGE). Cidades e estados. 2020. https://www.ibge.gov.br/cidades-e-estados (2019).
GBD 2016 Brazil Collaborators. Burden of disease in Brazil, 1990–2016: a systematic subnational analysis for the Global Burden of Disease Study 2016. Lancet 392(10149), 760–775. https://doi.org/10.1016/S0140-6736(18)31221-2 (2018).
NaçõesUnidasBrasil. Momento de ação global para as pessoas e o planeta. https://nacoesunidas.org/pos2015/ (2015).
GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 393(10184), 1958–1972. https://doi.org/10.1016/S0140-6736(19)30041-8 (2019).
Mink, P. J. et al. Flavonoid intake and cardiovascular disease mortality: a prospective study in. Am. J. Clin. Nutr. 85(3), 895–909. https://doi.org/10.1093/ajcn/85.3.895 (2014).
Brasil. Decreto no 5.090, de 20 de maio de 2004. Diário Oficial da União.Preprint at https://www2.camara.leg.br/legin/fed/decret/2004/decreto-5090-20-maio-2004-532380-publicacaooriginal-14402-pe.html (2004).
Brasil. Ministério da Saúde. Campanhasaúdenão tem preço. Portaria nº 184, de 03 de fevereiro de 2011. Preprint at https://portalarquivos.saude.gov.br/images/pdf/2014/junho/18/portaria184.pdf (2011).
Brasil. AgênciaNacional de VigilânciaSanitária (Anvisa). A Anvisa e o Controle dos ProdutosDerivados do Tabaco. https://portal.anvisa.gov.br/documents/106510/106594/A+Anvisa+e+o+Controle+dos+Produtos+Derivados+do+Tabaco/4af73983-9d76-4af4-93c0-e35f153a18a7 (2014).
Brasil. Ministério da saúde. Portaria nº 2.681, de 7 de novembro de 2013. Preprint at https://bvsms.saude.gov.br/bvs/saudelegis/gm/2013/prt2681_07_11_2013.html (2013).
Baena, C. P. et al. Tendency of mortality in acute myocardial infarction in Curitiba (PR) in the period of 1998 to 2009. Arq Bras Cardiol 98, 3. https://doi.org/10.1590/S0066-782X2012000300003 (2012).
Funding
This work was financed by the ‘Coordination for the Improvement of Higher Education Personnel’ - Brazil (CAPES, Coordination for the Improvement of Higher Education Personnel) - financing code 001.
Author information
Authors and Affiliations
Contributions
DLBS contributed to the conception and design of the work; CASS contributed to the acquisition, analysis, writing of original draft and review. Both authors contributed to data interpretation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Siqueira, C.A.d., de Souza, D.L.B. Reduction of mortality and predictions for acute myocardial infarction, stroke, and heart failure in Brazil until 2030. Sci Rep 10, 17856 (2020). https://doi.org/10.1038/s41598-020-73070-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-73070-8
- Springer Nature Limited