
Abstract
We evaluated whether breast arterial calcification (BAC) is associated with the progression of coronary atherosclerosis in asymptomatic women. This retrospective observational cohort study analysed asymptomatic women from the BBC registry. In 126 consecutive women (age, 54.5 ± 7.0 years) who underwent BAC evaluation and repeated coronary computed tomography angiography (CCTA) examinations, the coronary arterial calcification score (CACS) and segment stenosis score (SSS) were evaluated to assess the progression of coronary arterial calcification (CAC) and coronary atherosclerotic plaque (CAP). CAC and CAP progression were observed in 42 (33.3%) and 26 (20.6%) women, respectively (median interscan time, 4.3 years), and were associated with the presence of BAC and a higher BAC score at baseline. Women with BAC demonstrated higher CAC and CAP progression rates and showed higher chances for CAC and CAP progression during follow-up (p < 0.001 for both). In multivariable analyses, the BAC score remained independently associated with both CAC and CAP progression rates after adjustment for clinical risk factors (β = 0.087, p = 0.029; and β = 0.020, p = 0.010, respectively) and with additional adjustment for baseline CACS (β = 0.080, p = 0.040; and β = 0.019, p = 0.012, respectively) or SSS (β = 0.079, p = 0.034; and β = 0.019, p = 0.011, respectively). Thus, BAC may be related to the progression of coronary atherosclerosis and its evaluation may facilitate decision-making.
Similar content being viewed by others

Introduction
Breast arterial calcification (BAC), which is commonly observed on screening mammography, represents medial calcification of the mammary arteries and is considered as a benign and incidental finding from an oncological perspective. However, at the same time, BAC has been reported as a women-specific risk marker for cardiovascular disease1,2. Evidence gathered over the past several decades has demonstrated associations between BAC presence and traditional cardiovascular risk factors, as well as an increased risk for adverse cardiac events in women with BAC2,3,4. Moreover, recent studies have reported that the presence of BAC is associated with coronary artery calcification (CAC) and coronary atherosclerotic plaque (CAP)5,6. Especially, the BBC study (Women Health Registry Study for Bone, Breast, and Coronary Artery Disease) demonstrated that BAC evaluation in asymptomatic women provides an independent and incremental value to clinical risk factors for the prediction of subclinical coronary atherosclerosis6.
If coronary atherosclerosis progression could be predicted in individual patients by evaluating BAC, in addition to clinical risk factors, clinical decision-making regarding further cardiac tests and preventive medication would be facilitated. Furthermore, given that millions of women undergo mammography, the simultaneous evaluation of breast cancer and cardiovascular disease risk has tremendous appeal. However, to date, whether BAC evaluation is associated with coronary atherosclerosis progression has not been studied. Therefore, in this retrospective cohort study, we aimed to evaluate whether the presence and severity of BAC on mammography is associated with coronary atherosclerosis progression in asymptomatic women.
Materials and Methods
Study design and participants
This retrospective study was approved by the institutional review board of Seoul National University Bundang Hospital of Seoul National University, and the requirement of informed consent was waived. All experiments were performed in accordance with the Declaration of Helsinki and relevant guidelines and regulations.
The study participants were recruited from the BBC study, which was a retrospective observational cohort study that assessed the predictive value of BAC and bone mineral density for the presence of subclinical coronary artery disease (CAD). A total of 2,100 consecutive asymptomatic women aged ≥40 years who underwent digital mammography, dual-energy X-ray absorptiometry, and coronary computed tomography angiography (CCTA) as part of a general health evaluation at the Health Promotion Center, Seoul National University Bundang Hospital, between 2011 and 2013 were included in the BBC study. As we previously described, although most Korean health check-up centers are currently trying to curb the use of CCTA in asymptomatic individuals7, Korean individuals have been able to undergo CCTA through a self-referral mechanism. The design, characteristics, and primary findings of the BBC study have previously been described6.
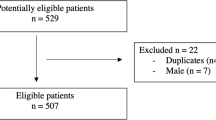
From the retrospective observational cohort of the BBC study, we identified 129 women who underwent repeated CCTA examinations. After excluding 3 women who underwent coronary revascularisation between two CCTA examinations, 126 women were included in the final analysis (Fig. 1). Of these, 43 (34.1%) underwent symptom-driven clinically indicated CCTA examinations, while 83 (65.9%) underwent CCTA as a part of a general health evaluation.

Flow diagram of the study population selection. BBC Registry, Women Health Registry for Bone, Breast, and Coronary Artery Disease; CCTA, coronary computed tomographic angiography.
Digital mammography
As previously described, standard two-view (craniocaudal and mediolateral oblique) screening mammography was performed using a full-field digital mammography system (Brestige; Medi-future) and retrospectively evaluated by a breast radiologist, blinded to the CCTA results and clinical outcomes, using a 5-megapixel monitor and picture-archiving and communication system (Infinitt PACS®; Infinitt Healthcare)6. For women with BAC, the number, length, and density of BACs were evaluated as previously described5,6. The number of calcified vessels in both breasts was coded as 0 to 6 (if more than 6 calcified vessels were detected, 6 was recorded). The calcification involvement within the entire length of the calcified vessel with the longest calcification among all mammary arteries, was scored as 0 to 3 (0, none; 1, <1/3; 2, between 1/3 and 2/3; 3, >2/3). Similarly, the density of a calcified vessel in its densest segment was scored as 0 to 3 (0, none; 1, vessel wall calcification with clear visualisation of the lumen; 2, vessel wall calcification with clouding of the lumen; 3, vessel wall calcification without visualisation of the lumen). The BAC score (BACS) was calculated by summing these 3 numbers5,6.
CCTA acquisition and analysis
As previously described, CCTA was performed using a 64-detector row computed tomography (CT) scanner (Brilliance 64; Philips Medical Systems, Best) and the images were transferred to an offline 3-dimensional workstation. CCTA images were independently analysed for CAC and CAP6. The CAC score (CACS) was measured using the Agatston scoring system8. CAP was defined as the presence of any clearly discernible atherosclerotic plaque lesion >1 mm2 that could be discriminated from the coronary artery in ≥2 independent image planes9. The segment stenosis score (SSS) was used as a measure of the overall CAP burden10. According to the modified American Heart Association 15-segment criteria11, each segment was graded from 0 to 2: 0, no CAP; 1, CAP with maximal diameter stenosis <50%; and 2, CAP with maximal diameter stenosis ≥50%. The scores of all 15 segments were summed to yield a SSS ranging from 0–30. CAC and CAP progression were defined as increase in the CACS and SSS, respectively, on follow-up CCTA compared to that on baseline CCTA. The CAC progression rate was calculated as the annualised difference between the square root of the baseline CACS and the square root of the follow-up CACS to minimise the effect of interscan variability12,13. The CAP progression rate was calculated as the annualised difference between the baseline and follow-up SSS.
Clinical follow-up
Medical records were reviewed to assess the occurrence of cardiac death, nonfatal myocardial infarction, unstable angina, and revascularisation.
Statistical analysis
All statistical analyses were performed using R statistical software (version 3.5.0, http://www.R-project.org/). Continuous variables are expressed as means and standard deviations, and categorical variables are expressed as proportions. Quantitative data were compared using the Student’s t, Kruskal-Wallis, χ2, and Fisher’s exact tests, as appropriate. The Kaplan-Meier method was used to visualise CAC and CAP progression, and the differences among groups with or without CAC or CAP progression were evaluated by the log-rank test. The date of the CCTA scan in which CAC or CAP progression was observed was assigned as the date of the event occurrence. Univariable and multivariable linear regression analyses were conducted to determine the effects of various characteristics on the annualised CAC and CAP progression. The results are expressed as the beta coefficient (β) and corresponding 95% confidence interval (CI). For the multivariable linear regression analysis, collinearity among all potential confounders was tested using variance inflation factors; values less than 2.0 were considered to indicate no collinearity. The independent association between the BACS and CAC or CAP progression rate was examined in several models: model 1, clinical risk factors + BACS; model 2, clinical risk factors + CACS + BACS; and model 3, clinical risk factors + SSS + BACS. We did not include CACS and SSS in the same model because of multicollinearity. The t value was used to estimate the contribution of each variable to the progression rates of CAC and CAP. A two-sided p-value < 0.05 was considered to represent a statistically significant difference.
Statistics and biometry
One of the authors has significant statistical expertise.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Study subjects or cohorts overlap
The study participants were recruited from the BBC study, which was a retrospective observational cohort study that assessed the predictive value of breast arterial calcification and bone mineral density for the presence of subclinical coronary artery disease.
Results
Baseline characteristics
Compared to those without follow-up CCTA (n = 1,971; mean age 52.3 ± 7.2 years), the women in the present study cohort (n = 126; mean age, 54.5 ± 7.0 years) were older and more likely to have hypertension and higher body mass index (Supplementary Table 1). They also were more likely to have CAC and CAP at baseline. However, BAC presence and score did not significantly differ between women with and without repeated CCTA examinations. Table 1 provides the baseline characteristics of the women in the present study cohort. At baseline, CAC and CAP were present in 27 (21.4%) and 39 (31.0%) women, respectively.
CAC and CAP progression
With a median interscan duration of 4.3 years (interquartile range, 3.2–5.0 years), CAC and CAP progression were observed in 42 (33.3%) and 26 (20.6%) women, respectively. Women who experienced CAC progression were significantly older and showed higher blood pressure, haemoglobin A1c (HbA1c), total cholesterol, triglyceride, and low-density lipoprotein (LDL) cholesterol than did women without CAC progression. They were also more likely to have CAC, CAP, and BAC at baseline (Table 1). Although women with CAP progression were older and had higher HbA1c than were those without CAP progression, the lipid profiles were not significantly different. They were also more likely to have CAC, CAP, and BAC at baseline.
CAC and CAP changes based on BAC presence
Women with BAC were more likely to have CAC at both baseline (55.6% vs. 15.7%; p < 0.001) and follow-up (77.8% vs. 29.6%; p < 0.001) than were women without BAC. Similarly, CAP was more frequently observed in women with BAC at both baseline (72.2% vs. 24.1%; p < 0.001) and follow-up (83.3% vs. 33.3%; p < 0.001). The CACS, SSS, and CAC and CAP progression rates stratified by BAC presence are shown in Fig. 2. CACS and SSS were significantly higher in women with BAC than in women without BAC at both baseline and follow-up. The progression rates of CAC and CAP were also higher in women with BAC than in women without BAC. The cumulative proportions of CAC and CAP progression stratified by BAC presence are shown in Fig. 3. Women with BAC at baseline had a significantly higher chance of CAC and CAP progression compared to that in women without BAC. Representative cases are shown in Fig. 4.

Progression of CAC (A) and CAP (B) according to the presence and absence of BAC. BAC, breast arterial calcification; CAC, coronary arterial calcification; CAP, coronary atherosclerotic plaque.

The cumulative proportion of CAC (A) and CAP (B) progression according to the presence and absence of BAC. BAC, breast arterial calcification; CAC, coronary arterial calcification; CAP, coronary atherosclerotic plaque.

Representative cases. A 63-year-old asymptomatic woman with a BAC score of 5 (yellow arrow heads) on screening mammography (A) demonstrated calcified plaque without significant stenosis (percent diameter stenosis, 10–20%) at the proximal LAD and mixed plaque (percent diameter stenosis, 10–20%) at the mid LAD (yellow arrow). (B) Three years later, she was referred to the emergency department with chest pain and underwent CCTA, which demonstrated progression of the mid LAD lesion (percent diameter stenosis, 90%; yellow arrow). (C) Invasive angiography also demonstrated the tight stenosis of the mid LAD (percent diameter stenosis, 90%) and percutaneous coronary intervention was performed. A 51-year-old asymptomatic woman without evidence of BAC (red arrow heads) on screening mammography (D) demonstrated calcified plaque (percent diameter stenosis, 30%) at the mid LAD (red arrow). (E) Five years later, she visited the outpatient clinic due to epigastric pain and underwent CCTA, which demonstrated no change in the mid LAD lesion (red arrow). (F) BAC, breast arterial calcification; CCTA, coronary computed tomographic angiography; LAD, left anterior descending artery.
Factors associated with CAC and CAP progression rates
Table 2 shows the results of the univariable linear regression analyses for CAC and CAP progression rates. The results of the multivariable linear regression analysis for the CAC progression rate are shown in Table 3. Among the clinical risk factors, age, number of parity, hypertension, current smoking, systolic blood pressure, serum creatinine, HbA1c, triglyceride, high-density lipoprotein cholesterol, LDL cholesterol, statin use at day 60 after the index CCTA were included in the multivariable analysis, after excluding variables showing multicollinearity. In models 1 and 2, HbA1c and BACS were independently associated with the CAC progression rate. In model 3, HbA1c, SSS, and BACS maintained independent associations with the CAC progression rate. The results of a similar multivariable linear regression analysis for the CAP progression rate are shown in Table 4. In models 1, 2, and 3, only the BACS maintained an independent association with the CAP progression rate.
Clinical outcomes based on BAC presence
A total of 2 adverse cardiac events (1 nonfatal myocardial infarction and 1 unstable angina) were observed in patients with BAC, whereas no adverse cardiac events occurred among patients without BAC (thus, Cox regression analysis was unavailable). Both women who experienced adverse cardiac events also demonstrated CAC and CAP progression. The annualised rate of adverse cardiac events was 2.5% and 0% in women with and without BAC, respectively (log-rank p < 0.001).
Discussion
We previously reported that BAC evaluation in asymptomatic women provides an independent and incremental value over conventional clinical risk factors for the prediction of subclinical coronary atherosclerosis6. Here, although the study population was limited to those with repeated CCTA examinations, we have additionally demonstrated that BAC presence and score are significantly associated with the progression of subclinical coronary atherosclerosis, as evidenced by increased CACS and SSS. In addition, the BACS is independently associated with the annualised progression of CAC and CAP.
BAC, incidentally observed at screening mammography, has been considered to be an insignificant finding without an increased risk of breast cancer. However, evidence that BAC presence is associated with an increased risk of cardiovascular disease morbidity and mortality is currently accumulating2,3,4. Nevertheless, limited data is currently available regarding the relationship between BAC and CAD, and the results are inconsistent2. With the exception of only one prospective study14, these previous studies retrospectively analysed symptomatic women who underwent invasive coronary angiography; thus, the study populations were necessarily limited to a small number of patients with suspected CAD2. Recently, Margolies et al. studied 292 women with digital mammography who also underwent non-gated chest CT5. Although CAC was assessed in a semiquantitative manner, the investigators showed a strong association between BAC and CAC. However, they failed to demonstrate an incremental predictive value of BAC over the conventional risk stratification algorithm, potentially due to the small number of study participants. In contrast, the BBC study, which included a large number of asymptomatic women, reported an association between BAC and subclinical CAD, including both CAC and CAP, as assessed on CCTA6. Additionally, BAC was shown to provide an independent and incremental predictive value over the conventional risk stratification algorithm. Therefore, BAC is currently expected to be useful for improving risk stratification, in a manner similar to that for CAC in previous studies2,15. Nevertheless, until recently, whether BAC presence and severity could also predict coronary atherosclerosis progression had never been evaluated. In the present preliminary study, we found an independent association between the BACS and the progression rates of CAC and CAP. Although the current analysis is based on a relatively small number of women with repeated CCTA examinations, which may raise concerns regarding generalizability, these results provide important clues regarding the association between BAC and the progression of coronary atherosclerosis.
Previous studies have demonstrated that CAC or CAP progression detected by serial CCTA is independently associated with adverse cardiovascular events16,17,18,19. Given that atherosclerosis is a dynamic process, CAC and CAP progression might provide insight into ongoing disease activity. However, although many experts have suggested that repeated testing provides a large amount of information regarding the progression of coronary atherosclerosis, no current guidelines advocate for more than one CAC scoring or CCTA for CAP evaluation. Additionally, the increasing cost of cardiovascular health care has become daunting. In contrast, current clinical practice guidelines recommend annual mammographic screening in asymptomatic women20, although the recommended age varies according to demographic characteristics and the available medical resources21. Thus, millions of women undergo mammography each year for the screening of breast cancer22. However, important information regarding the presence and severity of BAC is often omitted from the mammography report since it is considered as an insignificant finding without increased risk for breast cancer. Our study results suggest that BAC should be included in the mammography report and be treated as any other clinically relevant incidental finding. Of course, large randomised controlled trials are required before integrating BAC evaluation in risk stratification and personalised targeted preventive strategies.
Although evidence supporting the association of BAC with an increased risk for cardiovascular disease is accumulating, there remains uncertainty regarding the exact causal and pathophysiologic mechanism. While intimal calcification is commonly associated with atherosclerotic plaque, BAC is mostly (but not entirely) medial calcification15. Until the late twentieth century, medial calcification was considered rather benign because of the absence of stenotic lesions; however, it is currently recognised as a key negative predictor of cardiovascular morbidity and mortality23. It is not well understood why BAC predicts the presence and progression of subclinical coronary atherosclerosis. BAC may represent long-term exposure to shared cardiovascular risk factors, or it may be indicative of medial calcification co-existing in other vascular beds. Medial calcifications may lead to cardiovascular disease through increased arterial stiffness24,25. The decreased distensibility may contribute to higher peak pressure in distal vessels, leading to damage and remodelling, and an aggravation of ischaemia by co-existing atherosclerosis. Additionally, increased stiffness in large arteries may exacerbate atherosclerosis via altered blood flow characteristics15. As the BACS remained independently associated with CAC and CAP progression rates in the present study, further investigations are critical to deciphering the interactions between BAC and coronary atherosclerosis.
The major limitations of the present study are its observational retrospective design and the relatively small number of study participants, which subjected the study to many selection biases. Specifically, only 126 women of the 2,100 women in the BBC registry underwent repeated CCTA examinations. Although we were able to populate the BBC registry, because CCTA has been used as a screening tool through a self-referral mechanism in Korea, CCTA is not currently indicated in asymptomatic individuals7. Thus, it is not surprising that only a small number of women from the BBC registry underwent repeated CCTA examinations. Caution must be taken in applying the current preliminary results to the general population. Nevertheless, the current study provides valuable clues regarding the association between BAC and the progression of CAC and CAP that set the stage for an outcome trial, which is required to evaluate whether BAC evaluation on screening mammography translates into long-term clinical benefits. Additionally, in this retrospective study, CCTA follow-up was not guided by a specific study protocol. Therefore, the interscan duration varied among study participants; in an observational study, such effects are inevitable. To minimise the effect of variations in the interscan duration, we evaluated the association between BAC and annualised CAC and CAP progression (CAC and CAP progression rates). Finally, the CAP burden was estimated using the SSS instead of a volumetric measure of plaque because not all CCTA imaging data were stored at a sufficient level for plaque volumetry. Therefore, prospective studies are needed to determine whether BAC is predictive of increased CAP volume, and if so, whether it is also associated with changes in plaque composition.
Conclusions
BAC, which is currently suggested as a potential woman-specific risk marker for CAD, is also related to the progression of coronary atherosclerosis as evidenced by CCTA. Especially, the BACS is independently associated with the annualised progression of CAC and CAP. Although these findings support the value of BAC in identifying asymptomatic women at an increased risk for future cardiovascular disease without additional cost and radiation exposure, caution must be exercised in applying the current preliminary results to the general population considering the relatively small number of study participants. Further studies are warranted to determine whether the evaluation of BAC in asymptomatic women predicts the progression of coronary atherosclerosis and translates into long-term clinical benefits.
References
Polonsky, T. S. & Greenland, P. Breast Arterial Calcification: Expanding the Reach of Cardiovascular Prevention. Circulation 135, 499–501 (2017).
Suh, J. W. & Yun, B. L. Breast Arterial Calcification: A Potential Surrogate Marker for Cardiovascular Disease. J. Cardiovasc. Imaging 26, 125–134 (2018).
Kemmeren, J. M. et al. Breast arterial calcifications: association with diabetes mellitus and cardiovascular mortality. Work. progress. Radiology 201, 75–78 (1996).
Hendriks, E. J. et al. Breast arterial calcifications: a systematic review and meta-analysis of their determinants and their association with cardiovascular events. Atherosclerosis 239, 11–20 (2015).
Margolies, L. et al. Digital Mammography and Screening for Coronary Artery Disease. JACC Cardiovasc. Imaging 9, 350–360 (2016).
Yoon, Y. E. et al. Prediction of Subclinical Coronary Artery Disease With Breast Arterial Calcification and Low Bone Mass in Asymptomatic Women: Registry for the Women Health Cohort for the BBC Study. JACC Cardiovasc. Imaging 12, 1202–1211 (2019).
Kim, Y. J. et al. Korean guidelines for the appropriate use of cardiac CT. Korean J. Radiol. 16, 251–285 (2015).
Agatston, A. S. et al. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 15, 827–832 (1990).
Faletra, F. F. et al. Relation between coronary atherosclerotic plaques and traditional risk factors in people with no history of cardiovascular disease undergoing multi-detector computed coronary angiography. Heart 95, 1265–1272 (2009).
Min, J. K. et al. Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J. Am. Coll. Cardiol. 50, 1161–1170 (2007).
Achenbach, S. et al. Detection of calcified and noncalcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multidetector spiral computed tomography: a segment-based comparison with intravascular ultrasound. Circulation 109, 14–17 (2004).
McEvoy, J. W. et al. Coronary artery calcium progression: an important clinical measurement? A review of published reports. J. Am. Coll. Cardiol. 56, 1613–1622 (2010).
Hokanson, J. E. et al. Evaluating changes in coronary artery calcium: an analytic method that accounts for interscan variability. AJR Am. J. Roentgenol. 182, 1327–1332 (2004).
Zgheib, M. H. et al. Breast arterial calcifications on mammograms do not predict coronary heart disease at coronary angiography. Radiology 254, 367–373 (2010).
Iribarren, C. & Molloi, S. Breast Arterial Calcification: a New Marker of Cardiovascular Risk? Curr. Cardiovasc. Risk Rep. 7, 126–135 (2013).
Budoff, M. J. et al. Progression of coronary artery calcium predicts all-cause mortality. JACC Cardiovasc. Imaging 3, 1229–1236 (2010).
Budoff, M. J. et al. Progression of coronary calcium and incident coronary heart disease events: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 61, 1231–1239 (2013).
Motoyama, S. et al. Plaque Characterization by Coronary Computed Tomography Angiography and the Likelihood of Acute Coronary Events in Mid-Term Follow-Up. J. Am. Coll. Cardiol. 66, 337–346 (2015).
Gu, H. et al. Sex differences in coronary atherosclerosis progression and major adverse cardiac events in patients with suspected coronary artery disease. J. Cardiovasc. Comput. Tomogr. 11, 367–372 (2017).
In WHO Position Paper on Mammography Screening WHO Guidelines Approved by the Guidelines Review Committee (2014).
Lee, E. H. et al. The Korean guideline for breast cancer screening. J. Korean Med. Assoc. 58, 408–419 (2015).
Kerlikowske, K. Evidence-based breast cancer prevention: the importance of individual risk. Ann. Intern. Med. 151, 750–752 (2009).
Lanzer, P. et al. Medial vascular calcification revisited: review and perspectives. Eur. Heart J. 35, 1515–1525 (2014).
Abou-Hassan, N., Tantisattamo, E., D’Orsi, E. T. & O’Neill, W. C. The clinical significance of medial arterial calcification in end-stage renal disease in women. Kidney Int. 87, 195–199 (2015).
Hendriks, E. J. E. et al. Breast arterial calcifications and their association with incident cardiovascular disease and diabetes: the Prospect-EPIC cohort. J. Am. Coll. Cardiol. 65, 859–860 (2015).
Acknowledgements
This work was supported by a grant from the Basic Science Research Program through the National Research Foundation of Korea (NRF), sponsored by the Ministry of Science, ICT & Future Planning (NRF-2019R1F1A1059425).
Author information
Authors and Affiliations
Contributions
Y.E.Y. drafted the main manuscript text and K.M.K. prepared the figures. Y.E.Y., S.A., B. L.Y. and J.S. contributed the design of the work. Y.E.Y., K.M.K., S.Y. and W.L. contributed to the analysis and interpretation of data. B.L.Y., J.S., J.S.H., E.J.C. and S.I.C. substantially revised the manuscript. All authors reviewed and approved the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yoon, Y.E., Kim, K.M., Lee, W. et al. Breast Arterial Calcification is Associated with the Progression of Coronary Atherosclerosis in Asymptomatic Women: A Preliminary Retrospective Cohort Study. Sci Rep 10, 2755 (2020). https://doi.org/10.1038/s41598-020-59606-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-59606-y
- Springer Nature Limited