
Abstract
The interaction of genetic susceptibility and dietary habits in cardiovascular disease (CVD) remains undetermined. The purpose of this study was to investigate whether a Mediterranean dietary style modified the genetic risk of developing CVD in a Chinese cohort. A total of 2098 subjects with dietary information from a Chinese community cohort (CVDFACTS) were enrolled. Candidate genes, including SNP markers rs1333049 (CDKN2B, 9p21.3), rs17465637 (MIA3, 1q41) and rs501120 (CXCL12, 10q11.21), were genotyped to analyze the association with future CVD. The impact of dietary pattern was also analyzed according to adherence to the diet using the Mediterranean Diet Score (MDS). After an average follow-up of 7.8 years, only the C risk allele of rs1333049 at chromosome 9p21.3 was associated with a higher risk of MI with either an additive [HR = 1.78, 95% CI:1.23–2.5] or a recessive model [HR = 2.40, 95% CI: 1.42–4.04], and the CC genotype had a higher risk of developing MI (p = 0.009, log-rank test). There was no significant difference in the association of the lipid profile with future CV outcomes among the MDS tertiles. However, the high MI risk of the CC genotype in individuals consuming a less healthy diet (MDS1) (HR: 6.39, 95% CI: 1.74–23.43) significantly decreased to 2.38 (95% CI: 0.57–10.04) in individuals consuming a healthier diet (MDS3), indicating that a healthier dietary pattern (higher MDS) modified the risk of developing MI in carriers of variants in CDKN2B. In conclusion, genetic variants of CDKN2B at 9p21 were significantly associated with future MI risk in a Chinese cohort, and the genetic risk of MI could be modified by a healthier diet.
Similar content being viewed by others


Introduction
Cardiovascular disease (CVD) is associated with an increased risk of mortality and morbidity1. Although great effort has been made to prevent disease progression, the occurrence of adverse events, including myocardial infarction, ischemic stroke and cardiovascular death, remains a concern. Atherosclerosis is the central component in the pathogenesis of CVD and is considered a sustained inflammatory process comprising interactions among vascular inflammation, lipid accumulation, oxidative stress, and genetic susceptibility2. In addition to medical treatment, lifestyle modifications, especially healthy diets, are encouraged for CVD prevention. Among various CVD risk factors, genetic susceptibility is believed to play some role in determining future CV outcomes. However, there is limited information about the association between genetic risk and dietary habits to CVD.
The importance of dietary patterns to reduce CVD risk has been emphasized in several primary prevention studies for CVD3,4. Dietary recommendations of reducing fat intake, replacing saturated fats (cream, butter, cheese) and trans fats with unsaturated fats and increasing the intake of vegetables, fruits, and fish are suggested to prevent adverse CV events5. Adherence to different healthy diet patterns, such as the Mediterranean diet (MD)5 or the Dietary Approaches to Stop Hypertension (DASH) diet3, are reported to be associated with a lower risk of developing cardio-metabolic disorders, suggesting the benefit of a healthy dietary pattern for cardiovascular system protection. To our interest, dietary components differ across different geographic areas, cultures, and environmental exposures and may exert variable impacts in populations with different genetic backgrounds. A previous genome-wide association study has reported several significant associations with CVD, including CDKN2B (chromosome 9p21.3), MIA3 (1q41) and CXCL12 (10q11.21)6,7, but the association in the Asian population was not verified using a long-term follow-up cohort. In addition, the impact of a healthy diet on the future risk of cardiovascular disease in the Asian population was unknown. Therefore, it is important to investigate the interactions between the genetic risk for CVD and diet and whether healthy dietary patterns could modify the genetic risk for CVD in the Chinese population. Our current study aimed to investigate the genetic risk of developing CVD and the impact of healthy Mediterranean dietary patterns in a community Chinese cohort.
Methods
Study population
The study cohort was selected from the CardioVascular Disease risk FACtors Two-township Study (CVDFACTS), and the study protocol has been reported previously8,9. Briefly, the CVDFACTS was a community-based follow-up study investigating CVD occurrence and risk factors in Taiwan since 1989. Five villages with more than 1000 people and a population density greater than 200 persons per square kilometer were randomly selected from Chu-Dong (northwest Taiwan) and Pu-Tzu (southwest Taiwan). Data regarding lifestyle, CVD risk factors, a history of CVD, and urine and blood chemistry data were collected. Repeated examinations were carried out in 1989–1990, 1990–1993, 1994–1997, 1997–1999, and 2000–2002. A total of 5146 residents aged 30 years and older participated in the cycle-3 examination (1994–1996), in which biochemical data were collected; 2098 individuals with complete dietary information were enrolled. The study complied with the Declaration of Helsinki and was approved by the appropriate Ethics Committees of Academia Sinica, and all patients all provided written informed consent at baseline and follow-up visits.
Blood sampling and genetic markers associated with CVD
Blood samples were collected after an overnight fast. The plasma and buffy coat were separated by centrifugation, and all samples were stored at −70 °C. Biochemical profiles, including glucose, cholesterol, triglycerides, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C), were measured using a Monarch 2000 automatic analyzer. Genetic susceptibility may interact with environmental factors such as diet, sedentary habits, and smoking exposure to contribute to the complexity of CVD1. We studied 3 loci (1q41, 9p21.3, 10q11.21) that have been linked to CAD risk by previous GWAS6,7. We genotyped the 3 lead SNPs within the following loci: chromosome 9p21.3 (rs1333049, CDKN2B), 1q41 (rs17465637, MIA3) and 10q11.21 (rs501120, CXCL12)6,7. Genotyping was carried out using matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometry (Sequenom, MassARRAY, San Diego, CA, USA) using standard protocols and was performed at the Academia Sinica National Genotyping Center, Taiwan. Automated genotype calling was performed, and the data were analyzed using Sequenom Typer software.
Mediterranean dietary pattern
Dietary intake information was assessed using a food-frequency questionnaire that included foods and beverages commonly consumed in Taiwan. The Mediterranean Diet Score (MDS) was calculated based on components as reported previously5,10. For each of the dietary items, participants were asked to report the frequency of consumption and portion size. In brief, a total of 14 inclusive food groups, including vegetables, fruits, nuts, legumes, cereals, meats, dairy products, fish, eggs, monounsaturated lipids (e.g., olive oil), polyunsaturated lipids, saturated lipids, sugar, and sweetened and non-alcoholic beverages, were included. Each question was scored 0 or 1, and a higher MDS indicated greater adherence to the Mediterranean dietary pattern5,10.
Clinical follow-up for adverse CV events
Cardiovascular events, including ischemic stroke, fatal or nonfatal MI, and CV death, were identified from a review of self-reported disease histories, death certificates, and insurance claim records in the National Health Insurance (NHI) database dated until the end of 2002. The NHI included 99.5% of Taiwan’s population. The CV events were identified from NHI database records using codes 430 to 438 for ischemic stroke and 410 to 414 for CAD from the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Cardiovascular death was identified from death certificates. We used the National Death Registry database, which obtains information from certified death certificates and codes death according to the ICD-9. The sensitivity and specificity for event identification were 100% and 95%, respectively9,11,12.
Statistical analysis
All baseline data were expressed as either the mean ± standard deviation (SD) or number (percentage). SPSS statistical software version 10.0 (Chicago, IL) was used for statistical analysis. The significance of between-group differences in means was assessed using Student’s t-test, and the significance of differences between 2 proportions was tested with the chi-squared test. SNPs were excluded when the SNP call rate was<95% or not in Hardy–Weinberg equilibrium. Associations between SNPs and future adverse outcomes were evaluated in three models (additive, dominant, and recessive) after adjusting for covariates. Data on outcomes were censored either at the time of an ischemic stroke event or death or at the end of follow-up. Test for trend was also carried out by assigning the ordinal value 0, 1, and 2 according to the numbers of risk alleles and then examining the association of the resulting variable with the outcome. Kaplan–Meier curves with log-rank tests for event-free survival were constructed for genetic variants and dietary patterns as described previously13,14. To determine the hazard ratio (HR) of the genetic variant, a Cox model was performed. The results were presented as the HR with its corresponding 95% confidence interval (CI). A p value < 0.05 was considered statistically significant.
Ethics approval and consent to participate
The study complied with the Declaration of Helsinki, which was approved by the appropriate Health Authorities, independent Ethics Committees, and Independent Review Boards of Academia Sinica. All patients should give their written inform consent before enrollment.
Results
A total of 2,098 subjects, 917 males and 1181 females with a mean age of 49.9 ± 12.2 years, with complete dietary information were included in this study. Their baseline characteristics are shown in Table 1. The proportion with hypertension and that of smokers was 12.4% and 19.3%, respectively, and the proportion with diabetes was 3.1%. The BMI was 24.2 ± 3.3 kg/m2. Because study subjects were enrolled from the community and not from hospitals, the lipid profiles were relatively normal (LDL-C: 130.5 ± 44.5 mg/dL; HDL: 42.7 ± 15.5 mg/dL; triglycerides: 107.7 ± 76.5 mg/dL, respectively). The genotype call rate was above 99.4%, and the mean MDS was 5.1 ± 1.2 with normal distribution (Supplement Fig. 2). Frequencies of the candidate SNP markers, including rs1333049 (CDKN2B, 9p21.3), rs17465637 (MIA3, 1q41), and rs501120 (CXCL12, 10q11.21), are shown in Table 1.
After an average of 7.8 years of follow-up, a total of 134 major CV events were identified, including 54 ischemic strokes, 64 acute MIs, and 26 cardiovascular-related deaths (Table 1). Subjects with future CV events were older, more likely to be male, and had a higher prevalence of hypertension, diabetes, and cigarette smoking. There were no significant differences in lipid profiles at baseline between subjects with and without a CV event, but subjects with a CV event had a higher BMI and a higher level of high-sensitivity C-reactive protein (hsCRP), suggesting that an increased inflammatory state was present in those who later developed a CV event. Of the selected genetic SNP markers, only the C risk allele of rs1333049 at chromosome 9p21.3 was associated with an increased risk of future MI occurrence using either an additive (HR = 1.78, 95% CI: 1.23–2.58, p = 0.002) or a recessive (HR = 2.40, 95% CI: 1.42–4.04, p = 0.001) model after adjusting for age, sex, hypertension, diabetes, tobacco smoking, and lipid profile (Table 2). Kaplan–Meier survival analysis also showed that the CC genotype of the rs1333049 variant had a higher future MI risk (p = 0.009 by log-rank test) (Fig. 1). The Supplement Table 1 showed that CC genotype of rs1333049 variant had higher incidence of MI development during follow-up period (Supplement Table 1). There were no significant genetic associations observed among rs17465637 (MIA3) or rs501120 (CXCL12) and future adverse CV events, including MI, ischemic stroke, CV death and major adverse cardiovascular events (MACEs). The subgroup analysis (Supplement Fig. 1) further showed that the CC genotype of the rs1333049 polymorphism for MI risk was especially observed in females and those <65 years old, with a higher BMI, unfavorable lipid profile, and higher baseline CRP values.

Kaplan-Meier estimates of survival-free of future myocardial infarction according to rs1333049. The CC genotype has significant lower future event-free survival rates for MI (log-rank test, p = 0.022).
Impact of the Mediterranean dietary pattern on future events
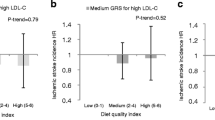
The impact of diet was analyzed based on the MDS5,10 and was categorized as tertiles for the analysis. The distribution of MDS in study population was presented in Supplement Fig. 2. The subject baseline characteristics by MDS tertiles (MDS1, MDS2, MDS3) are shown in Table 3. There were no significant differences in the lipid profiles, body weight, and CVD risk factors among the tertiles of the MDS. Subjects with healthier dietary patterns (MDS2, MDS3) tended to be older and have a higher baseline blood pressure than those with a less healthy dietary pattern (MDS1) (p < 0.05). As also demonstrated in Table 3, the genotype frequency and incidence of CV events were similar among these MDS tertiles. The Kaplan–Meier survival analysis did not show any differences in CV event-survival curves derived for the three MDS tertiles in future events, including MI, ischemic stroke, CV death and MACEs (Fig. 2).

Kaplan-Meier estimates of survival-free cardiovascular events including stroke (A), cardiovascular death (B), myocardial infarction (C) and total cardiovascular events (D) according to MDS tertiles in a cohort study. There is no significant association found between MDS and future cardiovascular events.
To investigate the interaction between the Mediterranean diet and the genetic risk of CVD, the hazard ratio (HR) of rs1333049 genotypes for MI risk according to MDS tertiles was examined. Although the MDS did not independently affect CV outcome in our study, the high MI risk of the CC genotype in the less healthy diet pattern (MDS1) (HR: 6.39, 95% CI: 1.74–23.43) significantly decreased to 2.38 (95% CI: 0.57–10.04) in the healthier dietary pattern (MDS3) (Fig. 3), while this phenomenon was not seen for those with the GG genotype, indicating that the genetic risk for MI could be modified by a healthier diet and that the effect of risk genes may not be evident if a healthy dietary pattern is maintained.

The association between dietary MDS and genetic risk (rs1333049) of developing future MI. The MI risk in CC genotype in the 1st MDS tertile decreased in the 3rd MDS tertile (healthier dietary pattern)(HR: 2.38, 95%CI:0.57–10.04) compared with the GG genotype in MDS3 (referent).
Discussion
The current study showed that the rs1333049 polymorphism at 9p21 was a genetic determinant for future MI in a Chinese population and that individuals with the CC genotype have a higher risk of developing an MI. Regarding dietary impact on CVD, although there was no significant association between the MDS and future CV risk, the risk of the C allele of rs1333049 at 9p21 for MI can be blunted by a Taiwanese Mediterranean-like diet (higher MDS), indicating that the genetic risk of developing MI may be modified by a healthier diet and supporting the notion that a favorable diet should be recommended for CV event prevention in Asian populations.
Most association studies of the genetic variants and CHD was the association between genetic markers and the prevalence of disease, and the association was inconsistent. The reason why there no association of 1q419 (rs17465637, MIA3) and 10q11.21 (rs501120, CXCL12) with future events was observed may come from the difference in various ethnicities or various CHD definitions (myocardial infarction, coronary angioplasty or bypass graft). This polymorphism (rs501120, CXCL12) has been studied in several populations. In Caucasians, this locus was found to be associated with coronary artery disease8,15 in large-scale association studies. However, Haver et al. failed to replicate the association of this locus with CVD events16. Inconsistency is also noted for the region of 1q419 (rs17465637, MIA3); this locus was associated with CAD identified by the GWAS study but was not in subsequent studies. Wang et al. reported the association of this SNP with CAD in American Caucasians17, whereas the association remained inconsistent in follow-up studies on Chinese people18,19. However, a subsequent meta-analysis on five Asian populations confirmed the association with CAD in this ethnic group20. The association of the genetic risk of variants of CDKN2B at 9p21 and CAD has been reported previously6. Although the C allele in rs1333049 has been identified as a risk allele having the strongest association with CAD in both the WTCCC and the German GWAS6, the associations between this loci and CAD were not consistent14. Buysschaert et al. reported that the at-risk C allele at rs1333049 was significantly and independently associated with recurrent MI and cardiac death13. Additionally, the C allele at rs1333049 was reported to be associated with a lower risk of re-infarction in patients after coronary intervention21. In this study, we demonstrated that the C allele at rs1333049 was associated with a risk of MI in an Asian general population using a prospective observation design. Lee et al. reported that rs4977574 at 9p21 is associated with CAD in Han Chinese but did not predict CV mortality22. A prospective study of a multiethnic cohort, which is similar to ours investigating the same SNP markers, 9p21.3 (rs1333049; CDKN2B), 1q419 (rs17465637, MIA3) and 10q11.21 (rs501120, CXCL12), reported 9 loci, including the 9p21 region, and CXCL12 (rs501120), which were statistically associated with incident CHD events in the white population but not in the Asian/Pacific population, and only the 9p21 region showed significant between-study heterogeneity23. Furthermore, the association between a SNP in the 9p21 region and incident CHD was replicated in Asian/Pacific ethnicity later, but no significant association between 1q419 (rs17465637, MIA3) or 10q11.21 (rs501120, CXCL12) and CHD was observed in the Asian population in this replication study23. The association of the 9p21 region with CHD has also been replicated in Asian populations, including Pakistani23,24, Japanese and Korean23,25,26 and Han Chinese23,27 populations, suggesting that the 9p21 region is the most robust common genetic risk factor in determining the risk of future CHD. Our current finding extended previous observations using a prospective cohort study that yielded causal evidence because exposure precedes the development of the disease28. Our study confirmed the association of 9p21 and CAD and the importance of the C allele of rs1333049 in predicting MI risk in the general population.
The Mediterranean diet, which is high in vegetables, fruit, fish, whole grains, red wine, and olive oil, has demonstrated protective effects toward multiple noncommunicable diseases. Recent studies of consuming a Mediterranean-style diet showed a reduction in CV events even to a greater degree than that of low-fat diets and a benefit equal to or greater than that of statin therapies8,9,11,12. The MDS indicates the degree of adherence to the Mediterranean diet29, and it has been used to evaluate the impact of the diet in determining CV risk and survival30. The Taiwanese diet in the 1990s included MD components such as vegetables, fruits, and fish but not olive oil, whole grains, or red wine. Instead, Taiwanese individuals used soybean oil or lard for cooking, consumed mostly white rice as a staple, and drank rice wine for social events. Our current study did not show a significant benefit of a Taiwanese MD-like diet (higher MDS) in CVD prevention. Nonetheless, subjects with a higher MDS tended to have favorable lipid profiles, although the difference between tertiles was not significant.
In our study, the risk of MI was greatest in individuals with the CC genotype of rs1333049 who consumed an unhealthy diet (lower MDS), but the risk was significantly reduced if individuals with the CC genotype of rs1333049 adhered to a healthier diet (higher MDS), indicating that the MD-like diet modified the genetic association of rs1333049 at 9p21 with the risk of MI, and the effect of the risk gene may not be evident if a healthy dietary pattern is maintained. Similar observations of genetic risk modified by lifestyle or healthy diet have been reported. Corella et al. first reported that a higher adherence to a Mediterranean-style diet attenuated the genetic risk of increased blood sugar in individuals with the TT genotype of rs7903146 in the TCF7L2 gene10. Furthermore, the higher stroke risk of the TT genotype shown in the control group (HR = 3.06, 95% CI: 1.43–6.59) was not observed in Mediterranean-style diet intervention groups after a 4.8-year follow-up10. Similarly, Zheng et al., who investigated the association between sugar-sweetened beverage (SSB) intake and MI risk in a Hispanic population with chromosome 9p21 variants, showed that the per–risk allele odds ratio (OR) of MI in subjects with the rs4977574 polymorphism was 1.44 in subjects with higher SSB consumption (>2 servings/day), 1.21 in subjects with average consumption (1–2 servings/day), and 0.97 in subjects lower consumption (<1 serving/d)31. This finding suggested that higher SSB intake could exacerbate the harmful effects of chromosome 9p21 variants on CAD and was consistent with our finding that genetic risk could be modified by diet.
There are some limitations of this study that should be taken into consideration. The mechanisms by which a healthy diet decreases the risks associated with the rs4977574 polymorphism remain undetermined. Several mechanisms have been proposed, including epigenetic regulation of a healthy diet changing methylation levels to a favorable profile in carriers of the risk allele. In addition, DNA methylation, histone modification and microRNA modulation affected by diet have also been mentioned32. Finally, many healthy eating behaviors co-occur with other healthy lifestyle behaviors, such as regular exercise, and these behaviors may confound the dietary results. Our current study results were in accordance with a recently published study that showed that a favorable lifestyle was associated with a nearly 50% decrease in the risk of CAD in patients at higher genetic risk33.
In conclusion, the association of the rs1333049 polymorphism at 9p21 with the risk of MI was confirmed in a Chinese cohort population, and a healthy Taiwanese MD-like diet attenuated its genetic risk for future MI.
References
Leu, H. B. et al. Identification of new biosignatures for clinical outcomes in stable coronary artery disease - The study protocol and initial observations of a prospective follow-up study in Taiwan. BMC Cardiovasc. Disord. 17, 42 (2017).
Leu, H. B. et al. Genetic variants of connexin37 are associated with carotid intima-medial thickness and future onset of ischemic stroke. Atherosclerosis 214, 101–106 (2011).
Mokhtari, Z. M. et al. Adherence to the Dietary Approaches to Stop Hypertension (DASH) diet and risk of total and cause-specific mortality: results from the Golestan Cohort Study, Int. J. Epidemiol. pii: dyz079, https://doi.org/10.1093/ije/dyz079. [Epub ahead of print] PubMed PMID: 31056682 (2019).
de Oliveira Otto, M. C. et al. American Heart Association Behavioral Change for Improving Health Factors Committee of the Council on Lifestyle and Cardiometabolic Health and Council on Epidemiology and Prevention; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Stroke Council, Dietary Diversity: Implications for Obesity Prevention in Adult Populations: A Science Advisory From the American Heart Association. Circulation 138, e160–e168 (2018).
Trichopoulou, A. T. et al. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 348, 2599–2608 (2003).
Samani, N. J. et al. WTCCC and the Cardiogenics Consortium, Genomewide association analysis of coronary artery disease. N. Engl. J. Med. 357, 443–453 (2007).
Zhang, Q. et al. Three SNPs on chromosome 9p21 confer increased risk of myocardial infarction in Chinese subjects. Atherosclerosis 207, 26–28 (2009).
Chuang, S. Y. et al. Fibrinogen independently predicts the development of ischemic stroke in a Taiwanese population: CVDFACTS study. Stroke 40, 1578–1584 (2009).
Chen, H. J. et al. Influence of metabolic syndrome and general obesity on the risk of ischemic stroke. Stroke 37, 1060–1064 (2006).
Corella, D. P. et al. Mediterranean diet reduces the adverse effect of the TCF7L2-rs7903146 polymorphism on cardiovascular risk factors and stroke incidence: a randomized controlled trial in a high-cardiovascular-risk population. Diabetes Care 36, 3803–3811 (2013).
Weng, L. C. et al. Is ischemic stroke risk related to folate status or other nutrients correlated with folate intake? Stroke 39, 3152–3158 (2008).
Chuang, S. Y. et al. Blood Pressure, Carotid Flow Pulsatility, and the Risk of Stroke: A Community-Based Study. Stroke 47, 2262–2268 (2016).
Buysschaert, I. et al. A variant at chromosome 9p21 is associated with recurrent myocardial infarction and cardiac death after acute coronary syndrome: the GRACE Genetics Study. Eur. Heart J. 31, 1132–1141 (2010).
Virani, S. S. et al. Chromosome 9p21 single nucleotide polymorphisms are not associated with recurrent myocardial infarction in patients with established coronary artery disease. Circ. J. 76, 950–956 (2012).
Schunkert, H. et al. Large-scale association analysis identifies 13 new susceptibility loci for coronary artery disease. Nat Genet 43, 333–338 (2011).
Haver, V. G. et al. The impact of coronary artery disease risk loci on ischemic heart failure severity and prognosis: association analysis in the COntrolled ROsuvastatin multiNAtional trial in heart failure (CORONA). BMC Med Genet 15, 140 (2014).
Wang, A. Z. et al. Association of SNP rs17465637 on chromosome 1q41 and rs599839 on 1p13.3 with myocardial infarction in an American caucasian population. Ann Hum Genet 75, 475–482 (2011).
Zhang, L. et al. Association of rs501120 and rsl7465637 gene polymorphisms with coronary heart disease in the Chinese Han population. J Chin Physician 13, 289 (2011).
Guo, J. et al. Association of single nucleotide polymorphism on chromosome 1p13 and 9p21 with acute cardiac infarction in Chinese population: the AMI study in China. Acad J Second Milit Med Univ 32, 822 (2011).
Li, X. et al. Meta-analysis identifies robust association between SNP rs17465637 in MIA3 on chromosome 1q41 and coronary artery disease. Atherosclerosis 231, 136–140 (2013).
Hara, M. et al. Investigators, Reduced risk of recurrent myocardial infarction in homozygous carriers of the chromosome 9p21 rs1333049 C risk allele in the contemporary percutaneous coronary intervention era: a prospective observational study. BMJ Open 4, e005438 (2014).
Lee, I. T. et al. Value of Chromosome 9p21 Polymorphism for Prediction of Cardiovascular Mortality in Han Chinese Without Coronary Lesions: An Observational Study. Medicine (Baltimore) 94, e1538 (2015).
Franceschini, N. et al. Association of genetic variants and incident coronary heart disease in multiethnic cohorts: the PAGE study. Circ Cardiovasc Genet 4, 661–672 (2011).
Saleheen, D. et al. Association of the 9p21.3 locus with risk of first-ever myocardial infarction in Pakistanis: case-control study in South Asia and updated meta-analysis of Europeans. Arterioscler Thromb Vasc Biol 30, 1467–1473 (2010).
Hiura, Y. et al. Validation of the association of genetic variants on chromosome 9p21 and 1q41 with myocardial infarction in a Japanese population. Circ J 72, 1213–1217 (2008).
Hinohara et al. Replication of the association between a chromosome 9p21 polymorphism and coronary artery disease in Japanese and Korean populations. J Hum Genet 53, 357–359 (2008).
Ding, H. et al. 9p21 is a shared susceptibility locus strongly for coronary artery disease and weakly for ischemic stroke in Chinese Han population. Circ Cardiovasc Genet 2, 338–346 (2009).
Maki, K. C. et al. Limitations of observational evidence: implications for evidence-based dietary recommendations. Adv. Nutr. 5, 7–15 (2014).
Trichopoulou, A. Diet and overall survival in elderly people. BMJ 311, 1457–1460 (1995).
Stewart, R. A. et al. Dietary patterns and the risk of major adverse cardiovascular events in a global study of high-risk patients with stable coronary heart disease. Eur. Heart J. 37, 1993–2001 (2016).
Zheng, Y. Y. et al. Sugar-sweetened beverage intake, chromosome 9p21 variants, and risk of myocardial infarction in Hispanics. Am. J. Clin. Nutr. 103, 1179–1184 (2016).
Corella, D. et al. How does the Mediterranean diet promote cardiovascular health? Current progress toward molecular mechanisms: gene-diet interactions at the genomic, transcriptomic, and epigenomic levels provide novel insights intonew mechanisms. Bioessays 36, 526–537 (2014).
Khera, A. V. et al. Genetic Risk, Adherence to a Healthy Lifestyle, and Coronary Disease. N. Engl. J. Med. 375, 2349–2358 (2016).
Acknowledgements
The study is sponsored by Academia Sinica and the sponsor has no roll in study design, study conduction, data acquisition, data interpretation, and paper writing.
Author information
Authors and Affiliations
Contributions
All investigators of this study (Hsin-Bang Leu, Chia-Min Chung, Jaw-Wen Chen, and Wen-Harn Pan) are in charge of collecting clinical informatics and tissue sample. Dr. Hsin-Bang Leu, and Chia-Min Chung contributed to data analysis and data interpretation. Dr. Hsin-Bang Leu and Wen-Harn Pan contributed to paper writing. All the investigators approved the paper.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Leu, HB., Chung, CM., Chen, JW. et al. The Mediterranean diet reduces the genetic risk of chromosome 9p21 for myocardial infarction in an Asian population community cohort. Sci Rep 9, 18405 (2019). https://doi.org/10.1038/s41598-019-54938-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-54938-w
- Springer Nature Limited