
Abstract
Hypertension not only has a high prevalence, but also brings disease burden to the affected patients. To assess the level of awareness, treatment and control of hypertension in the northeast of China, we investigated the rates of awareness, treatment and control of hypertension and identified its related factors among hypertensive patients aged 18 to 59 years old in Jilin, China. The data (n = 4632) for the present study were extracted from a cross-sectional study in Jilin. Among individuals with hypertension, the standardized rates of awareness, treatment and control of hypertension were 44.9%, 36.5%, 24.3%, respectively. The rates of awareness and treatment of hypertension among middle aged patients were higher than those among young patients. Compared to patients with normal Body Mass index (BMI), obese hypertensive patients had a higher rate of treatment (43.7% vs. 25.9%) and a lower rate of control (18.9% vs. 29.6%). Compared to patients with normal BMI, patients who were obese were more likely to take measures to treat hypertension (OR = 2.50, 95%CI: 2.05–3.05); but were less likely to have well-controlled blood pressure (OR = 0.55, 95%CI: 0.40–0.78). BMI is one of the influencing factors of hypertension awareness, treatment and control among patients 18 to 59 years old with hypertension.
Similar content being viewed by others


Introduction
Cardiovascular diseases (CVDs), a subtype of major non-communicable diseases, account for approximately one third of total global deaths1,2. It is predicted that CVD-related global deaths will climb to more than 23.3 million by 20303. Hypertension is a key risk factor for cardiovascular disease1. In 2008, approximately 40% of adults over 25 years of age had hypertension4. The prevalence of hypertension will be likely to increase 29% by 20255. Worldwide, there are 9.4 million hypertension-related deaths6. Hypertension is the cause of at least 45% of ischemic heart disease deaths, and 51% of stroke deaths7. In China, the prevalence of hypertension increased between 19598 and 20029 according to the National Nutrition and Health Survey (NNHS). It is estimated that 200 million people in China suffer from hypertension10. The prevalence of hypertension in north of China (including the northeast, middle north and northwest) is higher than that in south of China (including the east, middle south and southwest)11. The prevalence of hypertension in the Jilin province, which located in the northeast of China, was 37.3% in a reported study conducted in 201212.
Hypertension is one of the leading contributors to the global disease burden (7.0% of global disability-adjusted-life-years)6. It is estimated that 10% of healthcare spending is directly related to increased blood pressure and its complications13. Hypertension decreases the quality of life and increases the financial burden on health care systems4. Detecting hypertension early and taking measures to control it may be a cost-effective way to reduce the hypertension-related disease burden1. In China, the status of the awareness, treatment and control of hypertension has increased with time. From 1991 to 2011, the rate of awareness of hypertension increased from 33.7 to 54.9%, the rate of treatment increased from 19.9 to 45.9%, and the rate of control increased from 12.6 to 30.1% among hypertension patients14. However, the rates of awareness, treatment and control of hypertension are still lower than that of other countries15,16,17,18.
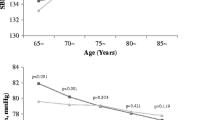
Mean systolic blood pressure decreased in older adults, but increased in younger adults, during the 24 years from 1989 to 201319. Hypertension is increasingly affecting people younger than 50 years old, many of whom die prematurely20. The rates of awareness, treatment and control of hypertension are at low levels among young and middle-aged hypertensive patients14,21. Early intervention programs have impressive influence on the hypertension awareness, treatment and control22. Accordingly, it is necessary to study the related factors of awareness, treatment and control among young and middle-aged hypertensive patients. Previous studies in Jilin province paid more attention to the prevalence and the risk factors of hypertension23,24, but epidemiological investigation of the awareness, treatment and control among hypertensive patients is limited, especially research on young and middle-aged patients. This study investigated the rates of awareness, treatment and control status among hypertensive patients aged 18 to 59 years old and identified the related factors for hypertension awareness, treatment and control.
Results
Characteristics of hypertensive patients
As shown in Table 1, a total of 4632(2556 males and 2076 females) participants completed the questionnaire and all examinations. To make the sampling survey more representatively, we used complex weighted computation throughout the data analysis. The median age of the participants was 49 years old (interquartile range, 43–54 years old). The percent of participants in the young and middle-aged groups were 41.7% and 58.3%, respectively. There were more male patients than female patients in this study (61.5% vs. 38.5%). The median BMI of participants was 25.55 kg/m2 (interquartile range, 23.39–28.07 kg/m2); 30.1% of the participants with normal BMI, 42.2% of the participants were overweight and 26.8% of the participants were obese.
Awareness, treatment and control of hypertension
Table 2 shows the rates of awareness, treatment and control of hypertension of patients in different categories. The rates of awareness, treatment and control of hypertension were 44.9%, 36.5% and 24.3%, respectively. Middle-aged hypertensive patients had higher rates of hypertensive awareness and treatment than young patients (54.2% vs 31.9%, P < 0.001and 45.3% vs 24.3%, P < 0.001, respectively). The incidence of awareness and treatment was lower in men than in women (38.4% vs 55.3%, P < 0.001and 29.7% vs 47.5%, P < 0.001, respectively). Among the target population, different BMI groups had different levels of hypertension awareness, treatment and control status (P < 0.05). Obese patients had higher rates of hypertension awareness (52.6% vs. 33.0%) and treatment (43.7% vs. 25.9%) than patients with normal BMI.
Factors associated with the awareness, treatment and control of hypertension
Table 3 shows the related factors associated with the awareness of hypertension. Middle-aged hypertensive patients were more likely to be aware of hypertension than young patients (OR = 2.07, 95%CI: 1.76–2.44). Male patients were less likely to be aware of hypertension than female (OR = 0.66, 95%CI: 0.54–0.80). Urban patients were less likely to be aware of hypertension than rural patients (OR = 0.73, 95%CI: 0.63–0.84). Single hypertensive patients were less likely to be aware of their blood pressure condition (OR = 0.40, 95%CI: 0.25–0.62) compared to patients who were married. Additionally, overweight patients (OR = 1.89, 95%CI: 1.60–2.24) and obesity patients (OR = 2.58, 95%CI: 2.13–3.12) were more likely to be aware of hypertension than those with normal BMI. Subjects who consumed alcohol products (OR = 0.64, 95%CI: 0.53–0.76) were less likely to be aware of hypertension than those who did not.
The results from the logistic regression model analyzing factors associated with hypertension treatment are shown in Table 4. The model showed that male patients(OR = 0.65,95%CI:0.54–0.79), urban patients(OR = 0.79,95%CI:0.68–0.92), single patients(OR = 0.43,95%CI:0.26–0.69) and individuals who consumed alcohol products(OR = 0.54,95%CI: 0.45–0.65) were less likely to take measures to treat hypertension. It was noted that retired patients (OR = 1.35, 95%CI:1.02–1.79) and patients who were overweight (OR = 1.84, 95%CI:1.55–2.20)or obese (OR = 2.50, 95%CI:2.05–3.05) were more likely to take measures to treat hypertension.
Table 5 shows that gender and urban-rural distribution were not influencing factors of blood pressure control among hypertensive patients. Middle-aged patients were less likely to have well-control BP (OR = 0.72, 95%CI: 0.54–0.95). Obesity (OR = 0.54, 95%CI: 0.39~0.76) was negatively associated with maintaining blood pressure in the appropriate range (BP <140/90 mmHg).
Discussion
In this survey, there were 4632 respondents. Among 18~59 years old respondents with hypertension, 44.9%were aware of their condition; approximately 36.5% of participants used antihypertensive medication while 24.3% had their BP controlled well.
Age is one of the factors that affect the awareness, treatment and control of hypertension in hypertensive patients. In our study, the level of hypertensive awareness and treatment were significantly lower in younger patients than in middle-aged patients, but there was no significant difference in the level of hypertension control. This result was consistent with a previous study in Kazakhstan25. It might be considered that young patients have more adverse life styles and habits than older patients. A study in Iran shows that the rates of awareness, treatment and control of hypertension increased with age26, and a study in Senegal has similar results27. Age is a powerful risk factor for the development of hypertension28. Management of age-associated hypertension may be a key issue in the prevention of cardiovascular events29. Gender differences have been shown in the management of hypertension30. We found that gender is associated with hypertension awareness and treatment; men had larger hypertension prevalence than women among young and middle-aged hypertensive patients but had a lower incidence of awareness and treatment of hypertension than women. This result is similar to those reported in a study in north China31, a study in Korea32 and a study in Malaysian33. There are some researchers in China who concluded that the rates of awareness, treatment and control of hypertension in women were higher than that in men14,34,35. However, Ursua, R. et al.36 found that the rates of awareness, treatment and control of hypertension were not significantly distinct between the sexes. The impact of sex on hypertension and antihypertensive therapy remains unclear. It has been estimated that the overall life expectancy for 50-year-old individuals is 4.9 years shorter for hypertensive women and 5.1 years shorter for hypertensive men compared to normotensive individuals of the same age37. Blood pressure management in male hypertensive patients should be strengthened. Location and marital status are associated with hypertension awareness and treatment. Previous studies have found that patients who lived in urban areas had more opportunities to be aware of their blood pressure level than those who lived in rural areas18,38,39. Interestingly, our study shows a completely opposite result. In our study, we found that patients who came from urban areas might be less likely to be aware of their blood pressure condition and take measures to treat hypertension than those came from rural areas. The reason for this phenomenon was that there were a larger proportion of rural subjects in our research. A previous study indicated that marital status was associated with hypertension awareness and control40. We found that single hypertensive patients were less likely to be aware of their blood pressure condition and be on treatment than patients who were married.
Different BMI groups are associated with hypertension awareness and treatment; obesity is negatively associated with hypertension control. From our research, we found that individuals who were overweight or obese were more likely to be aware of their conditions and be on treatment than those with normal BMI. Pereira, M. et al.41 also suggest that awareness of hypertension is directly associated with BMI in both males and females; participants who are overweight or obese are more likely to be aware of hypertension and take hypertension medication. Supiyev, A. et al.25 and Evelyn, P. et al.42 found that obese patients are more likely to be aware of their hypertension. Lei, W. et al.43 reported that a higher BMI was significantly associated with hypertension awareness and treatment in both 2001 and 2010 among an urban elderly population. Moreover, patients who were obese may not decrease their BP below 140/90 mmHg compared to those with normal BMI. Work by Pereira, M. et al.41 also suggested that BMI is associated with a lower likelihood of blood pressure control. Hu, M. et al.44 have a different view about the relationship between obesity and blood pressure control; they suggest that it is easier for obese patients to have well-control blood pressure. The prevalence of hypertension increases with increasing BMI21. The current study found that BMI was a more reliable predictor of hypertension for senior adults45. Obesity increases the risk of treatment-resistant arterial hypertension46. Thus, obese patients with hypertension should pay more attention to the control of their hypertension. Clinical trials have demonstrated that weight loss of approximately 10% of a patient’s original body weight, by calorie restriction and/or increased activity, is an effective means to achieve clinically meaningful reductions in blood pressure and mortality from cardiovascular disease47. Reductions in BMI are associated with decreases in carotid intima media thickness and improvements in the cardiovascular risk-factor profile, suggesting that weight loss is worthwhile because it might result in long-term benefit48.
Alcohol consumption is related to hypertension awareness, treatment and control. Individuals who consumed alcohol products could be more likely to ignore hypertension awareness and treatment than those who do not consumed alcohol. Yang, L. et al.35 concluded that abstaining from alcohol is associated with hypertension treatment and affects the control of hypertension. However, Hu, M. et al. have a different perspective and report that alcohol consumption is associated with a higher rate of hypertension awareness44.
The sample for this study was extracted from a complex sampling scheme, and the sample size was large. However, there are still some limitations to our study. This study was a cross-sectional study. The definitions of hypertension awareness and anti-hypertensive treatments were all acquired from self-reported questionnaires, which can cause reporting bias. The life styles (smoking, consuming alcohol products, physical exercises) were also self-reported and provided from memory, which may cause some recall bias.
In conclusion, the rates of awareness and treatment of hypertension among middle aged patients were higher than that in young patients. The condition of awareness and treatment among male hypertensive patients were poor. Obese hypertensive patients may be less likely to maintain blood pressure within the normal range. Young hypertensive patients, male hypertensive patients and obese hypertensive patients may benefit from improved hypertension management.
Methods
Population sample
This study is based on the 2012 Survey on Chronic Diseases in Jilin, China49,50. The survey data were collected from a multistage stratified cluster sample. The sample size has been estimated according to the prevalence of chronic disease in Jilin province. The sampling process included five stages. In the first stage, 9 cities (Changchun, Jilin, Siping, Liaoyuan,Tonghua, Baishan, Songyuan, Baicheng and Yanbian) were chosen from 32 districts/counties for inclusion in the study; they were identified by the proportion of the population, the location of the whole province and the race of their residents. In the second stage, towns were selected by stratified random sampling based on the size of the district. In the third stage, three committees which were near each selected towns were chosen by stratified random sampling. In the fourth stage, one village which was close to the selected committee was chosen by simple random sampling. In the fifth stage, individuals were chosen by cluster random sampling. Finally, 23050 subjects from 32 districts/counties were enrolled, and 21435 participants completed the survey (response rate: 84.9%)49. The survey included three aspects: a face-to-face questionnaire interview by trained investigators, a physical examination (measurement of height, weight and blood pressure) and a laboratory examination. The study was performed in accordance with the principles of the Declaration of Helsinki. Data in this study came from the epidemiologic investigation of the project (Survey on Chronic Diseases in Jilin, China, 2012), specifically from the part which contained information on participants with hypertension that were 18 to 59 years old. Ultimately, 4632 participants were included in the present study. The flowchart of the participants included in or excluded from the present study is shown in Fig. 1.

Flowchart of the participants included in or excluded from the present study.
Definition
Hypertension was defined as any blood pressure where the mean systolic blood pressure was equal to or higher than 140 mmHg and/or the mean diastolic blood pressure was higher than 90 mmHg, and/or the self-reported use of antihypertensive medication in the past two weeks after having had a diagnosis of hypertension by a physician at the county-level or above51. After at least 5 minutes rest first, blood pressure was measured two times by an electric sphygmomanometer (HEM-7200, OMRON, Dalian, China) on the arm in the sitting position; the final blood pressure was the average of the two measurement results.
Awareness of hypertension was defined as a self-reported diagnosis of hypertension by physicians. Individuals who had used anti-hypertension medications in the past 2 weeks prior to the interview were classified as being on treatment. Control was defined as systolic blood pressure lower than 140 mm Hg and diastolic blood pressure lower than 90 mm Hg among hypertensive patients who were being treated.
Subjects aged 18–44 years old were defined as the young group and subjects aged 45–59 years old were defined as the middle-aged group50. Education levels were divided into four groups: primary school or lower (including those who never attended school and those who only finished elementary school, years of education ≤6), junior high school (6 < years of education ≤9), senior high school (including those who attended senior high school and those who attended secondary vocational education, 9 < years of education ≤12) and university or above(including undergraduate and graduate levels of education, years of education >12). Occupation status was classified into four groups: manual workers (including farmers, factory workers, and service workers), mental workers (including teachers, researchers, office assistants, and others technical staff), retirees and other kinds of workers (including students and unemployed persons).
Body mass index (BMI) was calculated as weight in kilograms divided by height in metres squared; BMI was classified into four groups according to the Chinese BMI classification criteria: underweight (BMI <18.5 kg/m2), normal (18.5≤ BMI <24 kg/m2), overweight (24≤ BMI <28 kg/m2), and obese (BMI ≥28 kg/m2)52. Smoking status included three groups: Never, Current, and Past. Never smokers were individuals who reported never having smoked up to 100 cigarettes. Current smokers were individuals who consumed any kind of tobacco products per day in the past 30 days. Past smokers were individuals who had smoked before but had quit at least three months prior53. Participants who consumed any kind of alcoholic beverage during the past year before the interview were defined as current drinkers. Physical exercise (excluding regular activity associated with daily life) status was divided into three levels: the ‘Never or rare’ group included individuals who never or seldom exercised; the ‘Exercise sometimes’ group included individuals who exercised one or two times per week; the ‘Often exercise’ group included individuals who exercised more than three times per week54.
Ethics
The Health Bureau of Jilin province approved this project. The School of Public Health, Jilin University, organized the investigation. Each participants in the research signed written informed consent.
Statistical analysis
The analysis of this study was conducted using SPSS version 22.0 statistical software (IBM Corp, Armonk, NY, USA). We used a weighted approach throughout the data analysis. An all-data weighted statistical analysis was implemented using the complex sample function in SPSS. The data was weighted by age, sex, and region (urban or rural) according to the demographic data of the statistical bureau of Jilin province to make more it representative of the 18~59 years old hypertensive patients in that province. The characteristics of participants were described by frequency and percentage. Descriptive analyses for non-normally distributed of quantitative data were described by median and interquartile range. The standardized rates of awareness, treatment and control of hypertension were weighted by age, sex, and region (urban or rural) in Jilin Province of China. The comparison of the prevalence of awareness, treatment and control among hypertensive patients in different categories were conducted by Rao-Scott Chi-square tests for complex samples. The regression analysis was first carried out by univariate regression analysis first. Factors that had a significant P value in the univariate regression were brought into the multivariable regression analysis. The multivariable logistic regression analysis was mandatorily adjusted for age, gender and region (urban or rural). Binary logistic regression analyses (Method: Forward: LR) were performed to identify potential independent factors associated with the awareness, treatment and control of hypertension. The significance threshold was 0.05.
References
The World Health Organization in collaboration with the World Heart Federation and the World Stroke Organization. Cardiovascular Disease: Global Atlas on Cardiovascular Disease Prevention and Control (Geneva, 2012).
World Health Organization. GLOBAL STATUS REPORT on noncommunicable diseases 2014 (Geneva, 2014).
Mathers, C. D. & Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS medicine 3, e442, https://doi.org/10.1371/journal.pmed.0030442 (2006).
World Health Organization. A global brief on hypertension-silent killer, global public health crisis (2013).
Mittal, B. V. & Singh, A. K. Hypertension in the developing world: challenges and opportunities. American journal of kidney diseases: the official journal of the National Kidney Foundation 55, 590–598, https://doi.org/10.1053/j.ajkd.2009.06.044 (2010).
Lim, S. S. et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet (London, England) 380, 2224–2260, https://doi.org/10.1016/s0140-6736(12)61766-8 (2012).
Department of Health Statistics and Informatics, World Health Organization, Causes of death 2008: data sources and methods (Geneva, 2011).
JS, H. The summary report of the National Symposium on Heart and Vascular Diseases. (The Collection of Scientific Reports on the National Symposium on Heart and Vascular Diseases, Beijing, China, 1960).
Wang, L. D. et al. Nutrition and Health Status in Chinese People (Beijing, China, 2005).
Hu, S. S. et al. Outline of the report on cardiovascular disease in China, 2010. Biomedical and environmental sciences: BES 25, 251–256, https://doi.org/10.3967/0895-3988.2012.03.001 (2012).
Wang, X., Bots, M. L., Yang, F., Hoes, A. W. & Vaartjes, I. Prevalence of hypertension in China: a systematic review and meta-regression analysis of trends and regional differences. Journal of hypertension 32, 1919–1927; discussion 1927, https://doi.org/10.1097/hjh.0000000000000252 (2014).
Yu, J. et al. Risk Factors for Cardiovascular Disease and Their Clustering among Adults in Jilin (China). International journal of environmental research and public health 13, ijerph13010070, https://doi.org/10.3390/ijerph13010070 (2015).
Gaziano, T. A., Bitton, A., Anand, S. & Weinstein, M. C. The global cost of nonoptimal blood pressure. Journal of hypertension 27, 1472–1477, https://doi.org/10.1097/HJH.0b013e32832a9ba3 (2009).
Guo, J. et al. The dynamics of hypertension prevalence, awareness, treatment, control and associated factors in Chinese adults: results from CHNS 1991–2011. Journal of hypertension 33, 1688–1696, https://doi.org/10.1097/hjh.0000000000000594 (2015).
Polonia, J., Martins, L., Pinto, F. & Nazare, J. Prevalence, awareness, treatment and control of hypertension and salt intake in Portugal: changes over a decade. The PHYSA study. Journal of hypertension 32, 1211–1221, https://doi.org/10.1097/hjh.0000000000000162 (2014).
Ghaffari, S. et al. The prevalence, awareness and control rate of hypertension among elderly in northwest of Iran. Journal of cardiovascular and thoracic research 8, 176–182, https://doi.org/10.15171/jcvtr.2016.35 (2016).
Olives, C., Myerson, R., Mokdad, A. H., Murray, C. J. & Lim, S. S. Prevalence, awareness, treatment, and control of hypertension in United States counties, 2001–2009. PloS one 8, e60308, https://doi.org/10.1371/journal.pone.0060308 (2013).
Chow, C. K. et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. Jama 310, 959–968, https://doi.org/10.1001/jama.2013.184182 (2013).
Heiniger, S., Viswanathan, B., Gedeon, J., Paccaud, F. & Bovet, P. Trends in prevalence, awareness, treatment and control of high blood pressure in the Seychelles between 1989 and 2013. Journal of hypertension. https://doi.org/10.1097/hjh.0000000000001358 (2017).
World Health Organisation. Global health risks: mortality and burden of disease attributable to selected major risk. (Geneva, 2009).
Musinguzi, G. & Nuwaha, F. Prevalence, awareness and control of hypertension in Uganda. PloS one 8, e62236, https://doi.org/10.1371/journal.pone.0062236 (2013).
Jeemon, P. et al. Impact of comprehensive cardiovascular risk reduction programme on risk factor clustering associated with elevated blood pressure in an Indian industrial population. The Indian journal of medical research 135, 485–493 (2012).
Wei, Q. et al. Prevalence of hypertension and associated risk factors in Dehui City of Jilin Province in China. Journal of human hypertension 29, 64–68, https://doi.org/10.1038/jhh.2014.32 (2015).
Yang, G. et al. Prevalence and Correlates of Prehypertension and Hypertension among Adults in Northeastern China: A Cross-Sectional Study. International journal of environmental research and public health 13, 82, https://doi.org/10.3390/ijerph13010082 (2015).
Supiyev, A. et al. Prevalence, awareness, treatment and control of arterial hypertension in Astana, Kazakhstan. A cross-sectional study. Public health 129, 948–953, https://doi.org/10.1016/j.puhe.2015.02.020 (2015).
Khosravi, A. et al. The impact of a 6-year comprehensive community trial on the awareness, treatment and control rates of hypertension in Iran: experiences from the Isfahan healthy heart program. BMC cardiovascular disorders 10, 61, https://doi.org/10.1186/1471-2261-10-61 (2010).
Macia, E., Duboz, P. & Gueye, L. [Arterial hypertension in Dakar: Prevalence, awareness, treatment, and control]. Bulletin de la Societe de pathologie exotique (1990) 108, 49–56, https://doi.org/10.1007/s13149-014-0369-2 (2015).
Franklin, S. S. et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 96, 308–315 (1997).
Fukutomi, M. & Kario, K. Aging and hypertension. Expert review of cardiovascular therapy 8, 1531–1539, https://doi.org/10.1586/erc.10.78 (2010).
Gu, Q., Burt, V. L., Paulose-Ram, R. & Dillon, C. F. Gender differences in hypertension treatment, drug utilization patterns, and blood pressure control among US adults with hypertension: data from the National Health and Nutrition Examination Survey 1999-2004. American journal of hypertension 21, 789–798, https://doi.org/10.1038/ajh.2008.185 (2008).
Fan, G. et al. Prevalence, awareness, treatment and control of hypertension in rural areas in North China in 2013. Zhonghua yi xue za zhi 95, 616–620 (2015).
Moon, J. Y. et al. A trend analysis of the prevalence, awareness, treatment, and control of hypertension by age group. Journal of preventive medicine and public health=Yebang Uihakhoe chi 46, 353–359, https://doi.org/10.3961/jpmph.2013.46.6.353 (2013).
Abdul-Razak, S. et al. Prevalence, awareness, treatment, control and socio demographic determinants of hypertension in Malaysian adults. BMC public health 16, 351, https://doi.org/10.1186/s12889-016-3008-y (2016).
Ke, L. et al. Prevalence, awareness, treatment and control of hypertension in Macau: results from a cross-sectional epidemiological study in Macau, China. American journal of hypertension 28, 159–165, https://doi.org/10.1093/ajh/hpu121 (2015).
Yang, L. et al. Prevalence, Awareness, Treatment, Control and Risk Factors Associated with Hypertension among Adults in Southern China, 2013. PloS one 11, e0146181, https://doi.org/10.1371/journal.pone.0146181 (2016).
Ursua, R. et al. Awareness, treatment and control of hypertension among Filipino immigrants. Journal of general internal medicine 29, 455–462, https://doi.org/10.1007/s11606-013-2629-4 (2014).
Franco, O. H., Peeters, A., Bonneux, L. & de Laet, C. Blood pressure in adulthood and life expectancy with cardiovascular disease in men and women: life course analysis. Hypertension (Dallas, Tex.: 1979) 46, 280–286, https://doi.org/10.1161/01.HYP.0000173433.67426.9b (2005).
Li, W. et al. Hypertension prevalence, awareness, treatment, and control in 115 rural and urban communities involving 47 000 people from China. Journal of hypertension 34, 39–46, https://doi.org/10.1097/hjh.0000000000000745 (2016).
Gupta, R. et al. Association of Household Wealth Index, Educational Status, and Social Capital with Hypertension Awareness, Treatment, and Control in South Asia. American journal of hypertension, https://doi.org/10.1093/ajh/hpw169 (2017).
Abu-Saad, K. et al. Blood pressure level and hypertension awareness and control differ by marital status, sex, and ethnicity: a population-based study. American journal of hypertension 27, 1511–1520, https://doi.org/10.1093/ajh/hpu081 (2014).
Pereira, M., Azevedo, A. & Barros, H. Determinants of awareness, treatment and control of hypertension in a Portuguese population. Revista portuguesa de cardiologia: orgao oficial da Sociedade Portuguesa de Cardiologia=Portuguese journal of cardiology: an official journal of the Portuguese Society of Cardiology 29, 1779–1792 (2010).
Davila, E. P. et al. Prevalence, management, and control of hypertension among US workers: does occupation matter? Journal of occupational and environmental medicine 54, 1150–1156, https://doi.org/10.1097/JOM.0b013e318256f675 (2012).
Wu, L. et al. Trends in Prevalence, Awareness, Treatment and Control of Hypertension during 2001–2010 in an Urban Elderly Population of China. PloS one 10, e0132814, https://doi.org/10.1371/journal.pone.0132814 (2015).
Hu, M. et al. Prevalence, awareness, treatment, and control of hypertension and associated risk factors among adults in Xi’an, China: A cross-sectional study. Medicine 95, e4709, https://doi.org/10.1097/md.0000000000004709 (2016).
Chen, H. & Dai, J. BMI better explains hypertension in Chinese senior adults and the relationship declines with age. Aging clinical and experimental research 27, 271–279, https://doi.org/10.1007/s40520-014-0285-0 (2015).
Jordan, J. et al. Joint statement of the European Association for the Study of Obesity and the European Society of Hypertension: obesity and difficult to treat arterial hypertension. Journal of hypertension 30, 1047–1055, https://doi.org/10.1097/HJH.0b013e3283537347 (2012).
Appel, L. J. et al. Dietary approaches to prevent and treat hypertension: a scientific statement from the American Heart Association. Hypertension (Dallas, Tex.: 1979) 47, 296–308, https://doi.org/10.1161/01.hyp.0000202568.01167.b6 (2006).
Charakida, M. et al. Lifelong patterns of BMI and cardiovascular phenotype in individuals aged 60-64 years in the 1946 British birth cohort study: an epidemiological study. The lancet. Diabetes &. endocrinology 2, 648–654, https://doi.org/10.1016/s2213-8587(14)70103-2 (2014).
Wang, S. et al. Rural-urban differences in the prevalence of chronic disease in northeast China. Asia-Pacific journal of public health 27, 394–406, https://doi.org/10.1177/1010539514551200 (2015).
Wang, R. et al. Situation of Diabetes and Related Disease Surveillance in Rural Areas of Jilin Province, Northeast China. International journal of environmental research and public health 13, https://doi.org/10.3390/ijerph13060538 (2016).
Liu, L. S. 2010 Chinese guidelines for the management of hypertension. Zhonghua xin xue guan bing za zhi 39, 579–615 (2011).
Zhou, B. F. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomedical and environmental sciences: BES 15, 83–96 (2002).
Schoenborn, C. A. & Adams, P. E. Health behaviors of adults: United States, 2005–2007. Vital and health statistics. Series 10, Data from the National Health Survey, 1–132 (2010).
Wang, C. et al. Awareness, treatment, control of diabetes mellitus and the risk factors: survey results from northeast China. PloS one 9, e103594, https://doi.org/10.1371/journal.pone.0103594 (2014).
Acknowledgements
The data used for the current research is from the 2012 Survey on Chronic Diseases in Jilin, China. This Survey was funded by the Scientific Research Foundation of the Health Bureau of Jilin Province, China (Grant Number: 2011Z116). The study was performed in accordance with the principles of the Declaration of Helsinki.
Author information
Authors and Affiliations
Contributions
X.L., H.N., Y.Q., M.L., L.L., X.M., S.J., C.G., R.W., P.Z. and B.L. designed the study. X.L., H.N. and Y.Q. performed the study. X.L. analysed the data and drafted the manuscript. X.L., H.N., Y.Q., M.L. and L.L. participated in amending the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lv, X., Niu, H., Qu, Y. et al. Awareness, treatment and control of hypertension among hypertensive patients aged 18 to 59 years old in the northeast of China. Sci Rep 8, 17019 (2018). https://doi.org/10.1038/s41598-018-34923-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-34923-5
- Springer Nature Limited
Keywords
This article is cited by
-
Undiagnosed hypertension and its determinants among hypertensive patients in rural districts of northwest Ethiopia: a mediation analysis
BMC Health Services Research (2023)