
Abstract
Aldehyde dehydrogenase (ALDH) is a key enzyme for the catalytic oxidation of acetaldehyde to acetic acid. Genetic polymorphisms of ALDH2 have been associated with a wide range of diseases and cancers. However, little information is found about the association between ALDH2 polymorphisms and lumbar disc herniation (LDH) in Chinese Han population. We investigated the association between single nucleotide polymorphisms (SNPs) in ALDH2 and LDH risk in a case–control study that included 380 LDH cases and 692 healthy controls. Eight SNPs were selected and genotyped using the Sequenom MassARRAY platform. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using unconditional logistic regression after adjusting for gender and age. In the allele model analysis, we found the frequency of the “A” allele of rs671 was significantly higher in LDH cases than in controls (OR = 1.414, 95%CI: 1.109–1.803, P = 0.005). In the genetic model analysis, we found the minor allele “A” of rs671 was associated with increased risk of LDH under log-additive model (OR = 1.42, 95%CI: 1.11–1.82, P = 0.0062); and the minor allele “C” of rs7296651 was associated with decreased risk of LDH under over-dominant model (OR = 0.72, 95%CI: 0.53–0.97, P = 0.031). Additionally, the haplotype “GGCTCACG” constructed by rs886205, rs2238152, rs4648328, rs441, rs4646778, rs671, rs11066028, and rs7296651 was associated with increased risk of LDH (OR = 1.45; 95% CI = 1.11–1.90; P = 0.0071). Our data shed new light on the association between genetic polymorphisms of ALDH2 and LDH susceptibility in a Chinese Han population.
Similar content being viewed by others


Introduction
Lumbar disc herniation (LDH) is one of the most common diseases, which mainly caused by the varying degrees of degenerative changes of lumbar intervertebral disc1. LDH can stimulate or oppress the spinal nerve root and result in a series of clinical symptoms, including low-back pain, and unilateral leg pain2. Although it is a benign disease, it is still make patients suffer from debilitation, disability, low quality of life and work, and high costs of health care3. Epidemiologic studies identified that gender, age, body mass index, smoking, type of occupation and level of physical activity are primary risk factors for degeneration and herniation of lumbar disc4. However, subsequent twin studies showed that more than 70% of the LDH patients have genetic origin5, which means genetics may play a more important role than environmental factors in the occurrence and development of LDH. To date, genome wide association studies (GWAS) have identified several types of susceptibility genes associated with the degeneration of lumbar intervertebral disc, including structural related genes (ACAN, COL1, COL9, FN, HAPLN1, THBS), catabolic related genes (MMP and TIMP), inflammatory related genes (IL1, IL6, COX2) and so on6. However, this is still not enough to explain the hereditary susceptibility of LDH.
Aldehyde dehydrogenase (ALDH) is a key enzyme for the catalytic oxidation of acetaldehyde to acetic acid. Specifically, ALDH in the liver is responsible for the oxidation of ethanol (the composition of the wine) to acetaldehyde, and the acetaldehyde as a substrate is further catalyzed by ALDH and converted to non-hazardous acetic acid (the composition of the vinegar). ALDH has two isozymes, ALDH1 in the cytosol and ALDH2 in mitochondria. ALDH2 is located on chromosome 12q24.12 region. Previous studies have demonstrated that genetic polymorphisms of ALDH2 is associated with alcohol dependence7, flushing response8, and risk of digest tract cancers9,10. Recently, increased mitochondrial ALDH2 level has been found in skeletal muscle of SOD1 knockout mice, which may be involved in the nerve redox signaling in regulation of degenerative pathways in skeletal muscle11. However, little information is found about the association between genetic polymorphisms in ALDH2 and the risk of LDH.
In this case-control study, we genotyped eight single nucleotide polymorphism (SNPs) in ALDH2: rs886205, rs2238152, rs4648328, rs441, rs4646778, rs671, rs11066028, and rs7296651, and performed a comprehensive association analysis to identify SNPs associated with LDH risk in a Chinese Han population.
Results
A total of 380 LDH patients and 692 healthy controls were recruited in the study. The distribution of gender and age of the patient and control groups are described in Table 1. The mean age of the participants was 50.43 ± 12.27 years in the case group and 48.21 ± 10.38 years in the control group. There were no significant difference in the distributions of gender and age between LDH patients and healthy controls (p > 0.05). More than 90% LDH patients have herniation in L4-L5 and L5-S1. The percent of ligmaentum flayum hypertrophy and hyperplasia, dural sac compression, nerve root compression, spinal canal stenosis and abnormal MRI signal in LDH patients were 3.7%, 32.4%, 5.3%, 12.4% and 1.8%, respectively.
All SNP call rates exceeded 99%, which was considered high enough to perform association analyses. The basic information of the ALDH2 polymorphisms (rs886205, rs2238152, rs4648328, rs441, rs4646778, rs671, rs11066028, and rs7296651) are shown in Table 2, including gene, band, position, role, alleles and minor allele frequency (MAF). We compared the difference in frequency distributions of alleles between LDH cases and controls by Chi-square test and found one significant SNP was associated with LDH risk. The frequency of the “A” allele of rs671 was significantly higher in LDH cases than in controls (0.176 versus 0.132), which suggested that “A” allele of rs671 was a risk allele for LDH risk (OR = 1.414, 95%CI: 1.109–1.803, P = 0.005).
The genotype frequencies of the ALDH2 polymorphisms are shown in Table 3. We identified two SNPs, rs671 and rs7296651, associated with LDH risk after adjusted for gender and age. Compared with the GG genotype, the GA frequencies of rs671 polymorphism among cases were different from the controls (GA vs. GG: OR = 1.38; 95%CI = 1.04–1.84; p = 0.022), which suggested that the GA genotype of rs671 had an increased effect on LDH risk. Additionally, compared with individuals with the rs7296651 GG genotype, individuals with CG genotype had a decreased LDH risk (CG vs. GG: OR = 0.73; 95%CI = 0.54–0.99; p = 0.024).
Next, we assumed that the major allele of each SNP was a reference allele and calculated the odd ratio and 95%CI between each variant and LDH risk under four genetic models (Table 4). Two susceptibility SNPs were found to be associated with LDH risk after the adjustment: the minor allele “A” of rs671 was associated with increased risk of LDH under log-additive model (OR = 1.42, 95%CI: 1.11–1.82, P = 0.0062); the minor allele “C” of rs7296651 was associated with decreased risk of LDH under over-dominant model (OR = 0.72, 95%CI: 0.53–0.97, P = 0.031).
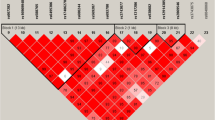
Finally, the relationship of ALDH2 haplotypes with the risk of developing LDH was also evaluated. Figure 1 showed the linkage disequilibrium (LD) block in ALDH2. The association between different haplotypes and BC risk was shown in Table 5. The haplotype “GGCTCACG” constructed by rs886205, rs2238152, rs4648328, rs441, rs4646778, rs671, rs11066028, and rs7296651 was associated with increased risk of LDH after the adjustment (OR = 1.45; 95% CI = 1.11–1.90; P = 0.0071).

D’ linkage map for the eight SNPs in ALDH2 The linkage disequilibrium (LD) block was constructed by rs886205, rs2238152, rs4648328, rs441, rs4646778, rs671, rs11066028, and rs7296651.
Discussion
To date, several studies have investigated the association between genetic polymorphisms and risk of intervertebral disc degeneration, and identified a wide range of susceptibility genes and SNPs for degeneration of intervertebral disc in different populations3,6. However, due to the small sample scale and the insufficient study designs and methods in the laboratory, the results identified in previous studies need further replication, and this research direction is still worth to be further explored. The goal of this study was to assess the association between genetic polymorphisms of ALDH2 and risk of LDH. Our findings indicate that the “A” allele of rs671 was associated with increased risk of LDH; while the “C” allele of rs7296651 was associated with decreased risk of LDH. Additionally, the haplotype “GGCTCACG” constructed by rs886205, rs2238152, rs4648328, rs441, rs4646778, rs671, rs11066028, and rs7296651 was associated with increased risk of LDH.
ALDH2 is a key enzyme for alcohol metabolism, and the ALDH2 gene is a highly polymorphic gene. By far, previous association studies have identified more than 80 SNPs in ALDH2 gene that associated with a wide range of disease and different types of cancers12. Among these SNPs, rs671 was most widely studied. Rs671, also known as Glu487Lys or Glu504Lys, is a functional SNP in exon 12 of ALDH2, which could destroy the combination of ALDH2 enzyme and its coenzymes and further lead to the decreased enzymatic activity of ALDH213,14. Rs671 polymorphism has been found closely associated with many types of cancers, including esophageal cancer, gastric cancer, hepatocellular carcinoma, colorectal cancer, squamous cell carcinoma of head and neck, and lung cancer12. Beyond that, rs671 was also associated with several types of age-related disease, including late-onset Alzheimer’s disease, Parkinson’s disease, type II diabetes mellitus, coronary heart disease and myocardial infarction15,16,17. However, there is a limited number of literatures about the ALDH2 polymorphisms associated with disease of orthopedics. In 2006, rs671 was found to be associated with osteoporosis in elderly Japanese population18. Until recently, one study pointed out that rs671 have a significant correlation with hip fracture19. Our study is the first reported that rs671 is associated with risk of LDH, which shed new light on the association between ALDH2 polymorphisms and disease of orthopedics.
In addition to rs671, we also investigated seven SNPs in the intron region of ALDH2. Rs886205 polymorphism was well studied in association studies, and has been identified have association with esophageal cancer in a Chinese population20. Rs2238152 polymorphism and its interaction with alcohol intake was associated with risk of hypertension21. Rs4648328 was found to be have effect on the methadone dose and adverse reactions in drug addicts22. Little information is found about the rest four SNPs, rs441, rs4646778, rs11066028, and rs7296651, in literatures. In the presents study, we found that rs7296651 is associated with risk of LDH, which still needs to be confirmed in a larger Chinese cohort.
Some limitations should to be considered in our study. First, all the participants were collected from our hospital, which may only represent a fraction of Chinese population. Second, LDH is a complex disease that influenced by multiple genes and environmental factors. Because we have no data on the specific information about body mass index, smoking status, type of work and level of physical activity, we could not explore the interactions between ALDH2 polymorphisms and environmental factors in development of LDH. Further studies will focus on the interactions between rs671 and rs7296651 in ALDH2 and environmental factors in risk of LDH.
In conclusion, the present study provided new evidence that rs671 and rs7296651 in ALDH2 are associated with risk of LDH in a Chinese Han population, which could be considered as potential target sites for novel treatment strategies for LDH. However, further functional study base on animal model must be conducted to demonstrate the biological role of rs671 and rs7296651 variants in the occurrence and development of LDH.
Materials and Methods
Subjects
All participants in our study were unrelated Han Chinese individuals and living in Shaanxi Province. A total of 380 LDH patients and 692 healthy controls were consecutively recruited between September 2015 and September 2017 at the Xi’an Jiaotong University Hospital Medical College Red Cross Hospital, Xi’an, People’s Republic of China. All the patients were recently diagnosed with LDH according to the magnetic resonance imaging (sagittal and axial images obtained with a 1.5-T imaging system), and a history of unilateral pain from the femoral or sciatic nerve to the corresponding dermatome of the nerve root for more than three months. Patients with trauma-related LDH, rheumatic, spinal tumor or spondylitis were excluded. The control group was randomly selected healthy individuals, which with no known disease, and no history of any cancers.
All subjects were at least 18 years old and were in good mental condition. All of the participants provided written informed consent.
SNP selection and genotyping
Eight SNPs were chosen from previously published polymorphisms associated with alcohol dependence21,23,24,25, with minor allele frequencies >5% in the HapMap Chinese Han Beijing population. To date, these SNPs have not been reported for LDH susceptibility. DNA extraction and concentrations were done as previously described26,27,28. SNP genotyping was performed by the Sequenom MassARRAY RS1000, and the data analyses were completed by Sequenom Type 4.0.
Statistical analyses
All of the statistical analyses were performed with Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and the SPSS 21.0 statistical package (SPSS, Chicago, IL, USA). Allele frequencies in the control subjects were tested for departure from Hardy–Weinberg Equilibrium (HWE) before analysis. Differences between the cases and controls in the distributions of gender, age and allele frequencies of the SNPs were evaluated using chi-square tests for categorical variables and Welch’s t tests for continuous variables. Associations between the genotypes of the ALDH2 polymorphisms, and the risk of LDH were estimated by computing odds ratios (ORs) and 95% confidence intervals (CIs) from unconditional logistic regression analysis with adjustment for gender and age. Four models (codominant, dominant, recessive, and log-additive) were used to assess the association between each genotype and the LDH risk. Akaike’s Information criterion (AIC) and Bayesian Information criterion (BIC) were used to select the best model for each SNP. The best model was with the minimum sum of AIC and BIC. All p values presented in this study were two sided, and p = 0.05 was considered the cutoff for statistical significance.
Haploview software version 4.2 was used to analyze the association between haplotypes and the LDH. Linkage disequilibrium (LD) analysis was performed using genotype data from all the subjects. The pattern of LD was analyzed using two parameters, r2 and D′. Statistical significance was established when p < 0.05.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Mio, M. F. et al. A Functional Polymorphism in COL11A1, Which Encodes the α1 Chain of Type XI Collagen, Is Associated with Susceptibility to Lumbar Disc Herniation. American Journal of Human Genetics 81, 1271 (2007).
Vialle, L. R., Vialle, E. N., Henao, J. E. S. & Giraldo, G. Hérnia discal lombar. Rev. bras. ortop 45, 17–22 (2010).
Eskola, P. J. et al. Genetic association studies in lumbar disc degeneration: a systematic review. Plos One 7, e49995 (2012).
Andersson, G. B. J. & Andersson, G. B. Epidemiology of low back pain. Acta Orthopaedica Scandinavica Supplementum 281, 28–31 (1998).
Battié, M. C., Videman, T., Levälahti, E., Gill, K. & Kaprio, J. Genetic and environmental effects on disc degeneration by phenotype and spinal level: a multivariate twin study. Spine 33, 2801–2808 (2008).
Mayer, J. E. et al. Genetic polymorphisms associated with intervertebral disc degeneration. Spine Journal 13, 299–317 (2013).
Matsuo, K. et al. Alcohol dehydrogenase 2 His47Arg polymorphism influences drinking habit independently of aldehyde dehydrogenase 2 Glu487Lys polymorphism: analysis of 2,299 Japanese subjects. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 15, 1009–1013, https://doi.org/10.1158/1055-9965.epi-05-0911 (2006).
Thomasson, H. R., Crabb, D. W., Edenberg, H. J. & Li, T. K. Alcohol and aldehyde dehydrogenase polymorphisms and alcoholism. Behavior genetics 23, 131–136 (1993).
Brooks, P. J., Enoch, M. A., Goldman, D., Li, T. K. & Yokoyama, A. The alcohol flushing response: an unrecognized risk factor for esophageal cancer from alcohol consumption. PLoS medicine 6, e50, https://doi.org/10.1371/journal.pmed.1000050 (2009).
Salaspuro, M. Interactions of alcohol and tobacco in gastrointestinal cancer. Journal of gastroenterology and hepatology 27(Suppl 2), 135–139, https://doi.org/10.1111/j.1440-1746.2012.07017.x (2012).
Sakellariou, G. et al. Comparison of whole body SOD1 knockout with muscle specific SOD1 knockout mice reveals a role for nerve redox signaling in regulation of degenerative pathways in skeletal muscle. Antioxid Redox Signal 28 (2017).
Li, R., Zhao, Z., Sun, M., Luo, J. & Xiao, Y. ALDH2 gene polymorphism in different types of cancers and its clinical significance. Life sciences 147, 59–66 (2016).
Crabb, D. W., Edenberg, H. J., Bosron, W. F. & Li, T. K. Genotypes for aldehyde dehydrogenase deficiency and alcohol sensitivity. The inactive ALDH2(2) allele is dominant. The Journal of clinical investigation 83, 314–316, https://doi.org/10.1172/jci113875 (1989).
Yoshida, A., Huang, I. Y. & Ikawa, M. Molecular abnormality of an inactive aldehyde dehydrogenase variant commonly found in Orientals. Proceedings of the National Academy of Sciences of the United States of America 81, 258–261 (1984).
Wang, B. et al. The association of mitochondrial aldehyde dehydrogenase gene (ALDH2) polymorphism with susceptibility to late-onset Alzheimer’s disease in Chinese. Journal of the Neurological Sciences 268, 172–175 (2008).
Xu, F. et al. ALDH2 genetic polymorphism and the risk of type II diabetes mellitus in CAD patients. Hypertension Research Official Journal of the Japanese Society of Hypertension 33, 49–55 (2010).
Han, H. et al. Association of genetic polymorphisms in ADH and ALDH2 with risk of coronary artery disease and myocardial infarction: a meta-analysis. Gene 526, 134–141 (2013).
Yamaguchi, J. et al. ALDH2 polymorphisms and bone mineral density in an elderly Japanese population. Osteoporosis International 17, 908–913 (2006).
Takeshima, K. et al. A missense single nucleotide polymorphism in the ALDH2gene, rs671, is associated with hip fracture. Scientific Reports 7 (2017).
Ilyar, S. DNA polymorphism and risk of esophageal squamous cell carcinoma in a population of North Xinjiang,China. World journal of gastroenterology 16, 641 (2010).
Chang, Y. C. et al. Common ALDH2 genetic variants predict development of hypertension in the SAPPHIRe prospective cohort: Gene-environmental interaction with alcohol consumption. BMC cardiovascular disorders 12, 58, https://doi.org/10.1186/1471-2261-12-58 (2012).
Tian et al. The genetic polymorphisms in ALDH2 influence the methadone dose and adverse reactions in patients with heroin addiction. Drug Metabolism Reviews 43, 26–26 (2011).
Haschemi Nassab, M. et al. No association between the ALDH2 promoter polymorphismrs886205, alcohol dependence, and risky alcohol consumption in a German population. Psychiatric genetics 25, 41–42, https://doi.org/10.1097/ypg.0000000000000073 (2015).
Dickson, P. A. et al. Effects of variation at the ALDH2 locus on alcohol metabolism, sensitivity, consumption, and dependence in Europeans. Alcoholism, clinical and experimental research 30, 1093–1100, https://doi.org/10.1111/j.1530-0277.2006.00128.x (2006).
Yang, H. et al. A novel polymorphism rs1329149 of CYP2E1 and a known polymorphism rs671 of ALDH2 of alcohol metabolizing enzymes are associated with colorectal cancer in a southwestern Chinese population. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 18, 2522–2527, https://doi.org/10.1158/1055-9965.epi-09-0398 (2009).
Zhang, S. et al. Polymorphisms in C-reactive protein and Glypican-5 are associated with lung cancer risk and Gartrokine-1 influences Cisplatin-based chemotherapy response in a Chinese Han population. Disease Markers 2015, 824304 (2015).
Xue, Y. et al. Genetic variant in ZFHX3 Geneon 16q22 associated with risk of stroke in Chinese Han population. International Journal of Clinical & Experimental Pathology 9, 8650–8656 (2016).
Du, Q. et al. SYNJ2 variant rs9365723 is associated with colorectal cancer risk in Chinese Han population. Int J Biol Markers 31, e138 (2016).
Acknowledgements
All of the participants provided written informed consent. The protocol was approved by the Clinical Research Ethics Boards of Xi’an Jiaotong University Hospital Medical College Red Cross Hospital, and complies with the Chinese Department of Health and Human Services regulations for the protection of human research subjects.
Author information
Authors and Affiliations
Contributions
D.H. conceived and supervised the project. SNP genotyping experiment was conducted by Q.D., K.Z. and D.L. Statistical Analyses was conducted by Q.D. and G.R. All the authors contributed to the discussion. Q.D. wrote the manuscript with help of D.H. and G.R.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dong, Q., Ren, G., Zhang, K. et al. Genetic polymorphisms of ALDH2 are associated with lumbar disc herniation in a Chinese Han population. Sci Rep 8, 13079 (2018). https://doi.org/10.1038/s41598-018-31491-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-31491-6
- Springer Nature Limited