
Abstract
NK cells are important in innate immunity for their capacity to kill infected or cancer cells. The killer cell immunoglobulin-like receptors (KIR) are a family of polymorphic genes with inhibitory and activating functions. The main driving force for gastric cancer (GC) development is a chronic response, which causes an increase of NK cells in the gastric mucosa. The aim of this work was to study polymorphisms in KIR genes in patients with either GC or non-atrophic gastritis (NAG). We studied 242 patients (130 with NAG and 112 with GC) and contrasted with 146 asymptomatic individuals. We analyzed diversity in the content and localization of KIR genes in the different clinical groups studied. Four activating and one inhibitory genes were associated with GC: 2DS1 (OR 3.41), 2DS3 (OR 4.66), 2DS5 (OR 2.25), 3DS1 (OR 3.35) and 2DL5 (OR 3.6). The following were also found as risk factors for GC: Bx genotype (OR 4.2), Bx-Bx centromere-telomere (OR 2.55), cA01|cB03 (OR 36.39) and tB01|tB01 (OR 7.55) gene content and three B motifs (OR 10.9). Polymorphisms in KIR genes were associated with GC and suggest that mutated NK cells may contribute to GC development by increasing gastric mucosa inflammation, leading to constant tissue damage.
Similar content being viewed by others


Introduction
NK cells represent a subset of lymphoid cells that are components of innate immunity acting as first line of defense against viral infection and other pathogens, and in the early cellular transformation and tumor surveillance1. The functions of NK cells are partly regulated by the family of KIR receptors (killer cell immunoglobulin-like receptor) coded by 11 genes (2DL1, 2DL2/2DL3, 2DL4, 2DL5, 2DS1, 2DS2, 2DS4, 2DS3/2DS5, 3DL1/3DS1, 3DL2 and 3DL3) and two pseudogenes (2DP1 and 3DP1) located on the chromosome 19q13.42,3,4. Some of these genes may present sequence variations; thus, it has been reported a 22 bp deletion in the second extracellular domain of 2DS4 that affect substantially the sequence of amino acids, whereas the exon 2 can be absent in 3DP15. Also, it has been found that 2DL5 gene is encoded by different loci (A and B)6. The KIR family is primarily expressed on NK cells, but they can also be expressed on CD4, CD8 and γδ T cells7,8,9. There are four promoter types based on intermediate promoters (ProI), which are associated with distinct expression in KIR genes, thus 2DL2, 2DS2 and 2DL3 are the first to be expressed by NK cells after Hemopoietic Stem Cell Transplantation10. The 3DL3 is not expressed by circulating CD56 dim NK cells, and 2DL4 is expressed by CD56-bright and dim NK cells in a non-variegated manner; and finally, the remaining KIR genes are expressed by CD56-dim NK cells10,11. T cells express 3DL2 more than other KIR genes, probably as a result of ProI activation earlier in the development of T cell10. In addition, the KIR gene family has bi-directional promoters, which control variegated expression, whereas ProI correlates with protein expression10.
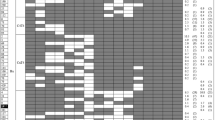
Composition of KIRs may be complex, thus, two haplotypes (A and B) and genotypes (AA and Bx, where x can be A or B) have been reported for KIR based on gene content12 (Fig. 1). Actually, there are over 500 different Bx genotypes (http://www.allelefrequencies.net). KIR genotype AA is homozygous for the A haplotype, which is an inhibitory haplotype formed by the loci 3DL3, 2DL3, 2DP1, 2DL1, 3DP1, 2DL4, 3DL1, 2DS4 and 3DL2; whereas Bx genotype has either one (AB heterozygous) or two (BB homozygous) B haplotypes, and is an activator haplotype (formed by 3DL3, 2DS2, 2DL2, 2DL5B, 2DS3/2DS5, 2DP1, 2DL1, 3DP1, 2DL4, 3DS1, 2DL5A, 2DS3/2DS5, 2DS1, 2DS4 and 3DL2 genes)13. The A haplotype usually has a fixed number of genes, while B has a variable gene content with additional activating KIR genes. KIR haplotypes consists of two regions, the centromeric region from 3DL3 to 3DP1, and the telomeric region from 2DL4 to 3DL2; and both regions can be cenA or cenB, and telA or telB depending on the haplotype13,14. 2DL5, 2DS3 and 2DS5 genes have been identified in centromeric and/or telomeric region14. Based on the gene content 9 centromeric regions (cA01, cA02, cA03, cB01, cB02, cB03, cB04, cB05 and cB06) and 8 telomeric regions (tA01, tB01, tB02, tB03, tB04, tB05, tB06 and tB07) have been described14,15,16,17. KIR B haplotype can also be classified according to B content genes, and B content score is calculated by adding the number of cenB and/or telB motifs in each genotype18.

Composition of KIR haplotypes (A and B) based on gene content. KIR genes are tightly organised head-to-tail over approximately 150 kb within the Leukocyte Receptor Complex (LCR). Inhibitory KIR genes are shown in white, activating genes in black and pseudogenes in gray.
Helicobacter pylori (H. pylori) infects the gastric mucosa of over 50% of the world population and represents the main risk factor to develop gastric cancer (GC) and duodenal ulcer19,20. Different immune cells are involved in the development of gastric pathologies by causing a chronic, unregulated mucosal inflammation21. Thus, cells of the innate and adaptive system such as T lymphocytes and natural killer (NK) cells have a critical role in the regulation of the immune response21. H. pylori causes an increase of NK cells in the gastric mucosa, where they produce TNF-α and INF-γ21,22,23, and have an important role in the inflammatory process that drive tissue damage. In this work we aimed to study polymorphisms in KIR receptors genes and identify any possible association with GC.
Results
The characteristics of the population studied are described in Table 1. We studied two groups of patients, one with a diagnosis of NAG and the other with GC, formed by 130 and 112 patients respectively, and both were compared with an asymptomatic group (n = 146). It can be observed that the NAG group showed significantly higher seroprevalence to H. pylori and to CagA, with an OR of 3.23 and 2.74, respectively, as compared to the asymptomatic patients.
KIR genes
In order to characterize the KIR genotype frequencies in the study groups, genomic DNA was isolated from peripheral blood leukocytes, and the KIR genes responsible for the activating signals (2DS1, 2DS2, 2DS3, 2DS4, 2DS5, 3DS1), the inhibitory signals (2DL1, 2DL2, 2DL3, 2DL4, 2DL5, 3DL1, 3DL2, 3DL3), and the two pseudogenes (2DP1 and 3DP1) were genotyped using single specific primer-polymerase chain reaction (SSP-PCR). KIR genotypes were assembled according to the presence or absence of each gene locus.
The frequency data obtained was analyzed between groups to determine differences in KIR genes between asymptomatic and disease groups. The framework genes of centromeric (3DL3 and 3DP1) and telomeric (2DL4 and 3DL2) regions were present in 100% of the three groups studied. The frequencies of 2DL1 (99.3%, 99.2% and 100%), 2DL3 (97.9%, 96.9% and 92.9%), 2DS4 (93.8%, 100% and 88.4%) and 2DP1 (99.3%, 99.2% and 100%) genes were not statistically different among the groups (Asymptomatic, NAG and GC, respectively). The KIR genes with a significant association with disease are shown in Table 2. When compared with healthy controls, most of the activating and inhibitory genes studied were found significantly associated with either NAG or GC, whereas some showed an increasing tendency of association from NAG to GC, like 2DS1 (OR of 2.56 to OR 5.45), 3DS1 (OR of 3.52 to OR 4.75) and 2DL5 (OR of 3.77 to OR 6.21). In contrast, 2DS3 presented a significantly decreasing tendency of association from NAG to GC, (OR of 187.7 to OR 24.98). 2DS2 and 2DL2 showed significant association with NAG (OR of 3.75 for the two genes), whereas 3DL1 was associated with protection for GC (OR 0.61). The above associations remained significant in a multivariate model of analyses (Table 3), where it can be observed that age was constantly associated with risk for GC, and H. pylori and gender for NAG. The multivariate analyses showed that 2DS1, 2DS3, 2DS5, 3DS1 and 2DL5 were found as risk for GC, whereas 3DL1 was found as protective (OR 0.21) (Table 3).
KIR haplotypes
In order to determine the association of genotypes with the disease groups, the genotypes were grouped as A or B based on gene content. We found that the genotype AA (inhibitory) was highly protective for NAG (OR 0.04, 95% CI 0.01–0.12) and GC (OR 0.22, 95% CI 0.08–0.57), whereas the genotype Bx (activator) was found as risk for both diseases (NAG OR 26.35, 95% CI 8.26–84.11; GC OR 4.57, 95% CI 1.74–12.0). Also, the results show that in our population the frequency of the genotype AA was close to 44%, while genotype Bx was 56%. The multivariate analyses confirmed the association with protection for genotype AA and with risk for genotype Bx (Table 4). As before, in this multivariate analyses gender was associated with NAG and age with GC.
Because the centromeric and telomeric regions have different gene content, genotypes AA and Bx were analyzed based on their distribution. Four different combinations of centromeric-telomeric (cAcA-tAtA, cAcA-tBx, cBx-tAtA and cBx-tBx) region of the genotypes were found. The cAcA-tAtA distribution was found significantly associated with protection (NAG OR 0.04, 95% CI 0.01–0.12; GC OR 0.22, 95% CI 0.08–0.57) and cBx-tBx with risk (NAG OR 10.65, 95% CI 4.84–23.44; GC OR 11.15, 95% CI 3.33–37.30) for both, NAG and GC. We noted that cAcA-tAtA was constant in asymptomatic population (43.8%), whereas cBx-tBx was more frequent in NAG (56.2%, vs 16.4% in asymptomatic and 33% in GC) and cAcA-tBx in GC (42.9%, vs 22.6% in asymptomatics and 33.1% in NAG). The multivariate analyses confirmed the association with protection for cAcA-tA-tA and with risk for cBx-tBx (Table 4).
KIR B score
The B content score analyses showed an association with protection of genotype AA for NAG (OR 0.04) and GC (OR 0.22) whereas the score 2 was associated with NAG (OR 9.7), and score 3 with GC (OR 78.7) (Table 5). The above associations were confirmed in a multivariate analysis (Table 6), and the risk of score 3 with GC remained as high (OR 10.9) as with age (OR 9.9).
KIR centromeric and telomeric distribucion
To further analyze the association of gene content of centromeric or telomeric regions with NAG and GC we studied the different combinations that have been reported. The multivariate analyses showed a strong association of risk for GC with cA01|cB03 (OR 36.3) and tB01|tB01 (OR 7.55), and of protection with tA01|tA01 (OR 0.23) (Table 7). The analysis also showed a strong risk for NAG with tA01|tB0X (OR 26.04) and high protection with tA01|tA01 (OR 0.08).
Discussion
In the present study, we showed the association of KIR receptors family genes with gastric pathologies. This association was observed with presence of genes, with genotypes, with centromere-telomere regions and with B score. Of particular interest, we observed that both activator and inhibitor genes were associated with GC. A balance between activator and inhibitor genes is necessary during immune surveillance by NK receptors; but when unregulated, their activity may contribute to pathogenesis of diverse diseases including tumor development24. We found that the presence of 2DS1, 2DS3 and 3DS1 activating genes was associated with risk for both, NAG and GC. In studies in other populations 2DS1 has also been found associated with cancer, although with breast cancer25, whereas 2DS1, 2DS3 and 3DS1 have been associated with more severe pulmonary tuberculosis in Asian population26; 2DS1 and 3DS1 with ankylosing spondylitis in Spain27, and 2DS2 with rheumatoid arthritis in Latin America28. In our population the activating 2DS5 gene was found associated with risk for GC, and of note, a recent meta-analysis concluded that 2DS5 was associated with risk for colorectal cancer29; these results would suggest that 2DS5 may be associated with cancers in the gastrointestinal tract.
Concerning the inhibitory genes, our results were contrasting; whereas 2DL5 was associated with risk for GC, 3DL1 showed association with protection. Interestingly, a study in Chinese population found that the expression of 3DL1 in NK cells was significantly increased in patients with gastric, pancreatic and colorectal cancer, but was not correlated with disease progression30. The inhibitory genes have also been reported associated with other immune and infectious diseases; 3DL1 in combination with the HLA-B*57 allele showed a protective effect against progression to AIDS in Zambian patients31, and 2DL2 was reported associated with rheumatoid arthritis28.
In our population Bx genotype was frequent and associated with both gastric diseases, although the risk was stronger for NAG than for GC. In our patients Bx genotypes were a combination of A and B haplotypes, with very few B homozygotes, which is in agreement with studies in other human populations in America, including Amerindian groups32. This high frequency of Bx genotype may have resulted from the selection by the infectious and chronic diseases that have been prevalent in our population for many generations; although this selection process may have caused an increased risk for GC in the region.
Our work shows eight KIR genes associated with gastric diseases, five of them were associated with risk for GC (2DS1, 2DS3, 2DS5, 3DS1, and 2DL5) and belong to B haplotype, which is an activator haplotype. This unexpected association might partially be explained by the pathogenesis of GC19, which main risk factor is an infection. H. pylori infection is strongly pro-inflammatory and invariably causes a chronic, decades-long inflammation of the gastric mucosa20. In the context of a decades-long mucosal inflammation, NK cells may be constantly and chronically recruited and activated; until in some patients the regulation of this activation might be lost.21 Unregulated NK cell may help to increase inflammation leading to mucosal damage and development of precancerous lesions and eventually to GC1,9,23,30. On the other hand, activating KIR haplotypes would have opposite effects on distinct malignancies depending on whether inflammation is or is not a major component of tumor pathogenesis33. Although, it should be noted that an activator haplotype could also be expected to be associated with increased ability to eliminate tumors1,34. In fact, it was reported that patients with metastatic colorectal cancer had complete response to FOLFIRI (5-fluorouracil, leucovorin and irinotecan) treatment when B haplotype was present35. Interestingly, there was a strong association between the KIR B haplotype and p53 alteration in Basal cell carcinoma tumors, with a higher likelihood that KIR B carriers harbor abnormal p5334.
Concerning the distribution of A and B, we observed that A was more frequent in centromere and telomere of asymptomatic healthy adults, whereas B was more common in both, NAG and GC. The multivariate analysis confirmed a highly significant association of cA01|cB03 with GC, in fact this association (OR 36.39) was over 3 times higher than the association with age (OR 10.65 for >50 years old), which was usually the strongest factor. In addition, whereas tB01|tB01 was also a significant risk factor for GC, tA01|tA01 showed a significant association with protection. To our knowledge, there is no report describing the analysis of gene content in centromere and telomere regions and gastric cancer. Our analysis also confirms that the telomeric part of the KIR B genotype may have a role in the development of gastric diseases, particularly the cluster of genes 2DS1, 2DS3, 2DS5, 3DS1 and 2DL5, which showed a risk association with GC. In contrast, genes 2DS2 and 2DL2 were found as risk for NAG; these genes are located in the centromeric region of B haplotype, and have been reported with high linkage disequilibrium16. Thus, in our population the telomeric region of KIR B was more associated with GC, and the centromeric region with NAG. Within the B haplotype the telomeric region is more diverse, and probably the observed association with GC is due to an unbalanced response by the NK cell and a reduced ability to kill cancer cells. In contrast, the centromeric region is more conserve and the response of the NK cell is probably more balanced and efficient to fight cancer.
In order to determine the participation of B motifs in GC, we evaluated the B score in centromere and telomere, and the multivariate analysis confirmed its importance in GC, showing a trend following the course of the disease. A B-score of zero was more frequent in asymptomatics and strongly protective for GC (OR 0.23), and a score of 2 was associated with NAG, whereas a score of 3 increased the risk for GC almost 11 times (OR of 10.9). These results suggest that the exacerbated function of the B haplotype contributes to the damage of the gastric mucosa, favoring the development of GC. The B-score was previously evaluated in patients with acute myelogenous leukemia, where patients receiving transplant from donors with a B-score of 2 or greater showed a better protection from relapses, and an increased disease-free survival18; which would suggest that the exacerbated function of B results in an efficient response against leukemia.
On the other hand, the A genotype was associated with protection for GC, although only the 3DL1 gene showed a significant protection. This gene is within the telomeric region of A genotype and probably the observed association could be due to the strong linkage disequilibrium that 3DL1 has with the other genes of the A genotype.
It was recently reported that tumor-infiltrating NK cells were decreased in human GC; moreover, the production of IFNγ and TNFα by these cells was impaired by tumor-associated monocytes/macrophages via TGFβ136. In contrast, patients with GC had a better survival when they presented higher concentrations of NK cells, an effect that was more evident in advanced stage cases37. Our work associates the risk to develop GC with the B KIR genotypes and the gene cluster included within the telomeric part. There is a need to better understand the functional role of the diversity in KIR genes content in GC, together with the participation of other factors involved in GC development, such as peptides derived from cancer that are presented by HLA class I molecules to KIR receptors34. Since HLA molecules are ligands of NK cells, they regulate the variation in immune responses to different antigens by selection and suppression/activation of NK cells, and have a relevant role in the combat against GC9,38. However, for the eight genes that presented association with NAG and GC in our study, only three ligands are known (2DS1-C2, 2DL2-C1 and C2, 3DL1-Bw4)38. In addition, it is known that B allotypes can influence the binding with 3DL1; thus, in the Bw4 dimorphic position 80, isoluecine (HLA-B*51-*53, *57, *58, HLA-A*24) generally exhibit stronger inhibition than threonine (HLA-B*13, B*27, B*37, B*44)33,39. Besides, 3DL1 and the other KIR genes associated with GC reported in this study are expressed by CD56-dim NK cells, which migrate to acute inflammatory sites and display a higher cytotoxic activity than CD56-bright cells40, and the B haplotype could also influence the cytotoxic activity on tumor cells. It is necessary to further study the role of HLA-Cw and KIR gene alleles in gastric cancer surveillance since receptor-ligand combinations are important in the regulation of NK cell responses38.
Although one limitation of our study is the sample size, we were still able to identify a strongly significant risk association of a gene cluster located in telomeric region of B genotype with GC. We should consider that GC is a multifactorial disease and consequently a multivariate analysis is necessary to better understand the importance of KIR gene variants in GC. We acknowledge that whereas our work present evidences of a significant association of KIR gene variants with gastric pathology, this association is not probe of causality and further studies are now needed to show that unregulated NK cells in the stomach mucosa may lead to gastric pathology. In conclusion, we found that 2DS1, 2DS3, 2DS5, 3DS1, 2DL5, Bx genotype, cBx-tBx, cA01|cB03, tA01|tB01, tB01|tB01 and B motifs were risk factors for GC. Mutated NK cells may contribute to GC development by increasing gastric mucosa inflammation, leading to constant tissue damage. The impact of the NK cell response on GC control might be determined in part by the genetic variation in KIR genes.
Materials and Methods
Study subjects
A total of 388 unrelated adults were recruited in this study, 146 healthy individuals (asymptomatic), 130 with non-atrophic gastritis (NAG) and 112 with GC. Patients with NAG were adults over 30 years old who were attended for symptoms at the gastroenterology service, whereas GC patients attended the oncology service for GC treatment; both groups attended the Instituto Mexicano del Seguro Social (IMSS) Medical Center in Mexico City. We selected NAG and GC patients without treatment of antibiotics, bismuth compounds, proton pump inhibitors and nonsteroidal anti-inflammatory drugs for at least two weeks prior to the study. GC patients without previous treatment for cancer were selected. Diagnosis was based on endoscopic examination and histopathology studies41. The individuals of the asymptomatic group were selected from healthy blood donors who attended the blood bank of the IMSS Medical Center, with an age over 30 years old and without any symptom or medication. To minimize the genomic diversity in different regions of the country of Mexico42,43,44,45, all groups of patients included in this study, patients and controls, received medical coverage from the same institute, IMSS at hospitals in the same city, Mexico City. Patients and controls were informed about the nature of the study and those willing to participate were asked to sign an informed consent letter. The study was approved by the ethics committee from the National Council for Research on Health, IMSS, Mexico and all procedures were performed in accordance with relevant guidelines and regulations.
Collection of samples
For the NAG patients seven gastric biopsies were taken and processed for histology to study the presence of precancerous lesions and H. pylori infection. Biopsies were collected from both the lesser and the greater curvature, four from antrum and three from corpus. Mucosal inflammation was graded according to the Karttunen classification46, and only patients without precancerous lesions were included. In the case of GC patients, a tissue sample from the tumor lesion and a sample from adjacent non-cancerous tissue was also obtained and the lesion was classified according to the Karttunen classification46. A sample of 5 ml of peripheral blood was drawn from each patient, and each healthy volunteer, and mononuclear cells were purified by centrifugation through a Ficoll-Hypaque density gradient. DNA was isolated from these cells using the salting-out microtechnique47 and frozen at −70 °C until genotyping. The serum fraction was frozen at −20°C until tested.
Definition of H. pylori infection
Serum samples were tested by ELISA to detect IgG antibodies against H. pylori whole-cell extract and against recombinant CagA protein, as previously described48. Infection was also diagnosed by histology in both antrum and corpus. The patient was considered infected with H. pylori when either tests, ELISA and/or histology, were positive, and non-infected when both tests were negative.
Genotyping of KIR
The presence of each KIR gene was used to define the KIR gene content of patients. KIR genes were tested using a commercial kit (Invitrogene, Brown Deer, Wisconsin, USA) based on the technique of single specific primer-polymerase chain reaction (SSP-PCR), which can identify 2DL1, 2DL2, 2DL3, 2DL4, 2DL5A, 2DL5B, 2DS1, 2DS2, 2DS3, 2DS4, 2DS5, 3DL1, 3DL2, 3DL3, 3DS1, 2DP1 and 3DP1 genes (including the variants of 2DS4 and 3DP1). PCR reaction and cycling conditions were according the instructions recommended by the manufacturer.
Statistical analysis
The gene, genotype, centromere-telomere gene content and B score frequencies in patients with NAG and GC were compared with the asymptomatic group. Chi-squared or Fisher’s exact test were used to test differences among groups, using the Epidat 3.1 Software; p values ≤ 0.05 were considered as significant49. The significance of association was assessed using odds ratios (OR) with confidence intervals (CI) of 95%50. OR values were corrected for gender and age using a logistic regression model. The analyses were performed using SPSS Statistics 22.0 (IBM SPSS Data Collection). The role of H. pylori, gender and age as variables influencing risk factor for GC was estimated in a multivariable logistic regression analysis.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding authors on reasonable request.
References
Vivier, E. et al. Innate or adaptive immunity? The example of natural killer cells. Science 331, 44–49, https://doi.org/10.1126/science.1198687 (2011).
Ordonez, D. et al. Duplication, mutation and recombination of the human orphan gene KIR2DS3 contribute to the diversity of KIR haplotypes. Genes Immun 9, 431–437, https://doi.org/10.1038/gene.2008.34 (2008).
Williams, F. et al. Multiple copies of KIR 3DL/S1 and KIR 2DL4 genes identified in a number of individuals. Hum Immunol 64, 729–732, https://doi.org/10.1016/S0198-8859(03)00089-2 (2003).
Wilson, M. J. et al. Plasticity in the organization and sequences of human KIR/ILT gene families. Proc Natl Acad Sci USA 97, 4778–4783, https://doi.org/10.1073/pnas.080588597 (2000).
Hsu, K. C. et al. Killer Ig-like receptor haplotype analysis by gene content: evidence for genomic diversity with a minimum of six basic framework haplotypes, each with multiple subsets. J Immunol 169, 5118–5129, https://doi.org/10.4049/jimmunol.169.9.5118 (2002).
Vilches, C., Gardiner, C. M. & Parham, P. Gene structure and promoter variation of expressed and nonexpressed variants of the KIR2DL5 gene. J Immunol 165, 6416–6421, https://doi.org/10.4049/jimmunol.165.11.6416 (2000).
McMahon, C. W. & Raulet, D. H. Expression and function of NK cell receptors in CD8+ T cells. Curr Opin Immunol 13, 465–470, https://doi.org/10.1016/S0952-7915(00)00242-9 (2001).
Remtoula, N., Bensussan, A. & Marie-Cardine, A. Cutting edge: selective expression of inhibitory or activating killer cell Ig-like receptors in circulating CD4+ T lymphocytes. J Immunol 180, 2767–2771, https://doi.org/10.4049/jimmunol.180.5.2767 (2008).
Thielens, A., Vivier, E. & Romagné, F. NK cell MHC class I specific receptors (KIR): from biology to clinical intervention. Curr Opin Immunol 24, 239–245, https://doi.org/10.1016/j.coi.2012.01.001 (2012).
Li, H., Wright, P. W., McCullen, M. & Anderson, S. K. Characterization of KIR intermediate promoters reveals four promoter types associated with distinct expression patterns of KIR subtypes. Genes Immun 17, 66–74, https://doi.org/10.1038/gene.2015.56 (2016).
Trompeter, H. I. et al. Three structurally and functionally divergent kinds of promoters regulate expression of clonally distributed killer cell Ig-like receptors (KIR), of KIR2DL4, and of KIR3DL3. J Immunol 174, 4135–4143, https://doi.org/10.4049/jimmunol.174.7.4135 (2005).
Uhrberg, M. The KIR gene family: life in the fast lane of evolution. Eur J Immunol 35, 10–15, https://doi.org/10.1002/eji.200425743 (2005).
Middleton, D. & Gonzelez, F. The extensive polymorphism of KIR genes. Immunology 129, 8–19, https://doi.org/10.1111/j.1365-2567.2009.03208.x (2010).
Jiang, W. et al. Copy number variation leads to considerable diversity for B but not A haplotypes of the human KIR genes encoding NK cell receptors. Genome Res 22, 1845–1854, https://doi.org/10.1101/gr.137976.112 (2012).
Hou, L., Chen, M., Ng, J. & Hurley, C. K. Conserved KIR allele-level haplotypes are altered by microvariation in individuals with European ancestry. Genes Immun 13, 47–58, https://doi.org/10.1038/gene.2011.52 (2012).
Pyo, C. W. et al. Different patterns of evolution in the centromeric and telomeric regions of group A and B haplotypes of the human killer cell Ig-like receptor locus. PLoS One 5, e15115, https://doi.org/10.1371/journal.pone.0015115 (2010).
Vierra-Green, C. et al. Allele-level haplotype frequencies and pairwise linkage disequilibrium for 14 KIR loci in 506 European-American individuals. PLoS One 7, e47491, https://doi.org/10.1371/journal.pone.0047491 (2012).
Cooley, S. et al. Donor selection for natural killer cell receptor genes leads to superior survival after unrelated transplantation for acute myelogenous leukemia. Blood 116, 2411–2419, https://doi.org/10.1182/blood-2010-05-283051 (2010).
Ang, T. L. & Fock, K. M. Clinical epidemiology of gastric cancer. Singapore Med J 55, 621–628, https://doi.org/10.11622/smedj.2014174 (2014).
Torres, J. et al. A Comprehensive Review of the Natural History of Helicobacter pylori Infection in Children. Archives of Medical Research 31, 431–469, https://doi.org/10.1016/S0188-4409(00)00099-0 (2000).
Hafsi, N. et al. Human dendritic cells respond to Helicobacter pylori, promoting NK cell and Th1-effector responses in vitro. J Immunol 173, 1249–1257, https://doi.org/10.4049/jimmunol.173.2.1249 (2004).
Agnihotri, N. et al. Characterization of lymphocytic subsets and cytokine production in gastric biopsy samples from Helicobacter pylori patients. Scand J Gastroenterol 33, 704–709, https://doi.org/10.1080/00365529850171639 (1998).
Tarkkanen, J., Kosunen, T. U. & Saksela, E. Contact of lymphocytes with Helicobacter pylori augments natural killer cell activity and induces production of gamma interferon. Infect Immun 61, 3012–3016 (1993).
Beziat, V., Hilton, H. G., Norman, P. J. & Traherne, J. A. Deciphering the killer-cell immunoglobulin-like receptor system at super-resolution for natural killer and T-cell biology. Immunology 150, 248–264, https://doi.org/10.1111/imm.12684 (2017).
Ozturk, O. G., Gun, F. D. & Polat, G. Killer cell immunoglobulin-like receptor genes in patients with breast cancer. Med Oncol 29, 511–515, https://doi.org/10.1007/s12032-011-9932-x (2012).
Lu, C. et al. Association of killer cell immunoglobulin-like receptors with pulmonary tuberculosis in Chinese Han. Genet Mol Res 11, 1370–1378, https://doi.org/10.4238/2012.May.15.7 (2012).
Diaz-Pena, R. et al. Activating killer immunoglobulin-like receptors genes are associated with increased susceptibility to ankylosing spondylitis. Clin Exp Immunol 180, 201–206, https://doi.org/10.1111/cei.12568 (2015).
Ramirez-De los Santos, S. et al. Associations of killer cell immunoglobulin- like receptor genes with rheumatoid arthritis. Dis Markers 33, 201–206, https://doi.org/10.3233/DMA-2012-0927 (2012).
Ghanadi, K., Shayanrad, B., Ahmadi, S. A., Shahsavar, F. & Eliasy, H. Colorectal cancer and the KIR genes in the human genome: A meta-analysis. Genom Data 10, 118–126, https://doi.org/10.1016/j.gdata.2016.10.010 (2016).
Peng, Y. P. et al. Comprehensive analysis of the percentage of surface receptors and cytotoxic granules positive natural killer cells in patients with pancreatic cancer, gastric cancer, and colorectal cancer. J Transl Med 11, 262, https://doi.org/10.1186/1479-5876-11-262 (2013).
Lopez-Vazquez, A. et al. Interaction between KIR3DL1 and HLA-B*57 supertype alleles influences the progression of HIV-1 infection in a Zambian population. Hum Immunol 66, 285–289, https://doi.org/10.1016/j.humimm.2005.01.001 (2005).
Flores, A. C. et al. KIR genes polymorphism in Argentinean Caucasoid and Amerindian populations. Tissue Antigens 69, 568–576, https://doi.org/10.1111/j.1399-0039.2007.00824.x (2007).
Kulkarni, S., Martin, M. P. & Carrington, M. The Yin and Yang of HLA and KIR in human disease. Semin Immunol 20, 343–352, https://doi.org/10.1016/j.smim.2008.06.003 (2008).
Vineretsky, K. A. et al. Skin Cancer Risk Is Modified by KIR/HLA Interactions That Influence the Activation of Natural Killer Immune Cells. Cancer Res 76, 370–376, https://doi.org/10.1158/0008-5472.CAN-15-0547 (2016).
De R, V. et al. Genetic diversity of the KIR/HLA system and outcome of patients with metastatic colorectal cancer treated with chemotherapy. PLoS One 9, e84940, https://doi.org/10.1371/journal.pone.0084940 (2014).
Peng, L. S. et al. Tumor-Associated Monocytes/Macrophages Impair NK-Cell Function via TGFbeta1 in Human Gastric Cancer. Cancer Immunol Res 5, 248–256, https://doi.org/10.1158/2326-6066.CIR-16-0152 (2017).
Rosso, D. et al. Correlation of natural killer cells with the prognosis of gastric adenocarcinoma. Arq Bras Cir Dig 25, 114–117, https://doi.org/10.1590/S0102-67202012000200011 (2012).
Ivarsson, M. A., Michaelsson, J. & Fauriat, C. Activating killer cell Ig-like receptors in health and disease. Front Immunol 5, 184, https://doi.org/10.3389/fimmu.2014.00184 (2014).
Carr, W. H., Pando, M. J. & Parham, P. KIR3DL1 polymorphisms that affect NK cell inhibition by HLA-Bw4 ligand. J Immunol 175, 5222–5229, https://doi.org/10.4049/jimmunol.175.8.5222 (2005).
Poli, A. et al. CD56bright natural killer (NK) cells: an important NK cell subset. Immunology 126, 458–465, https://doi.org/10.1111/j.1365-2567.2008.03027.x (2009).
Rugge, M. et al. Gastric mucosal atrophy: interobserver consistency using new criteria for classification and grading. Aliment Pharmacol Ther 16, 1249–1259, https://doi.org/10.1046/j.1365-2036.2002.01301.x (2002).
Alvarado-Hernández, D. L., Hernández-Ramírez, D., Noyola, D. E. & García-Sepúlveda, C. A. KIR gene diversity in Mexican mestizos of San Luis Potosí. Immunogenetics 63, 561–575, https://doi.org/10.1007/s00251-011-0540-x (2011).
Gutiérrez-Rodríguez, M. E. et al. KIR Gene in Ethnic and Mestizo Populations from Mexico. Immunogenetics 67, 85–93, https://doi.org/10.1016/j.humimm.2005.11.007 (2006).
Contreras, G. et al. Distribution of the killer cell immunoglobulin-like receptors in Mexican Mestizos. Tissue Antigens 69, 125–129, https://doi.org/10.1111/j.1399-0039.2006.76212.x (2007).
Machado-Sulbaran, A. C. et al. Distribution of KIR genes and KIR2DS4 gene variants in two Mexican Mestizo populations. Human Immunology 78, 614–620, https://doi.org/10.1016/j.humimm.2017.07.010 (2017).
Genta, R. M. In Surgical Pathology of the GI tract, liver, biliary tract and pancreas (eds Odze, R. D. Goldblum, J. R. & Crawford J. M.) Ch. 8, 169 (Saunders, 2004).
Miller, S. A., Dykes, D. D. & Polesky, H. F. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acid Research 16, 1215 (1988).
Camorlinga-Ponce, M. et al. Validation of a serologic test for the diagnosis of Helicobacter pylori infection and the immune response to urease and CagA in children. Am J Gastroenterol 93, 1264–1270, https://doi.org/10.1111/j.1572-0241.1998.00407.x (1998).
Hervada Vidal, X. et al. Epidat 3.0 programa para analisis epidemiológico de datos tabulados. Rev Esp Salud Publica 78, 277–280 (2004).
Petrie, A. & Sabin, C. Medical statistics at a glance. First edn, 78–79 (Blackwell Science Ltd, 2000).
Acknowledgements
The study was supported by Coordinacion Nacional de Investigacion en Salud, IMSS, México, grants FIS/IMSS/PROT/PRIO/13/027 and FIS/IMSS/PROT/130; and the Consejo Nacional de Ciencia y Tecnologia (Fronteras de la Ciencia grant 773), México.
Author information
Authors and Affiliations
Contributions
E.G.H. performed K.I.R. genotyping. O.P.R., M.N.R. and I.R.V. participated in the sample collection. O.P.R. and M.C.P. performed seroprevalence of H. pylori. J.T. conceived and participated in design and coordination and provided helpful discussions and helped to edit the manuscript. M.P.R. conceived and participated in statistical analysis, and in design and coordination and edited the manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hernandez, E., Partida-Rodriguez, O., Camorlinga-Ponce, M. et al. Genotype B of Killer Cell Immunoglobulin-Like Receptor is Related with Gastric Cancer Lesions. Sci Rep 8, 6104 (2018). https://doi.org/10.1038/s41598-018-24464-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-24464-2
- Springer Nature Limited
This article is cited by
-
Comparative genetics of KIR haplotype diversity in humans and rhesus macaques: the balancing act
Immunogenetics (2022)
-
Association of killer cell immunoglobulin-like receptors with endemic Burkitt lymphoma in Kenyan children
Scientific Reports (2021)
-
Coexistence of inhibitory and activating killer-cell immunoglobulin-like receptors to the same cognate HLA-C2 and Bw4 ligands confer breast cancer risk
Scientific Reports (2021)
-
Diversity of KIRs in invasive breast cancer patients and healthy controls along with the clinical significance in ER/PR/HER2+ patients
Genes & Immunity (2020)