
Abstract
There is emerging evidence that microRNAs (miRNAs) dysregulation is involved in the genesis and the progression of Prostate Cancer (PCa), thus potentially increasing their use in urological clinical practice. This is the first pilot study which utilizes Illumina Deep Sequencing to examine the entire miRNAs spectrum existent in urine exfoliated prostate cells (UEPCs) of PCa patients. A total of 11 male patients with histological diagnosis of PCa were enrolled in the present study. First-catch urine (30 mL) was collected following a prostate massage. Total RNA was extracted from urine and sequenced using an HiSeq2500 System (Illumina). QPCR assay was used to validate the highest NGS results in PCA patients and in age-matched, caucasian men. Remarkably, PCA let-7 family was down-regulated (P < 0.01), compared to the controls. The results of our study support the notion of a relatively high diagnostic value of miRNA family for PCa detection, especially in the let-7 family. The present research confirmed the potential use of miRNAs as non-invasive biomarkers in the diagnosis of PCa, potentially reducing the invasiveness of actual clinical strategy.
Similar content being viewed by others


Introduction
With the introduction of serum Prostate-Specific Antigen (PSA) test, the incidence of PCa has increased, leading to an increased number of unnecessary biopsies and the diagnosis of clinically insignificant tumors that were not life threatening. PSA has several limitations because of its well-known non-cancer specificity, with raising levels for many other urological conditions such as infections, inflammation or benign prostatic hyperplasia, resulting in high false-positive rates1. Prostate biopsy is currently the only way to definitively identify the presence of PCa following anomalous PSA and/or DRE2. One of the problems of prostate biopsy is the hitch in tissue sampling follow-on a sensitivity insufficiency (false negatives). Additionally, it should be underlined that prostate biopsy is not only a highly invasive diagnostic tool, but even that patients may suffer from several complications, such as infection, potentially leading to discomfort until up to one month after the procedure3. However, prostate biopsy constitutes the gold standard for prostate cancer diagnosis and is the starting point for preoperative pathologic grading and cancer volume estimation. The introduction of multiparametric Magnetic Resonance Imaging (mp-MRI) has improved PCa detection rate, allowing the execution of fusion MRI/ultrasound prostate biopsy. Histological grading which predicts prognosis and helps guide the therapy method is the Gleason score (GS).
It has been universally accepted that one of the main goals in PCa diagnosis and treatment is to detect cancer at an early stage, and to predict which patients will harbor intermediate and high-risk cancer, and thus initiate immediate medical treatment4. If diagnosed at an early stage, PCa can be successfully treated with different therapeutic strategies, such as active surveillance, hence delaying or avoiding radical treatment. Rapid and growing advances in whole genome sequencing allows to focus on molecular marker tracking as well as coding and non-coding RNA, revealing different sensitivity and specificity for PCa detection in urine5,6. Notably, non-coding RNA biomarkers are microRNAs (miRNAs) that constitute an evolutionarily conserved class of small RNA molecules. MiRNAs comprise one of the more abundant classes of gene regulatory molecules in multicellular organisms and likely influence the output of many protein-coding genes. MiRNAs regulate post-transcriptional gene-expression mainly by binding to the 3′ untranslated region (UTR) of their target messenger RNA (mRNA)7 resulting in protein synthesis inhibition8,9. MiRNAs play a fundamental role in the regulation of biological functions10,11, and there is an emerging evidence that their dysregulation is involved in the genesis and the progression of PCa.
The first human microRNA ever identified, lethal-7 (let-7), is known to be intimately involved in the division and differentiation of stem cells. It has been observed that the expression of let-7 family members is downregulated in many cancer types during tumor progression promoting cell cycle progression. A number of studies revealed in cancer patients significant let-7 family downregulation in renal cell, lung, bladder, colon, gastric, hepatocellular, breast, uterine and ovarian cancer12.
It has been demonstrated that miRNAs are detectable in urine of PCa patients collected after DRE (digital rectal examination)13,14. As demonstrated in our last study quantitative real-time PCR (qPCR) miRNA analysis could be considered a non-invasive promising tool for diagnostic testing on PCa, and on its prognostic status15.
Rapid advancement in miRNAs profiling technologies has made it possible to study microRNAs expression profiles through Next Generation Sequencing (NGS), which provides several advantages respect to methodologies previously employed16. NGS showed the largest dynamic range of detection and the greatest detection sensitivity17,18; representing a unique tool to investigate the transcriptome complexity at an incredibly high level of resolution19.
In our study, the primary research aim was to examine the entire miRNome profiling of UEPCs in PCa patients after DRE, by the NGS approach. Consequently, the highest predicted selection of miRNAs was validated by using qPCR analysis and compared with age-matched healthy control subjects.
Material and Methods
Patient selection
Eleven patients with clinical diagnosis of PCa and ages ranging from 51 to 68 years were included in NGS study. In qPCR assay 11 healthy control age-matched caucasian subjects (C) were enrolled, in addition to NGS patients. All samples (PCa and C) were collected for clinical diagnostic tests, after the prostatic massage, at the Hospital of Santa Maria della Misericordia (Perugia, Italy) in the department of Urological, Andrological and Minimally Invasive Techniques. Collection of patient samples has been performed according to national legislation concerning ethical requirements. Use of these samples has been approved by medical ethics committee on 7th February 2013 (protocol n. 2012-11 047R) and the CEAS Committee of Umbria Region on 21 February 2013 (CEAS Register n° 12 2085/13). Written informed consents were obtained from all study subjects and the samples were analyzed anonymously. This research is a retrospective study using archival sample. All oncological patients had a biopsy-proven diagnosis of PCa and underwent robotic radical prostatectomy within 1 month from clinical evaluation. Before biopsy, all patients underwent mp-MRI allowing us to perform a cognitive fusion biopsy technique, with at least 14 cores (median:18, ranging from 16 to 22). All control patients were enrolled after exclusion of any pathological urological conditions. Exclusion criteria were age >75 years, the presence of any other cancer type, bladder urinary lithiasis, urinary infection, previous therapy concerning prostate, as any endoscopic procedures or pharmacological treatment with 5-aromatase inhibitors or alpha-lithics, and presence of family history of PCa. Clinical parameters of subjects enrolled in the study are provided in Table 1.
Urine collection and total RNA extraction
First-catch urine (roughly 30 mL) was collected after the prostatic massage, as previously described by Lewis et al.20. The samples were collected using Urine Preservative (Norgen, Biotek Corp, Ontario, Canada), which is designed for the preservation of nucleic acids and proteins in fresh urine samples at room temperature. Urine was centrifuged at 650 g × 5 min. Once the supernatant was discarded, the urine sediment was washed twice with phosphate-buffered saline (PBS) and RNA extraction was performed using Urine Exfoliated Cell and Bacteria RNA Purification Kit (Norgen, Biotek Corp, Ontario, Canada) slightly modifying manufacturers’ instructions. To remove genomic DNA, all the samples were treated with RNase-free DNase I according to the manufacturer’s protocol (Norgen, Biotek Corp, Ontario, Canada). RNA concentration was assessed using the Qubit RNA assay (ThermoFisher Scientific, Kandel, Germany) and it was stored at −80 °C until further investigation.
Small RNA sequencing
Indexed libraries of PCa patients were prepared from purified RNA (25 ng) with SMARTer® smRNA-Seq Kit for Sample Prep Kit (Clontech Laboratories, Mountain View, CA, USA) according to manufacturer’s instructions. Libraries were quantified using the Tape Station 4200 (Agilent Technologies, Santa Clara, CA, USA) and pooled to obtain an index-tagged sample present in equimolar amounts, with a final concentration of the pooled samples of 2 nM. The pooled samples were subject to cluster generation and sequencing using an Illumina HiSeq2500 System (Illumina, San Diego, CA, USA) in a 1 × 50 single read format with a final concentration of 10 pM.
Data processing miRNA sequencing
The raw sequences file generated underwent quality control analysis using FASTQC (http://www.bioinformatics.babraham.ac.uk/projects/fastqc/). Before aligning sequences to a reference genome, the sequencing adaptors (Illumina), which were used in the sequencing library preparation, were trimmed using sRNAtoolbox. In order to generate sRNAbench sequence alignments, sRNAtoolbox was used. The alignment was performed setting the following parameters: seed length for alignment = 20, minimum read-count = 2, bowtie-alignment type = n, allowed number of mismatch = 0, minimum read length = 15 and maximum number of multiple mappings = 10. MiRNAs expression among the several samples was normalized to Read per Million (RPM) value, as computed by sRNAbench. Heat maps of expressed miRNAs were generated using tMev version 4.9 on RPM normalized values.
Prediction of miRNA targets and functional analysis of target genes
Computationally predicted mRNA targets of the top-62 miRNAs were identified using “microRNA Target Filter” of Ingenuity Pathway Analysis (IPA); considering TarBase mRNA target21. We performed a Gene Ontology (GO) and pathways analysis in order to investigate the relationships between these genes and PCa. IPA “Core Analysis” was used and only statistically significant data was considered (FDR ≤ 0.05, Benjamini-Hochberg for “Biological Function” and P ≤ 0.05 for pathways analysis).
Let-7 family qPCR in PCa and in age-matched healthy control subjects
The urine samples were collected using Urine Preservative (Norgen, Biotek Corp, Ontario, Canada) and Urine Exfoliated Cell and Bacteria RNA Purification Kit (Norgen, Biotek Corp, Ontario, Canada) was used to isolate RNA in 11 healthy subjects (control). After extraction, RNA was subjected to qualitative assessment through Bioanalyzer and NanoDrop. Total RNA was quantified by Qubit RNA Assay (ThermoFisher Scientific, Kandel, Germany) and stored at −80 °C until use. RNA used for 11 PCa patients previously extracted for library purified preparation (as previously described). Purified RNA (10 ng) derived from C and PCa subjects was reverse-transcribed using cDNA Universal cDNA Synthesis Kit II (Exiqon, Vedbæk, Denmark), according to manufacturer’s protocol. RNA spike-in control (0.5 µL) was introduced in 10 µL total volume of the retrotranscription mix before incubation as positive cDNA synthesis control (UniSp6, provided with cDNA synthesis kit). The procedure was optimized to maximize signal and minimize effects of inhibitors as recommended by Instruction Manual for miRCURY LNA™ Universal RT microRNA PCR.
QPCR amplification was carried out using 4 µL of cDNA (diluted 1:20), 5 µL of ExiLENT SYBR® Green master mix (Exiqon, Vedbæk, Denmark) and 1 µL of miRCURY LNA specific PCR primer (Exiqon, Vedbæk, Denmark) in a final volume of 10 μL according to manufacturer’s recommendations.
The following microRNA LNA™ PCR primers (Exiqon, Vedbæk, Denmark) were used for qPCR: hsa-let-7a-5p (Exiqon product number 205727), hsa-let-7b-5p (204750), hsa-let-7c-5p (204767), hsa-let-7d-5p (204124), hsa-let-7e-5p (205711), hsa-let-7f-5p (204359), hsa-let-7g-5p (204565) and hsa-let-7i-5p (204394).
All quantitative PCR values were normalized to has-miR-191 (Exiqon product number 204306) reference gene, in accordance with previously published paper14. Thermo-cycling conditions on iCycler iQ Real-Time PCR (Bio-Rad, Hercules, CA) consisted of an initial denaturation of 10 min at 95 °C, followed by 45 cycles of 15 s at 95 °C for denaturing double stranded DNA and 1 min at 60 °C for annealing/extension steps. Melting curves were plotted at the end of each cycle series to assess amplification specificity, through the verification of the presence of one-gene specific peak and the absence of primer dimers. Three biological replicates were used for the qPCR to verify the expression level of miRNAs and no template controls (NTC) were included in the analysis. For each sample, LNA control primer set was used to amplify UniSp4 and UniSp6 spike-in positive control. Bio-Rad software plotted the fluorescence intensity against the number of cycles providing cycle threshold (Ct) value using the automatic method.
To normalize expression value of target miRNAs, 2-ΔCt method was used (ΔCt = Ct target miRNA - Ct has-miR-191)22,23.
Statistical analysis of Let-7 family qPCR data
RT-qPCR technical replicates were averaged and only samples with a standard error lower than 0.2 Ct were maintained. The dataset normality was tested by Shapiro-Wilks test and a P ≤ 0.05 was considered statistical significant. T-test for independent samples was used. Statistical analysis was carried out with R software.
Results
RNA quality and quantity
Mean RNA integrity number (RIN) was 8.7 (range 8.3–9.0) and 260/280 ratio was 1.84 (range 1.84–2.03), indicating the high purity of RNA preparation in every sample. In healthy men RNA yield was approximately 10 ng/µL (0.5 µg RNA/30 mL urine) and 50 ng/µL (2.5 µg RNA/30 mL urine) in PCa subjects.
NGS of PCa miRNA
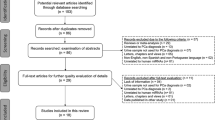
MiRNA profile was examined using Illumina small RNA sequencing. For all PCa samples, in average 20071425 raw reads were obtained. After trimming the adapter sequence and removing those with low quality, we obtained, in average, 11275265 reads and of these, about 60% can be mapped to the human genome (hg19) with high confidence (Fig. 1). MiRNA was considered expressed when detected, in at least one sample, with a RPM normalized expression value ≥ the first quantile of expression distribution. Applying this statistical cut-off, we identified 236 miRNAs as shown in supplemental table.

Sequencing results. Deep sequencing results overview showing the average number of raw reads, filtered reads and mapped reads obtained in the small-RNA sequencing experiment. Filtered and mapped reads were analyzed using sRNABench bioinformatics tool.
Gene ontology analysis and Pathway analysis of the predicted miRNA target genes
To predict mRNA targets and biological pathways, we selected the top-62 expressed miRNAs including let-7 family validated by qPCR assay.
Functional analysis was performed with Core Analysis and revealed that most top-62 were involved in cancer, cellular development, cellular growth and proliferation and cell death and cell survival (FDR ≤ 0.05, Benjamini-Hochberg) (Fig. 2). Interestingly, among the several pathways statistically enriched (P ≤ 0.05, Fisher’s test), some genes were involved in Prostate Cancer Signaling, especially Ras, P ten and Cyclin D1 (Fig. 3).

List of diseases and functions of miRNAs target. Bar-chart showing the 19 Gene ontologies found to be most highly statistically enriched in response to PCa urine cells miRNAs (FDR ≤ 0.05 Benjamini-Hochberg). MiRNA targets were computed using “microRNA Target Filter” of Ingenuity Pathway Analysis, taking in consideration only validated mRNAs target listed in TarBase.

List of statistically enriched pathways of miRNAs target. Bar-chart showing the statistically enriched pathways (P ≤ 0.05, Fisher’s test) where the mRNAs target of miRNAs are involved. Pathways analysis was performed using “Core Analysis” function of Ingenuity Pathway Analysis software.
QPCR validation of let-7 family
To validate the activities of PCa miRNAs predicted by NGS we selected let-7 family. Let-7 family were amplified by qPCR in age-matched healthy control and PCa subjects. Let-7 family miRNA panel was chosen for the potential promising diagnostic and therapeutic role in PCa. In fact, results showed that PCa let-7 family was down-regulated (P ≤ 0.0001) compared to healthy controls, as shown in Fig. 4.

MiRNA expression levels. Normalized expression value (2-ΔCt) of let-7 family miRNAs in post-DRE urine sediments from PCa (left) and controls subjects. The solid symbols show the observed subjects and the bar indicate the mean of observations. The 2-ΔCt method was used to calculate the miRNAs normalized expression as follows: 2-(Ct target miRNA - Ct miR-191).
Discussion
Given the indolent nature of localized low-grade PCa, its over detection has led to overtreatment in many affected men. The identification of molecular biomarkers has been researched thoroughly in order to identify PCa early and robustly. De facto, PSA-based screening is limited in that a non-trascurable amount of high-risk cancer will not be detectable. Since 1997 the European Randomised Study of Screening for Prostate Cancer (ERSPC) set the PSA > 3 ng/mL as an indication to prostate biopsy overlooking other imaging or clinical aspects6,24,25,26,27,28,29.
The widespread diffusion of mpMRI has changed the diagnostic paradigm of localized PCa. This imaging modality has a high sensitivity and high negative predictive value for the aggressive disease30. To improve PCa detection rate, biopsy of the suspicious area should be performed after mp-MRI of the prostate, even using a simple cognitive fusion technique, based on the observation and localization of prostatic lesions on the MRI image. At least 12 cores should be taken in each patient, in consideration of multifocal entity of PCa31.
The development of a panel of biomarkers could be helpful in diagnostic and prognostic accuracy. The number of potential biomarkers in PCa will rise in the next years. In particular, miRNAs are object of intense study5,32,33, as they can be extracted from a wide range of biological samples and are highly stable in various storage conditions34. In this study, we investigated UEPC miRNA expression levels using NGS technology to identify the entire miRNome in PCa patients. Subsequently, we compared levels of the highest selected PCa miRNAs with those in age-matched healthy control subjects. The main advantages of UEPC collection is a non-invasive and relatively fast and cost-efficient procedure compared with other clinical samples18. Due to the anatomic proximity of the prostate gland to the urethra, detection of biomarkers may be found in urine. In particular, when the sample is enriched with prostate cells after performing a prostate massage35. Urine after DRE is the only biological matrix containing prostate cancer-derived cells, furthermore, this non-invasive sampling permits repeated procedures and follow-up monitoring.
The first study on altered miRNAs in PCa began in 2007 and aimed to identify a specific panel by systematically profiling prostate cancer cell lines36. Since then, several authors proposed different miRNA profiles, using different approaches37. To the best of our knowledge, this research is among the first to utilize NGS Illumina Deep Sequencing to examine the entire spectrum of miRNAs from UEPCs. The key advantage of small RNA sequencing is the identification of low miRNA abundance and the successful detection of novel miRNAs without a priori knowledge of sequences9.
Through the NGS approach we performed the GO analysis of top-60 miRNAs, allowing us an enrichment analysis by comparing top-60 miRNAs to all available biological pathways. Our study provides additional evidence that top-60 miRNAs are involved in Prostate Cancer Signaling, in particular, through the modulation of Ras, P ten and Cyclin D1 genes. One suggested function of Pten in the nucleus is to induce G1 cell cycle arrest partially by the reduction of Cyclin D1 levels through its protein phosphatase activity38 or through controlling MAPK signaling39. Recent research using NGS suggests Ras/MAPK as a potential driver in human prostate cancer pathogenesis and progression40,41. We have validated let-7 family among all miRNAs for their potential promising therapeutic role in PCa. It showed the highest AVG Expression RPM and in one of our previous papers15, demonstrated that let-7 family was able to discriminate in serum patients with PCa from those harboring BPH when both presented altered PSA levels (3 ng/mL)15.
Originally, the let-7 family was discovered as a crucial gene in Caenorhabditis elegans and, later, as one of the first miRNAs42. Even if several characteristics of let-7 family are conserved across species, there are some remarkable differences between the let-7 family genes in C. elegans and orthologous genes in more complex organisms. For instance, in humans, thirteen let-7 family precursor miRNAs were described and coded 10 different mature let-7 miRNAs isoform43. Although the role of this miRNA family is not fully understood, its aberrant expression is associated with cancer44,45.
The results obtained in our previous research15 are in accordance with our findings. In conclusion, our results lead us to hypothesize that the profile of let-7 family in UEPC could really become new, easily accessible, affordable, non-invasive, and promising testing tool for the personalized management of patients with PCa. Probably, during the next few years, the circulating let-7 expression analysis may be a useful tool to predict the therapeutic outcomes of patients’ response to specific disease states and oligonucleotide antagonists therapy with let-7 miRNA-inhibitor will become available to determine the therapeutic future of this potentially very powerful technology.
References
Dall’Era, M. A. et al. Active surveillance for prostate cancer: a systematic review of the literature. Eur. Urol. 62, 976–983 (2012).
Xu, W. & Zhou, M. A concise update on prostate pathology. Českoslov. Patol. 50, 120–128 (2014).
Loeb, S. et al. Systematic review of complications of prostate biopsy. Eur. Urol. 64, 876–892 (2013).
Wittmann, J. & Jäck, H.-M. Serum microRNAs as powerful cancer biomarkers. Biochim. Biophys. Acta 1806, 200–207 (2010).
Fabris, L. et al. The Potential of MicroRNAs as Prostate Cancer Biomarkers. Eur. Urol. 70, 312–322 (2016).
Van Neste, L. et al. Detection of High-grade Prostate Cancer Using a Urinary Molecular Biomarker-Based Risk Score. Eur. Urol. https://doi.org/10.1016/j.eururo.2016.04.012 (2016).
Ambros, V. The functions of animal microRNAs. Nature 431, 350–355 (2004).
Giraldez, A. J. et al. Zebrafish MiR-430 promotes deadenylation and clearance of maternal mRNAs. Science 312, 75–79 (2006).
Song, C. et al. Expression profile analysis of microRNAs in prostate cancer by next-generation sequencing. The Prostate 75, 500–516 (2015).
Inui, M., Martello, G. & Piccolo, S. MicroRNA control of signal transduction. Nat. Rev. Mol. Cell Biol. 11, 252–263 (2010).
Fang, Y.-X. & Gao, W.-Q. Roles of microRNAs during prostatic tumorigenesis and tumor progression. Oncogene 33, 135–147 (2014).
Masood, N. & Yasmin, A. Entangling Relation of Micro RNA-let7, miRNA-200 and miRNA-125 with Various Cancers. Pathol. Oncol. Res. POR 23, 707–715 (2017).
Egidi, M. G. et al. Characterization of Kallireins and microRNAs in Urine Sediment for the Discrimination of Prostate Cancer from Benign Prostatic Hyperplasia. J. Cancer Sci. Ther. 7 (2015).
Egidi, M. G. et al. Stability Assessment of Candidate Reference Genes in Urine Sediment of Prostate Cancer Patients for miRNA Applications. Dis. Markers 2015, e973597 (2015).
Cochetti, G. et al. Different levels of serum microRNAs in prostate cancer and benign prostatic hyperplasia: evaluation of potential diagnostic and prognostic role. OncoTargets Ther. 9, 7545–7553 (2016).
Creighton, C. J., Reid, J. G. & Gunaratne, P. H. Expression profiling of microRNAs by deep sequencing. Brief. Bioinform. 10, 490–497 (2009).
Tam, S., de Borja, R., Tsao, M.-S. & McPherson, J. D. Robust global microRNA expression profiling using next-generation sequencing technologies. Lab. Investig. J. Tech. Methods Pathol. 94, 350–358 (2014).
Matullo, G., Naccarati, A. & Pardini, B. MicroRNA expression profiling in bladder cancer: the challenge of next-generation sequencing in tissues and biofluids. Int. J. Cancer 138, 2334–2345 (2016).
Mestdagh, P. et al. Evaluation of quantitative miRNA expression platforms in the microRNA quality control (miRQC) study. Nat. Methods 11, 809–815 (2014).
Lewis, H. et al. miR-888 is an expressed prostatic secretions-derived microRNA that promotes prostate cell growth and migration. Cell Cycle Georget. Tex 13, 227–239 (2014).
Sethupathy, P., Corda, B. & Hatzigeorgiou, A. G. TarBase: A comprehensive database of experimentally supported animal microRNA targets. RNA N. Y. N 12, 192–197 (2006).
Schmittgen, T. D. & Livak, K. J. Analyzing real-time PCR data by the comparative C(T) method. Nat. Protoc. 3, 1101–1108 (2008).
Livak, K. J. & Schmittgen, T. D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods San Diego Calif 25, 402–408 (2001).
Bill-Axelson, A. et al. Radical prostatectomy or watchful waiting in early prostate cancer. N. Engl. J. Med. 370, 932–942 (2014).
Schröder, F. H., Raaijmakers, R., Postma, R., van der Kwast, T. H. & Roobol, M. J. 4-year prostate specific antigen progression and diagnosis of prostate cancer in the European Randomized Study of Screening for Prostate Cancer, section Rotterdam. J. Urol. 174, 489–494; discussion 493–494 (2005).
Postma, R. & Schröder, F. H. Screening for prostate cancer. Eur. J. Cancer Oxf. Engl. 1990(41), 825–833 (2005).
Postma, R. et al. Incidence and follow-up of patients with focal prostate carcinoma in 2 screening rounds after an interval of 4 years. Cancer 103, 708–716 (2005).
Catalona, W. J. Screening for prostate cancer. Lancet Lond. Engl. 343, 1437 (1994).
Catalona, W. J. et al. Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J. Urol. 151, 1283–1290 (1994).
Fütterer, J. J. et al. Can Clinically Significant Prostate Cancer Be Detected with Multiparametric Magnetic Resonance Imaging? A Systematic Review of the Literature. Eur. Urol. 68, 1045–1053 (2015).
Fandella, A. et al. Italian Prostate Biopsies Group: 2016 Updated Guidelines Insights. Anticancer Res. 37, 413–424 (2017).
Catto, J. W. F. et al. MicroRNA in prostate, bladder, and kidney cancer: a systematic review. Eur. Urol. 59, 671–681 (2011).
Ferro, M. et al. Biomarkers in localized prostate cancer. Future Oncol. Lond. Engl. 12, 399–411 (2016).
Chen, X. et al. Characterization of microRNAs in serum: a novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 18, 997–1006 (2008).
Filella, X. & Foj, L. Prostate Cancer Detection and Prognosis: From Prostate Specific Antigen (PSA) to Exosomal Biomarkers. Int. J. Mol. Sci. 17 (2016).
Porkka, K. P. et al. MicroRNA expression profiling in prostate cancer. Cancer Res. 67, 6130–6135 (2007).
Bertoli, G., Cava, C. & Castiglioni, I. MicroRNAs as Biomarkers for Diagnosis, Prognosis and Theranostics in Prostate Cancer. Int. J. Mol. Sci. 17, 421 (2016).
Weng, L. P., Brown, J. L. & Eng, C. PTEN coordinates G(1) arrest by down-regulating cyclin D1 via its protein phosphatase activity and up-regulating p27 via its lipid phosphatase activity in a breast cancer model. Hum. Mol. Genet. 10, 599–604 (2001).
Chung, J.-H. et al. The ERK1/2 pathway modulates nuclear PTEN-mediated cell cycle arrest by cyclin D1 transcriptional regulation. Hum. Mol. Genet. 15, 2553–2559 (2006).
Bakin, R. E., Gioeli, D., Sikes, R. A., Bissonette, E. A. & Weber, M. J. Constitutive activation of the Ras/mitogen-activated protein kinase signaling pathway promotes androgen hypersensitivity in LNCaP prostate cancer cells. Cancer Res. 63, 1981–1989 (2003).
Colombatti, M. et al. The prostate specific membrane antigen regulates the expression of IL-6 and CCL5 in prostate tumour cells by activating the MAPK pathways. PloS One 4, e4608 (2009).
Reinhart, B. J. et al. The 21-nucleotide let-7 RNA regulates developmental timing in Caenorhabditis elegans. Nature 403, 901–906 (2000).
Roush, S. & Slack, F. J. The let-7 family of microRNAs. Trends Cell Biol. 18, 505–516 (2008).
Johnson, C. D. et al. The let-7 microRNA represses cell proliferation pathways in human cells. Cancer Res. 67, 7713–7722 (2007).
Boyerinas, B., Park, S.-M., Hau, A., Murmann, A. E. & Peter, M. E. The role of let-7 in cell differentiation and cancer. Endocr. Relat. Cancer 17, F19–36 (2010).
Acknowledgements
The authors would like to thank Gabriel Falcinelli and Anna Beatrice Casano for their skillful technical assistance and Diana Cella for improving the use of English in the manuscript.
Author information
Authors and Affiliations
Contributions
G.G., D.Z., and G.C.’A made substantial contributions to conception and design; acquisition of data was undertaken by G.G., V.S., S.D., A.B. and E.M.; data analysis and interpretation was undertaken by G.G., V.S. and A.B.’A; the manuscript was drafted by G.G., V.S. and G.C., and all authors critically revised the manuscript for important intellectual content. G.G. and D.Z. performed the statistical analysis and EM obtained funding. Administrative, technical or material support was provided by G.G. and A.B., while G.C., A.B. and E.M. provided supervision.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guelfi, G., Cochetti, G., Stefanetti, V. et al. Next Generation Sequencing of urine exfoliated cells: an approach of prostate cancer microRNAs research. Sci Rep 8, 7111 (2018). https://doi.org/10.1038/s41598-018-24236-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-24236-y
- Springer Nature Limited
This article is cited by
-
miR-939, as an important regulator in various cancers pathogenesis, has diagnostic, prognostic, and therapeutic values: a review
Journal of the Egyptian National Cancer Institute (2024)
-
Novel insights on perils and promises of miRNA in understanding colon cancer metastasis and progression
Medical Oncology (2023)
-
The relationship between microRNAs and bladder cancer: are microRNAs useful to predict bladder cancer in suspicious patients?
International Urology and Nephrology (2023)
-
CircLRP6 contributes to prostate cancer growth and metastasis by binding to miR-330-5p to up-regulate NRBP1
World Journal of Surgical Oncology (2021)
-
Bladder mesenchymal stromal cell-derived exosomal miRNA-217 modulates bladder cancer cell survival through Hippo-YAP pathway
Inflammation Research (2021)