

Abstract
Fetal growth restriction (FGR) is the major single cause of stillbirth1 and is also associated with neonatal morbidity and mortality2,3, impaired health and educational achievement in childhood4,5 and with a range of diseases in later life6. Effective screening and intervention for FGR is an unmet clinical need. Here, we performed ultrahigh performance liquid chromatography–tandem mass spectroscopy (UPLC–MS/MS) metabolomics on maternal serum at 12, 20 and 28 weeks of gestational age (wkGA) using 175 cases of term FGR and 299 controls from the Pregnancy Outcome Prediction (POP) study, conducted in Cambridge, UK, to identify predictive metabolites. Internal validation using 36 wkGA samples demonstrated that a ratio of the products of the relative concentrations of two positively associated metabolites (1-(1-enyl-stearoyl)-2-oleoyl-GPC (P-18:0/18:1) and 1,5-anhydroglucitol) to the product of the relative concentrations of two negatively associated metabolites (5α-androstan-3α,17α-diol disulfate and N1,N12-diacetylspermine) predicted FGR at term. The ratio had approximately double the discrimination as compared to a previously developed angiogenic biomarker7, the soluble fms-like tyrosine kinase 1:placental growth factor (sFLT1:PlGF) ratio (AUC 0.78 versus 0.64, P = 0.0001). We validated the predictive performance of the metabolite ratio in two sub-samples of a demographically dissimilar cohort, Born in Bradford (BiB), conducted in Bradford, UK (P = 0.0002). Screening and intervention using this metabolite ratio in conjunction with ultrasonic imaging at around 36 wkGA could plausibly prevent adverse events through enhanced fetal monitoring and targeted induction of labor.


Similar content being viewed by others
Data availability
Source data for Figs. 1,2 and Extended Data Figs. 2,5,6,7 are available online. As the individual patient data contain confidential information, it can be supplied only in an anonymized format to suitably qualified researchers who can make appropriate institutional commitments relating to data security and confidentiality. Data requests should be addressed to U.S. or G.C.S.S.
References
Gardosi, J., Madurasinghe, V., Williams, M., Malik, A. & Francis, A. Maternal and fetal risk factors for stillbirth: population based study. BMJ 346, f108 (2013).
Chauhan, S. P. et al. Neonatal morbidity of small- and large-for-gestational-age neonates born at term in uncomplicated pregnancies. Obstet. Gynecol. 130, 511–519 (2017).
Moraitis, A. A., Wood, A. M., Fleming, M. & Smith, G. C. S. Birth weight percentile and the risk of term perinatal death. Obstet.Gynecol. 124, 274–283 (2014).
MacKay, D. F., Smith, G. C., Dobbie, R. & Pell, J. P. Gestational age at delivery and special educational need: retrospective cohort study of 407,503 schoolchildren. PLoS Med. 7, e1000289 (2010).
Källén, B., Finnström, O., Nygren, K.-G. & Otterblad Olausson, P. Association between preterm birth and intrauterine growth retardation and child asthma. Eur. Respir. J. 41, 671–676 (2013).
Barker, D. J. Adult consequences of fetal growth restriction. Clin. Obstet. Gynecol 49, 270–283 (2006).
Gaccioli, F. et al. Screening for fetal growth restriction using ultrasound and the sFLT1/PlGF ratio in nulliparous women: a prospective cohort study. Lancet Child Adolesc Health 2, 569–581 (2018).
Reddy, U. M. et al. Prepregnancy risk factors for antepartum stillbirth in the United States. Obstet. Gynecol. 116, 1119–1126 (2010).
Monier, I. et al. Poor effectiveness of antenatal detection of fetal growth restriction and consequences for obstetric management and neonatal outcomes: a French national study. BJOG 122, 518–527 (2015).
Bricker, L., Medley, N. & Pratt, J. J. Routine ultrasound in late pregnancy (after 24 weeks’ gestation). Cochrane Database Syst. Rev. 6, CD001451 (2015).
Royal College of Obstetricians & Gynaecologists The investigation and management of the small for gestational age fetus (Green-top Guideline No. 31). (RCOG, 2013). .
Smith, G. C. Researching new methods of screening for adverse pregnancy outcome: lessons from pre-eclampsia. PLoS Med. 9, e1001274 (2012).
Spong, C. Y. Defining “term” pregnancy: recommendations from the Defining “Term” Pregnancy Workgroup. JAMA 309, 2445–2446 (2013).
MacDonald, T. M., McCarthy, E. A. & Walker, S. P. Shining light in dark corners: diagnosis and management of late-onset fetal growth restriction. Aust. N. Z. J. Obstet. Gynaecol. 55, 3–10 (2015).
Sovio, U., White, I. R., Dacey, A., Pasupathy, D. & Smith, G.C.S. Screening for fetal growth restriction with universal third trimester ultrasonography in nulliparous women in the Pregnancy Outcome Prediction (POP) study: a prospective cohort study. Lancet 386, 2089–2097 (2015).
Gong, S. et al. Placental polyamine metabolism differs by fetal sex, fetal growth restriction, and preeclampsia. JCI Insight 13, e120723 (2018).
Sharp, S. J., Poulaliou, M., Thompson, S. G., White, I. R. & Wood, A. M. A review of published analyses of case-cohort studies and recommendations for future reporting. PLoS One 9, e101176 (2014).
Zeisler, H. et al. Predictive value of the sFlt-1:PlGF ratio in women with suspected preeclampsia. N. Engl. J. Med. 374, 13–22 (2016).
Delaney, S. S., Coley, R. Y. & Brown, Z. 1,5-Anhydroglucitol: a new predictor of neonatal birth weight in diabetic pregnancies. Eur. J. Obstet. Gynecol. Reprod. Biol. 189, 55–58 (2015).
Eriksson, H., Gustafsson, J. A. & Sjovall, J. Excretion of steroid hormones in adults. C19 and C21 steroids in faeces from pregnant women. Eur. J. Biochem. 12, 520–526 (1970).
Tanaka, T., Suguro, N. & Kubodera, A. A simple radioimmunoassay for estriol 3-sulfate in pregnancy plasma without deconjugation. Steroids 46, 649–657 (1985).
Kunz, J. & Keller, P. J. Ultrasound and biochemical findings in intrauterine growth retardation. J. Perinat. Med. 4, 85–94 (1976).
Raeside, J. I. A brief account of the discovery of the fetal/placental unit for estrogen production in equine and human pregnancies: relation to human medicine. Yale J. Biol. Med. 90, 449–461 (2017).
Brien, M., Berthiaume, L., Rudkowska, I., Julien, P. & Bilodeau, J. F. Placental dimethyl acetal fatty acid derivatives are elevated in preeclampsia. Placenta 51, 82–88 (2017).
Brosens, I., Pijnenborg, R., Vercruysse, L. & Romero, R. The “Great Obstetrical Syndromes” are associated with disorders of deep placentation. Am. J. Obstet. Gynecol. 204, 193–201 (2011).
Mifsud, W. & Sebire, N. J. Placental pathology in early-onset and late-onset fetal growth restriction. Fetal Diagn. Ther. 36, 117–128 (2014).
Neveux, L. M., Palomaki, G. E., Larrivee, D. A., Knight, G. J. & Haddow, J. E. Refinements in managing maternal weight adjustment for interpreting prenatal screening results. Prenat. Diagn. 16, 1115–1119 (1996).
Sorensen, S., Momsen, G., Sundberg, K., Friis-Hansen, L. & Jorgensen, F. S. First-trimester risk calculation for trisomy 13, 18, and 21: comparison of the screening efficiency between 2 locally developed programs and commercial software. Clin. Chem. 57, 1023–1031 (2011).
Pasupathy, D. et al. Study protocol. A prospective cohort study of unselected primiparous women: the pregnancy outcome prediction study. BMC Pregnancy Childbirth 8, 51 (2008).
Gaccioli, F., Lager, S., Sovio, U., Charnock-Jones, D. S. & Smith, G. C. S. The pregnancy outcome prediction (POP) study: investigating the relationship between serial prenatal ultrasonography, biomarkers, placental phenotype and adverse pregnancy outcomes. Placenta. 59, S17–S25 (2017).
Sovio, U. et al. 4-Hydroxyglutamate is a novel predictor of pre-eclampsia. Int. J. Epidemiol. https://doi.org/10.1093/ije/dyz098 (2010).
Gardosi, J., Mongelli, M., Wilcox, M. & Chang, A. An adjustable fetal weight standard. Ultrasound Obstet. Gynecol. 6, 168–174 (1995).
Raynor, P. & Born in Bradford Collaborative Group. Born in Bradford, a cohort study of babies born in Bradford, and their parents: protocol for the recruitment phase. BMC Public Health 8, 327 (2008).
Wright, J. et al. Cohort profile: the Born in Bradford multi-ethnic family cohort study. Int. J. Epidemiol. 42, 978–991 (2013).
Hadlock, F. P., Harrist, R. B. & Martinez-Poyer, J. In utero analysis of fetal growth: a sonographic weight standard. Radiology 181, 129–133 (1991).
Sovio, U. et al. Prediction of preeclampsia using the soluble fms-like tyrosine kinase 1 to placental growth factor ratio: a prospective cohort study of unselected nulliparous women. Hypertension 69, 731–738 (2017).
Evans, A. M., DeHaven, C. D., Barrett, T., Mitchell, M. & Milgram, E. Integrated, nontargeted ultrahigh performance liquid chromatography/electrospray ionization tandem mass spectrometry platform for the identification and relative quantification of the small-molecule complement of biological systems. Anal. Chem. 81, 6656–6667 (2009).
Acknowledgements
The work was supported by the National Institute for Health Research (NIHR) Cambridge Biomedical Research Centre (Women’s Health theme), the Medical Research Council (MRC) (G1100221 to G.C.S.S. and D.S.C.-J. and MR/N024397/1 to D.A.L.), the Wellcome Trust (WT101597MA), National Institutes of Health (R01 DK10324), the European Research Council (669545), and the NIHR Biomedical Centre at the University Hospitals Bristol NHS Foundation Trust and the University of Bristol (Reproductive and Perinatal Health theme), which funds N.M.’s PhD studentship. N.G., N.M. and D.A.L. work in a unit that receives support from the MRC (MC_UU_00011/6) and University of Bristol. The funders did not have any role in the design, analysis or preparation of the manuscript for publication. We are grateful to the participants in the POP and BiB studies and staff who recruited and assessed these participants. We thank L. Bibby, S. Ranawaka, K. Holmes, J. Gill and R. Millar for technical assistance.
Author information
Authors and Affiliations
Contributions
G.C.S.S. had the original idea. G.C.S.S., D.S.C.-J. and D.A.L. designed the experiments. U.S. and G.C.S.S. conceived the analysis. N.G., N.M. and U.S. conducted the analysis. E.C., F.G. and D.S.C.-J. conducted the laboratory work. U.S. and G.C.S.S. drafted the initial version of the manuscript. All authors have seen and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
Direct: Cambridge Enterprise (UK) have filed a patent relating to the associations described in this paper with U.S., D.S.C.-J. and G.C.S.S. as the named inventors. Indirect: G.C.S.S. reports research support in kind from GE Healthcare and Roche, and financial support of research from GlaxoSmithKline (GSK) and Sera Prognostics. G.C.S.S. has been paid to attend advisory boards by GSK and Roche. G.C.S.S. has acted as a paid consultant to GSK and is a member of a Data Safety and Monitoring Committee for a GSK vaccine trial. D.A.L. has received support in kind from Roche Diagnostics and Medtronic Ltd.
Additional information
Peer review information Michael Basson was the primary editor on this article and managed its editorial process and peer review in collaboration with the rest of the editorial team.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Flow diagram of the selection of cases and controls using a case-cohort design in the POP study cohort.
One of the six women who did not have any blood samples available for analysis had FGR at term. POP, Pregnancy Outcome Prediction; wkGA, weeks of gestational age; FGR, fetal growth restriction; BW, birth weight, ACGVD1, abdominal circumference growth velocity in the lowest decile.
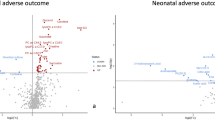
Extended Data Fig. 2 Distribution of P values from the composite Chi-squared test (two-sided) for the measurements at 20/28 wkGA.
The P values of 829 metabolites with a known structural identity were calculated from the test for interaction between term FGR and gestational age. The analysis included metabolite measurements from 175 FGR cases and 299 controls. wkGA, weeks of gestational age; FGR, fetal growth restriction.
Extended Data Fig. 3 Flow diagram of the selection of cases and controls in the first BiB study sample.
The sample selection was performed to provide a subsample of 1,000 women suitable for multi-omics assessment. Hence, only women with GWAS and DNA samples suitable for DNA methylation analyses at the time of selection were included. BiB, Born in Bradford; GWAS, genome-wide association study; FGR, fetal growth restriction.
Extended Data Fig. 4 Flow diagram of the selection of cases and controls in the second BiB study sample.
The selection of 2,000 women was performed using a case-cohort design. BiB, Born in Bradford; GWAS, genome-wide association study; HDP, hypertensive disorders of pregnancy; FGR, fetal growth restriction.
Extended Data Fig. 5 Sensitivity and false positive rate across 100 cutoff points of EFW and metabolite ratio at 36wkGA in relation to delivery of an infant with FGR at term.
There were 160 FGR cases and 273 controls in the analysis. Both EFW and the metabolite ratio were expressed as percentiles. In a, the first cutoff point was EFW <1st and metabolite ratio >99th. The remaining cutoff points were defined by progressively increasing the EFW threshold by 1 and decreasing the metabolite threshold by 1 (that is EFW <ith and metabolite ratio >100-ith percentile, i=1, …, 99). The cutoff point corresponding to the combination of EFW<20th and metabolite ratio >80th percentile is marked on the graph. The screening statistics (95%CI) for this combination were positive LR 10.8 (6.4 to 18.4), negative LR 0.47 (0.39–0.56), sensitivity 55.6% (47.8%–63.2%), specificity 94.9% (91.5%–96.9%), PPV 33.1% (21.8%–46.7%), NPV 97.9% (97.3%–98.4%), and DOR 23.2 (12.6–41.6). In b, the cutoff points were EFW <ith and/or metabolite ratio >100-ith percentile, i=1, …, 99. The cutoff point corresponding to EFW<20th and/or metabolite ratio >80th percentile is marked on the graph. The screening statistics (95%CI) for this were positive LR 2.5 (2.2 to 2.9), negative LR 0.07 (0.03–0.15), sensitivity 95.6% (91.0%–97.9%), specificity 61.9% (56.0%–67.5%), PPV 10.3% (8.2%–12.8%), NPV 99.7% (99.3%–99.9%), and DOR 35.5 (16.3–77.3). EFW, estimated fetal weight; wkGA, weeks of gestational age; FGR, fetal growth restriction; LR, likelihood ratio; PPV, positive predictive value; NPV, negative predictive value; DOR, diagnostic odds ratio.
Extended Data Fig. 6 Odds ratios (95% confidence intervals) of metabolite measurements at ~24–28 wkGA in relation to subsequent FGR (defined as birth weight <3rd percentile corrected only for GA and fetal sex) in the POP study and the BiB study samples 1 and 2.
Odds ratios are given for one standard deviation increase in the log-transformed metabolite ratio. The POP study included 136 FGR cases and 294 controls, the BiB 1 study included 20 FGR cases and 950 controls, and the BiB 2 study included 41 cases and 1513 controls. wkGA, weeks of gestational age; FGR, fetal growth restriction; SGA, small for gestational age; 1-(1-enyl-stear)-2-o-GPC, 1-(1-enyl-stearoyl)-2-oleoyl-GPC (P-18:0/18:1); 1,5-AG, 1,5-anhydroglucitol; 5α-androstan, 5α-androstan-3α,17α-diol disulfate; 4-androsten-3β2, 4-androsten-3β,17β-diol monosulfate (2); POP, Pregnancy Outcome Prediction; BiB, Born in Bradford.
Extended Data Fig. 7 Receiver operating characteristic (ROC) curve analysis of the metabolite ratio at 28wkGA comparing preterm FGR (n=32) and controls (n=305) in the POP study.
Area under the ROC curve (AUC) = 0.60 (95% CI: 0.48 to 0.72). For the null hypothesis of AUC=0.5, z test P=0.10 (two-sided). Preterm FGR was defined as delivery at <37wkGA with customized birth weight <10th percentile. FGR, fetal growth restriction; wkGA, weeks of gestational age; POP, Pregnancy Outcome Prediction.
Supplementary information
Supplementary Information
Supplementary Tables 1–10.
Source data
Source Data Fig. 1
Statistical Source Data
Source Data Fig. 2
Statistical Source Data
Source Data Extended Data Fig. 2
Statistical Source Data
Source Data Extended Data Fig. 5
Statistical Source Data
Source Data Extended Data Fig. 6
Statistical Source Data
Source Data Extended Data Fig. 7
Statistical Source Data
Rights and permissions
About this article

Cite this article
Sovio, U., Goulding, N., McBride, N. et al. A maternal serum metabolite ratio predicts fetal growth restriction at term. Nat Med 26, 348–353 (2020). https://doi.org/10.1038/s41591-020-0804-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-020-0804-9
- Springer Nature America, Inc.
This article is cited by
-
Metabolic dynamics and prediction of sFGR and adverse fetal outcomes: a prospective longitudinal cohort study
BMC Medicine (2023)
-
Small molecule metabolites: discovery of biomarkers and therapeutic targets
Signal Transduction and Targeted Therapy (2023)
-
Effect of common pregnancy and perinatal complications on offspring metabolic traits across the life course: a multi-cohort study
BMC Medicine (2023)
-
Associations of severe adverse perinatal outcomes among continuous birth weight percentiles on different birth weight charts: a secondary analysis of a cluster randomized trial
BMC Pregnancy and Childbirth (2022)
-
Gestational age-dependent development of the neonatal metabolome
Pediatric Research (2021)