
Abstract
A chronic Kidney Disease of unknown etiology (CKDu) has emerged with disproportionately high prevalence across dry lowland agricultural communities globally. Here we present the results of a prospective cohort of 293 patients with CKDu in the endemic region of Wilgamuwa, Sri Lanka, in whom we measured baseline kidney function and undertook quarterly follow up over 2 years. Well water was the primary historic drinking water source in the region, although a majority (68%) of participants reported switching to reverse osmosis water during study follow ups. Participants who reported ever drinking from well water had estimated glomerular filtration rates −6.7 (SD: 2.8) ml/min/1.73 m2 lower than participants who did not drink from well water historically (p = 0.0184) during the study period. Geospatial analysis identifies a cluster within the region where CKDu progression is significantly higher than the surrounding area. Samples of household wells (n = 262) indicated 68% had detectable agrochemical compounds with concentration above global water quality standards. It is expected that the detected contaminants compounds are indicators of poor water quality and that there is likely additional agrochemical exposure including commercial additives that may contribute to CKDu onset and/or progression. Thus, our study finds that well water exposure during a person’s lifetime in this region is associated with kidney function decline and identifies and quantifies putative nephrotoxic agrochemicals above safe drinking water concentrations in these wells.
Similar content being viewed by others

Introduction
The rising global death toll from chronic kidney disease (CKD), now the world’s 12th leading cause of death, is considered a downstream consequence of the growing global prevalence of diabetes (4.7% of adults in 1980 and 8.5% in 2014) and hypertension (31.1% among adults, 90% increase from 1975–2015)1,2. In the same period, however, there has been a rapid increase in a “non-traditional” type of CKD in rural lowland agricultural communities that is not associated with uncontrolled diabetes and hypertension, termed chronic kidney disease of “unknown etiology” (CKDu) in South Asia3, also known as Mesoamerican Nephropathy (MeN) in Central and South America4 and the Central Valley of California5. While a majority of CKD is characterized as a primarily glomerular disease3,4, CKDu is a tubulointerstitial disease with varying degrees of interstitial fibrosis, interstitial inflammation, and tubular atrophy3,5. Both types move inevitably toward kidney failure and death unless there is intervention through hemodialysis or a kidney transplant.
Sri Lanka is one of the world’s hot spots for CKDu with prevalence highest in the “dry zone”, North Central and Central Provinces6,7. In the post-world war-II (WWII) period, the emergence of the Green Revolution brought Sri Lanka and other low- and middle-income counties (LMICs) the promise of food self-sufficiency through high yield seeds, use of agrochemicals, reliable water sources, and increasing mechanization. The need for land and resources to implement the Green Revolution called for reestablishment of the irrigation system, known as the tank cascade irrigation systems developed in the fourth to sixth century (CE) and resettlement of farmers from the land-starved “wet zone” into the dry8,9. From the 1950s to the end of the 1980s, funding from the World Bank and other international agencies resulted in the development of one of the largest irrigation projects in the world, involving the damming of Sri Lanka’s major river, the Mahaweli, and the development of reservoirs, spillways, and channels throughout the dry zone areas10.
In the early 1990s, cases of kidney failure began to appear in health care facilities in the dry zone provinces, primarily among male and to a lesser extent among female farmers11. By the start of the new millennium, CKDu had become a major epidemic, especially for the poorest households, resulting in the loss of adult income earners, contributing to poverty, and increasing the cost of health care systems as a result of the expansion of hemodialysis and kidney transplant units. The current CKDu prevalence among 30- to 60-year-old men in dry zone districts is 15.1–22.9%6,7,11. The once valued occupation of farming has become stigmatized, contributing to the ill health, inability to work, and mortality of farmers12.
Review of PubMed peer-review publications indicates over 110 publications during the last decade primarily focused on a search for the etiology of CKDu in Sri Lanka using cross-sectional or case-control approaches. The inability to generate conclusive results has left researchers and public health officials with little to communicate to the population at risk. Tracking progression of kidney disease in dry zone residents with CKDu may offer an alternative, complementary approach to investigating etiology.
This paper examines the association between water source contamination and kidney function decline, drawing on data from the Kidney Progression Project (KiPP)13, a Sri Lanka-US collaboration of geochemists, anthropologists, and nephrologists, funded by the Fogarty International Center of the US National Institutes of Health. This transdisciplinary project explores the environmental, behavioral, and clinical factors associated with lower kidney function in a cohort of patients with established CKDu, generating data that allows us to examine the role of water consumption and kidney function.
Results
Demographics
Table 1 summarizes the demographics, water use, and clinical data at baseline. Consistent with the known clinical and demographic characteristics of CKDu, 74% of our participants were men and 96% had 1+ urine protein or less but had substantial reduction in kidney function, with mean eGFR 37.5 ml/min/1.73 m2. Over half (53%) had lived in Wilgamuwa from birth, 92% of participants had farmed during their lifetime, and 66% reported that they were still engaged in farming for an average of 33 lifetime years.
Drinking water sources
Historic drinking water source included well water for 89% of participants. All the wells in this study have been used as drinking water sources in the past. Water sources changed substantially during the study period. Figure 1 shows the water consumption patterns of participants over the KiPP study period, with a clear transition from the consumption of well water to RO water sources or other alternative sources. Supplemental Table 1a and Table 1b present demographic information stratified by baseline RO water use, versus not and by ever well water use versus not. A fewer proportion of participants with baseline RO water use were women, and a greater proportion owned farming land, compared with participants without baseline RO water use. Participants without any well water use were younger, and a greater proportion reported living in Wilgamuwa all their life.

Note the number of participants at each time point is specified as not all participants were available at each follow up.
GIS analysis
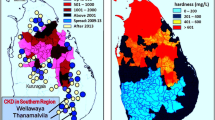
GIS analysis is summarized in Figs. 2 and 3. These identify key spatial trends including the spatial distribution of the baseline eGFR of the participants across the region (Fig. 2) and their rates of progression across the region. Figure 3 identifies two important clusters of low progression or improvement in the north–west region surrounding the medical clinic and a region just below this, also to the west where 24 participants have a significantly faster decline in eGFR relative to other participants. The average eGFR progression across the blue region is −1.2 ± w ml/min/1.73 m2/year and that of the relatively rapidly declining cluster (red region) is −2.1 ml/min/1.73 m2/year. Note, though both regions show decline in kidney function, this analysis identifies not the fastest rates of decline in the study, but rather individuals who are declining faster relative to their surrounding neighbors. It is also noteworthy that the blue region (slower CKDu progressors) is located at higher elevations in the drainage basin and upstream of the red regions (relatively faster CKDu progression) are located at lower elevations and downstream from the blue regions.

Also illustrated on the map are the locations of reverse osmosis (RO) plants which ration free drinking water to residents as of late 2017 and the location of the three regional clinics/hospitals.

The analysis also shows that participants in the uppermost north–west surrounding a medical clinic are performing significantly better (no progression or improvement) than surrounding regions.
Water quality
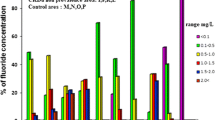
Domestic well water for every participant in the sample was tested for inorganic metals, target complex ions and targeted organic agrochemicals14. Of the 26 inorganic metals that were quantified, all were within recommended water quality thresholds (Shipley et al. 2022). Of the 272 sampled wells, 68% yielded positive detections of the target agrochemical compounds (Table 2). All wells with positive detections had concentrations of at least one agrochemical that exceeded global drinking water guidelines and 40% had at least two. The wells with positive detections showed no discernable spatial patterns (Shipley et al., 2022).
Table 3 shows the relationship between ever consuming well water and eGFR. Participants who reported using well water during their lifetime had lower age- and sex-adjusted eGFR (−6.7 ± 2.8 ml/min/1.73 m2/year) over the study period, compared with participants not using any well water (p = 0.0184). Current water use at the time of study initiation was not associated with eGFR during the study period and of the 68% of the wells with high compound concentrations, <10% were still being used for drinking water by the end of the study period.
Discussion
Analysis of well water has established contamination that can contribute to nephrotoxicity. Diazinon, and organophosphate insecticide, is the most frequently detected agrochemical in this study. It is reported to induce nephrotoxicity in rats through depletion of antioxidant enzymes15 and the study proposes that oxidative stress could be used as an early intervention that may be beneficial in monitoring diazinon toxicity. DDT and its longer-lived metabolite p,p'-DDE are organochlorine insecticides and proven nephrotoxins in rats where sub-acute treatment leads to oxidative stress and apoptosis, the proposed mechanism of DDT-induced nephrotoxicity16. Propanil is a chlorinated herbicide and it too has been identified as a nephrotoxin in in-vivo studies wherein a metabolite resulting from propanil oxidation is suspected to contribute to propanil cytotoxicity17. Endosulfan II (banned by the Stochkholm Convention in 2011 though still in use in Asia) is an organochlorine insecticide. When introduced orally to rats, endosulfan II induced pathological alterations in the kidney including chronic glomerulonephritis, glomerulosclerosis, adenoma, and glomerulus deposits18.
In addition to the agrochemicals, two other water quality parameters were high. These include water hardness, which has been weakly associated with incident kidney stones19,20 but not a feature of CKDu. Phosphate was higher than that recommended for drinking water samples based on US EPA standards in 80% of the wells. Though high dose phosphate preparations have been implicated in acute kidney dysfunction, kidney biopsy examinations of patients with CKDu have not supported this potential causative pathway21,22. To our knowledge, elevated phosphate levels have not been reported in other CKDu studies to date. Nonetheless, patients with CKD are at particular risk of further complications when exposed to high phosphate levels as the kidney’s ability to regulate phosphate homeostasis is compromised21.
While causation cannot be inferred from these results, there is strong evidence for concern about water contamination and CKDu both for the etiology of CKDu and the relative rapidity of progression. It is likely that there is no single compound of concern but rather a multiple stressor interactor effect across environmental and agrochemical exposure, behavior, and clinical factors. The detected compounds do show water contamination from nearby paddy agriculture and are indicators of numerous other possible substances that would be expected to be in the water including additives and uptake enhancers associated with the detected active compounds in commercial mixtures. In addition, since this is a single-time point analysis, prior exposure(s) to other compounds is likely, even among households in whose wells we did not detect compounds in the current study. As tube and dug wells are fed from aquifer systems, groundwater flow fields and direction are important considerations in local water quality, however, greater temporal sampling is required to examine this further.
GIS analysis has revealed a cluster of participants in the western region which are progressing significantly faster than the surrounding participants. This cluster occurs at low relative elevations for the region where upstream waters are collected and stagnate. The resolution of the well sampling is not temporally robust to compare the water quality across this cluster (only single water samples collected at each location across the region). Thus, future sampling should focus on the synoptic sampling of water in this region across all seasons relative to controls. GIS analysis has also revealed a cluster of relatively lower disease progression that may be associated with proximity to clinical care though clusters surrounding the remaining two clinics do not show this consistently. Alternatively, this may be related to the direction of water flow as this cluster occurs at a higher elevation and upstream in the region. Proximity to RO water is another possible indicator of less CKDu progression however this cannot be assessed at this time. The RO plants are relatively new (all installed in late 2017 and early 2018 and are managed by the Sri Lankan Navy, providing free rations to residents). The impact of these plants is too recent to be captured in this baseline study; however the population will continue to be monitored in an ongoing study and these results are a critical reference point.
This study has established a significant association between well water consumption and lower kidney function in patients with CKDu. The concern about drinking water contamination has led the Government of Sri Lanka to make a substantial investment in RO water and to explore alternatives for decontamination. While this approach may be effective in the short run, dependence on RO units with a limited running life is not a long-term solution. This study has strengths that include prospective data, that participants are randomly selected and representative of the affected CKDu population, and good geographic spread within the study area. Improvements for continuing efforts include increasing the limited sample size, to include the evaluation of a nearby non-endemic rice paddy community, and additional water quality parameters including microbial loads and associated toxins.
In summary, this study of a prospective cohort of patients with kidney disease living in Sri Lanka’s endemic CKDu region, study finds that well water exposure during a person’s lifetime is associated with kidney function decline and identifies and quantifies known nephrotoxins above safe drinking water concentrations in these well waters. Implementation of resettlement projects without providing basic life requirements such as safe drinking water, health care, education, sanitary facilities, and safety from hazards, both environmental and wildlife has led to serious implications to social and human health in these rural communities. Settlers initially suffered with water scarcity associated with epidemics of water-borne diseases, but later had to depend on whatever water was made available to them. Further, living areas are embedded within the farming areas exposing domestic water sources to agrochemicals used in farming in addition of groundwater contaminants. Agrochemical use in paddy and other agricultural practices that have characterized the last 70 years of the Green Revolution in Sri Lanka may now be contributing to ill health, rapid progression of disease, and mortality. Farming, traditionally a highly respected occupation and the well, part of the “wealth” of the household is now a source of danger and risk. We propose further comprehensive baseline evaluation, provision of basic life requirements and monitoring are essential in resettlements to avoid future health hazards. New approaches are needed to develop safe drinking water, while reducing the introduction of agrochemical contaminants in Sri Lanka and other tropical countries to reduce the growing prevalence of CKDu.
Methods
Kidney progression project
The Kidney Progression Project was initiated in 2017 in the Wilgamuwa Divisional Secretariat, a highly endemic CKDu area of 40,000 people in the lowland dry zone area of the Central Province (Supplementary Fig. 1). All protocols were reviewed and approved by review boards at the University of Connecticut in the US and National Hospital in Kandy, Sri Lanka. The detailed methodological approach including a description of behavioral and clinical and expanded environmental variables is described in Vlahos et al. (2018)13. Briefly, in 2016, the Ministry of Health conducted a screening of urine and blood in Wilgamuwa for residents 11 years and older to identify those with CKDu. Using the resulting serum creatinine values obtained during this screening effort, the KiPP team calculated CKD-EPI eGFR23, which resulted in a total of 330 people at Stage 3 and 4 of CKDu (eGFR in the range of 20-60 ml/min/1.73 m2), who did not have identifiable cause for CKD with evidence of chronic interstitial nephritis in renal biopsies or small echogenic kidney. Of these, 304 agreed to participate but ultimately 293 answered the baseline questionnaire and came for at least one serum creatinine measurement and were included in this analysis.
Baseline survey components
All participants were administered a baseline survey that focused on environmental exposure, behavioral and occupational factors, and clinical values as described in the KiPP protocol13. We probed water sources in detail. Water sources in the study area and the dry zone in general include household wells dug by hand that are 10 meters deep or shallower, tube wells dug to a depth of 20–30 m with drilling equipment, and lesser-used sources including surface water (tanks, channels and river water), rainwater collection, natural spring water, publicly supplied pipe water, and public water delivered to individual houses by truck (bowsers) and stored in large roof containers. The rise in CKDu cases led the government to invest heavily in reverse osmosis (RO) units and nanofiltration membrane technology for many dry zone villages14. These were installed at the end of 2017 and early 2018 to provide rationed, free drinking water.
Baseline water samples and analysis
The wells of each participant household were sampled once for target agrochemicals as described in Shipley et al.24. In all, 272 household wells were sampled with 31 households sharing wells.
Agrochemical analyses
Agrochemical analyses follow methods of Shipley et al., (2022)24 and EPA (2018)25. Briefly, 1 L well water samples were collected at each participant’s home and pre-filtered through a 0.45 µm nominal GFF to remove particulates. The sample was then extracted using 3 mL Chromabond C-18 SPE cartridges and a Supelco Visiprep SPE vacuum manifold. Three deuterated surrogate standards (chrysense d12, acenaphthene d10, and 1,4-dichlorobenzene d4) were loaded onto the cartridge before elution with 5 ml of acetonitrile and nitrogen reduction to 1 ml. Recoveries ranged from 70 to 101%.
An initial non-targeted analysis was run on samples in scan mode which identified over 100 compounds, including pyrolytic compounds that are likely the result of field burning practices in preparation for the new season. We supplemented these analyses with data from a local list of agrochemicals for the year 2017–2018 supplied by the Sri Lankan Ministry of Environment. Based on these data, targeted analyses were performed for 30 agrochemicals using selective ion mode.
Inorganic analyses
Phosphate in samples was measured with an Ion Chromatograph (Thermo Dionex ICS-1100). For repeated analyses of selected samples, an analytical precision better than ±5% of relative standard deviations was achieved. Total hardness was determined by EDTA titration method (APHA 2012)26.
Follow up: From December 2017 to the beginning of 2020, study participants had quarterly follow-up visits assessing behavioral changes including water consumption and serum creatinine testing. Serum creatinine was tested using an IDMS-calibrated enzymatic assay and converted to estimated glomerular filtration using the CKD-EPI equation.
GIS Analysis: Using GPS coordinates recorded by the field team for the domestic wells of each participant, individual eGFR at baseline and eGFR slopes over the study period were plotted over the ArcMap World Topographic map. For the baseline eGFR map, values were separated into five categories using Jenks Natural breaks provided by the ArcGIS software. The uppermost category was manually set to 65 mL/min/1.73 m2 and points with null or <15 mL/min/1.73 m2 are not displayed. Annual slopes were measured in mL/min/1.73 m2/year and integrated over the area covered by the eGFR points using the default settings of the Inverse Distance Weighted (Spatial Analysis) tool. Five categories were determined based on the severity of the increase or decrease. RO plants and hospitals were plotted using GPS data from the field team to convey proximity to clean water and health care across participants.
GIS analyses
Analysis was performed on the annual slopes using ArcGIS Hot Spot Analysis which uses Getis-Ord Gi*. This analysis identifies significant clusters of points which are higher or lower than expected relative to surrounding points on a two-dimensional grid. Default values for grouping neighbors were used which maximizes the probability that all points have included neighbors. Visualization was changed such that the points with particularly negative slopes (rapid progressors) were labeled in red to provide clarity as to the areas of greatest eGFR progression. Blue points indicate places where slopes are significantly higher (less negative (slow progressors) or even positive (improvers)).
Statistical analysis
Baseline characteristics are described using mean (SD) and n (proportion) as appropriate. In order to test the hypothesis that drinking water exposure was associated with eGFR decline, we used liner mixed models (LMM) accounting for age, sex and time points following Boucquemont et al. (2014)27. The major advantage of LMMs is that they do not require equally spaced time intervals between patient follow ups (consecutive measurements), nor the same number of measurements per patient. LMM therefore uses all available information in the analysis, including participants who may have fewer (even one) follow up-visits. In our study, the response variable was eGFR and each participant had up to six data points at three to four-month interval clinical follow ups. Exposure categories were current and historic (ever) water sources including well water or not, and baseline water sources including reverse osmosis water or not. Before conducting the model we used Q-Q plots to check the normality of residuals of eGFR (assumption of normality held), and checked for correlations among the predictors with the Variance Inflation Factor (values ranging 1.04–1.50) indicating no significant multicollinearity. The two types of water categories (historic or baseline) were tested in separate models, in which the time point of eGFR collection, water source, age, gender were included as fixed effects, and participants as random effects. The model was fitted in the MIXED procedure in SAS version 9.5 (SAS Institute Inc, Cary, NC, USA).
Data availability
Data associated with this publication is available from the corresponding author and through the KIiPP project website at https://env.chem.uconn.edu/kipp-nih/.
References
NCD Risk Factor Coll. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 389, 37–55 (2017).
Carney, E. F. The impact of chronic kidney disease on global health. Nat. Rev. Nephrol. 16, 251 (2020).
Lunyear, J. et al. CKD of uncertain etiology: a systematic review. Clin. J. Am. Soc. Nephrol. 11, 379–385 (2016).
Correa-Rotter, R., Wesseling, C. & Johnson, R. J. CKD of unknown origin in Central America: the case for a Mesoamerican nephropathy. Am. J. Kidney Dis. 63, 506–520 (2014).
Anand, S., Staniec, A., Montez-Rath, M. & Vlahos, P. Using GIS mapping to track hot spots of kidney disease in California. N. Engl. J. Med. 382, 2265–2267 (2020).
Iqbal, M. C. M. & Dissanayake, C. B. CKDu in Sri Lanka. Science 344, 981 (2014).
Nanayakkara, N. et al. Tackling the fallout from chronic kidney disease of unknown etiology: why we need to focus on providing peritoneal dialysis in rural, low-resource settings. Kidney Int. Rep. 2, 1–4 (2017).
Abeywardana, N., Bebermeier, W. & Schütt, B. Ancient water management and governance in the dry zone of Sri Lanka until abandonment, and the influence of colonial politics during reclamation. Water 10, 1746 (2018).
Mahatantila, K., Chandrajith, R., Jayasena, H. A. H. & Ranawana, K. B. Spatial and temporal changes of hydrogeochemistry in ancient Tank Cascade Irrigation Systems (TCIS) in Sri Lanka: evidence for a constructed wetland. Water Environ. J. 22, 17–24 (2008).
WHO. WHO-International expert consultation on CKDu. Colombo, Sri Lanka http://www.searo.who.int/srilanka/documents/report_international_expert_consultation_on_ckdu.pdf (2016).
Weeraratne, S. & Wimalawamsa, S. A major irrigation project - accelerated Mahaweli program and the chronic kidney disease of multifactorial origin in Sri Lanka. Int. J. Agric. Environ. Res. 1, 16–27 (2015).
Rajapakse, S., Shivanthan, M. C. & Selvarajah, M. Chronic kidney disease of unknown etiology in Sri Lanka. Int. J. Occup. Environ. Health 22, 259–264 (2016).
Vlahos, P. et al. Kidney Progression Project (KiPP): protocol for a longitudinal cohort study of progression in chronic kidney disease of unknown etiology in Sri Lanka. Glob. Pub. Health 10, 1–13 (2018).
Cooray, T. et al. Drinking-water supply for CKDu affected areas of Sri Lanka, using nanofiltration membrane technology: from laboratory to practice. Water 11, 2512 (2019).
Shah, M. D. & Iqbal, M. Diazinon-induced oxidative stress and renal dysfunction in rats. Food Chem. Toxicol. 48, 3345–3353 (2010).
Marouani, N. et al. Involvement of oxidative stress in the mechanism of p,p’-DDT-induced nephrotoxicity in adult rats. Gen. Phys. Biophys. 36, 309–320 (2017).
Rankin, G. O. et al. In vitro nephrotoxicity induced by propanil. Environ. Tox. 23, 435–442 (2008).
Choudhary, N., Sharma, M., Verma, P. & Joshi, S. C. Hepato and nephrotoxicity in rat exposed to endosulfan. J. Environ. Biol. 24, 305–308 (2003).
Bellizzi, V. et al. Effects of water hardness on urinary risk factors for kidney stones in patients with idiopathic nephrolithiasis. Nephron 81, 66–70 (1999).
Shuster, J. et al. Water hardness and urinary stone disease. J. Urol. 128, 422–425 (1982).
Anand, S. et al. Prospective biopsy-based study of CKD of unknown etiology in Sri Lanka. CJASN 14, 224–232 (2019).
Vervloet, M. et al. The role of phosphate in kidney disease. Nat. Rev. Nephrol. 13, 27–38 (2017).
Levey et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 5, 604–612 (2009).
Shipley, E., Vlahos, P. & Chandrajith, R. (2022) Water quality in Sri Lankan inland water sources. (Env. Adv) in press.
EPA. Environmental Chemistry Methods (ECM) Index–E. https://www.epa.gov/pesticide-analytical-methods/environmental-chemistry-methods-ecm-index-e (2018).
APHA. AWWA. Standard Methods for the Examination of Water and Water 22nd edn (American Public Health Association, American Water Works Association, Water Environment Federation, 2012).
Boucquemont, J. et al. Regression methods for investigating risk factors of chronic kidney disease outcomes: the state of the art. BMC Nephrol. 15, 45 (2014).
IUPAC. Propanil regulation from IUPAC technical report, Pure Appl. Chem. 75, 1123–1155 (2003).
Acknowledgements
We thank the participants of the study from Wilgamuwa for their continued enthusiasm, dedication and support of the KiPP project We are grateful to the research team of of H.P.M. Hewavitharane (research coordinator), S.M.R.G. Godavita (RA), H.P.N. Santhushya (RA), D.M.D.A. Dissanayake (RA), W.M.K.G.P. Wijerathne (RA), R.D.M.B. Karunrathne (RA), H.S. Sandaruwan (RA), A.M.C.M. Athanayake (field assistant), P.N. Hewavitharane (field assistant), working in to collect participant and environmental data. This work was supported by the U.S. NIH Fogarty International Center under Grant R21TW010425 and NIH RO1 DK127138. Dr. Anand is also supported by NIDDK K-23. The investigators would also like to acknowledge the support of the Sri Lankan Ministry of Health for the facilitation of the above research and Saman Rathnayake, Director, Teaching Hospital, Kandy, Kandy Kidney Protection Society, Wilgamuwa and Girandurukotte, Ministry of Health, Central Province.
Author information
Authors and Affiliations
Contributions
P.V. was the lead PI on the NIH Fogarty award, led the study design and analysis and prepared this manuscript. S.L.S., T.S., R.C., N.N., L.H., and J.J.S. are all co-PIs on the project and contributed to project design, implementation and have approved this manuscript. S.A. contributed to the project design, data analysis, and preparation of this manuscript. E.S. performed the agrochemical analysis and revisions of this manuscript, S.D. performed the field sampling and inorganic analyses, C.H. and T.H. performed statistical analyses, A.S. performed GIS analyses, P.H. was the field team manager and managed all data collection and entries.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vlahos, P., Schensul, S.L., Anand, S. et al. Water sources and kidney function: investigating chronic kidney disease of unknown etiology in a prospective study. npj Clean Water 4, 50 (2021). https://doi.org/10.1038/s41545-021-00141-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41545-021-00141-2
- Springer Nature Limited
This article is cited by
-
Screening of Micro-organic Compounds in Groundwater from Areas with Chronic Kidney Disease of Unclear Aetiology (CKDu) in the Dry Zone of Sri Lanka
Exposure and Health (2024)
-
Geochemical Characteristics of Groundwater Consumed by Patients with Chronic Kidney Disease with Unknown Aetiology in the Crystalline Dry Zone Terrain of Sri Lanka
Exposure and Health (2024)