
Abstract
Vaccine development targeting SARS-CoV-2 in 2020 was of critical importance in reducing COVID-19 severity and mortality. In the U.K. during the initial roll-out most individuals either received two doses of Pfizer COVID-19 vaccine (BNT162b2) or the adenovirus-based vaccine from Oxford/AstraZeneca (ChAdOx1-nCoV-19). There are conflicting data as to the impact of age, sex and body habitus on cellular and humoral responses to vaccination, and most studies in this area have focused on determinants of mRNA vaccine immunogenicity. Here, we studied a cohort of participants in a population-based longitudinal study (COVIDENCE UK) to determine the influence of age, sex, body mass index (BMI) and pre-vaccination anti-Spike (anti-S) antibody status on vaccine-induced humoral and cellular immune responses to two doses of BNT162b2 or ChAdOx-n-CoV-19 vaccination. Younger age and pre-vaccination anti-S seropositivity were both associated with stronger antibody responses to vaccination. BNT162b2 generated higher neutralising and anti-S antibody titres to vaccination than ChAdOx1-nCoV-19, but cellular responses to the two vaccines were no different. Irrespective of vaccine type, increasing age was also associated with decreased frequency of cytokine double-positive CD4+T cells. Increasing BMI was associated with reduced frequency of SARS-CoV-2-specific TNF+CD8% T cells for both vaccines. Together, our findings demonstrate that increasing age and BMI are associated with attenuated cellular and humoral responses to SARS-CoV-2 vaccination. Whilst both vaccines induced T cell responses, BNT162b2 induced significantly elevated humoral immune response as compared to ChAdOx-n-CoV-19.
Similar content being viewed by others

Introduction
SARS-CoV-2 is the causative agent of coronavirus disease 2019 (COVID-19). As of February 2024 SARS-CoV-2 has infected over 774 million people and is responsible for over 6.9 million deaths worldwide1, however this is likely to be an under-estimation as excess mortality due to COVID-19 in April 2022 was estimated to be 18 million people2. SARS-CoV-2 also causes the debilitating illness, long-COVID, which affects around 10% of those infected3. Due to the profound morbidity and mortality caused by SARS-CoV-2, the development of vaccines in 2020 was of critical importance. In the U.K. three vaccines were licenced for use by the start of 2021. These include the mRNA vaccines from Pfizer (BNT162b2) and Moderna (mRNA-1273) and the adenovirus-based vaccine from AstraZeneca/Oxford (ChAdOx1-nCoV-19)4. In 2020-2021 during the initial roll-out of COVID-19 vaccination in the U.K., most individuals received a primary course comprising two doses of BNT162b2 or ChAdOx1-nCoV-195,6.
Individuals who are male, older in age, or with high Body Mass Index (BMI) are at increased risk of morbidity and mortality from COVID-197,8—therefore, studies have focussed on vaccine immunogenicity in these at risk populations. Increasing age has been associated with reduced IgG and neutralising antibody titre after two BNT162b2 vaccine doses9,10. In contrast, a study assessing both BNT162b2 or ChAdOx1 immunogenicity showed no significant difference in humoral or cellular immune response after vaccination in those ≥80 years as compared to those <80 years11. The published BMI studies show conflicting results, with either no effect10,12, decreased13,14 or increased15 humoral BNT162b2 vaccine immunogenicity observed with increased BMI. Few studies have shown any influence of sex on vaccine efficacy—of those mentioned above, only one identified that females have a higher anti-Spike IgG antibody titre post-BNT162b2 vaccination10.
There are relatively few studies investigating the cellular and humoral immune response to both BNT162b2 and ChAdOx1-nCoV-19 in those individuals at risk, with most studies focussing on the impact of individual demographics on mRNA vaccine efficacy. There is also a lack of studies assessing individuals’ determinants on cellular versus humoral immunity. Here, we assessed a population-based cohort from the COVIDENCE study16, who had either two doses of BNT162b2 or ChAdOx-n-CoV-19 to determine the influence of individual demographic variables such as age, sex, BMI, and pre-vaccination IgG/A/M anti-Spike seropositivity on SARS-CoV-2 antibody and antigen-specific CD4+ and CD8+ T cell response, bulk T cell functional phenotypes and antigen-induced whole blood cytokine secretion following to the first two doses of the vaccines BNT162b2 and ChAdOx-n-CoV-19.
Results
Identification of individual correlates of immunogenicity
Characteristics of the 115 participants with humoral and cellular data included in the analyses are presented in Table 1. The median age was 66.4 years (IQR 61.0–68.9), 47 (41%) males and 68 (59%) females, 57 (49.6%) had a BMI less than 25, 45 (39.1%) had a BMI of 25–30 and a further 13 (11.3%) had a BMI of greater than 30. Of the participants 77 (66.9%) received ChAdOx1 and 38 (33.0%) received BNT162b2. When individuals were separated according to vaccine type received, the individual characteristics were similar (Supplementary Table 1). To identify demographic and technical factors associated with humoral and cellular responses to COVID-19 vaccination we first performed univariate analysis of ten factors: age, sex, ethnicity, general health category, vaccine type, number of days between 1st and 2nd vaccination [inter-vaccine days], days post second vaccine, pre-vaccine SARS-CoV-2 serostatus, BMI value, and BMI category. This analysis identified seven factors, which had a significant association with cellular and/or humoral immune responses: age, sex, pre-vaccine SARS-CoV-2 serostatus, BMI category, vaccine type, inter-vaccine days, and days post second vaccine (Supplementary Tables 2a–i). These seven factors were adjusted for in subsequent analyses to identify independent associations.
Immune correlates with anti-Spike and SARS-CoV-2 neutralising antibody titres after SARS-CoV-2 vaccination
First, we investigated whether there was any relationship between humoral and cellular immune responses we measured and post-vaccine anti-Spike and neutralising titres, adjusting for the seven baseline and post-vaccination covariates identified in univariate analyses described above. Post-vaccination titres of anti-Spike combined IgG/A/M antibody ratio responses were identified to be associated with neutralising antibody concentrations, three spike-specific CD4+T cell phenotypes and spike-stimulation induced IFNγ secretion (Fig. 1, Supplementary Table 3; quadratic regression for general linear models with adjustment for covariates). In addition, neutralising antibody concentrations significantly correlated with SARS-CoV-2-specific TNF+CD8+ T cell frequency (p = 0.0003, Supplementary Table 4; quadratic regression for general linear models with adjustment for covariates). As expected, post-vaccination titres of neutralising and anti-Spike IgG/A/M antibody ratio correlated positively with each other (R = 0.47, p < 0.0001, Fig. 1a; Pearson correlation and quadratic regression for general linear models with adjustment for covariates respectively). In addition, anti-S IgG/A/M antibody ratio correlated positively with IFNy secretion from SARS-CoV-2 peptide-stimulated whole blood (R = 0.31, p = 0.001; Fig. 1b; Pearson correlation and quadratic regression for general linear models with adjustment for covariates respectively). The three spike-specific CD4+T cell populations from PBMC SARS-CoV-2 peptide-stimulated cultures that positively correlated with anti-Spike IgG/A/M antibody ratio post-vaccination were all double-positive cytokine producers: IFN-γ+IL2+ (R = 0.37, p = 0.0003; Pearson correlation and quadratic regression for general linear models with adjustment for covariates respectively); TNF+IL-2+ (R = 0.35, p = 0.0004; Pearson correlation and quadratic regression for general linear models with adjustment for covariates respectively); IFN-γ+TNF+ (R = 0.32, p = 0.001; Pearson correlation and quadratic regression for general linear models with adjustment for covariates respectively) (Fig. 1c). There was also a trend (q = 0.1) for a positive correlation between anti-Spike IgG/A/M and SARS-CoV-2 peptide-specific CD4+IL-2 single positive T cells (Supplementary Table 3; quadratic regression for general linear models with adjustment for covariates). Significant correlations were maintained between anti-Spike combined IgG/A/M antibody and neutralising antibody concentrations and spike-stimulation induced IFNγ secretion when not including vaccine type as a covariate adjustment (R = 0.56; Pearson correlation and Supplementary Fig. 4).

Correlation between post-COVID-19 vaccine anti-S IgG/A/M antibody ratio and a, neutralising antibody titre IC50, b, whole blood IFNγ production after S peptide stimulation and c, percent of cytokine positive CD4+ T after PBMC stimulation with S peptide as determined by intracellular cytokine staining. Coloured according to IFNγ production from S peptide-stimulated whole blood (SARS-S WB). Data presented on x and y axes are normalised including log2 transformation and adjusted for the baseline and post-vaccination covariates (age, sex, BMI category, pre-vaccine SARS-CoV-2 serostatus, vaccine type, vitamin D randomisation, inter-vaccine days, and days post second vaccine), p values derived using the quadratic regression for general linear models with adjustments for covariates, all q < 0.01. Trend line indicates Pearson correlation (R-statistic).
Influence of pre-vaccination anti-S IgG/A/M antibody ratio on post-vaccine humoral and cellular responses
We next determined whether there was a relationship between pre-vaccine anti-Spike IgG/A/M antibody ratio on post-vaccine humoral and cellular responses (Supplementary Table 5), including adjustment for baseline and post-vaccination covariates (age, sex, BMI category, vitamin D randomisation, vaccine type, inter-vaccine days, and days post second vaccine). Pre-vaccine anti-Spike IgG/A/M antibody ratios were significantly correlated with post-vaccine anti-Spike IgG/A/M antibody ratios (p < 0.001; Pearson correlation and quadratic regression for general linear models with adjustment for covariates respectively) (Fig. 2a), frequency of IFNγ+CD4+ and IFNγ+CD8 + SARS-CoV-2-specific T cells (p < 0.001; quadratic regression for general linear models with adjustment for covariates) (Fig. 2b, c) and frequency of effector memory CD4+T cells in unstimulated PBMC (p = 0.006; Supplementary Table 5; quadratic regression for general linear models with adjustment for covariates). Comparing those who were considered seropositive (anti-Spike IgG/A/M antibody ratio ≥1) vs seronegative pre-vaccination, post-vaccine anti-Spike IgG/A/M antibody ratios and frequency of IFNγ+CD4+SARS-CoV-2-specific T cells remained significantly different (p < 0.001) (Supplementary Table 6; t-test for general linear models with adjustment for covariates). Together, these data demonstrate that individuals with baseline seropositivity due to prior SARS-CoV-2 infection had a stronger absolute cellular immune response following SARS-CoV-2 vaccination than those who were anti-S seronegative. These responses will be a combination of the original infection induced T cell memory and that expanded by the vaccination, as baseline PBMC were not taken, T cell expansion could not be assessed.

Correlation between pre-COVID-19 vaccine anti-S IgG/A/M antibody ratio and post-COVID-19 vaccine. a anti-S IgG/A/M antibody ratio, and frequency of IFNy+ b, CD4+ and c, CD8+ T cells after S peptide stimulation, b, c coloured according to anti-S IgG/A/M antibody ratio normalised to mean 0 and variance ±1. Data presented on x and y axes are normalised including log2 transformation and adjusted for the baseline and post-vaccination covariates (age, sex, BMI category, vaccine type, vitamin D randomisation, inter-vaccine days, and days post second vaccine), p value derived using thequadratic regression for general linear models with adjustments for covariates, all q < 0.01. Trend line indicates Pearson correlation (R-statistic).
Influence of vaccine type, inter-dose interval and time from vaccination to blood sampling on post-vaccine immune responses
Having identified cellular and humoral correlates of post-vaccination anti-S and neutralising antibody titre, irrespective of vaccine type, we next investigated whether there were any differences in cellular and humoral correlates between those who received BNT162b2 and ChAdOx1-nCoV-19. Adjusting for the other baseline and post-vaccination covariates, as above, we found BNT162b2 induced significantly higher anti-S IgG/A/M antibody ratio and neutralising antibody titres compared to ChAdOx1-nCoV-19 (Fig. 3a, b, Supplementary Table 7; t-test for general linear models with adjustment for covariates). There were, however, no significant differences in unstimulated or antigen-stimulated cellular responses that we measured in PBMC or whole blood between those who received BNT162b2 compared with those who received ChAdOx1-nCoV-19 (Supplementary Table 7). Separately analysing post-vaccination anti-S IgG/A/M antibody ratio correlations for each vaccine type, BNT162b2 had a stronger correlation compared to ChAdOx1-nCoV-19 with neutralising antibody titres (R = 0.691 vs R = 0.467, respectively; Pearson correlation) (Fig. 3c) and spike-stimulation induced IFNγ secretion (R = 0.418 vs R = 0.345, respectively) (Fig. 3d), although BNT162b2 Pearsons correlations were less significant due to smaller sample size compared to ChAdOx1-nCoV-19. Post-vaccination anti-S IgG/A/M antibody ratio correlations with the three polyfunctional spike-specific CD4+T cell populations previously identified, irrespective of vaccine type (Fig. 1c), showed stronger correlation for BNT162b2 with TNF+IL-2+CD4+T cells (R = 0.51, vs R = 0.31 ChAdOx1-nCoV-19; Pearson correlation) and IFN-γ+IL2 + CD4+T cells (R = 0.39, vs R = 0.35 ChAdOx1-nCoV-19; Pearson correlation); whereas ChAdOx1-nCoV-19 had stronger for IFN-γ+TNF+CD4+T cells (R = 0.33, vs R = 0.14 BNT162b2; Pearson correlation) (Supplementary Fig. 5).

Cumulative data showing a anti-Spike IgG/A/M antibody ratio and b neutralising antibody titre IC50 in participants post-vaccination with either BNT162b2 or ChAdOx1-nCoV-19. Line indicated Median. Data points are plotted without covariate adjustment. Correlations plotted separately for participants who received either BNT162b2 (blue) or ChAdOx1-nCoV-19 (yellow) comparing post-vaccination anti-S IgG/A/M antibody ratio, and post-vaccination. c neutralising antibody (NAB) titre IC50. d whole blood IFNγ production after S peptide stimulation. Data presented on x and y axes are normalised including log2 transformation and adjusted for the baseline and post-vaccination covariates (age, sex, BMI category, pre-vaccine SARS-CoV-2 serostatus, vitamin D randomisation, inter-vaccine days, and days post second vaccine), p value derived using t-test (a and b) or quadratic regression (c and d) for general linear models with adjustment for covariates. Trend line indicates Pearson correlation (R-statistic).
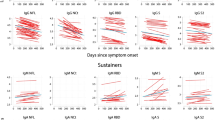
When analysing whether there was an impact of the number of days between vaccinations and measured immune responses, we only identified a trend for the frequency of SARS-CoV-2 peptide-specific TNF+IFNγ+CD4+T cells and TNF+CD8+ T cells (p ≤ 0.007; q = 0.16) when adjusting for the other baseline and post-vaccination covariates (Supplementary Table 8; quadratic regression for general linear models with adjustment for covariates). However, we did find that the delay from the date of the second vaccine dose to the date of blood draw was positively correlated with the level of SARS-CoV-2 peptide-induced whole blood secretion of IL-6, IL-8 and TNF (p ≤ 0.0004), and a trend for negative correlation with Neutralising antibody titres (p = 0.01; q = 0.14) (Supplementary Table 9; linear regression for general linear models with adjustment for covariates).
Increasing age significantly altered the immune response to vaccination
Having determined the vaccine type and timing variables independently associated with vaccine-induced humoral and cellular immune responses, we next analyzed demographic correlates adjusting for all other baseline and post-vaccination covariates as previously. We found that increasing age was independently associated with lower anti-S antibody titres post-vaccination (R = −0.277, all participants adjusting for vaccine type; Pearson correlation) (Fig. 4a). There was no difference when analysing each vaccine type independently (R = −0.26, BNT162b2; R = −0.27, ChAdOx1-nCoV-19, Supplementary Fig. 6A; Pearson correlation). However, due to lower number of individuals who received BNT162b2, this did not reach statistical significance. For all participants, the frequency of polyfunctional spike-specific CD4+T cells from PBMC SARS-CoV-2 peptide-stimulated cultures post-vaccination also negatively correlated with increasing age for IFN-γ+IL-2+ (R = −0.24, p = 0.012; Pearson correlation and linear regression for general linear models with adjustment for covariates respectively) and TNF+IL-2+CD4+T cells (R = −0.24, p = 0.013; Pearson correlationand linear regression for general linear models with adjustment for covariates respectively) (Supplementary Table 10; and Fig. 4b). Supplementary Fig. 6B, C shows the same analysis separating by vaccine type, ChAdOx1-nCoV-19 had a stronger negative correlation for both CD4+T cell populations with age, compared to BNT162b2 (IFN-γ+IL-2+, R = −0.34 vs R = −0.15 and TNF+IL-2+, R = −0.32 vs −0.14; Pearson correlation), although the larger and younger age range of those who received ChAdOx1-nCoV-19 may have improved the strength of correlation for ChAdOx1-nCoV-19. As would be expected, we also found increasing age was independently associated with lower frequency of naive CD8+ T cells (p < 0.0001) and higher frequency of CD8 + EM (p = 0.004) and EMRA T cells (p = 0.004). These data collectively show that increasing age was associated with reduced humoral immunity associated with reduced double-positive cytokine-producing spike-specific CD4+T cells, and vaccine type having no or only minor effect on these age-related differences.

a Correlation between age and post-vaccine anti-Spike IgG/A/M antibody ratio, coloured according to frequency of naive (CD45RA+CD27+) CD8+ T cells present in the peripheral blood of the individuals. b percent of cytokine positive CD4+T after PBMC stimulation with S peptide as determined by intracellular cytokine staining, coloured according to anti-S IgG/A/M antibody ratio normalised to mean 0 and variance ±1. Data presented on y axis is normalised including log2 transformation and adjustment for baseline and post-vaccination covariates (sex, BMI category, pre-vaccine SARS-CoV-2 serostatus, vaccine type, vitamin D randomisation, inter-vaccine days, and days post second vaccine), p values derived using linear regression for general linear models with adjustments for the same covariates, all q < 0.1. Trend line indicates Pearson correlation (R-statistic).
Influence of BMI and gender on post-vaccine immune responses
Finally, we tested for associations between sex and BMI with SARS-CoV-2 cellular and humoral immunity, with analyses adjusted for baseline and post-vaccination co-variates as previously. We found a highly significant lower frequency of SARS-CoV-2-specific TNF+CD4+ and CD8+ T cells (p < 0.0001) correlated with increasing BMI category (Supplementary Table 11; ANOVA for general linear models with adjustment for covariates), as well as trends of lower SARS-CoV-2-specific IL-2+CD4+T cells and higher CRP (p ≤ 0.014, q < 0.156). There was no significant association between higher BMI category and anti-Spike or neutralising antibodies. (Supplementary Table 11; ANOVA for general linear models with adjustment for covariates), despite our finding that the level of neutralising antibodies significantly correlated with SARS-CoV-2-specific TNF+CD8+ T cells (Supplementary Table 5), which were decreased with increasing BMI. This remained true if we analysed each vaccine type separately.
When analysing associations between sex immune correlates, the most significant difference was in our control assay with higher LPS induced IL-6 secretion in whole blood stimulated plasma (p < 0.0001). Males also had a higher frequency of CD8+ (p = 0.0001) and CD4+ (p = 0.011) EM T cells, whilst females had a higher frequency of naive CD4+ (p = 0.012) and CD8+ (p = 0.002) T cells (Supplementary Table 12; t test for general linear models with adjustment for covariates). However, these differences did not impact upon SARS-CoV-2-specific cellular or humoral responses post-vaccination between males and females with no significant differences observed (Supplementary Table 11). Collectively these data show sex had no impact on SARS-CoV-2 vaccine immunogenicity, whilst BMI had significant effects on single cytokine producing SARS-COV-2-specific T cell functions we independently identified to be associated with SARS-CoV-2 neutralising antibody concentrations post-vaccination.
Discussion
In this study, we observed that there was a significant positive correlation between humoral and cellular SARS-CoV-2-specific immunity post vaccination which were modified by increasing age and BMI but not sex of individuals. The levels of anti-Spike IgG/M/A and SARS-CoV-2 neutralising antibodies were significantly correlated with SARS-CoV-2 induced cytokine secreting double-positive CD4+T cells or TNF+CD8+ T cells, respectively. As expected, those individuals who were seropositive prior to vaccination had the largest humoral and cellular immune response following SARS-CoV-2 vaccination, irrespective of vaccine type. We observed that there were significantly higher antibody titres and a stronger correlation between anti-Spike and neutralising antibody titres in participants that received BNT162b2 as compared to those that received ChAdOx1-nCoV-19. However, no unique antigen-specific cellular immunity differences were observed post-SARS-CoV-2 vaccination that explained these vaccine immunogenicity differences although there were differences in the strength of correlation with the frequency of distinct spike-specific CD4+T cell populations. By contrast, no impact of biological sex was observed for SARS-CoV-2 vaccine cellular and humoral immunity, despite cellular functional phenotype differences identified.
Previous studies have observed that BNT162b2 was more efficacious as a vaccine as compared to ChAdOx1-nCoV-19 at reducing infections and hospital admissions17,18,19. We observed that there were increased anti-S IgG/A/M antibody ratio and neutralising antibody titres with BNT162b2 as compared to ChAdOx1-nCoV-19, in line with previous observations11,15. Interestingly, whilst we did not observe any unique SARS-CoV-2 antigen-specific T cell populations induced by the different vaccines, BNT162b2 induced anti-Spike IgG/M/A titres had the strongest correlation with Spike-specific TNF+IL-2+CD4+T cells, whereas the strongest correlation for ChAdOx1-nCoV-19 was for TNF+IFN-γ+CD4+T cells. It is important to note that both vaccines still resulted in a good humoral and cellular immune response in the participants in this study. In line with the current literature15,20, we observed that there was increased COVID-19 vaccine immunogenicity in individuals that have had a prior infection with SARS-CoV-2. This boost in immunogenicity is believed to be due to the phenomenon of hybrid vigour immunity21.
It has been shown that older adults have reduced vaccine efficacy to influenza and shingles vaccine22,23, which is believed to be in part to immunosenescence and inflammageing24,25. This was particularly worrying at the start of the pandemic as older adults had increased morbidity and mortality from COVID-198. Therefore, when the vaccines were developed, studies were performed to assess COVID-19 vaccine efficacy in older adults—the resulting studies were conflicting with results demonstrating similar vaccine efficacy (as determine by infection events and hospitalisation) by age or reduced vaccine efficacy. In this study we observed that increasing age was associated with reduced post-vaccine anti-S antibody titre, in line with other studies which have shown reduced responses post-SARS-CoV-2 vaccination10,26, although older age has been associated with lower risk of breakthrough infection19. In our study, our older adults were not as old as (oldest individual 78 years old) previous studies into ageing where the age range was 80-86 years old11, suggesting that age-associated decline in immunogenicity is linear and may start declining in middle-age. This reduced antibody response with increasing age has been shown to be alleviated after SARS-CoV-2 vaccine booster9,26. Interestingly, we also observed a trend for decreased IFN-γ+IL-2+ and TNF+IL-2+CD4+T cells, which we found to be independently associated with post-vaccination anti-Spike IgG/M/A levels. This, therefore, links decreased T cell immunity with age to decreased humoral immunity.
Due to the inflammatory nature of obesity27, and the detrimental role that inflammation plays in antigen-specific immunity24, and the data which shows that obesity in humans and mice increases COVID-19 disease severity and increased hospitalisation in humans despite vaccination28,29—the impact of obesity on vaccine immunogenicity was investigated. Unlike in the large COVIDENCE cohort where we found increased BMI associated with higher anti-Spike IgG/A/M antibody ratio titres15 we did not observe the same relationship in this sub-study. Interesting, despite not identifying any relationship to increased BMI with humoral immunity, BMI category was associated with SARS-CoV-2-specific TNF+CD8+ and CD4+T cells, with TNF+CD8+ T cells independently highly correlated with SARS-CoV-2 neutralising antibody titres. It may be that a non-linear relationship exists between BMI category and neutralising antibodies. We also may not have power to detect this relationship, given we also did not identify the relationship between BMI and anti-Spike IgG/A/M antibody ratios identified in the larger cohort which included more individuals with BMI > 30 (11.8% here vs 18.5% in larger cohort). However, other studies have also either not observed any effect of increased BMI on SARS-CoV-2 vaccination using BNT162b210,12 or showed reduced antibody response post- BNT162b2 or CoronaVac vaccination in individuals with high BMI30. The difference between these studies may be due to the lower average BMI observed in our study as compared to previous studies10,12.
The main strength of this study was that it was a population-based study in which we applied multivariate analyses to identify independent and associated predictors of immune correlates post-COVID-19 vaccination. In addition, most studies to-date have focussed on BNT162b2 vaccine immunogenicity, the strength of our study is that we assessed vaccine Pfizer BNT162b2 and ChAdOx1-nCoV-19 vaccination allowing us to compare immune responses to the two vaccines administered at the same stage of the pandemic. One finding from our study was that we observed that the concentration of anti-Spike IgG/A/M antibody ratio significantly correlated with antigen-specific CD4+T cell immunity and induced cytokine secretion—demonstrating the strengths of combining a comprehensive characterisation of humoral responses with PBMC and whole blood antigen stimulation assays. The use of the combined IgG/A/M ELISA is another strength of this study, as a previous study has shown that when measuring individual IgG, IgA, and IgM isotypes during the pandemic, it was found that testing the individual isotypes alone was not as sensitive for picking up mild SARS-CoV-2 infections as the combined approach of IgG/A/M—demonstrating that the combined ELISA approach is best for identifying the breath of the antibody response. Another strength of the study was the robust co-variate adjustment ensuring that the differences we observed where due to the variable. The limitations to this study were that we had a bias towards older individuals in the study population, with limited number of people under 35 years old. In addition, there was a modest bias towards female sex (59% vs 41%) in our study population. Another limitation to the study was that it was a single time-point after COVID-19 vaccination, this means we were not able to look at waning immunity over time. It would also have been additive to the study to have collected PBMC samples pre- and post-vaccination, however this was not possible to the fast pace of the pandemic.
To conclude age, vaccine type and prior infection influence the humoral and cellular immune response to SARS-CoV-2 vaccination, whilst BMI affected cellular immunogenicity that independently associated with neutralising antibody levels. We found no difference in vaccine immunogenicity by sex. This study supports the need to include diverse populations during early vaccine efficacy testing, with demographic features related to poor infection outcome, and the benefits of parallel measurement of humoral and cellular immune functions to enable a thorough understanding of vaccine-induced immune correlates of protection.
Methods
Study design
This study was a sub-study nested within the CORONAVIT randomised controlled trial as reported elsewhere16,31. 6200 U.K. residents aged 16 years or older participated in the COVIDENCE U.K. study as described previously16, all of whom provided dried blood spot samples (prior to vaccination) for the determination of combined IgG, IgA and IgM (IgG/A/M) antibody responses to the Spike protein of SARS-CoV-2, as described below. A subset of the participants (123 individuals in total) returned after full informed written consent was obtained, after COVID-19 vaccination and provided a dried blood spot for antibody analysis and a sodium heparin blood sample to assess cellular immunity to SARS-CoV-2 using antigen-stimulated whole blood and peripheral blood mononuclear cell (PBMC) assays. Serum was also collected for C Reactive protein (CRP) and SARS-CoV-2 neutralising antibody quantification. The trial was sponsored by Queen Mary University of London, approved by the Queens Square Research Ethics Committee, London, U.K. (ref 20/HRA/5095), and registered with ClinicalTrials.gov (NCT04579640) on 8 October 2020, before enrolment of the first participant on 28 October 2020.
In vitro cellular immune response assays
Heparinised blood collected from all sub-study participants was used to assess cellular immunity post vaccination using two approaches:
Whole blood was stimulated in the presence or absence of PepTivator® SARS-CoV-2 Prot_S Complete (1 µg/mL; Miltenyi Biotec) or E. coli lipopolysaccharide (LPS, 1–1000 ng/mL; Invivogen) for 24 h at 37 °C in 5% CO2. Following incubation plasma was collected and stored at −80 °C for cytokine assessment by cytometric bead array as detailed below.
PBMCs were isolated from heparinised blood using Ficoll (Merck Life Science) density gradient, washed twice in Hanks Balanced Salt Solution (Merck Life Science) and cryopreserved in 10% dimethylsulphoxide (DMSO) in Fetal Calf Serum (Invitrogen). Subsequently, 5 × 105 cells/condition of cryopreserved PBMCs were recovered and stimulated with nothing (negative control) or PepTivator® SARS-CoV-2 Prot_S Complete (Miltenyi Biotec, 1 µg/mL) or 1 µg/mL of soluble CD3 monoclonal antibody (OKT3, Functional Grade, Invitrogen) for 1 h at 37 °C in 5% CO2. Brefeldin A (2.5 µg/mL) was then added to the cells, which were incubated for a further 15 h at 37 °C in 5% CO2. Cells were collected and analysed by flow cytometry as detailed below.
Flow cytometric analysis
Cells were cell surface stained for CD3 (clone: HIT3a; 5 in 100 dilution; catalogue no.300306), CD4 (RPA-T; 3 in 100 dilution; catalogue no.4300528), CD8 (SK1; 2 in 100 dilution; catalogue no. 344732), CD27 (O232; 2 in 100 dilution; catlog no.302832), CD45RA (HI100; 4 in 100 dilution; catlog no.304108) and Zombie NIR viability dye (Biolegend, San Diego, CA, USA) in the presence of Brilliant Buffer (BD Biosciences). Cells were washed and then fixed in Intracellular Fixation Buffer (eBioscience), permeabilised in eBioscience Permeablization Buffer and stained for intracellular IL-2 (JES6-5H4; 1 in 100 dilution; catalogue no. 503810), IFN-γ (4 S.B3; 1 in 100 dilution; catalogue no.502528) and TNF (Mab11, 0.5 in 100 dilution; catalogue no.502932) (Biolegend). Cells were then washed and acquired using the ACEA Novocyte 3000 flow cytometer (Agilent). Data were analysed using FlowJo Version X (BD Biosciences). A representative flow cytometry gating strategy is shown in Supplementary Fig. 1. Following single cell and live cell gating, once CD3+CD4+ and CD8+ cells were identified then proportion cytokine expression was calculated in the stimulated conditions based upon the unstimulated control. In addition, T cell phenotypic staining was performed on unstimulated cells using the markers CD27 and CD45RA to determine if the CD4+ or CD8+ T cell are naive (CD27+CD45RA+), central memory (CM, CD27+CD45RA−), effector memory (EM, CD27-CD45RA-) or senescent-like effector memory re-expressing CD45RA (EMRA; CD27-CD45RA+). A representative flow cytometry gating strategy for T cell memory phenotypes and representative plots from young (<40 years) and old (≥60 years) donors is shown in Supplementary Fig. 2.
Anti-spike (S) IgG/A/M serology testing
Anti-S IgG/A/M titres were determined by the Clinical Immunology Service at the Institute of Immunology and Immunotherapy of the University of Birmingham using an ELISA that measures combined IgG/A/M responses to the SARS-CoV-2 trimeric Spike glycoprotein (product code MK654, The Binding Site [TBS], Birmingham, U.K.), as previously described15,32. This assay has been CE-marked with 98.3% (95% confidence interval [CI] 96.4–99.4) specificity and 98.6% (92.6–100.0) sensitivity for RT-PCR-confirmed mild-to-moderate COVID-1932,33, and has been validated as a correlate of protection against breakthrough SARS-CoV-2 infection in two populations33,34. A cut-off ratio relative to the TBS assay cut-off calibrators was determined by plotting 624 pre-2019 negatives in a frequency histogram. A cut-off coefficient was then established for IgG/A/M (1.31), with ratio values classed as positive (≥1) or negative (<1). Dried blood spot eluates were pre-diluted 1:40 with 0.05% PBS-Tween using a Dynex Revelation automated absorbance microplate reader (Dynex Technologies). Plates were developed after 10 min using 3,30,5,50-tetramethylbenzidine core, and orthophosphoric acid used as a stop solution (both TBS). Optical densities at 450 nm were measured using the Dynex Revelation.
SARS-CoV-2 neutralising antibody
Serum titres of neutralising antibodies to SARS-CoV-2 were measured as previously described using an authentic virus (Wuhan Hu-1 strain) microneutralisation assay35.
C-reactive protein assessment
Serum was analysed for C-Reactive protein concentrations using Human C-Reactive Protein/CRP DuoSet ELISA (Biotechne, R+D systems) according to the manufacturers protocol.
Cytometric bead array
A cytometric bead array to measure IL-8, IL-6, IFN-γ and TNF in whole blood stimulated plasma was carried out according to the manufacturer’s protocol (BD Biosciences). Samples were analysed using the ACEA Novocyte 3000 flow cytometer (Agilent). The lower limit of detection was 1.5 pg/mL.
Statistical analysis
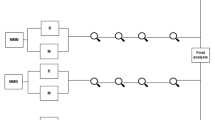
Principle component analysis (PCA) and general linear modelling (GLM) was conducted using Qlucore Omics Explorer 3.7 (Qlucore AB, Lund, Sweden). Analyte concentrations were log2 converted and normalised to the mean for each analyte with variance -1 to +1. Missing values were imputed by K nearest neighbours (k-NN). Of the 127 participants with acquired data, 12 were excluded from statistical analysis (two due to haematological malignancy with an absence of CD4+T cells, four due to immunodeficiency, three for being on immunosuppressive medication, one as having reported worst health and two who were identified as outliers on PCA (Supplementary Fig. 3). Similarity between two analytes analysed by Pearson correlation. Parameters whose concentration differed significantly between vaccination type, sex and pre-vaccination anti-Spike serostatus were identified using the t-test for GLM, differences based on BMI category, ethnicity and general health category were assessed by multinomial linear regression, whilst parameters affected by age, BMI value and days post second vaccination were identified using a liner regression model and inter-vaccine days were analysed by quadratic regression, all with adjustment for baseline COVIDENCE trial arm allocation [placebo, low vitamin D supplementation, high vitamin D supplementation] although we found no significant effect of vitamin D supplementation on vaccine efficacy in the trial16. All baseline and post-vaccination covariates identified in univariate analysis to influence the inflammatory profile, were then reanalysed using the same approach but with additional adjustment for all other identified significant covariates. Covariate adjustment was performed using the eliminated factors approach that fits a multiple regression model to all covariates and subtracts the expression values predicted by this model from the observed values in order to remove covariate effects between patients36. Anti-spike ratios pre- and post-vaccination and NAB titres post-vaccination were analysed by quadratic regression, with similar adjustment for all identified baseline and post-vaccination covariates. These analyses yield t-statistics representing the magnitude of difference in concentration of a given parameter between groups being compared (calculated as the regression coefficient for each parameter divided by its standard deviation), p values and q values (Benjamini–Hochberg false discovery rate. Thresholds of 0.05 were applied for p and q values throughout.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
The data that support the findings of this study are available on request from the corresponding author, [ES Chambers]. The data are not publicly available due to it containing information that could compromise the privacy of research participants.
References
WHO. WHO coronavirus (COVID-19) dashboard. Available: https://covid19.who.int/.
Collaborators, C.-E.M. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020-21. Lancet 399, 1513–1536 (2022).
Davis, H. E., McCorkell, L., Vogel, J. M. & Topol, E. J. Long COVID: major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 21, 133–146 (2023).
Francis, A. I., Ghany, S., Gilkes, T. & Umakanthan, S. Review of COVID-19 vaccine subtypes, efficacy and geographical distributions. Postgrad. Med. J. 98, 389–394 (2022).
Voysey, M. et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 397, 99–111 (2021).
Polack, F. P. et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 383, 2603–2615 (2020).
Palaiodimos, L. et al. Severe obesity, increasing age and male sex are independently associated with worse in-hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 108, 154262 (2020).
Williamson, E. J. et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 584, 430–436 (2020).
Renia, L. et al. Lower vaccine-acquired immunity in the elderly population following two-dose BNT162b2 vaccination is alleviated by a third vaccine dose. Nat. Commun. 13, 4615 (2022).
Pellini, R. et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine 36, 100928 (2021).
Parry, H. et al. Differential immunogenicity of BNT162b2 or ChAdOx1 vaccines after extended-interval homologous dual vaccination in older people. Immun. Ageing 18, 34 (2021).
Bates, J. T. et al. IgG antibody response to the Pfizer BNT162b2 SARS-CoV-2 vaccine in healthcare workers with healthy weight, overweight, and obesity. Vaccines (Basel) 10, 512 (2022).
Faizo, A. A. et al. A potential association between obesity and reduced effectiveness of COVID-19 vaccine-induced neutralizing humoral immunity. J. Med. Virol. 95, e28130 (2023).
Gaborit, B. et al. Early humoral response to COVID-19 vaccination in patients living with obesity and diabetes in France. The COVPOP OBEDIAB study with results from the ANRS0001S COV-POPART cohort. Metabolism 142, 155412 (2023).
Jolliffe, D. A. et al. Determinants of antibody responses to SARS-CoV-2 vaccines: population-based longitudinal study (COVIDENCE UK). Vaccines (Basel) 10, 1601 (2022).
Jolliffe, D. A. et al. Vitamin D supplementation does not influence SARS-CoV-2 vaccine efficacy or immunogenicity: sub-studies nested within the CORONAVIT randomised controlled trial. Nutrients 14, 3821 (2022).
Wei, J. et al. Comparative effectiveness of BNT162b2 and ChAdOx1 nCoV-19 vaccines against COVID-19. BMC Med. 21, 78 (2023).
Andrews, N. et al. Covid-19 vaccine effectiveness against the omicron (B.1.1.529) variant. N. Engl. J. Med. 386, 1532–1546 (2022).
Vivaldi, G. et al. Risk factors for SARS-CoV-2 infection after primary vaccination with ChAdOx1 nCoV-19 or BNT162b2 and after booster vaccination with BNT162b2 or mRNA-1273: a population-based cohort study (COVIDENCE UK). Lancet Reg. Health Eur. 22, 100501 (2022).
Reynolds, C. J. et al. Heterologous infection and vaccination shapes immunity against SARS-CoV-2 variants. Science 375, 183–192 (2022).
Crotty, S. Hybrid immunity. Science 372, 1392–1393 (2021).
John, A. R. & Canaday, D. H. Herpes zoster in the older adult. Infect. Dis. Clin. North Am. 31, 811–826 (2017).
Fleming, D. M. & Elliot, A. J. The impact of influenza on the health and health care utilisation of elderly people. Vaccine 23, S1–S9 (2005).
Chambers, E. S. & Akbar, A. N. Can blocking inflammation enhance immunity during aging? J. Allergy Clin. Immunol. 145, 1323–1331 (2020).
Pereira, B., Xu, X. N. & Akbar, A. N. Targeting inflammation and immunosenescence to improve vaccine responses in the elderly. Front. Immunol. 11, 583019 (2020).
Romero-Olmedo, A. J. et al. Induction of robust cellular and humoral immunity against SARS-CoV-2 after a third dose of BNT162b2 vaccine in previously unresponsive older adults. Nat. Microbiol. 7, 195–199 (2022).
Vandanmagsar, B. et al. The NLRP3 inflammasome instigates obesity-induced inflammation and insulin resistance. Nat. Med. 17, 179–188 (2011).
van der Klaauw, A. A. et al. Accelerated waning of the humoral response to COVID-19 vaccines in obesity. Nat. Med. 29, 1146–1154 (2023).
O’Meara, T. R. et al. Reduced SARS-CoV-2 mRNA vaccine immunogenicity and protection in mice with diet-induced obesity and insulin resistance. J. Allergy Clin. Immunol. 152, 1107–1120 e1106 (2023).
Kara, Z. et al. Antibody response to SARS-CoV-2 vaccines in people with severe obesity. Obes. Surg. 32, 2987–2993 (2022).
Jolliffe, D. A. et al. Effect of a test-and-treat approach to vitamin D supplementation on risk of all cause acute respiratory tract infection and covid-19: phase 3 randomised controlled trial (CORONAVIT). BMJ 378, e071230 (2022).
Cook, A. M. et al. Validation of a combined ELISA to detect IgG, IgA and IgM antibody responses to SARS-CoV-2 in mild or moderate non-hospitalised patients. J. Immunol. Methods 494, 113046 (2021).
Shields, A. M. et al. COVID-19: seroprevalence and vaccine responses in UK dental care professionals. J. Dent. Res. 100, 1220–1227 (2021).
Vivaldi, G. et al. Correlation between postvaccination anti-spike antibody titers and protection against breakthrough severe acute respiratory syndrome coronavirus 2 infection: a population-based longitudinal study. J. Infect. Dis. 226, 1903–1908 (2022).
Reynolds, C. J. et al. Discordant neutralizing antibody and T cell responses in asymptomatic and mild SARS-CoV-2 infection. Sci. Immunol. 5, eabf3698 (2020).
MJ, W. The coordinate-free approach to linear models, Chapter 6. Cambridge University Press (2006).
Acknowledgements
COVIDENCE UK has received support from Barts Charity (MGU0459, MGU0466), Pharma Nord, the Fischer Family Foundation, DSM Nutritional Products, the Exilarch’s Foundation, the Karl R Pfleger Foundation, the AIM Foundation, Synergy Biologics, Cytoplan, the UK National Institute for Health and Care Research Clinical Research Network (52255; 52257), the Health Data Research UK BREATHE Hub, the UK Research and Innovation Industrial Strategy Challenge Fund (MC_PC_19004), Thornton & Ross, Warburtons, Matthew Isaacs (personal donation), Barbara Boucher (personal donation), and Hyphens Pharma. The views expressed are those of the authors and not necessarily those of the funders. We thank all participants of COVIDENCE UK, and the following organisations who supported study recruitment: Asthma UK/British Lung Foundation, the British Heart Foundation, the British Obesity Society, Cancer Research UK, Diabetes UK, Future Publishing, Kidney Care UK, Kidney Wales, Mumsnet, the National Kidney Federation, the National Rheumatoid Arthritis Society, the North West London Health Research Register (DISCOVER), Primary Immunodeficiency UK, the Race Equality Foundation, SWM Health, the Terence Higgins Trust, and Vasculitis UKAKC. JMG is supported by Rosetrees Trust (CF1\100003). AKC is supported by the NHMRC (GNT2020750). We would like to thank Professor Áine McKnight whose lab developed the neutralising antibody assay that was used in this study.
Author information
Authors and Affiliations
Contributions
A.R.M. wrote the study protocol. E.S.C. designed the cellular assays and along with WC performed the whole blood and PBMC experiments S peptide and LPS experiments. S.F. and A.G.R. developed, validated, and performed assays for anti-spike immunoglobulin (Ig) G, IgA, and IgM (IgG/A/M) Antibody ratio. N.P. and W.L. were responsible for patient recruitment and sample collection. J.M.G. and C.P. developed, validated, and performed assays for neutralising antibodies. A.K.C. and G.V. contributed to data management and statistical analyses. E.S.C. and A.K.C. generated figures. E.S.C., A.K.C. and A.R.M. wrote the first draught of the report. All authors reviewed the manuscript critically for important intellectual content, gave final approval of the version to be published. E.S.C. and W.C. are joint first co-author and A.K.C. and A.R.M. are joint co-last author.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chambers, E.S., Cai, W., Vivaldi, G. et al. Influence of individuals’ determinants including vaccine type on cellular and humoral responses to SARS-CoV-2 vaccination. npj Vaccines 9, 87 (2024). https://doi.org/10.1038/s41541-024-00878-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41541-024-00878-0
- Springer Nature Limited