
Abstract
Objective The aim of this study was to assess the current status of implant teaching within dental hygiene and therapy schools in the UK and Ireland.
Methods An online questionnaire relating to current and future possible trends in dental implantology education was developed and distributed to programme directors in each of the 23 dental hygiene and therapy schools in the UK and Ireland.
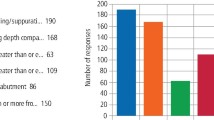
Results All responding schools (response rate of 60%) provided implant training for their students. The teaching is mainly delivered in lecture-based or phantom head room settings. The majority of schools provided direct clinical experience in procedures relating to peri-implant maintenance, although in some schools it was stated that not every student was guaranteed to receive such experience. In 86% of schools, students gained experience in oral hygiene and scaling, while 71% and 64% provided experience of non-surgical management of patients with peri-implant mucositis and peri-implantitis, respectively. The main barrier to developing the implant programme was an insufficient number of suitable cases.
Conclusions Although all responding schools provide implant training, the overall findings show that further development and improvement of implant teaching in dental hygiene and therapy schools within the UK and Ireland is required, particularly with respect to direct clinical experience. This will ensure that newly qualified dental hygienists and therapists are sufficiently prepared for managing implant patients in their clinical practice.
Similar content being viewed by others

Key points
-
Provides an overview of teaching trends in implant dentistry within dental hygiene and therapy schools in the UK and Ireland.
-
Identifies potential areas for improvements in implant teaching.
-
Discusses the challenges involved in developing and incorporating implant education into the curricula.
Introduction
In the UK, it has been acknowledged that effective use of skill mix in dental teams is part of the solution to meeting the nation's changing oral healthcare needs and this has resulted in a drive to restructure the UK dental workforce.1 The General Dental Council's document Corporate Strategy 2016-2019 sets out plans for dental care professionals (DCPs) to play a greater role in the provision of dental care.2 Part of the strategy includes dental hygienists and therapists (DH/Ts) being granted prescribing powers, which has now been implemented by the General Dental Council (GDC) and is known as 'direct access'. However, this has been slow to arrive due mainly to legislative restrictions and interfacing with NHS regulations.3 Direct access came into effect from 1 May 2013, and enables dental hygienists and therapists (DH/Ts) to carry out their full scope of practice without needing a prescription from a dentist.3 At present, this is optional and those who choose to take advantage of this opportunity must be sure that they are trained and competent to carry out any of the tasks they undertake and indemnified to do so.4 In the future, it is likely that more DH/Ts, if not all, will take up the opportunities of direct access. There is the anticipation that these changes will allow dentists to place emphasis on other procedures, while DH/Ts continue with their entire scope of practice.1,2 Findings from Evans et al. in 2007, showed that 43% of dentists' clinical time is taken up by activities that could be undertaken by DH/Ts.5 If full prescribing powers were taken up by DH/T cohorts, it has been calculated that this could result in 58% of dental clinical time being provided by DH/Ts.5 With the forecast that demand for DH/Ts will rise and that DH/Ts will play a greater role in the dental workforce, it is more than likely that this will have an impact on the training and education requirements of DH/Ts.2,6
In the context of implant dentistry, considering the increasing popularity of such treatment modalities, which is reportedly worth a global market value of $3.5 billion Swiss Francs (approximately £2.7 billion) as of 2016, and the changes in dental workforce structure, it is foreseeable that DH/Ts will become more exposed to the issues of peri-implant maintenance and potentially they will encounter and be required to act upon (identify and refer) dental implant diseases.7 Currently, the GDC expects DH/Ts in the UK to be competent at maintaining peri-implant health and describing the risks related to dental implant therapy as published in the document Preparing for practice: Dental team learning outcomes for registration in 2015.8 It follows that there is a necessity for DH/T schools within the UK to provide the relevant implant training, in order to fulfil the standards set by the GDC as well as to best prepare students for such future changes to their clinical practice on qualification.
Currently, there are limited data on the teaching trends of implant dentistry in DH/T schools across the UK and Ireland. Knowledge on the current status of implant education will help inform various organisations, specifically educational providers, regulators and policy makers as to whether curriculum requirements set by the GDC are adequate and being met. This information will provide guidance for any potential future changes and developments that are required in implant training and education for DH/T students. This survey, therefore, aimed to determine the status of current implant education within DH/T schools within the UK and Ireland.
Materials and methods
An online questionnaire, consisting of 31 questions was developed to assess the level of teaching in implant teaching at DH/T schools across the UK and Ireland. The online questionnaire was constructed using software developed by Bristol University (Bristol Online Surveys). Both 'open' and 'closed' style questions were included. The questionnaire was developed and pre-piloted within Cardiff Dental School. This was subsequently amended, reviewed and approved by the Cardiff Dental School research ethics committee (Reference No: 1703a).
In March 2017, an email was sent to the programme directors of the 23 UK and Irish DH/T schools, providing them with the hyperlink for the questionnaire, together with a participant information sheet. Topics included:
Current level of teaching of dental implants at their institution
Planned changes in this teaching during the subsequent 12-month period
The respondent's perception of what dental implant training/education for dental hygiene and therapy students would be like at their institution in five years' time.
Reminder emails were sent at two and four weeks from the initial email. Due to a low response rate, a further postal questionnaire was sent. After a six-month reply period, the data were collated and examined. The Bristol Online Surveys software programme permitted collection and analysis of the data. Descriptive statistics are reported.
Results
Completed questionnaires were received from 14 out of 23 (60%) DH/T schools. It is understood that the responses were completed by the programme director or by a senior academic with teaching responsibilities relating to implant dentistry.
Current teaching
All responding schools (100%) reported that they provided training in implant dentistry for their undergraduates. In addition, all had requirements within their curricula for undergraduates to receive implant training. The time at which implant training was introduced varied. Eleven schools (50%) stated that implant training occurred during the second year. Implant teaching occurred in the first year for 23% of schools and in the third year in the remaining 27% of schools.
Respondents reported that the school of hygiene and therapy primarily provided implant teaching (56%), while seven schools (39%) indicated that the restorative department provided teaching, and one school (5%) stated that their oral and maxillofacial surgery staff provided teaching. Table 1 describes the mode of delivery of dental implant teaching to dental undergraduates. Table 2 summarises the responses of schools when asked what topics were covered in their implant programme. 'Other' topics included 'peri-implant diseases' and 'the role of the dental hygienist and therapist in the maintenance of implants'.
The number of sessions devoted to the implant programme varied between schools. Nine schools (57%) devoted one to three sessions, five schools (36%) assigned four to six sessions and one school (7%) provided more than six sessions. Four schools had recommended textbooks and references on implants as part of the programme's reading lists. These are listed in Box 1. One school stated that they recommended mostly contemporary journal articles, which are updated every year. Respondents were also asked to list what educational resources they had available to students relating to dental implants and these are listed in Table 3.
Schools were asked whether students observed live implant surgery and restorative implant procedures. In two of the 14 schools (14%), students observed live implant surgery. In three schools (21%), students observed restorative implant procedures. In the majority of schools, students did not observe such procedures. Schools were also asked whether students gained direct clinical experience relating to peri-implant maintenance. The responses are shown in Table 4. Four schools commented that not all students were guaranteed to receive direct clinical experience and this would be dependent on the availability of suitable cases. Schools that offered direct clinical experience in non-surgical management of peri-implant diseases were also asked to state the types of implant restorations that students treated. The results are shown in Table 5.
Three schools (30%) provided measures of student competence for non-surgical management of peri-implant mucositis and two schools (22%) provided competence testing for peri-implantitis management. Tables 6 and 7 describe the modes of instrumentation used by dental schools for non-surgical supragingival and subgingival debridement of dental implants. Two out of 14 schools (14%) indicated that they received support from implant companies for the provision of implant training. The companies involved were Dentsply (67%) and Biomet 3i (33%). One school commented that they received resources from the trade for hands-on clinical simulation.
Future plans for dental implant training: next 12 months
Seven schools responded when asked whether there were any plans to introduce direct clinical experience in non-surgical therapy for the management of peri-implant diseases (that is, peri-implant mucositis and peri-implantitis). One school stated that they planned to introduce such teaching in the next 12 months.
Current challenges to the provision of implant training
Each dental school was asked what challenges there have been to introducing/developing implant teaching into the dental hygiene and therapy programme. The responses are shown in Table 8.
Future predictions for implant teaching: five years' time
When asked if there will be clinical requirements relating to non-surgical therapy of peri-implant diseases for students within the next five years, seven schools (50%) felt this would be the case, while the other seven (50%) felt that this would not be the case.
Discussion
Contrary to undergraduate dentistry programmes of study, there exists very little data on implant teaching in DH/T schools across the UK and worldwide. It has, therefore, been difficult to evaluate and discuss the current status of implant education within the dental hygiene and therapy curricula. Some US data by Ward et al. in 2012 revealed that in a survey of 213 dental hygienists, 51% of respondents did not receive any training on implant care while attending dental hygiene school.9 These findings do not directly assess implant education and are insufficient data from which to draw any conclusions.
In general, litigation in UK dentistry has risen substantially. The 'Riskwise' publication by the indemnity organisation Dental Protection, in 2015, reported an increase in the number and frequency of complaints relating to implants in the UK.10 In 2015, implants accounted for 28.8% of UK claims by value, the second highest claim (periodontal cases constituted 44.7%). Multiple factors contributing to this rise included inadequate consent, treatment planning and record keeping, unrealistic patient expectations together with inadequate risk assessment, inadequate post-treatment monitoring and aftercare, and lack of experience in the relevant procedures involved. In addition, a higher number of cases (5.5% claims by value) relating to peri-implantitis and peri-implant mucositis have been reported and there is growing consensus that this is likely to increase in the future. Notably, it was found that among these claims, clinicians that did not place or restore the implants originally became subject to claims and complaints for alleged supervised neglect of implant cases. Clearly ignorance of dental implant methodologies is not appropriate, this emphasises further the necessity of DH/T training programmes to ensure clinicians are adept at recognising health and disease of dental implants upon qualification.
So concerning was this issue of peri-implantitis, that it was raised by Baroness Gardner of Parkes at the House of Lords in July 2014.11 It was stated that 'peri-implantitis is now a serious possible consequence of implantation' and highlighted that the 'Royal College of Surgeons points out that long-term assessment and maintenance need to be assured'. It is clear that this worrying situation further emphasises the need to implement structured and comprehensive implant training at a trainee level, in order to ensure patient safety and minimise the risk regarding claims and complaints against dentists and DCPs. Considering the popularity of implant treatment, it is important to know whether DH/Ts are receiving the necessary implant training, as they will likely be increasingly involved with the provision of peri-implant maintenance.
In this study, an electronic survey provided a simple means of data collection. However, due to a lower response rate, follow-up postal questionnaires were subsequently distributed. The final response rate of 60% was still slightly lower in comparison to other dental questionnaires.12 It is possible that the questionnaire was not seen as a priority by participants or that the response rate was otherwise an indication of questionnaire fatigue to this form of information gathering. Interpretation of this survey data must, therefore, take into account the lower number of respondents and the risk of interpretation bias.
It is positive to see that all responding DH/T schools provided implant training for their students and recognised that there were curriculum requirements to provide such training. The GDC's publication Preparing for Dental Practice: Dental learning outcomes for registration expects DH/Ts to have the competence to 'describe the risks related to dental implant therapy and manage the health of peri-implant tissues'.8 Most schools provided implant training for their undergraduates during the second year. There would be opportunity in this respect for students to develop the necessary core knowledge and skills before approaching a subject that is more complex. Primarily, the school of hygiene and therapy department (56%) provided implant teaching with some involvement by the restorative, and oral and maxillofacial surgery specialties. A multidisciplinary approach in teaching should be encouraged to enhance students' learning and understanding of the subject.
Theory and practical study are both important aspects for the acquisition of skills and knowledge necessary for students to fulfil the DH/T learning outcomes in implant dentistry. A number of methods have been employed to deliver theoretical teaching and there appears to be no difference in the effectiveness of one method over another.13 Where practical skills are concerned, clinical hands-on training provides a safe and controlled environment for students to develop and demonstrate competence in practical procedures before treating patients.
Findings revealed that implant teaching was delivered mainly in lecture-based (100%) and phantom head hands-on (71%) settings, both of which are considered effective pre-clinical teaching modalities. Most schools, but not all, covered core topics in their implant programme which included peri-implant maintenance (93%), implant surgery (86%), treatment planning (71%), and implant restoration (71%). To fulfil the GDC's curriculum requirements, however, it would seem reasonable to expect every school to cover these topics. Clinical learning is best achieved by direct clinical exposure to patients and dental implants in a clinical setting. Only very few schools offered students the opportunity to observe live implant surgery (14%) and restorative implant procedures (21%). Observing implant procedures allow students to see first-hand the complexities associated with implant placement and restoration, especially given that these procedures are out with the scope of DH/T practice. Certainly, if students are to fully appreciate the impact these procedures can have on the outcome of treatment and future implant maintenance, it would seem necessary for all schools to provide observation experience for their students.
Although the majority of schools provided students with direct clinical experience in procedures related to 'managing the health of peri-implant tissues' (a GDC curriculum requirement), some schools stated that not all students were guaranteed to receive such experience. Preventive care, stabilisation of the periodontal condition before implant placement, and non-surgical management of peri-implant diseases encompass the key clinical components of managing the health of peri-implant tissues. Fewer schools (64%) offered clinical experience in non-surgical management of peri-implantitis. The cases that were treated included mostly single unit and edentulous removable scenarios. A limited number of schools provided measures of competence for the management of peri-implant diseases. The most common instruments used for non-surgical supra- and sub-gingival debridement were gold or titanium curettes, ultrasonic with plastic insert tips and graphite curettes. Ultrasonic with metal tips and mechanical instrumentation using materials harder than titanium may damage the implant surface and make it susceptible to biofilm formation, thereby increasing susceptibility to peri-implantitis.14 Guidelines published by the Association of Dental Implantology in 2012 recommends the use of titanium scalers for mechanical debridement and advises against the use of plastic instruments due to reduced efficiency in removing subgingival plaque from implant surfaces.15 Interestingly, a small number of schools indicated that they used plastic-coated scalers, stainless steel curettes and ultrasonic devices with stainless steel tips for mechanical debridement of implants. This study shows that schools teach a variety of methods, which reflects the poor evidence base in existence for the optimum method of removing the biofilm from dental implants.
Incorporating additional implant teaching into the curricula is challenging. However, it is essential that schools keep pace with current developments and remain evidence-based. The overriding challenge faced by most was the lack of suitable cases, which is an interesting contrast to dental undergraduate schools whereby funding, lack of available time, and staff training were the main challenges.16 Increasing the number of cases for the implant programme may be overcome by establishing stronger relationships with other departments that provide implant treatment or receive implant referrals. Although only one school stated that funding was a challenge, there is likelihood that in the future, increasing demands to provide implant training may place funding pressures on schools. Currently, only two schools received support from implant companies for the provision of implant training. Provided that educational content is led by academic institutions and not driven by commercial pressures, obtaining sponsored educational resources from implant manufacturers may alleviate funding pressures related to the provision of clinical implant training.
Despite the majority of schools providing implant training, the overall findings show that further development and improvement of implant teaching in DH/T schools is required. There is particular concern that not every school is providing students with direct clinical experience in the clinical components required to be competent at 'managing the health of peri-implant tissues'. It is interesting that there was divided opinion among schools when asked to predict if there will be clinical requirements relating to non-surgical therapy of peri-implant disease for students in five years' time. Given the increasing trends in the use of implants, it is in the authors' opinion that such requirements should already be an essential requisite in the implant curricula. There is also the worry that not every student is guaranteed to receive direct clinical experience in implant training, which can be considered a fundamental component for meeting the GDC's curriculum requirements.
To the authors' knowledge, this is the first survey to focus on this particular topic and there are no previous studies or data to compare with other countries. The results shown in this survey are vastly different from the findings relating to implant education for dental undergraduate students. Therefore, it is necessary that this survey be repeated in five years to assess implant education trends specific to dental hygiene and therapy training, in order to determine whether further improvements to implant education within DH/T schools are necessary to meet the expectations of the GDC.
Conclusions
Although all responding schools provide implant training, the overall findings reveal that the amount of training is varied. Further development and improvement of implant teaching is required, particularly with respect to direct clinical experience, in order to ensure that newly qualified dental hygienists and therapists are sufficiently prepared for managing implant patients independently in their clinical practice. It is hoped that the findings of this survey will help inform educational providers of the current teaching trends so as to promote standardisation, improvement and development of the implant curricula across UK and Ireland.
References
Cowpe J, Barnes E, Bullock A. Skill-mix in dental teams in Wales. Vital 2013; 10: 38-43.
General Dental Council. The General Dental Council Corporate Strategy 2016-2019. 2015. Available at https://www.gdc-uk.org/api/files/2015-11-04_4.1%20GDC%20Corporate%20Strategy%20App%201%20Clean.pdf (accessed April 2019).
General Dental Council. Direct Access. 2013. Available at www.gdc-uk.org/professionals/standards/direct-access (accessed April 2019).
British Society of Dental Hygiene and Therapy. Direct Access - Guidance to BSDHT Members. 2016. Available at http://www.bsdht.org.uk/resources-app/direct-access-guidance-to-bsdht-members (accessed April 2019).
Evans C, Chestnutt I G, Chadwick B L. The potential for delegation of clinical care in general dental practice. Br Dent J 2007; 203: 695-699.
Centre for Workforce Intelligence. Securing the future workforce supply: Dental care professionals stocktake. 2014. Available at https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/507376/CfWI_Dental_care_professionals_stocktake.pdf (accessed April 2019).
Straumann Group. Markets: Leadership in a CHF 7 billion market. 2016. Available at www.straumann.com/content/dam/media-centre/group/en/documents/annual-report/2016/Markets.pdf (accessed April 2019).
General Dental Council. Preparing for practice: Dental team learning outcomes for registration. 2015. Available at https://www.gdc-uk.org/api/files/Preparing%20for%20Practice%20(revised%202015).pdf (access April 2019).
Ward S T, Czuszak C A, Thompson A L, Downey M C, Collins M A. Assessment and maintenance of dental implants: clinical and knowledge-seeking practices of dental hygienists. J Dent Hyg 2012; 86: 104-110.
Dental Protection. Riskwise: An increasing number of costly claims involving dental implants and periodontal disease. 2015. Available at https://www.dentalprotection.org/docs/librariesprovider4/default-document-library/riskwise-uk.pdf?sfvrsn=0 (accessed April 2019).
Hansard. Baroness Gardner of Parkes asked for Health: Dental Implants - Question for Short Debate. 2014. Available at https://hansard.parliament.uk/Lords/2014-07-23/debates/14072388000071/HealthDentalImplants (accessed April 2019).
Tan R T, Burke F J T. Response rates to questionnaires mailed to dentists. A review of 77 publications. Int Dent J 1997; 47: 349-54.
Gopinath V, Nallaswamy D. A Systematic Review on the Most Effective Method Teaching Dentistry to Dental Students Compared to Video Based Learning. Am J Educ Res 2017; 5: 63-68.
Matarasso S, Quaremba G, Coraggio F, Vaia E, Cafiero C, Lang N P. Maintenance of implants: an in vitro study of titanium implant surface modifications subsequent to the application of different prophylaxis procedures. Clin Oral Implants Res 1996; 7: 64-72.
Association of Dental Implantology. A Dentist's Guide to Implantology. 2012. Available at www.adi.org.uk/resources/guidelines_and_papers/dentist_guide (accessed April 2019).
Chin J S, Lynch C D, Rees J, Locke M, Thomas M B M, Addy L D. Teaching of implant dentistry in undergraduate dental schools in the UK and Ireland. Br Dent J 2018; 225: 763-768.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chin, J., Addy, L., Rees, J. et al. Teaching of implant dentistry in dental hygiene and therapy schools in the UK and Ireland. Br Dent J 226, 692–696 (2019). https://doi.org/10.1038/s41415-019-0259-x
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-0259-x
- Springer Nature Limited