
Abstract
Infraocclusion is a term used to describe a tooth which has stopped its relative occlusal growth into the arch after the period of active eruption; as a result, the tooth becomes depressed below the occlusal plane. Although many aetiological mechanisms have been proposed, ankylosis is considered the primary cause of infraocclusion. Complex cases benefit from multidisciplinary management. This paper concentrates on the diagnosis and management of infraoccluded second primary molars, without permanent successors and without significant malocclusion, and provides clinicians with a treatment decision tree to aid in treatment planning.
Similar content being viewed by others


Key points
-
Improves knowledge on how to diagnose infraoccluded primary teeth.
-
Demonstrates how to manage cases of early ankylosis in young patients with remaining growth potential with deciduous dental extractions.
-
Presents a treatment algorithm as guidance for these clinical situations.
-
Provides advice on when to refer patients in complex malocclusions.
Introduction
Infraocclusion is a term used to describe a tooth which has stopped its relative occlusal growth into the arch after the period of active eruption; as a result, it becomes depressed below the occlusal plane.1,2 Traditionally, the term 'submerged' was used to describe these teeth, however, numerous other terms have also been used in the literature, and some examples are listed in Box 1. The authors prefer the term infraocclusion and have used it throughout this paper.
The prevalence of infraoccluded primary molars varies between studies. Bjerklin et al. (1992) stated that 55% of retained primary second molars show some degree of infraocclusion.3 Kurol (1981), in a study of 1,059 Swedish children, reported the prevalence figure at 8.9%,4 however other studies have given figures between 1.3% and 38.5%.5,6 In all of these studies, the subjects had a mixture of permanent successor's presence or absence.
Despite the wide variation between population groups, many studies have identified a familial occurrence of infraocclusion with a significantly higher incidence between siblings.4,7,8,6,9 The distribution based on gender is reported to be equal.6,10,11 Andraesen et al.12 stated that infraocclusion is most often registered at the interval of 6-11 years,5,6,10 but has been described in patients as young as three-years-old.6,13,14
This phenomenon tends to occur bilaterally1 with the most commonly affected teeth being the mandibular primary molars.4,6,10 The occurrence of infraocclusion can occur in the presence or absence of a permanent successor tooth. There are no clear guidelines to the general dental practitioner (GDP) on the management of infraoccluded primary molars when the adult premolar is absent; which, importantly, is the most common presentation of mild hypodontia, as second premolars are often developmentally absent. Clinicians can often find the decision-making challenging on whether to extract the infraoccluded teeth or to retain them. The aim of this article is to give a brief overview of the current literature surrounding infraoccluded primary molars and to provide clinicians with an understanding of treatment options available when managing infraoccluded second primary molars with absent permanent successors.
Aetiology
Although many aetiological mechanisms have been proposed (Box 2), ankylosis is considered the main cause of infraoccluded primary molars.1,4,15,16 Noble et al. (2007) describes ankylosis of the infraerupted primary molar as one that has 'stopped its vertical movement relative to others along the occlusal plane such that marginal ridges are not at the same height as adjacent teeth'.17 This is due to failure of the periodontal ligament to separate cementum and dentine from the bone during resorption, causing fusion of the tooth to alveolar bone.10 This results in the primary tooth remaining static while the eruption of adjacent teeth continues with vertical growth and occlusal development.11,18 Two main theories have been proposed to explain why infraoccluded primary molars become ankylosed.
The first of these theories considers local factors as the main cause and the second is based on genetic factors, although, to date, no genes have been identified. Biederman suggested that ankylosis may be due to a change in metabolism caused by local disturbances in the periodontal ligament.19 Bone turnover is a complex process involving the close interaction of osteoclasts and osteoblasts along with periodontal ligament cells.20 Studies have identified that disturbances in this process could also cause tooth ankylosis.20
The second theory based on genetic factors is well supported. A study of monozygotic twins, and another study assessing the prevalence of infraoccluded teeth in different races, have shown evidence of a genetic aetiology and familial occurrence of infraoccluded teeth.18 It has been suggested that 'infraocclusion and other dental anomalies including those of shape, texture, number, and eruption may all represent microsymptoms of an inheritable disturbance because of a general disruption of the tooth developmental structures'.18
Although these theories do have evidence to support them within the literature, the exact cause of ankylosis of primary molars remains unknown. Other reported, but less common causes of infraocclusion in the literature are listed in Box 2. For teeth with permanent successors, the ankylosed condition of the primary tooth usually, but not always, disappears concurrently with the physiological resorption process, which is delayed, indicating that ankylosis is usually a transient phenomenon.21 However, there are cases where deciduous molars with a permanent successor remain ankylosed.22
Clinical features
Developmental anomalies are often identified by the GDP during routine examination21 and infraocclusion of primary teeth is one such condition that is usually diagnosed on clinical examination. As the name signifies, typically, the infraoccluded tooth appears depressed below the occlusal plane at varying levels of severity (Fig. 1).4,6,10

Severe infraocclusion of 65 and 75. The teeth are significantly depressed below occlusal plane almost to gingival level
Other clinical findings that can be associated with infraoccluded teeth are listed in Box 3 (which includes references to Figure 2, Figure 3 and Figure 4). Tipping of adjacent teeth is often noted, owing to the tension in the transeptal fibres between the infraoccluded and non-infraoccluded teeth, as the infraoccluded tooth sinks below the occlusal plane.23 A high-pitched percussive tone has been described due to the ankylosis of the tooth to the surrounding bone, but this is a largely a subjective measure as it only occurs when at least 20% of the root surface is ankylosed.21 Other clinical features include: an apical position of the gingival margin; overeruption of opposing teeth; lateral open bites; and incomplete alveolar process development.24 Root resorption detected radiographically without expected increase in mobility may occur, which suggests ankyloses of the tooth.1 A loss of mobility with infraoccluded teeth occurs when more than 10% of the root becomes ankylosed.21

Tipping of 24 distally adjacent to infraoccluded 65

Overeruption of tooth 15 against infraoccluded 85

a) Occlusal view shows a horizontal bony defect; b) right side buccal view shows a vertical defect in the same patient
Use of radiography in management of infraoccluded primary molars
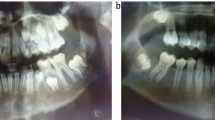
The presence of a non-mobile primary molar with a pronounced degree of physiological root resorption may be a sign of ankylosis and warrants further investigation. The use of radiographs enables the clinician to identify if there is a successor present; in addition, radiographs facilitate the diagnosis of dental pathology including caries and root resorption. Periapical radiographs may show periodontal ligament space obliteration which is an indicator of ankylosis and differences in occlusal heights can also be seen. Other features that can be seen radiographically include oblique interproximal bone levels 'bone notching', that slope down towards the infraoccluded tooth (Fig. 5).

Orthopantomogram showing 3 quadrants of infraoccluded teeth with evidence of ankylosis at the apex, lack of alveolar development and bone notching in between the deciduous mandibular right second molar and the first permanent molar
However, conventional radiographs only offer a two-dimensional view of the infraoccluded tooth and, given that ankylosis is microscopic,25 it is unsurprising that radiographic interpretation is limited. Some histological studies including Raghoebar et al.21 and Henderson26 have reported that most ankylosed molars had osteoid tissue deposited in the furcation area. Thornton et al.27 and Krakowiak10 found that teeth without successors showed ankylosis in the vicinity of the apex. However, despite these conclusions, radiographic presentation is of limited value to the majority of clinicians.
Cone beam computer tomography (CBCT) scans have shown that there is obliteration of the periodontal ligament in cases of ankylosis.28 CBCT is also useful in managing complex cases requiring the surgical removal of infraoccluded teeth, as it enables the surgeons to identify and localise the anatomical structures such as the inferior dental nerve.24 However, CBCT should only be used in selective cases where the benefit outweighs the risks associated with this technique.
Classification
There are numerous classification systems in the literature. Two most frequently used are Kjaer et al. (2008), where primary molar eruption is classified according to the distance from the occlusal level of the primary molars to the adjacent teeth in millimetres.12 The other frequently used classification is by Brearley et al. (1973), as shown in Table 1.6 For the purpose of this article, the authors have chosen to use the Brearley classification.
Prognosis of infraoccluded molars
Studies have shown that ankylosed mandibular and maxillary second primary molars have a better prognosis than ankylosed first primary molars.29 Due to the increased incidence of permanent second molar absence, there is more available literature regarding their longevity. Bjerklin et al. (2000) analysed 41 subjects longitudinally, from age 11 years into adulthood, who had all retained lower second primary molars, of which 55% had some degree of infraocclusion.29 Out of 59 teeth in 41 subjects, only seven retained primary second molars were lost, of which none were lost after the age of 20.30 This suggests that if primary molars are retained past the age of 20, then the prognosis is good and other studies have drawn a similar conclusion.29
As previously stated, decision making around infraoccluded primary molars can be complex and confusing. The next part of this paper provides a simplified summary of the literature and a flow chart to aid clinicians in treatment planning cases of infraoccluded primary molars with missing permanent successors.
Treatment planning
Management of infraoccluded teeth is influenced by several factors such as timing of diagnosis, age of the patient, type and degree of malocclusion, the degree of ankyloses and whether there is a permanent successor present. Management of pathology-free ankylosed primary second molars with a missing permanent successor in a child without any significant malocclusion depends on the timing of diagnosis. Mildly ankylosed teeth, diagnosed before the child's pubertal growth spurt, should be monitored biannually to ensure that the ankylosis is not getting worse. If the ankylosis worsens over time or is diagnosed as severe at the time of diagnosis, the clinicians should consider extracting the tooth, ideally before the child's growth spurt. This is done in order to avoid a significant vertical bone defect.31 This will prevent greater challenges in future management of these cases where continued infraocclusion results in a lack of alveolar bone development.
Pathology-free mildly ankylosed primary molar teeth with missing underlying permanent successor that are diagnosed after the child's growth spurt could be retained. Progression of infraocclusion is shown to be slower in children aged 15-17-years-old with a mean increase of 0.5 mm per year.32 However, it is important to retain the integrity of the occlusal table. The infraoccluded primary molar could be built up to the correct occlusal plane with direct composite or with an indirect restoration like a ceramic or composite onlay. An onlay may be more suitable to build up to the occlusal table and establish a contact point with the adjacent first premolar.33 The primary molars could also benefit from placement of a preformed metal crown (PMC); which prevents tipping of the adjacent teeth, restores the occlusion to the correct height and prevents overeruption of the opposing teeth.34 Clinicians must be careful when selecting the size of the PMC, as PMCs have the risk of being oversized and this may compromise the leeway space.34 These treatment strategies also act as alveolar ridge maintainers in children, should this tooth need to be extracted and restored in the future with a fixed/removable prosthesis.34
There is often a restorative challenge in replacing lower second deciduous molars, as the mesiodistal width of the tooth is greater than a premolar width. Some clinicians advocate interproximal reduction (IPR). This is carried out using either hand files, rotary files or discs, and over a few appointments removes up to 2.5 mm of interproximal width. This procedure must be undertaken with caution, as the relatively large pulp horns place the primary teeth at a risk of pulpal inflammation and could stimulate premature root resorption and sensitivity.34 In addition, the discing of primary molars may alter contact point height, which leads to food packing and increases caries risk. However, there is a lack of long-term studies on retained second primary molars that have been reduced with IPR,34 therefore it should be used with caution in selected cases.
Pathology-free severely ankylosed primary molars with missing underlying permanent successor that are diagnosed after the pubertal growth spurt often need to be referred to secondary care services. Guidance can be sought from an orthodontist regarding the timing of extraction of the infraoccluded primary molar and if orthodontic space closure would be possible.34 Early removal of the infraoccluded molars is often required and facilitates efficient tooth movements.
A majority of severely infraoccluded teeth need to be surgically extracted, which may necessitate the use of general anaesthesia in anxious children. Concerns involved with extraction of severely ankylosed primary second molars is the potential alveolar bone loss, which could be critical if the future management plan includes an implant-supported prosthesis.35 Ostler et al. and Kokich et al. showed that 25% of the bucco-lingual width would be lost in the first three years, post-extraction of mandibular second primary molars.35,36 Potentially, ridge preservation techniques could be considered to maintain soft and hard tissue volume. Sandor et al. (1993) described a technique to place coral granules in the primary second molar extraction site,37 which had a 93.5% success rate in preserving the alveolar process and meant that implants were placed without the need for bone grafting.37 An alternative ridge preservation technique described by Smalley involves decoronating the crown of the primary second molar, leaving the roots within the alveolus.38 This technique is used for ankylosed primary molars where a traumatic surgical extraction would be required, resulting in significant bone loss. The decoronation technique helps to preserve the bone until an implant can be placed in the future.38
When assessing the patient orthodontically, lower incisor position can influence the treatment plan and the decision to extract or maintain the retained primary molars. If the lower incisors are at the correct angulation, then space closure should be avoided as excessive retroclination can be detrimental to the patient's profile. In addition, patients with minimal crowding, deep overbites, reduced anterior face height and flat mandibular plane angles are often treated with a non-extraction approach.34 In patients with these non-extraction characteristics, providing the roots of the mandibular second molars are favourable with mild or no infraocclusion present, then these teeth should be retained and maintained with a fixed prosthesis such as a ceramic onlay or full coverage crown. However, if the ankylosis is severe then extraction and space maintenance or closure may be indicated.34
In patients where the space left by the extraction of the infraoccluded second molar would be too large to be closed orthodontically, then extraction of the infraoccluded molar followed by implant placement is a long-term treatment option to consider. The benefits of an implant-retained prosthesis having a reliable long-term solution needs to be weighed against the longer treatment times, surgical operation, higher treatment fees and ongoing costs for patients.34
If the space is not adequate for restorative or implant rehabilitation, then orthodontists can place temporary anchorage devices to help protract posterior teeth to avoid lower incisor retroclination and eliminate the need for restorative replacement.39 Excessive lower incisor retraction would compromise facial aesthetics in these cases.34
There is lack of clear guidance and information to enable GDPs to manage cases of infraocclusion of primary molars in practice, taking account of the aforementioned scenarios. The authors propose a treatment tree (Fig. 6) that can aid in treatment planning cases of infraoccluded primary molars without permanent successors and without any associated significant malocclusion. The decision tree cannot be fully evidence-based, given the small volume of research in this area, and so it is based on the authors' experience. Complex cases of infraocclusion with or without significant malocclusions would benefit from a multidisciplinary specialist input, and referral to orthodontics, restorative and paediatric dentistry would be prudent.

A treatment algorithm for cases of infraoccluded primary second molars without permanent second premolar successors and without significant malocclusion
Conclusion
Early diagnosis of an infraoccluded molar is essential to avoid common problems associated with this clinical scenario. The treatment modalities depend on a number of factors including age of the patient, presence of a permanent successor, the time of diagnosis in relation to a patient's growth spurt, and the malocclusion present. Complex cases would benefit from multidisciplinary input; however, in a majority of simple cases, the given decision tree which is based on the authors' experience would aid clinicians in formulating a suitable treatment plan.
References
Ekim S L, Hatibovic-Kofman S. A treatment decision-making model for infraoccluded primary molars. Int J Paediatr Dent 2001; 11: 340-346.
Via W F Jr. Submerged deciduous molars: familial tendencies. J Am Dent Assoc 1964; 69: 127-129.
Bjerklin K, Kurol J, Valentin J; Ectopic eruption of maxillary first permanent molars and association with other tooth and developmental disturbances. Eur J Orthod 1992; 14: 369-375.
Kurol J. Infraocclusion of primary molars: an epidemiologic and familial study. Community Dent Oral Epidemiol 1981; 9: 94-102.
Andlaw R J. Submerged deciduous molars: a review, with special reference to the rationale of treatment. J Int Assoc Dent Child 1974; 5: 59-66.
Brearley L J, McKibben D H Jr. Ankylosis of primary molar teeth. I. Prevalence and characteristics. ASDC J Dent Child 1973; 40: 54-63.
Dewhurst S N, Harris J C, Bedi R. Infraocclusion of primary molars in monozygotic twins: report of two cases. Int J Paediatr Dent 1997; 7: 25-30.
Douglass J, Tinanoff N. The aetiology, prevalence, and sequelae of infraclusion of primary molars. ASDC J Dent Child 1991; 58: 481-483.
Mueller C T, Gellin M E, Kaplan A L, Bohannan H M. Prevalence of ankylosis of primary molars in different regions of the United States. ASDC J Dent Child 1983; 50: 213-218.
Krakowiak F J. Ankylosed primary molars. ASDC J Dent Child 1978; 45: 288-292.
Biederman W. The incidence and aetiology of tooth ankylosis. Am J Orthod 1956; 42: 921-926.
Kjaer I, Fink-Jensen M, Andreasen J O. Classification and sequelae of arrested eruption of primary molars. Int J Paediatr Dent 2008; 18: 11-17.
Steigman S, Koyoumdjisky-Kaye E, Matrai Y. Submerged deciduous molars in preschool children: an epidemiologic survey. J Dent Res 1973; 52: 322-326.
Rune B. Submerged deciduous molars. Odontol Revy 1971; 22: 257-273.
Andlaw R J. Submerged deciduous molars: a prevalence survey in Somerset. J Int Assoc Dent Child 1977; 8: 42-45.
Leonardi M, Armi P, Baccetti T, Franchi L, Caltabiano M. Mandibular growth in subjects with infraoccluded deciduous molars. Angle Orthod 2005; 75: 927-934.
Noble J, Karaiskos N, Wiltshire W A. Diagnosis and management of the infraerupted primary molar. Br Dent J 2007; 203: 632-634.
Teague A M, Barton P, Parry W J. Management of the submerged deciduous tooth: I. Aetiology, diagnosis and potential consequences. Dent Update 1999; 26: 292-296.
Biederman W. The problem of the ankylosed tooth. Dent Clin North Am 1968; 409-424.
Curl L, Tan C W, Dreyer C W, Samspson W. A qualitative investigation of RANKL, RANK and OPG in a rat model of transient ankylosis. Aust Orthod J 2014; 30: 143-151.
Raghoebar G M, Boering G, Stegenga B, Vissink A. Secondary retention in the primary dentition. ASDC J Dent Child 1991; 58: 17-22.
Tieu L D, Walker S L, Major M P, Flores-Mir C. Management of ankylosed primary molars with premolar successors: a systematic review. J Am Dent Assoc 2013; 144: 602-611.
Becker A, Karnei-R'em R M. The effects of infraocclusion: Part 1. Tilting of the adjacent teeth and local space loss. Am J Orthod Dentofacial Orthop 1992; 102: 256-264.
Arhakis A. Boutiou E. Etiology, Diagnosis, Consequences and Treatment of Infraoccluded Primary Molars. Open Dent J 2016; 10: 714-719.
Santos L L. Treatment planning in the presence of congenitally absent second premolars: a review of the literature. J Clin Paediatr Dent 2002; 27: 13-17.
Henderson H Z. Ankylosis of primary molars. a clinical, radiographic, and histologic study. ASDC J Dent Child 1979; 46: 117-122.
Thornton M, Zimmerman E R. Ankylosis of primary teeth. J Dent Child 1964; 31: 120-126.
Fernandes M, de Ataide I, Wagle R. Tooth resorption part II - external resorption: Case series. J Conserv Dent 2013; 16: 180-185.
Bjerklin K, Bennett J. The long-term survival of lower second primary molars in subjects with agenesis of the premolars. Eur J Orthod 2000; 22: 245-255.
Altay N, Cengiz S B. Space-regaining treatment for a submerged primary molar: a case report. Int J Paed Dent 2002; 12: 286-289.
Sabri R. Management of over-retained mandibular deciduous second molars with and without permanent successors. World J Orthod 2008; 9: 209-220.
Kurol J, Thilander B. Infraocclusion of primary molars with aplasia of the permanent successor: A longitudinal study. Angle Orthod 1984; 54: 283-294.
Evans R D, Briggs P F. Restoration of an infraoccluded primary molar with an indirect composite onlay: A case report and literature review. Dent Update 1996; 23: 52-54.
Kennedy D B. Treatment strategies for ankylosed primary molars. Eur Arch Paediatr Dent 2009; 10: 201-210.
Ostler M S, Kokich V G. Alveolar ridge changes in patients with congenitally missing mandibular second premolars. J Prosthet Dent 1994; 71: 144-149.
Kokich V G, Kokich V O. Congenitally missing mandibular second premolars: Clinical options. Am J Orthod Dentofacial Orthop 2006; 130: 437-444.
Sandor G K, Kainulainen V T, Queiroz J O, Carmichael R P, Oikarinen K S. Preservation of ridge dimensions following grafting with coral granules of 48 post-traumatic and post-extraction dento-alveolar defects. Dent Traumatol 2003; 19: 221-227.
Smalley W M. Comprehensive Interdisciplinary Management of Dentitions with Missing and/or Abnormally Proportioned Teeth. In Cohen M (ed) Interdisciplinary Treatment Planning: Principles, Design and Implementation. New Malden: Quintessence, 2008.
Fines C D, Rebellato J, Saiar M. Congenitally missing mandibular second premolar: Treatment outcome with orthodontic space closure. Am J Orthod Dentofacial Orthop 2003; 123: 676-682.
Becker A, Shochat S. Submergence of a deciduous tooth: its ramifications on the dentition and treatment of the resulting malocclusion. Am J Orthod 1982; 81: 240-244.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hua, L., Thomas, M., Bhatia, S. et al. To extract or not to extract? Management of infraoccluded second primary molars without successors. Br Dent J 227, 93–98 (2019). https://doi.org/10.1038/s41415-019-0207-9
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-0207-9
- Springer Nature Limited
This article is cited by
-
Restorative dentistry clinical decision-making for hypodontia: retained primary molars
British Dental Journal (2023)