
Abstract
The heritability of intelligence or general cognitive ability is estimated at 41% and 66% in children and adults respectively. Many rare copy number variants are associated with neurodevelopmental and neuropsychiatric conditions (ND-CNV), including schizophrenia and autism spectrum disorders, and may contribute to the observed variability in cognitive ability. Here, we reviewed studies of intelligence quotient or cognitive function in ND-CNV carriers, from both general population and clinical cohorts, to understand the cognitive impact of ND-CNV in both contexts and identify potential genotype-specific cognitive phenotypes. We reviewed aggregate studies of sets ND-CNV broadly linked to neurodevelopmental and neuropsychiatric conditions, and genotype-first studies of a subset of 12 ND-CNV robustly associated with schizophrenia and autism. Cognitive impacts were observed across ND-CNV in both general population and clinical cohorts, with reports of phenotypic heterogeneity. Evidence for ND-CNV-specific impacts were limited by a small number of studies and samples sizes. A comprehensive understanding of the cognitive impact of ND-CNVs would be clinically informative and could identify potential educational needs for ND-CNV carriers. This could improve genetic counselling for families impacted by ND-CNV, and clinical outcomes for those with complex needs.
Similar content being viewed by others

Introduction
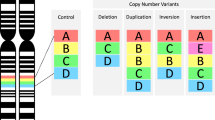
Heritability estimates for general cognitive ability (or intelligence) range from 41% in childhood to 66% in adults [1]. Different forms of genetic variation, common and rare, may contribute to cognition, such as loss of function or missense single nucleotide variants (SNV), single nucleotide polymorphisms (SNP), and copy number variants (CNV). To date 11,600 SNPs in 148 loci have been linked to cognitive ability, however each have very small effects [2]. Polygenic scores, which are the weighted sum of trait associated variants, account for only 4.3% of variance in cognition [2]. Cognitive ability may be further accounted for by rare structural variants of larger effect, such as CNV [3]. CNV refer to variation in chromosomal copy typically leading to a loss (deletion) or gain (duplication) of sections of DNA that may include one or many genes. They can be common or rare, defined based on their frequency in the population and may be inherited or arise de novo in the germline. While CNV are commonly found in the general population and often benign, they can also be pathogenic. There has been particular interest in investigating rare CNV in human health and disease since these are likely more deleterious due to increased selection pressure [4]. Recurrent CNV are deletions or duplications that occur at specific genomic regions frequently associated with incomplete penetrance and variable expressivity. Although their phenotypic impact is not fully understood, many rare recurrent CNV have been linked to neurodevelopmental and neuropsychiatric conditions (ND-CNV) and contribute to associated traits such as variability in cognitive ability.
CNV burden and effect sizes of deletions and duplications on cognition
Many CNV studies of cognition have focused on total CNV burden, defined as total length or number of base pairs impacted by a CNV [5, 6], and also numbers of affected genes in some studies [5, 7]. These studies examine unfiltered CNVs (i.e., they do not filter for neurodevelopmental-related CNV). Deletions and duplications are assessed either together or separately. CNV burden studies show mixed findings. Multiple general population studies suggest no effect of rare CNV burden, total number of CNV, or number of affected genes on general cognitive ability [3, 8, 9]. However, rare deletion burden has been shown to have a more deleterious effect in some studies in relation to IQ and components of cognition such as phonological working memory and selective attention [10, 11].
A recent meta-analysis of nine studies in clinical and population-based cohorts showed no association of CNV burden with intelligence quotient (IQ) [5]. Nor did they find association of burden and IQ within a subsequent analysis of a large cohort of psychosis patients and family members. Noteworthy, many of the clinical cohort studies included in the meta-analysis did show effects of rare CNV burden on cognition, although others have reported variable results [5, 12, 13]. Some of the discrepancies may be accounted for by differences between studies in the definition of rare CNV. Studies using a frequency cut-off of 1% for rare CNVs have reported associations more often than those using a 5% frequency cut-off [8,9,10]. Inadequate power and small sample size, particularly in clinical cohorts is also a factor.
An alternative to CNV burden is the use of constraint scores, e.g., “probability of being loss of-function-intolerant” (pLI). The pLI score classifies genes within CNV as being loss of function-intolerant, and the sum of all pLI scores of genes in a deletion are used to estimate the effect size of deletions on IQ [11]. In contrast to many CNV burden studies, these studies suggest that there is an impact of CNVs on cognition. Studies showed effects of deletions on IQ [11], and demonstrated a 3:1 effect size for of deletions and duplications on non-verbal IQ (NVIQ) [14]. Moreover, similar effect sizes were observed for deletions and duplications on IQ in unselected or general populations and autism spectrum disorders (ASD) cohorts [14]. Deleting 1 point of pLI had the same effect on NVIQ scores in both autism and population cohorts, indicating that CNV deletions do not differentially impact cognition in clinically ascertained and general population cohorts [14]. Overall, these studies suggest an impact of CNVs in aggregate on cognition. Some studies have adopted a more targeted approach focused on lists of CNV implicated in neurodevelopmental and neuropsychiatric conditions to further understand their specific contribution to cognitive ability [5, 15].
Rare neurodevelopmental and neuropsychiatric associated CNVs (ND-CNVs)
Many rare CNVs have been broadly linked to neurodevelopmental and neuropsychiatric conditions (ND-CNV) including autism, schizophrenia (SCZ) and intellectual disability (ID). Some studies have investigated a list of aggregated ND-CNV, while others have used a gene-first approach, most commonly within a subset of 12 recurrent ND-CNV found to be robustly associated with neurodevelopmental and neuropsychiatric conditions [16, 17]. ND-CNVs show incomplete penetrance and variable phenotypes. Understanding the broader cognitive impact of ND-CNVs, or whether there are genotype-specific cognitive profiles may inform genetic counselling and guidance for carriers and their family members regarding the potential cognitive impact. It may also improve the implementation of cognitive and educational supports for those that may have more complex needs [18]. This review aimed to summarize the current research on ND-CNV cognitive phenotypes with a focus on (1) cognitive impact of aggregated lists of ND-CNV in both general and clinical cohorts to provide a better understanding of their impact in these populations, and (2) genotype-first approaches to understand if there are specific cognitive impacts associated with 12 recurrent ND-CNVs (Supplementary Table 1) [17]. This set of 12 ND-CNV were the focus here as they are well defined and most frequently reported in the literature. The rarity of ND-CNV leads to challenges in conducting sufficiently powered studies, therefore these ND-CNV are more likely to have genetic-first studies of cognition than more recently identified ND-CNV.
The term “carrier” is typically used to describe people with a genetic variation who do not express an associated phenotype, however, for the purpose of this review we use the term to refer to anyone with an ND-CNV, regardless of clinical phenotype (i.e., both clinical and non-clinical cohorts, or probands and familial carriers for some studies).
Methods
Pub-Med and Embase databases were searched for studies that assessed the cognitive impact of ND-CNV. Included were studies that investigated pre-defined lists of ND-CNV in aggregate that also included one or more of the 12 recurrent ND-CNV, and studies that evaluated the individual effects of 12 recurrent ND-CNV on cognitive phenotypes [17]. For the individual effects of ND-CNV, 22q11.2 deletion was subsequently excluded from the review as the cognitive phenotype has previously been reviewed and characterized [19]. The 16p11.2BP4-BP5 CNV was included as it is associated with neurodevelopmental and neuropsychiatric conditions [20].
Final searches were conducted between the 16th of November 2021 and 6th of December 2021 and included any publication date up until the date searches were completed (see Supplementary Methods for search terms). Studies assessing cognition were included if they reported cohort performance on at least one cognitive test spanning cognitive domains of executive function, attention, learning and memory, language, perceptual-motor function, social cognition, or at minimum a measurement of overall intellectual functioning such as Full-Scale IQ (FSIQ), Verbal IQ (VIQ) or Performance IQ (PIQ). Studies were included if they assessed cognition in ND-CNVs in either general population or clinical cohorts across all age ranges with at least 5 subjects. Multiple studies from the same consortium or patient registry were included if the study provided an extension to previously reported analyses, or if additional participants were included. Exclusion criteria were studies not published in English, systematic or narrative reviews, meta-analyses, case reports, studies that assessed cognition in animal models, and studies that did not report any cognitive assessment score.
We identified 1227 papers in total from database searches, and two further papers were identified from reference lists of the studies included, review papers, or from publication lists associated with Generation Scotland, UK Biobank (UKB), Simons VIP and IMAGEN datasets. After screening and filtering, 35 papers met criteria for inclusion in the review (Fig. 1).

Papers were identified through database searches and then screened for eligibility for inclusion based on specific criteria.
Cognitive impact of predefined sets of ND-CNVs in aggregate
Eleven studies investigated performance on a range of cognitive measures in pre-defined sets of ND-CNVs in aggregate (Table 1) [5, 10, 15, 18, 21,22,23,24,25,26,27]. Four studies were in general population cohorts [10, 15, 23, 24]; and seven were in clinically ascertained cohorts [5, 18, 21, 22, 25,26,27]. Each study investigated a slightly different ND-CNV list (see Supplementary Table 2 for full list for each study), with inclusion of at least one ND-CNV from the list of 12 ND-CNV subsequently reported in the genetic-first section below.
The cognitive impact of specific ND-CNV sets have been identified in population-based cohorts of varying size. Kendall et al. (2017) investigated 53 pathogenic CNVs, 12 SCZ-associated and 41 other ND-CNVs, in 152,728 individuals from the UKB and their effects on seven cognitive tests (reaction time, simple and complex processing speed, fluid intelligence, numeric working memory, and visual attention, and cognitive performance) [24]. Sample sizes and statistical power varied by cognitive sub-test. ND-CNV carriers had poorer performance compared with non-carriers overall and ND-CNV carriers had the poorest performance with largest effects observed on fluid intelligence. Performance in the ND-CNV carriers was intermediate between non-carriers and a subgroup of individuals with SCZ identified in the cohort. A further study in 500,000 UKB participants identified significant associations with at least one measure of cognition or general functioning in 24 of 33 ND-CNV analyzed individually [15]. CNV penetrance was associated with effects on cognition; 16p11.2 duplication and distal deletion carriers showed greatest impacts. Mirror effects on cognition for reciprocal deletions and duplications were not observed. Average effect sizes were modest but assume equal weighting of performance on all tasks, although the numbers completing each were variable. A study in the Icelandic population (n = 101,655) identified 176 carriers of one of 24 ND-CNV [23]. They showed significantly poorer performance on cognitive tasks (PIQ, VIQ, letter and category fluency, Trail Making performance, set-shifting ability, spatial working memory, rapid visual processing and logical memory task), although the effects on cognitive performance in a SCZ subgroup was greater. When the analyses were controlled for IQ, only global functioning was significantly different between the groups. No differences in cognitive performance were observed in carriers of other large CNV not associated with neurodevelopmental or neuropsychiatric conditions in comparison with controls. A final study of ND-CNVs (n = 29) found significant effects of deletions, but not duplications, on IQ, non-word repetition and social cognition [10]. These findings suggest a greater impact of deletions on cognition; however, multiple testing correction was not conducted, and sample sizes for individual tasks were small.
Cognitive impacts of ND-CNV have also been reported in clinically ascertained cohorts. Chawner et al. (2019) reported that carriers of one of 13 ND-CNVs (n = 238) had significant differences in cognitive measures and traits linked to neurodevelopmental conditions compared with non-carrier siblings (n = 106) [18]. The observed effects were robust to correction for multiple testing and controlling for IQ. Specifically, large effects were observed in FSIQ, PIQ, VIQ, and sustained attention. Effects on spatial working memory, spatial planning and set-shifting ability were moderate and were small for processing speed. Significant effects were mostly observed when deletion and duplication carriers were separately compared. High levels of traits linked to neurodevelopmental conditions were observed in all ND-CNV carriers, while the observed effects on cognitive traits were weaker and more variable. No dosage effects of ND-CNV were observed and there were no specific profiles associated with deletions and duplications. The qualitative and quantitative nature of CNV effects were explored by ranking mean z-scores for each trait supporting differences between genotypes. Genotype predicted 5%-20% of variance in phenotypic traits, and significantly predicted the observed effects on FSIQ, PIQ and VIQ scores, processing speed and spatial planning, but not sustained attention, spatial working memory and set-shifting.
Cunningham et al. (2021) found that poor motor co-ordination was highly prevalent in children with ND-CNVs and closely linked to lower intellectual function and increased likelihood of mental health conditions [26]. They reported an association between motor co-ordination and low FSIQ, PIQ and VIQ, and increased ADHD and ASD symptoms in children with ND-CNVs (n = 169) compared with their closest-in-age unaffected siblings (n = 72). Motor co-ordination ability was found to fully mediate anxiety symptoms and to partially mediate FSIQ, PIQ and VIQ scores and ADHD and ASD symptoms.
Two studies assessed cognitive impacts in autism cohorts. Jensen et al. (2020) investigated the effects of 78 pathogenic CNV and de novo likely-gene disruptive (LGD) variants in 2290 autistic individuals from the Simons Simplex Collection (SSC), with and without intellectual disability [22]. Carriers of CNV or LGD variants in both groups had lower IQ compared with non-carriers in the same groups. The likelihood of carrying a deleterious variant was reduced in individuals with an IQ over 100. They reported an average decrease of 12.8 IQ points in carriers of de novo variants in a set of 173 autism-associated genes compared with non-carriers indicating a role for these genes in both autism and IQ. Barone et al. (2021) compared IQ or general quotient (GQ) in three groups of autistic children; carriers of autism associated CNV (ASD-CNV) (n = 7) or a non-causative CNV (n = 18), and non-carriers (n = 84) [25]. There were no significant differences in rates ID or developmental delay between the three groups, although those with ASD-CNV had IQ or GQ less than 70. The results were likely impacted by the small samples size in ASD-CNV group.
Finally, two studies assessed SCZ-associated CNVs in SCZ cohorts. Hubbard et al. (2021) found that carriers of 12 SCZ-CNV had lower general cognitive ability than non-carriers in both a discovery (n = 15 CNV carrier and 860 non-carrier) and replication sample (n = 8 carrier and 511 non-carrier), although SCZ-CNV samples sizes were low in both datasets [21]. Rare CNVs impacting genes intolerant to loss of function were associated with greater effects on cognition than genes impacted by CNV duplications. Poorer performance in immediate and delayed recall tasks of memory has also been reported within carriers of one of a pre-defined list of 27 SCZ-CNV from a dataset of individuals with schizophrenia and relatives (n = 29), suggesting specific cognitive impacts of these SCZ-CNV [5].
Overall, the aggregate studies reviewed showed moderate impacts across a broad range of cognitive domains were observed in ND-CNV carriers compared to non-carriers in the general population [15], and to a lesser degree than in those with an NDC [10, 23]. Carriers of some ND-CNV with an NDC show poorer cognition than non-carriers with an NDC, but this is not the case for all ND-CNV [21, 28]. The identification of overlapping or distinct cognitive traits among ND-CNV may help to understand how the underlying mechanisms disrupted in ND-CNV carriers contribute to differences in neurodevelopment and phenotypic traits such as cognition.
Cognitive outcomes in groups defined by ND-CNV
Two studies separately compared cognition in different ND-CNVs to non-ND-CNV carriers from the general population or the SSC. Bishop et al. (2017) analyzed five de novo ND-CNVs identified in five or more individuals including 16q11.2 deletions and duplications, 15q11.2–13 duplications, 1q21.1 duplications and 7q11.23 duplications and compared to the SSC [27]. NVIQ and VIQ scores were above the SSC mean in 1q21.1 duplication carriers, and lower in 15q11.2–13 duplication and 16p11.2 duplication and deletion carriers, suggesting these ND-CNVs impact cognition to a greater extent. However, extrapolation of specific phenotypic signatures was difficult as sample sizes were small and there was high variability within ND-CNV carrier groups.
Individual analysis of the cognitive phenotype of 11 ND-CNVs in comparison to non-carrier controls in a general population cohort showed that 16p11.2 deletions, 17p12 deletions and duplications, and 16p12.1 deletions were significantly associated with VIQ with large effect sizes, while 16p11.2 deletions and 16p13.11 duplications were significantly associated with PIQ [23]. Overall carriers of 16p11.2 deletions displayed greatest impact across cognitive tasks. 16p11.2 deletions and duplications were associated with spatial working memory performance, and 16p11.2 deletions were also associated with letter fluency, stroop task and preservative errors on the Wisconsin card sorting task (WCST). 16p11.2 deletions and 22q11.2 duplications were associated with category fluency performance. 15q11.2BP1–2 deletions were associated with difficulties in reading and mathematics, while effects on other cognitive measures were only modest in nature, particularly when IQ was controlled for. All cognitive measures were impacted in 22q11.2 duplication carriers, although not all were statistically significant. These two studies suggest cognitive differences in specific ND-CNV. In the next section we focus on genotype-first studies to elucidate any distinct cognitive impacts of specific ND-CNV.
Cognitive impact of a predefined list of 12 ND-CNV using a genetic-first approach
We identified 24 papers using a genotype-first approach to characterize cognition one of 12 recurrent ND-CNVs (Table 2). No studies assessing 3q29 deletions or 16p13.11 duplications were found using our search criteria. Within the 12 pre-defined ND-CNVs, impacts on at least one measure of mean FSIQ, PIQ or VIQ score, or fluid intelligence were found in both unaffected and clinically ascertained cohorts [29,30,31,32,33]. Genetic-first studies of ND-CNV are discussed separately.
1q21.1 duplication and deletion
Two studies assessed cognition in 1q21.1 duplication and deletion carriers in clinically ascertained participants and familial carriers from the Simons Variation in Individuals Project (VIP) and Intellectual Disability and Mental Health: Assessing the Genomic Impact on Neurodevelopment (IMAGINE-ID) cohorts, and one from the UKB general population [29, 33, 34]. Study outcomes were not consistent. One study of clinically ascertained children found lower FSIQ, PIQ, and VIQ compared to familial non-carriers in association with 1q21.1 duplications or deletions [34]. Separately a small sample of clinically ascertained adults identified reduced FSIQ, PIQ and VIQ in deletion carriers [34]. In contrast, Bernier et al. (2016) found significantly lower VIQ and NVIQ in duplication carriers compared to familial non-carriers [29]. They found no difference between duplication and deletion carriers. Phonological processing was in the extremely low range in both carrier types [29]. The discrepancies may be related to different sample sizes. Both studies included the Simons VIP cohort, giving rise to potential for overlapping participants. Analysis of the UKB identified poorer performance, processing speed, executive functioning, and declarative memory for 1q21.1 deletion carriers, and in reaction time and reasoning and problem-solving tasks for duplication carriers compared to controls [33]. This suggests different in cognitive impacts between 1q21.1 deletions and duplications, and that they both impact cognition in the absence of neurodevelopmental conditions.
2p16.3 (NRXN1) deletion
One study assessed a small sample of five people with NRXN1 deletions and ID diagnosis and reported four participants with below average cognitive ability and one in the low average range. It is worth noting that different cognitive measures such as NVIQ, FSIQ or DQ are reported for each participant [35].
7q11.23 duplication
Variability in cognitive, language and academic abilities was observed in children and adult carriers of 7q11.23 microduplications [31]. This was a case-only descriptive study of children with classic 7q11.23 microduplication, ascertained clinically and two smaller groups of toddlers and adults identified by cascade testing. Key findings in the toddler group were low average cognition associated with relatively poorer expressive compared with receptive language. The school age children had lower general conceptual ability (GCA), verbal, spatial, and nonverbal reasoning compared with the normative mean, and receptive language and expressive vocabulary scores in the average range. Adult carriers had average FSIQ and PIQ and low average VIQ that was significantly discrepant from PIQ in over half of carriers. They had relative reductions in expressive language compared with receptive language scores.
15q11.2 BP1-BP2 deletion
Three studies in 15q11.2 BP1-BP2 deletion carriers showed impacts on mathematical skills and aspects of language [23, 36, 37]. Lower reading and mathematical ability were identified in carriers in a population cohort compared with non-carriers [23, 36]. In a study using a web-based tool, poorer neurocognitive performances on tasks of arithmetic reasoning and a reverse memory span task of working memory were identified in 15q11.2 BP1-BP2 deletion carrier parents compared with age, gender and education matched population controls [37].
In the UKB, two studies of 15q11.2 BP1-BP2 deletion carriers showed significantly poorer performance on either four or five out of seven measures including fluid intelligence, Trail Making B, reaction time, digit-symbol substitution tasks, and digit span, when compared to controls [38, 39]. Duplication carriers did not differ significantly to non-carriers on any cognitive measure in one study [38], and had poorer performance in a pairs matching task only in the second study [39]. Copy number dosage at 15q11.2 BP1-BP2 was observed to have significant effects on reaction time, fluid intelligence and Trail Making B [38]. Overall, findings show that 15q11.2 BP1-BP2 deletions, but not duplications, impact multiple aspects of cognition.
15q11.2-q13.1 duplication (Dup15q Syndrome)
15q11.2-q13.1 duplications are frequently associated with isodicentric or interstitial duplication subtypes. Genetic subtype and epilepsy were associated with impairments in verbal and non-verbal developmental quotient (VDQ/NVDQ) in a group of children with different subtypes [40]. Isodicentric duplications were associated with lower VDQ and NVDQ compared to interstitial duplications although VDQ differences were likely related to co-occurring epilepsy in the isodicentric subtype. A prior study of a small subset of this cohort found no differences between isodicentric (n = 10) and interstitial (n = 3) genetic subtypes, likely due to the small sample size [41]. Separately, FSIQ was reported to be the low to average range in a small sample of interstitial duplication carriers (n = 9) [42].
15q13.3 deletion
One case-only study of 18 adolescent 15q13.3 microdeletion carriers reported mean FSIQ, VIQ and NVIQ to be significantly lower than the normative mean, with no difference between VIQ and NVIQ [32]. There was high variability in FSIQ scores, and 5/18 individuals also had a second CNV of uncertain clinical significance.
16p11.2 deletion and duplication
Reduced cognitive ability in carriers of 16p11.2 deletions has been reported by five studies [30, 43,44,45,46]. Three of these included participants ascertained by the Simons VIP consortium, resulting in a high probability of overlapping samples [30, 44, 46]. An initial case-only study (n = 11) showed high variability in VIQ and NVIQ [43].
Reduced FSIQ was reported in probands and parent and sibling carriers of 16p11.2 deletions compared to non-carrier familial controls [46]. There was no significant difference between probands and relative carriers or between de novo or inherited deletion carriers. Carriers had significantly lower mean VIQ compared to NVIQ, and 20% met the DSM-IV-TR criteria for ID. Hanson et al. (2015) observed similar effects on FSIQ, VIQ and NVIQ in addition to poorer spoken language scores, word reading and numerical operations academic tasks [30]. Mean NVIQ significantly below the normative mean in children and adults with 16p11.2 deletions, and language impairments, e.g., reduced word reading, and spelling scores were also reported in a case only study [44]. 60% of children had expressive and receptive language impairments.
One study compared 16p11.2 deletion carriers (n = 17) with ASD (n = 121) and neurotypical (NT) comparison groups (n = 45) [45]. The cognitive phenotype in 16p11.2 deletion carriers was between ASD and NT groups. Mean VIQ was 10-points higher in carriers compared to the ASD group. Both 16p11.2 deletion carrier and ASD groups had significantly lower FSIQ compared to NT group.
Six studies assessed cognitive phenotypes in both 16p11.2 deletions and duplication carriers. Results of comparisons between deletion and duplication carriers were mixed. Four studies used SVIP cohort with potential for overlap in samples, however, any studies with different analysis approaches are included [47,48,49,50].
D’Angelo et al. (2016) found reduced mean FSIQ, NVIQ and VIQ in duplication carriers compared with controls, and reduced mean FSIQ in deletion carriers compared to controls, even when accounting for ASD and seizures [48]. There was greater variance in FSIQ and larger effects on FSIQ in duplication carriers compared with non-carrier familial controls. There were IQ differences between carriers of de novo versus inherited deletions, but not duplication carriers. However, the IQ of transmitting parents accounted for 36% of the variance in inherited duplication carriers. Expanding on this, Hippolyte et al. (2016) found lower scores on measures of language (non-word repetition, oromotor sequences, sentence repetition, lexical and written language skills) and executive function (verbal inhibition) in deletion carriers [49]. Duplication carriers performed better than familial controls on tasks of verbal long-term memory, such as encoding and delayed recall tasks, and on verbal long-term memory. Deletion carriers had poorer performance than duplication carriers on tasks of non-word repetition, oromotor sequences, verbal short- and long-term memory, and inhibition supporting the observation of distinct cognitive differences between 16p11.2 CNV sub-types.
Reports from other studies comparing IQ between deletion and duplication subtypes have been mixed. Two reported lower cognitive scores in duplication carriers [28, 50], one reported lower scores in deletion carriers [51], and one reported no significant difference between groups [47]. These discrepancies may be related to sample size or study exclusion criteria. For example, one study focused on deletion and duplication carriers from the SVIP cohort that also completed neuroimaging which excluded individuals with reduced language and cognitive abilities.
Although FSIQ did not differ between deletion and duplication carriers in one study, both groups had lower FSIQ compared to case-matched non-carrier controls, similar to previous findings [47]. Further, a study that reported lower VIQ in deletion carriers compared to duplication carriers found a higher number of additional rare CNVs was associated with lower VIQ and NVIQ in deletion carriers, and NVIQ in duplication carriers [51], suggesting additional genetic influences on cognitive abilities.
In contrast, another study reported lower NVIQ in duplication carriers compared to deletion carriers and showed that poorer cognition significantly predicted lower functional communication in both groups when including verbal and minimally verbal individuals [50]. Even here, excluded participants were often minimally verbal, had significantly lower IQ and were more likely to be diagnosed with ASD compared to those who were included, therefore, conclusions regarding effects of ASD and NVIQ on language are limited.
Finally, Chawner et al. (2021) compared 16p11.2 deletion and duplication carriers, 22q11.2 deletion and duplication carriers, and an ASD group from the IMAGINE-ID cohort [28]. Similar to Kim et al. (2021), 16p11.2 duplication and 22q11.2 deletion carriers had lower FSIQ, VIQ and PIQ relative to 16p11.2 deletion and 22q11.2 duplication carriers. Cognitive performance in duplication carriers was more variable than deletion carriers. 16p11.2 deletion carriers with ASD had similar cognitive impairment to the ASD group, whereas duplication carriers with ASD had a poorer PIQ compared to the ASD group.
Overall, 16p11.2 deletions impact cognition, however it will be important to elucidate reasons for the discrepancies between studies comparing 16p11.2 deletions and duplications, and whether they relate to participant ascertainment or inclusion criteria for each study, or other factors such as additional CNVs.
Domain-specific cognitive phenotypes in carriers of specific ND-CNVs
While only a limited number of ND-CNV have been investigated using adequately powered studies, general impacts across multiple cognitive domains were reported, some ND-CNV appeared to show greater effect sizes than others for different cognitive tasks which may suggest that some cognitive domains are more affected in certain ND-CNVs [15, 18].
Reduced grammatical and numerical reasoning were reported in 15q11.2BP1-BP2 deletion carriers in the general population and parent carriers [23, 37], with similar patterns observed in those with a diagnosis of dyslexia and dyscalculia [36]. These cognitive impacts are supported by neuroimaging studies, with reduced grey matter volume in left fusiform gyrus observed in 15q11.2BP1-BP2 deletion carriers [36], dyslexia [52] and dyscalculia [53]. Reduced differences in functional activity between phonological & orthographic familiar words and unfamiliar word forms within the fusiform gyrus in 15q11.2BP1-BP2 deletion carriers also suggests a lack of differentiation between word and non-word forms [36], similar to that observed in dyslexia [54].
16p11.2 CNVs are considered highly penetrant, and carriers exhibit the greatest degree of global cognitive impact in general population studies [15, 23]. 16p11.2 deletions have also been associated with language impacts [30, 44, 49], with large effects observed on VIQ in the general population [23], and lower non-verbal ability with poorer expressive, receptive, lexical and written language and verbal memory observed in clinically ascertained individuals [30, 49]. Brain structural differences in 16p11.2 deletion carriers compared with non-carriers have also been shown in language and phonological processing regions such as the transverse superior and middle temporal gyri [55].
One study showed relative strengths in verbal long-term memory in 16p11.2 duplication carriers, however this is the only study that reported increased cognitive performance associated with an ND-CNV [49]. Replication in a separate cohort is necessary, as reduced cognitive ability has been reported in other studies [18, 28].
The literature to date is limited, and the lack of in-depth speech and language assessment across ND-CNVs makes it difficult to draw inference about specific language impacts. While the suggested broad impacts of language abilities across ND-CNV is supported by reports of speech and language delay or language difficulties in some ND-CNV [56,57,58,59], a comprehensive language characterization across ND-CNVs is needed to fully understand their impact.
Cognitive impact of deletions and duplications at the same loci
Some ND-CNVs are associated with duplications and deletions at the same locus, with gene dosage effects reported for traits such as height, body mass index (BMI), and macrocephaly/microcephaly in 1q21.1 CNV carriers [29, 60], and BMI and macrocephaly/ microcephaly in 16p11.2 CNV carriers [55, 60]. While carriers of both 16p11.2 deletions and duplications showed cognitive impacts [18], only one study suggested potential gene-dosage effects, with greater verbal long-term memory in 16p11.2 duplications compared to deletion carriers and NVIQ matched controls [49]. However, this requires replication in a larger sample. As for 1q21.1 CNV carriers, cognitive reports are inconsistent in clinical cohorts of children and adults [18, 29, 34], with greater impacts associated with 1q21.1 deletion compared to duplication in the general population [15, 33]. Similarly, deletions at 15q11.2 BP1-BP2 locus affected multiple aspects of cognition, while duplications did not [36, 38]. Overall, gene dosage effects on cognitive phenotypes were not observed, although findings mostly support the greater impact of deletions compared to duplications which is likely explained by haploinsufficiency or loss of function having greater impact than gain of function.
Influence of additional factors on variability in cognitive phenotypes
Chawner at al. (2019) showed that genotype accounted for between 5 and 20% of phenotypic variance, depending on the trait. Wide heterogeneity in cognitive ability within ND-CNVs reported in numerous studies implies the influence of other factors. For example, age effects have been reported, with increasing age associated with greater impairments in FSIQ and spatial working memory and reduced attention and set-shifting impairments in ND-CNV carriers [18]. Longitudinal studies are needed to accurately assess age effects on neurocognitive phenotypes in ND-CNV carriers throughout development. While sex effects have also been observed, with poorer performance on tasks of sustained attention and superior perceptual organization skills in males compared to females, sex accounted for a small amount of cognitive variation [18]. Many studies, especially genotype-first studies, may not be adequately powered to assess sex differences, leading to insufficient evidence of robust findings.
Physical traits such as motor difficulties are reported in many ND-CNV [18, 30], and may impact cognitive task performance [29]. While poorer coordination has been linked to reduced IQ in ND-CNV carriers [26], it could lead to reduced performance on certain tasks unrelated to an individual’s cognitive ability. Not all studies reviewed here assessed motor skills. However, motor skills should be considered when assessing performance on certain cognitive tasks.
When considering genetics, the size and location of a deletion or duplication within a CNV may contribute to the variability in cognitive phenotype observed between individual carriers of the same ND-CNV. For example, within the 15q11.2-q13.1 duplication (Dup15q), children with isodicentric duplications had lower VDQ and NVDQ compared to interstitial duplications, suggesting differential impacts [40]. Noteworthy, the isodicentric duplication often results in a triplication rather than a duplication leading to four copies and typically includes the 15q11.2 region, whereas the interstitial typically results in three copies of the 15q11.2-q13.1 region. While the information was not available for all studies, phenotypic heterogeneity is also potentially introduced through parent of origin and CNV coordinates as some may include the 15q11.2 BP1-BP2 region while others may include the 15q13.3 BP3-BP5 region. As for NRXN1 deletions (2p16.3), exonic deletions are thought to be more clinically relevant than intronic deletions, with suggestions that exon 6–24 deletions are more penetrant with increased likelihood of developing ID and SCZ [61, 62]. While cognition has not been specifically compared across different deletions within the NRXN1 gene, different cognitive impacts may also be present.
Apart from NRXN1 deletions, the loci of the ND-CNV we reviewed affect multiple genes, many of which are highly expressed in the brain and associated with key functions, including synaptic formation and signalling [63]. A recent study linked genes within the 16p11.2 CNV locus and phenotypic traits, with the SPN gene shown to be associated with IQ and BMI, and the YPEL3 gene with SCZ [64]. More in-depth analysis of genes and molecular mechanisms associated with ND-CNV phenotypes is required. While individual gene products may be affected by CNVs at specific locations, the potential downstream convergence on common mechanisms may also explain cross-genotype similarities in cognitive phenotypes.
Evidence for cognitive impacts of inheritance patterns remains unclear based on the reviewed articles [11, 46, 48], as many of the studies did not analyze the effect of inheritance status on cognitive outcomes. Further research is needed to examine suggestions that CNVs arising de novo are more deleterious, as it is thought they may negatively affect reproductive success and therefore have a reduced likelihood of being inherited [23]. For example, if two individuals have an identical CNV which is de novo in one person and inherited in the other, the CNV should have similar penetrance, although, the clinical and/or cognitive outcomes are likely influenced by other genetic or environmental factors. Another factor that hampers our understanding is that inheritance patterns are typically only available in clinical rather than population cohorts.
Quantifying the effect of ND-CNV in isolation is difficult, and cognitive phenotypes are additionally influenced by an individual’s genetic and environmental background. Family-based studies including parents and siblings may help to elucidate ND-CNV impacts relative to genetic background. Also, additional deleterious variants in the genetic background likely interact with ND-CNVs [65, 66]. A recent analysis 16p11.2 deletion carriers showed a correlation between FSIQ and number of additional rare variants [65], with a significant excess of additional variants also observed in 16p11.2 deletion proband carriers relative to carrier parents. To date, the cognitive impact of “other hits” has not been widely studied in the presence of ND-CNVs, although this is a growing area of research [66]. Further understanding of all possible genetic factors and their interactions is required to provide accurate prognostic information to ND-CNV carriers and families.
While we do not have sufficient evidence of impacts of environmental factors specifically in ND-CNV carriers, it is important to consider whether or how they cognitive or behavioural phenotypes, or later functional outcomes. Factors such as early life in utero exposures, birth traumas, or exposure to drugs during pregnancy may be important to consider although are often not systematically available in genetic cohorts. Future studies of ND-CNV carriers would benefit from the inclusion of psychosocial factors to evaluate their impact. In addition, more prevalent use of family-based study designs that are informative regarding inheritance may provide more insight into the heterogeneity of on cognitive and mental health outcomes.
Functional outcomes and cognitive impact in ND-CNV
IQ is a predictor of many life outcomes, such as educational attainment, occupation, physical and mental health, and mortality [67,68,69]. Functional outcome impacts have been reported in ND-CNVs carriers in general or unselected population studies [15, 55]. Although fluid intelligence score altered the effect size of ND-CNVs on income, the low correlation between performance on certain cognitive tasks and functional outcomes suggests that cognition is not the only factor to consider. Other factors could influence functional outcomes, such as increased susceptibility for co-occurring medical conditions, which may impact educational opportunities or cognitive function [70]. In 15q11.2-q13.1 CNV carriers, cognitive ability was associated with poorer adaptive behaviour [40], suggesting impacts on daily living skills. Whether cognitive interventions help to improve adaptive behaviours and functional outcomes in ND-CNV carriers is yet to be evaluated.
Limitations
Although the 12 ND-CNVs selected for review of genotype-first studies are based on a well-defined list [17], no genetic-first studies were identified for 3q29 deletions or 16p13.11 duplications. However, research in rare ND-CNV is evolving, such that, a study of cognition in 3q29 deletions was published following the literature searches conducted for this review. Klaiman et al. (2023) showed that participants with 3q29 deletions had a lower than average FSIQ overall, with over half showing a relative strength in verbal ability [71]. It is also worth noting that the of 12 ND-CNV is not exhaustive as suggested by the reviewed studies of aggregate ND-CNV (see supplementary Table 2 for full list of ND-CNV included in each study). As the ND-CNV field progresses review of genetic-first studies of other ND-CNV will be imperative to understand their cognitive impact.
The low prevalence of ND-CNVs often leads to small sample sizes and inadequate power to assess the impact of individual ND-CNVs on cognition. The probable sample overlap in studies including data from SVIP also affects interpretation of findings and cross-study comparisons. Sufficiently powered studies are necessary to understand ND-CNV-specific cognitive impacts and relative strengths, and replication of findings will be imperative to ensure robustness of findings.
Ascertainment bias, study criteria and statistical analysis should all be considered when interpreting discrepancies between studies. For example, general population samples, such as UKB, may have lower rates of neurodevelopmental or neuropsychiatric condition diagnoses or numbers of ND-CNV carriers due to enrolment criteria [15]. Conversely, clinically ascertained samples likely overestimate ND-CNV effects, as individuals are ascertained based on clinical phenotype and may have several other genetic and environmental factors contributing to cognitive phenotypes. Another consideration is the optimal comparison group to use. Non-carrier siblings have the advantage of partially controlling for shared background genetics, while general population controls do not [18]. Although closest in age sibling is often used, these studies are somewhat limited by the inability to strictly age and gender match. Choice of statistical model, variables and covariates may also affect comparison of findings between studies [72]. Some studies reviewed covaried for IQ in their analysis, however, this may overcorrect results as cognitive tasks are measuring processes which contribute to IQ [73].
Finally, different genotype arrays and CNV calling techniques have been used in the reviewed studies of aggregate ND-CNV. For the majority of genotype-first studies reviewed, the provision of a clinical genetic report is mentioned as inclusion criteria, but no details of genotype array or CNV calling are described. Differences in arrays and CNV calling algorithms used across the studies may contribute to the heterogeneity findings. Advances in whole genome sequencing and improved CNV calling methods are likely to lead in the future to more consistency across studies [74]. Additionally, WGS will provide more detailed information about the range of genetic variants contributing to outcomes in ND-CNV carriers.
Future directions
Collaboration, registries, biobanks, and initiatives including the Genes to Mental Health Network (https://genes2mentalhealth.com/) are key for sufficient samples sizes to comprehensively characterize ND-CNV. Studies are currently underway for ND-CNV lacking in sufficient genotype-first cognitive phenotyping [75, 76]. Longitudinal studies will be important to understand the impacts of ND-CNV throughout the lifespan.
ND-CNVs are associated with heterogeneity in clinical features and cognitive ability, making it difficult to select appropriate measures to assess multiple cognitive domains across a wide range of abilities. The alignment research protocols and cognitive task batteries across studies would allow for collaboration and better comparison of similarities and differences between ND-CNV.
As ND-CNVs present with variable penetrance and phenotypic heterogeneity, a better understanding of the impacts of both common and rare genetic variance, gene-gene or gene-environment interactions, and environmental factors are required to elucidate their combined effects [65, 66].
Conclusion
ND-CNV research is invaluable for understanding how underlying biological mechanisms are associated with neurocognitive and clinical outcomes. Greater knowledge of ND-CNV cognitive phenotypes may help the provision of appropriate clinical and educational supports to improve cognitive and functional outcomes for ND-CNV carriers who may have complex needs.
References
Haworth CM, Wright MJ, Luciano M, Martin NG, de Geus EJ, van Beijsterveldt CE, et al. The heritability of general cognitive ability increases linearly from childhood to young adulthood. Mol Psychiatry. 2010;15:1112–20.
Davies G, Lam M, Harris SE, Trampush JW, Luciano M, Hill WD, et al. Study of 300,486 individuals identifies 148 independent genetic loci influencing general cognitive function. Nat Commun. 2018;9:2098.
MacLeod AK, Davies G, Payton A, Tenesa A, Harris SE, Liewald D, et al. Genetic copy number variation and general cognitive ability. PLoS One. 2012;7:e37385.
Shephard E, Milosavljevic B, Mason L, Elsabbagh M, Tye C, Gliga T, et al. Neural and behavioural indices of face processing in siblings of children with autism spectrum disorder (ASD): a longitudinal study from infancy to mid-childhood. Cortex. 2020;127:162–79.
Thygesen JH, Presman A, Harju-Seppanen J, Irizar H, Jones R, Kuchenbaecker K, et al. Genetic copy number variants, cognition and psychosis: a meta-analysis and a family study. Mol Psychiatry. 2021;26:5307–19.
Jensen M, Kooy RF, Simon TJ, Reyniers E, Girirajan S, Tassone F. A higher rare CNV burden in the genetic background potentially contributes to intellectual disability phenotypes in 22q11.2 deletion syndrome. Eur J Med Genet. 2018;61:209–12.
Marshall CR, Howrigan DP, Merico D, Thiruvahindrapuram B, Wu W, Greer DS, et al. Contribution of copy number variants to schizophrenia from a genome-wide study of 41,321 subjects. Nat Genet. 2017;49:27–35.
McRae AF, Wright MJ, Hansell NK, Montgomery GW, Martin NG. No association between general cognitive ability and rare copy number variation. Behav Genet. 2013;43:202–7.
Bagshaw AT, Horwood LJ, Liu Y, Fergusson DM, Sullivan PF, Kennedy MA. No effect of genome-wide copy number variation on measures of intelligence in a New Zealand birth cohort. PLoS One. 2013;8:e55208.
Guyatt AL, Stergiakouli E, Martin J, Walters J, O’Donovan M, Owen M, et al. Association of copy number variation across the genome with neuropsychiatric traits in the general population. Am J Med Genet B Neuropsychiatr Genet. 2018;177:489–502.
Huguet G, Schramm C, Douard E, Jiang L, Labbe A, Tihy F, et al. Measuring and estimating the effect sizes of copy number variants on general intelligence in community-based samples. JAMA Psychiatry. 2018;75:447–57.
van Scheltinga AF, Bakker SC, van Haren NE, Derks EM, Buizer-Voskamp JE, Cahn W, et al. Schizophrenia genetic variants are not associated with intelligence. Psychol Med. 2013;43:2563–70.
Yeo RA, Gangestad SW, Liu J, Ehrlich S, Thoma RJ, Pommy J, et al. The impact of copy number deletions on general cognitive ability and ventricle size in patients with schizophrenia and healthy control subjects. Biol Psychiatry. 2013;73:540–5.
Huguet G, Schramm C, Douard E, Tamer P, Main A, Monin P, et al. Genome-wide analysis of gene dosage in 24,092 individuals estimates that 10,000 genes modulate cognitive ability. Mol Psychiatry. 2021;26:2663–76.
Kendall KM, Bracher-Smith M, Fitzpatrick H, Lynham A, Rees E, Escott-Price V, et al. Cognitive performance and functional outcomes of carriers of pathogenic copy number variants: analysis of the UK Biobank. Br J Psychiatry. 2019;214:297–304.
Kirov G, Rees E, Walters JT, Escott-Price V, Georgieva L, Richards AL, et al. The penetrance of copy number variations for schizophrenia and developmental delay. Biol Psychiatry. 2014;75:378–85.
Kirov G. CNVs in neuropsychiatric disorders. Hum Mol Genet. 2015;24:R45–9.
Chawner S, Owen MJ, Holmans P, Raymond FL, Skuse D, Hall J, et al. Genotype-phenotype associations in children with copy number variants associated with high neuropsychiatric risk in the UK (IMAGINE-ID): a case-control cohort study. Lancet Psychiatry. 2019;6:493–505.
Moberg PJ, Richman MJ, Roalf DR, Morse CL, Graefe AC, Brennan L, et al. Neurocognitive functioning in patients with 22q11.2 deletion syndrome: a meta-analytic review. Behav Genet. 2018;48:259–70.
Moreno-De-Luca D, Sanders SJ, Willsey AJ, Mulle JG, Lowe JK, Geschwind DH, et al. Using large clinical data sets to infer pathogenicity for rare copy number variants in autism cohorts. Mol Psychiatry. 2013;18:1090–5.
Hubbard L, Rees E, Morris DW, Lynham AJ, Richards AL, Pardinas AF, et al. Rare copy number variants are associated with poorer cognition in schizophrenia. Biol Psychiatry. 2021;90:28–34.
Jensen M, Smolen C, Girirajan S. Gene discoveries in autism are biased towards comorbidity with intellectual disability. J Med Genet. 2020;57:647–52.
Stefansson H, Meyer-Lindenberg A, Steinberg S, Magnusdottir B, Morgen K, Arnarsdottir S, et al. CNVs conferring risk of autism or schizophrenia affect cognition in controls. Nature. 2014;505:361–6.
Kendall KM, Rees E, Escott-Price V, Einon M, Thomas R, Hewitt J, et al. Cognitive performance among carriers of pathogenic copy number variants: analysis of 152,000 UK biobank subjects. Biol Psychiatry. 2017;82:103–10.
Barone R, Gulisano M, Amore R, Domini C, Milana MC, Giglio S, et al. Clinical correlates in children with autism spectrum disorder and CNVs: Systematic investigation in a clinical setting. Int J Dev Neurosci. 2020;80:276–86.
Cunningham AC, Hall J, Owen MJ, van den Bree MBM. Coordination difficulties, IQ and psychopathology in children with high-risk copy number variants. Psychol Med. 2021;51:290–9.
Bishop SL, Farmer C, Bal V, Robinson EB, Willsey AJ, Werling DM, et al. Identification of developmental and behavioral markers associated with genetic abnormalities in autism spectrum disorder. Am J Psychiatry. 2017;174:576–85.
Chawner S, Doherty JL, Anney RJL, Antshel KM, Bearden CE, Bernier R, et al. A genetics-first approach to dissecting the heterogeneity of autism: phenotypic comparison of autism risk copy number variants. Am J Psychiatry. 2021;178:77–86.
Bernier R, Steinman KJ, Reilly B, Wallace AS, Sherr EH, Pojman N, et al. Clinical phenotype of the recurrent 1q21.1 copy-number variant. Genet Med. 2016;18:341–9.
Hanson E, Bernier R, Porche K, Jackson FI, Goin-Kochel RP, Snyder LG, et al. The cognitive and behavioral phenotype of the 16p11.2 deletion in a clinically ascertained population. Biol Psychiatry. 2015;77:785–93.
Mervis CB, Klein-Tasman BP, Huffman MJ, Velleman SL, Pitts CH, Henderson DR, et al. Children with 7q11.23 duplication syndrome: psychological characteristics. Am J Med Genet A. 2015;167:1436–50.
Ziats MN, Goin-Kochel RP, Berry LN, Ali M, Ge J, Guffey D, et al. The complex behavioral phenotype of 15q13.3 microdeletion syndrome. Genet Med. 2016;18:1111–8.
Sonderby IE, van der Meer D, Moreau C, Kaufmann T, Walters GB, Ellegaard M, et al. 1q21.1 distal copy number variants are associated with cerebral and cognitive alterations in humans. Transl Psychiatry. 2021;11:182.
Linden SC, Watson CJ, Smith J, Chawner S, Lancaster TM, Evans F, et al. The psychiatric phenotypes of 1q21 distal deletion and duplication. Transl Psychiatry. 2021;11:105.
Alfieri P, Scibelli F, Sinibaldi L, Valeri G, Caciolo C, Novello RL, et al. Further insight into the neurobehavioral pattern of children carrying the 2p16.3 heterozygous deletion involving NRXN1: report of five new cases. Genes Brain Behav. 2020;19:e12687.
Ulfarsson MO, Walters GB, Gustafsson O, Steinberg S, Silva A, Doyle OM, et al. 15q11.2 CNV affects cognitive, structural and functional correlates of dyslexia and dyscalculia. Transl Psychiatry. 2017;7:e1109.
Woo YJ, Kanellopoulos AK, Hemati P, Kirschen J, Nebel RA, Wang T, et al. Domain-specific cognitive impairments in humans and flies with reduced CYFIP1 dosage. Biol Psychiatry. 2019;86:306–14.
Writing Committee for the, E.-C.N.V.W.G., van der Meer D, Sonderby IE, Kaufmann T, Walters GB, Abdellaoui A, et al. Association of copy number variation of the 15q11.2 BP1-BP2 region with cortical and subcortical morphology and cognition. JAMA Psychiatry. 2020;77:420–30.
Silva AI, Kirov G, Kendall KM, Bracher-Smith M, Wilkinson LS, Hall J, et al. Analysis of diffusion tensor imaging data from the UK biobank confirms dosage effect of 15q11.2 copy number variation on white matter and shows association with cognition. Biol Psychiatry. 2021;90:307–16.
DiStefano C, Wilson RB, Hyde C, Cook EH, Thibert RL, Reiter LT, et al. Behavioral characterization of dup15q syndrome: toward meaningful endpoints for clinical trials. Am J Med Genet A. 2020;182:71–84.
DiStefano C, Gulsrud A, Huberty S, Kasari C, Cook E, Reiter LT, et al. Identification of a distinct developmental and behavioral profile in children with Dup15q syndrome. J Neurodev Disord. 2016;8:19.
Urraca N, Cleary J, Brewer V, Pivnick EK, McVicar K, Thibert RL, et al. The interstitial duplication 15q11.2-q13 syndrome includes autism, mild facial anomalies and a characteristic EEG signature. Autism Res. 2013;6:268–79.
Hanson E, Nasir RH, Fong A, Lian A, Hundley R, Shen Y, et al. Cognitive and behavioral characterization of 16p11.2 deletion syndrome. J Dev Behav Pediatr. 2010;31:649–57.
Mei C, Fedorenko E, Amor DJ, Boys A, Hoeflin C, Carew P, et al. Deep phenotyping of speech and language skills in individuals with 16p11.2 deletion. Eur J Hum Genet. 2018;26:676–86.
Osorio JMA, Rodriguez-Herreros B, Romascano D, Junod V, Habegger A, Pain A, et al. Touch and olfaction/taste differentiate children carrying a 16p11.2 deletion from children with ASD. Mol Autism. 2021;12:8.
Zufferey F, Sherr EH, Beckmann ND, Hanson E, Maillard AM, Hippolyte L, et al. A 600 kb deletion syndrome at 16p11.2 leads to energy imbalance and neuropsychiatric disorders. J Med Genet. 2012;49:660–8.
Blackmon K, Thesen T, Green S, Ben-Avi E, Wang X, Fuchs B, et al. Focal cortical anomalies and language impairment in 16p11.2 deletion and duplication syndrome. Cereb Cortex. 2018;28:2422–30.
D’Angelo D, Lebon S, Chen Q, Martin-Brevet S, Snyder LG, Hippolyte L, et al. Defining the effect of the 16p11.2 duplication on cognition, behavior, and medical comorbidities. JAMA Psychiatry. 2016;73:20–30.
Hippolyte L, Maillard AM, Rodriguez-Herreros B, Pain A, Martin-Brevet S, Ferrari C, et al. The number of genomic copies at the 16p11.2 locus modulates language, verbal memory, and inhibition. Biol Psychiatry. 2016;80:129–39.
Kim SH, Green-Snyder L, Lord C, Bishop S, Steinman KJ, Bernier R, et al. Language characterization in 16p11.2 deletion and duplication syndromes. Am J Med Genet B Neuropsychiatr Genet. 2020;183:380–91.
Hudac CM, Bove J, Barber S, Duyzend M, Wallace A, Martin CL, et al. Evaluating heterogeneity in ASD symptomatology, cognitive ability, and adaptive functioning among 16p11.2 CNV carriers. Autism Res. 2020;13:1300–10.
Kronbichler M, Wimmer H, Staffen W, Hutzler F, Mair A, Ladurner G. Developmental dyslexia: gray matter abnormalities in the occipitotemporal cortex. Hum Brain Mapp. 2008;29:613–25.
Rykhlevskaia E, Uddin LQ, Kondos L, Menon V. Neuroanatomical correlates of developmental dyscalculia: combined evidence from morphometry and tractography. Front Hum Neurosci. 2009;3:51.
van der Mark S, Bucher K, Maurer U, Schulz E, Brem S, Buckelmuller J, et al. Children with dyslexia lack multiple specializations along the visual word-form (VWF) system. Neuroimage. 2009;47:1940–9.
Martin-Brevet S, Rodriguez-Herreros B, Nielsen JA, Moreau C, Modenato C, Maillard AM, et al. Quantifying the Effects of 16p11.2 Copy Number Variants on Brain Structure: A Multisite Genetic-First Study. Biol Psychiatry. 2018;84:253–64.
Al Shehhi M, Forman EB, Fitzgerald JE, McInerney V, Krawczyk J, Shen S, et al. NRXN1 deletion syndrome; phenotypic and penetrance data from 34 families. Eur J Med Genet. 2019;62:204–9.
Brignell A, St John M, Boys A, Bruce A, Dinale C, Pigdon L, et al. Characterization of speech and language phenotype in children with NRXN1 deletions. Am J Med Genet B Neuropsychiatr Genet. 2018;177:700–8.
Benitez-Burraco A, Barcos-Martinez M, Espejo-Portero I, Fernandez-Urquiza M, Torres-Ruiz R, Rodriguez-Perales S, et al. Narrowing the Genetic Causes of Language Dysfunction in the 1q21.1 Microduplication Syndrome. Front Pediatr. 2018;6:163.
Rosenfeld JA, Coppinger J, Bejjani BA, Girirajan S, Eichler EE, Shaffer LG, et al. Speech delays and behavioral problems are the predominant features in individuals with developmental delays and 16p11.2 microdeletions and microduplications. J Neurodev Disord. 2010;2:26–38.
Owen D, Bracher-Smith M, Kendall KM, Rees E, Einon M, Escott-Price V, et al. Effects of pathogenic CNVs on physical traits in participants of the UK Biobank. BMC Genomics. 2018;19:867.
Castronovo P, Baccarin M, Ricciardello A, Picinelli C, Tomaiuolo P, Cucinotta F, et al. Phenotypic spectrum of NRXN1 mono- and bi-allelic deficiency: A systematic review. Clin Genet. 2020;97:125–37.
Cosemans N, Vandenhove L, Vogels A, Devriendt K, Van Esch H, Van Buggenhout G, et al. The clinical relevance of intragenic NRXN1 deletions. J Med Genet. 2020;57:347–55.
Torres F, Barbosa M, Maciel P. Recurrent copy number variations as risk factors for neurodevelopmental disorders: critical overview and analysis of clinical implications. J Med Genet. 2016;53:73–90.
Vysotskiy M, Zhong X, Miller-Fleming TW, Zhou D, C. Autism Working Group of the Psychiatric Genomics, C. Bipolar Disorder Working Group of the Psychiatric Genomics. et al. Integration of genetic, transcriptomic, and clinical data provides insight into 16p11.2 and 22q11.2 CNV genes. Genome Med. 2021;13:172.
Pizzo L, Jensen M, Polyak A, Rosenfeld JA, Mannik K, Krishnan A, et al. Rare variants in the genetic background modulate cognitive and developmental phenotypes in individuals carrying disease-associated variants. Genet Med. 2019;21:816–25.
Dinneen TJ, Ghralaigh FN, Walsh R, Lopez LM, Gallagher L. How does genetic variation modify ND-CNV phenotypes? Trends Genet. 2022;38:140–51.
Deary IJ, Harris SE, Hill WD. What genome-wide association studies reveal about the association between intelligence and physical health, illness, and mortality. Curr Opin Psychol. 2019;27:6–12.
Deary IJ, Hill WD, Gale CR. Intelligence, health and death. Nat Hum Behav. 2021;5:416–30.
Strenze T. Intelligence and socioeconomic success: A meta-analytic review of longitudinal research. Intelligence. 2007;35:401–26.
Wisk LE, Weitzman ER. Expectancy and achievement gaps in educational attainment and subsequent adverse health effects among adolescents with and without chronic medical conditions. J Adolesc Health. 2017;61:461–70.
Klaiman C, White SP, Saulnier C, Murphy M, Burrell L, Cubells J, et al. A distinct cognitive profile in individuals with 3q29 deletion syndrome. J Intellect Disabil Res. 2023;67:216–27. https://doi.org/10.1111/jir.12919.
Chowdhury MZI, Turin TC. Variable selection strategies and its importance in clinical prediction modelling. Fam Med Community Health. 2020;8:e000262.
Dennis M, Francis DJ, Cirino PT, Schachar R, Barnes MA, Fletcher JM. Why IQ is not a covariate in cognitive studies of neurodevelopmental disorders. J Int Neuropsychol Soc. 2009;15:331–43.
Trost B, Thiruvahindrapuram B, Chan AJS, Engchuan W, Higginbotham EJ, Howe JL, et al. Genomic architecture of autism from comprehensive whole-genome sequence annotation. Cell. 2022;185:4409–27.e18.
Murphy MM, Lindsey Burrell T, Cubells JF, Espana RA, Gambello MJ, Goines KCB, et al. Study protocol for The Emory 3q29 Project: evaluation of neurodevelopmental, psychiatric, and medical symptoms in 3q29 deletion syndrome. BMC Psychiatry. 2018;18:183.
Cooke J, Molloy CJ, Caceres ASJ, Dinneen T, Bourgeron T, Murphy D, et al. The synaptic gene study: design and methodology to identify neurocognitive markers in Phelan-McDermid syndrome and NRXN1 deletions. Front Neurosci. 2022;16:806990.
Acknowledgements
This work was supported by the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No 777394 for the project AIMS-2-TRIALS. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA and AUTISM SPEAKS, Autistica, SFARI. Any views expressed are those of the author(s) and not necessarily those of the funders.
Author information
Authors and Affiliations
Contributions
CM and LG were responsible for the initial review concept. CQ, CM, AMN, and LL contributed to the literature review searches, filtering of articles and summaries of included articles. CM and CQ contributed to the writing of the first draft of the manuscript, and LG provided extensive input and critical revisions of the manuscript. All authors approved the final version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Molloy, C.J., Quigley, C., McNicholas, Á. et al. A review of the cognitive impact of neurodevelopmental and neuropsychiatric associated copy number variants. Transl Psychiatry 13, 116 (2023). https://doi.org/10.1038/s41398-023-02421-6
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-023-02421-6
- Springer Nature Limited