
Abstract
Study design
Article.
Objective
To elucidate the association of age-adjusted D-dimer (AAD) with deep vein thrombosis (DVT) risk to lower limbs in patients with spinal cord injury (SCI).
Setting
Rehabilitation Medicine Department of the First Affiliated Hospital of China University of Science and Technology.
Methods
Retrospective analysis of 250 patients with SCI in the rehabilitation department from August 2018 to December 2021. Quartiles divided the D-dimer level into four groups to analyze the association between AAD level and DVT risk.
Results
Age was identified as a covariate of D-dimer and DVT risk. For non-adjusted model, when D-dimer increased by 1 mg/L, DVT risk increased 0.23-fold (P < 0.05); for minimally-adjusted model (adjusted for age), the risk increased 0.22-fold (P < 0.05); and for fully-adjusted model (adjusted for age, sex, pulmonary infection, degree, grades, and career), it increased 0.19-fold (P < 0.05). AAD had a curvilinear association with DVT risk, and the fold point was 1.9 mg/L (P < 0.05). When serum AAD level was <1.9 mg/L (K < 1.9), the estimated change in DVT risk was 3.34 (P < 0.05), and when serum AAD level was >1.9 mg/L (K > 1.9), the estimated change was 1.14 (P < 0.05). Urinary tract infection (UTI) and fibrinogen(tertile) had a interaction association with D-dimer level and DVT risk (P interaction < 0.05).
Conclusion
Patients with SCI who receive rehabilitation treatment with AAD level >1.9 mg/L need to be paid close attention to, especially those with UTI and high levels of fibrinogen.
Similar content being viewed by others

Introduction
Deep vein thrombosis (DVT) is a common complication among patients with spinal cord injury (SCI) [1]. A study found that D-dimer level was higher (≥10 μg/mL) in 15 (21.4%) out of 70 patients with SCI, and 9 (12.9%) out of these 15 were asymptomatic patients with venous thromboembolism (VTE) [2]. VTE incidence for patients with acute cervical SCI was reported to be 19.3%, and the researchers suggested that if ultrasound examination revealed DVT formation or D-dimer level increased to ≥10 μg/mL, the patient should undergo contrast examination to detect VTE, including DVT or pulmonary embolism [3]. A serum D-dimer level >10 µg/mL is a high-risk threshold for DVT in patients with SCI. After SCI, the blood flow rate in the veins slows down due to varying degrees of paralysis of the limbs and decreased muscle pumping function, and, thus, the blood is prone to hypercoagulation; as a result, it is the academic consensus that SCI leads to increased serum D-dimer levels [4,5,6,7]. For patients with SCI suspected of having DVT, if the combined application of B-ultrasound and serum examination determines that the D-dimer level is <1000 ng/mL, the probability of the patient not having DVT is 96.9% and the specificity is 66.9% [8]. The D-dimer level mainly reflects the fibrinolytic function and has certain predictive values for DVT formation [9, 10].
After adjusting for age, serum D-dimer level can improve the diagnosis of DVT [10]; age-adjusted D-dimer (AAD) cutoff value not only showed higher specificity than the existing D-dimer value (24.6% vs. 8.5%) but also had a higher negative predictive value (91.8% vs. 89.7%); thus, the researchers concluded that DVT can be ruled out using AAD levels [11]. Compared to the conventional D-dimer, the AAD performed better in DVT screening, which was clinically useful [12]. However, another study found that changing the laboratory-reported D-dimer reference interval for pulmonary embolism (PE) evaluation was not associated with a decrease in advanced chest imaging, such as computed tomography pulmonary angiography, and there was a significant difference in the AAD reference interval in the post-intervention period [13].
However, for patients with SCI hospitalized in the Department of Rehabilitation Medicine for treatment, the relationship between serum AAD level and the DVT risk in the lower limbs is yet to be fully elucidated. The present study was aimed at understanding the association between AAD and the DVT risk for SCI, which has a great value for the screening and diagnosis of DVT.
Methods
Data collection and flow chart of the study
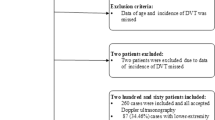
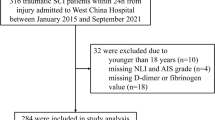
Patient data were obtained for 262 patients with SCI hospitalized in the Rehabilitation Medicine Department of the First Affiliated Hospital of China University of Science and Technology from August 1, 2018, to December 31, 2020. Nine patients with SCI were excluded due to cause of SCI were not clear and lack of lower-limb Doppler ultrasound examination findings. Another three cases were excluded because degree and American Spinal Cord Injury Association (ASIA) grades were not assessed. Finally, 250 (95.42%) patients were included, of whom 86 (34.40%) had lower-extremity DVT during hospitalization in the rehabilitation department (Fig. 1).

Inclusion and exclusion criteria are as follows. ASIA American Spinal Cord Injury Association, DVT deep vein thromobosis.
Statistical methods
The mean (standard deviation) [Mean (SD)] and median (minimum−maximum) [Median (Min−Max)] are expressed for continuous variables. Number of cases (N, N%), odds ratio (OR), and 95% confidence interval (CI) are expressed for categorical variables. Univariate and multivariate binary logistic regression model were used to analysis the association between D-dimer level and DVT risk with three distinct models. Model 1 was the non-adjusted model with no covariates adjusted. Potential confounders were selected if they changed the estimates of DVT risk by at least 10% in the final models [14, 15]. Model 2 was the minimally-adjusted model with age adjusted. Model 3 was the fully-adjusted model with the confounders, demographic factors (sex and age) and unbalanced probable variables (presented in Table 2 adjusted). Threshold saturation effect analysis, Student’s t-test, Mann–Whitney U rank-sum test, and Pearson’s chi-square tests were used to analyze the data. We used the generalized additive model (GAM) and smooth curve fitting (penalized spline method) to address the nonlinearity between D-dimer and DVT risk. The fold point was first computed using a recursive algorithm when nonlinearities were detected, and then a two-piece binary logistic regression model was constructed on either side of the fold point. Subgroup analysis was performed using a stratified binary logistic regression model. For D-dimer level, we first converted it to categorical variables according to fourth quartile (Quartile, Q1–4 group), and then performed an interaction analysis. To modify the effect on the subgroup indicator was followed by a test for the likelihood ratio. In addition, we also conducted a sensitivity analysis to analyze the robustness of the results. To validate the results of D-dimer as a continuous variable and investigate the likelihood of nonlinearity, D-dimer was transformed into a categorical variable according to the fourth quartile(Quartile, Q1–4 group). A generalized estimated equation model was applied for multivariable logistic regression analysis as a covariate screening test. A two-sided P < 0.05 was indicated as statistically significant. All analyses were performed using R statistical package (R Foundation; http://www.r-project.org; version 3.4.3) and EmpowerStats (www.empowerstats.com; X&Y Solutions Inc.).
Results
Characteristics of study population
Based on the serum D-dimer level, a four-class grouping was performed, with 62 cases in the Q1 and Q2 groups and 63 cases in the Q3 and Q4 groups. The age, D-dimer level, rate of trauma, degree of complete injury, pulmonary infection, and DVT risk were highest in Q4 group, followed by followed by Q3, Q2, and Q1 groups (P < 0.05). The ASIA-A grades, urinary tract infection and the proportion of patients with SCI who were farmer were higher in Q4 group, followed by Q2, Q3, and Q1 groups (P < 0.05). Serum fibrinogen levels in the patients were the highest in Q3 group, followed by Q4, Q2, and Q1 groups (P < 0.05). TThe rate of patients with SCI with neck was the highest in Q3 group, followed by Q2, Q4, and Q1 groups (P < 0.05). There was no significant difference in sex and smoking history ratio among the four groups (P > 0.05; Table 1).
Univariate logistic regression analysis of D-dimer level and DVT risk
Univariate logistic regression analysis found that if age increased by 1 year, the DVT risk increased 0.06-fold among patients with SCI (P < 0.05). For every increase of 1 mg/L of the D-dimer level, the DVT risk increased 0.23-fold (P < 0.05). The DVT risk increased 1.35-fold among patients with SCI with pulmonary infection compared to those without pulmonary infection (P < 0.05) and increased 0.69-fold for patients with complete SCI compared to those with incomplete SCI (P < 0.05). The DVT risk in ASIA-D decreased 0.95-fold compared to that in ASIA-A (P < 0.05). Furthermore, the DVT risk increased 0.68-fold in patients with SCI who were farmers compared to those who were not (P < 0.05). An increase of 1 mg/L of the D-dimer level resulted in an increase in the DVT risk, which was 2.68-fold higher in Q4 group than in Q1 group (P < 0.05), 1.84-fold higher in Q3 group than in Q1 group (P < 0.05), and 0.41-fold higher in Q2 group than in Q1 group(P > 0.05) (Table 2).
Multivariate binary logistic regression analysis of D-dimer level and DVT risk
Covariate screening test showed that age was a covariate of D-dimer and DVT risk. Multivariate regression analysis found that in the minimally-adjusted model (adjusted for age), for every increase of 1 mg/L of D-dimer level, the DVT risk increased 0.22-fold (P < 0.05); and in the fully-adjusted model (adjusted for age, sex, pulmonary infection, degree, grades, and career), it increased 0.19-fold (P < 0.05; Table 3 and Supplementary Table 1).
Curve line correlation between AAD level and DVT risk
After the covariate-age was adjusted, the AAD had a curvilinear association with DVT risk (Fig. 2). In order to further verify the association; we transformed the D-dimer level into Log10, and had a logarithmic linear growth association with DVT risk (Supplementary Fig 1).

The black continual line is a fitting line of AAD and DVT risk, and the interval between the black dot lines is the 95%CI.
Threshold saturation effect between AAD level and DVT risk
Threshold saturation effect analysis was performed between serum AAD level and DVT risk in patients with SCI. The logarithmic likelihood ratio test showed that AAD had a curvilinear association with DVT risk, and there was a fold point (K = 1.9 mg/L) (P < 0.05). When the AAD level was <1.9 mg/L (K < 1.9), the estimated change in DVT risk was 3.34 and 95% CI was 1.84–6.04. The mean DVT risk increased 234% with an increase of 1 mg/L in the AAD level when it was <1.9 mg/L, and the difference was statistically significant (P < 0.05). The mean DVT risk increased 11% with an increase of 1 mg/L in the AAD level when it was >1.9 mg/L, and the difference was also statistically significant (P < 0.05; Table 4).
Sensitive analysis of D-dimer level and DVT risk
Subgroup and interaction analysis were performed between serum D-dimer level and DVT risk in patients with SCI. The estimated change in DVT risk was >1 in different groups and the plot were at the right of reference, indicate the D-dimer level would be an independent risk factor for DVT (P < 0.05). In non-traumatic reason and ASIA-C grades of SCI, the 95%CI crossed with reference line (P < 0.05), however, the estimated change was still >1 (Fig. 3).

The back square indicates OR value. The perpendicular line is a reference line and the horizontal line indicates 95%CI.
Interaction screening analysis showed urinary tract infection (UTI) and fibrinogen tertile had an interaction association with D-dimer level and DVT risk (P interaction <0.05; Supplementary Table 2). Adjusted the confounders (Model I: age), meanwhile we adjusted demographic factors and unbalanced probable variables (Model II: sex, age, pulmonary infection, degree, grades, and career; presented in Table 2), fibrinogen(tertile) and UTI were still the effect modifier (P interaction <0.05; Supplementary Tables 3, 4).
Discussion
In our study, 86 (34.40%) patients with SCI had lower-extremity DVT during hospitalization in the rehabilitation department. Moreover, our study found that age was related to the DVT risk and that age was a synergy variable between D-dimer and DVT risk. After adjusting the covariate of age, a curvilinear relationship was noted between the ADD level and DVT risk, and there was a fold point. Fibrinogen (tertile) and UTI were the effect modifier of D-dimer level and DVT risk.
The incidence of total DVT ranges from 50 to 100% in untreated patients, and PE was the third most common cause of mortality in these patients [16]. A total of 14 patients with SCI (31%) were diagnosed with DVT using duplex ultrasonography [17]. D-dimer assays vary widely depending on the antibody used, capture method, instrumentation required, and calibration standards [18]. Although D-dimer can improve the diagnostic efficiency of DVT [19], in clinical settings, misdiagnosis caused by other factors should be considered. However, another study concluded that the application of an AAD threshold in patients with suspected PE increased the number of patients in whom imaging can be withheld [20].
The National Institute for Health and Care Excellence recently recommended the use of AAD for VTE investigations to help reduce the burden of diagnostic imaging in over-extended radiology [21, 22]. In India, higher age and quadriplegia were found to be the only factors that could be correlated to DVT and PE following SCI [23]. Moreover, a study found that both traditional D-dimer and AAD were associated with a high and similar negative predictive value and similar utility in the diagnosis of DVT [24]. However, another study found that the AAD cutoff level was not useful in the diagnostic algorithm of DVT in an ambulatory care setting [25]. To the best of our knowledge, there is no specific research on the traditional D-dimer or AAD level of the effect value of DVT risk for patients with SCI in a rehabilitation department, which is disadvantageous to the prevention of DVT in these patients. In order to reflect the overall picture of clinical research more objectively and comprehensively and to reflect the real-world clinical research, not only age but also other variables with significant differences in baseline data were adjusted in this study; the D-dimer level still remained associated with DVT risk among the patients with SCI and was very similar to that in the non-adjusted model.
A study found that the incidence of DVT in patients with SCI was 100% detected by the 125I-labeled fibrinogen test and confirmed by contrast venography [26], and 125I fibrinogen lower limbs scanning was a more sensitive indicator of DVT events than impedance venography or plethysmography [27]. Neurogenic bladder disorders are common among patients with SCI, which can result in UTI [28]. A study reported a patient with DVT and PE secondary to neurogenic bladder [29], another study reported a patient with DVT caused by compression on the right iliac vein by a distend bladder [30]. Our study also found that fibrinogen and UTI were the effect modifier of D-dimer level and DVT risk.
In this study, AAD had a curvilinear association with DVT risk, and the fold point was 1.9 mg/L (P < 0.05). The estimated change of DVT risk was higher for AAD levels <1.9 mg/L than for those >1.9 mg/L (3.34 vs. 1.14). Therefore, more attention should be paid to patients with SCI, especially those whose AAD levels are <1.9 mg/L. Moreover, patients with SCI having increased D-dimer levels should be suggested to undergo DVT preventive measures, including rehabilitation and anticoagulant treatments, and especially should pay more attention to those with UTI and higher serum fibrinogen level. Our research results may be valuable as reference for other researchers to conduct clinical randomized controlled studies in the future.
This study has some limitations. First, it did not conduct PE evaluations; only Doppler ultrasound was used to examine lower-extremity DVT. Second, this study had a cross-sectional design without follow-up, which thereby cannot explain the causal relationship between D-dimer and DVT, nor can it predict long-term DVT risk. It only describes an association between D-dimer and lower-extremity DVT risk during rehabilitation for patients with SCI. Third, this is a single-center study, and the application of research conclusions to other centers may not be accurate. Fourth, this research was conducted as a retrospective cross-sectional study; although our study found the fibrinogen and urinary tract infection had a interaction association for the association of D-dimer level and DVT risk, we can’t conclude a longitudinal cohort reason between them, further higher quality studies should be conducted in the future, such as random control trials or cohort studies. Finally, this study could not observe the impact of uncollected variables on D-dimer and DVT risk, and there may also be other covariates that affect the relationship between AAD and DVT risk.
Conclusion
Patients with SCI who receive rehabilitation treatment with D-dimer level >1.9 mg/L need to be paid close attention to, especially those with UTI and high levels of fibrinogen.
Data and materials availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Hon B, Botticello A, Kirshblum S. Duplex ultrasound surveillance for deep vein thrombosis after acute traumatic spinal cord injury at rehabilitation admission. J Spinal Cord Med. 2020;43:298–305.
Kumagai G, Wada K, Kudo H, Asari T, Ichikawa N, Ishibashi Y. D-dimer monitoring combined with ultrasonography improves screening for asymptomatic venous thromboembolism in acute spinal cord injury. J Spinal Cord Med. 2020;43:353–7.
Ichikawa N, Kumagai G, Wada K, Kudo H, Asari T, Xizhe L et al. High incidence of venous thromboembolism after acute cervical spinal cord injury in patients with ossification of the posterior longitudinal ligament. J Spinal Cord Med. 2020: https://doi.org/10.1080/10790268.2020.1758385.
Rathore MF, Hanif S, New PW, Butt AW, Aasi MH, Khan SU. The prevalence of deep vein thrombosis in a cohort of patients with spinal cord injury following the Pakistan earthquake of October 2005. Spinal Cord. 2008;46:523–6.
Riklin C, Baumberger M, Wick L, Michel D, Sauter B, Knecht H. Deep vein thrombosis and heterotopic ossification in spinal cord injury: a 3 year experience at the Swiss Paraplegic Centre Nottwil. Spinal Cord. 2003;41:192–8.
Rouleau P, Guertin PA. Early changes in deep vein diameter and biochemical markers associated with thrombi formation after spinal cord injury in mice. J Neurotrauma. 2007;24:1406–14.
McDonald JW, Sadowsky C. Spinal-cord injury. Lancet (Lond, Engl). 2002;359:417–25.
Michiels J, Maasland H, Moossdorff W, Lao M, Gadiseur A, Schroyens W. Safe exclusion of deep vein thrombosis by a rapid sensitive ELISA D-dimer and compression ultrasonography in 1330 outpatients with suspected DVT. Angiology. 2016;67:781–7.
Kellermair J, Fellner A, Bittinger A, Schneider S, Akbari K, Kammler J, et al. Soluble platelet endothelial cell adhesion molecule 1 (sPECAM-1) improves diagnostic accuracy of D-Dimer in patients with suspected deep vein thrombosis (DVT). J thrombosis thrombolysis. 2020;50:380–5.
Parpia S, Takach Lapner S, Schutgens R, Elf J, Geersing G, Kearon C. Clinical pre-test probability adjusted versus age-adjusted D-dimer interpretation strategy for DVT diagnosis: A diagnostic individual patient data meta-analysis. J Thrombosis Haemost. 2020;18:669–75.
Broen K, Scholtes B, Vossen R. Predicting the need for further thrombosis diagnostics in suspected DVT is increased by using age adjusted D-dimer values. Thrombosis Res. 2016;145:107–8.
Wu J, Qing J, Yao Y, Chen D, Jiang Q. Performance of age-adjusted D-dimer values for predicting DVT before the knee and hip arthroplasty. J Orthop Surg Res. 2021;16:82.
Ghobadi A, Lin B, Musigdilok V, Park S, Palmer-Toy D, Gould M, et al. Effect of using an age-adjusted D-dimer to assess for pulmonary embolism in community emergency departments. Academic Emerg Med. 2021;28:60–69.
Ernst M, Hartz A. Phenylpropanolamine and hemorrhagic stroke. N. Engl J Med. 2001;344:1094. author reply 1095
Jaddoe V, de Jonge L, Hofman A, Franco O, Steegers E, Gaillard R. First trimester fetal growth restriction and cardiovascular risk factors in school age children: population based cohort study. BMJ (Clin Res ed). 2014;348:g14.
Piran S, Schulman S. Thromboprophylaxis in Patients with Acute Spinal Cord Injury: A Narrative Review. Semin Thrombosis Hemost. 2019;45:150–6.
Cho JH, Kim JB, Lee DG. Correlation between D-Dimer level and deep venous thrombosis in patients with acute spinal cord injuries. Am J Phys Med Rehabil. 2020;99:613–6.
Linkins LA, Takach, Lapner S. Review of D-dimer testing: Good, Bad, and Ugly. Int J Lab Hematol. 2017;39:98–103.
King A. Thrombosis: Selective D-dimer testing improves efficiency of DVT diagnosis. Nat Rev Cardiol. 2013;10:118.
Tritschler T, Kraaijpoel N, Le Gal G, Wells PS. Venous thromboembolism: advances in diagnosis and treatment. JAMA. 2018;320:1583–94.
NICE guideline NG158:Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2019). NICE guideline NG158: Available at: https://www.nice.org.uk/guidance/ng158. Last accessed 26th March 2020.
Soyode E, Pritchard W, Hayman M, Davenport A, Sivasothy P, Thomas W. Valid age-adjusted D-dimer Ambul deep vein thrombosis diagnostic Serv: beware superficial thrombophlebitis. Br J Haematol.2020;191:e94–e96.
Saraf SK, Rana RJ, Sharma OP. Venous thromboembolism in acute spinal cord injury patients. Indian J Orthop. 2007;41:194–7.
Parpia S, Takach Lapner S, Schutgens R, Elf J, Geersing GJ, Kearon C. Clinical pre-test probability adjusted versus age-adjusted D-dimer interpretation strategy for DVT diagnosis: A diagnostic individual patient data meta-analysis. J Thromb Haemost. 2020;18:669–75.
Jimenez-Guiu X, Romera-Villegas A, Huici-Sanchez M, Martinez-Rico C, Vila-Coll R. Role of an age-adjusted D-dimer cutoff level in the diagnosis algorithm of lower limb deep venous thrombosis in outpatients. J Vasc Surg Venous Lymphat Disord. 2020;8:734–40.
Myllynen P, Kammonen M, Rokkanen P, Böstman O, Lalla M, Laasonen E. Deep venous thrombosis and pulmonary embolism in patients with acute spinal cord injury: a comparison with nonparalyzed patients immobilized due to spinal fractures. J Trauma. 1985;25:541–3.
Todd JW, Frisbie JH, Rossier AB, Adams DF, Als AV, Armenia RJ, et al. Deep venous thrombosis in acute spinal cord injury: a comparison of 125I fibrinogen leg scanning, impedance plethysmography and venography. Paraplegia. 1976;14:50–7.
Chang SC, Zeng S, Tsai SJ. Outcome of different approaches to reduce urinary tract infection in patients with spinal cord lesions: a systematic review. Am J Phys Med Rehabil. 2020;99:1056–66.
Kawada T, Yoshioka T, Araki M, Nose H, Oeda T. Deep vein thrombosis and pulmonary embolism secondary to urinary retention: a case report. J Med case Rep. 2018;12:78.
Ruiz Peñalba L, López Lirola E, Pageo Giménez M, Chamorro García P. [Edema in the lower right extremity simulating deep vein thrombosis secondary to urinary retention]. Rev espanola de Geriatr y gerontologia. 2010;45:113–4.
Acknowledgements
We sincerely thank Tingting Zhang, CuicuiChang, Tingting Bao, Nanzu Chengjiang, Liai Sun, and Lina Ma for collecting and sorting participants’ data. We also thank Yan Huang, Chaomin Ni, and Ming Wu for providing the train of studying thought. We also thank Xinglin Chen for helping us to analyze the data. We would like to thank Editage (www.editage.com) for English language editing.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
JLZ: Conducted the study and wrote the draft. YYF: Designed the study, interpreted the data, and edited the manuscript. HYP, YT, JZ, and SSZ: Collected the data. CW: Planned the project, created and statistical analyzed the data. The authors all read and approved the final manuscript
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethics approval and consent to participate
Informed consent was waived due to the nature of the retrospective study for participants, which coincident with ethical requirements and waiver from the ethics committee, the study approved by Ethics Committee of First Affiliated Hospital of the University of Science and Technology of China (Anhui Provincial Hospital), the approved number was 2020-RE-008.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Zhang, J., Fang, Y., Pang, H. et al. Association of age-adjusted D-dimer with deep vein thrombosis risk in patients with spinal cord injury: a cross-sectional study. Spinal Cord 60, 90–98 (2022). https://doi.org/10.1038/s41393-021-00647-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-021-00647-z
- Springer Nature Limited
This article is cited by
-
D-dimer/fibrinogen ratio for the prediction of deep venous thrombosis after traumatic spinal cord injury
Spinal Cord (2023)
-
Role of a new age-adjusted D-dimer cutoff value for preoperative deep venous thrombosis exclusion in elderly patients with hip fractures
Journal of Orthopaedic Surgery and Research (2021)