
Abstract
Background:
Men with negative prostate biopsies or those diagnosed with low-risk or low-volume intermediate-risk prostate cancers often require a second prostate biopsy prior to a treatment decision. Prostate HistoScanning (PHS) is an ultrasound imaging test that might inform prostate biopsy in such men.
Methods:
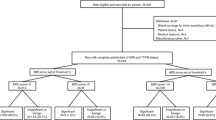
PICTURE was a prospective, paired-cohort validating trial to assess the diagnostic accuracy of imaging in men requiring a further biopsy (clinicaltrials.gov, NCT01492270) (11 January 2012–29 January 2014). We enrolled 330 men who had undergone a prior TRUS biopsy but where diagnostic uncertainty remained. All eligible men underwent PHS and transperineal template prostate mapping (TTPM) biopsy (reference standard). Men were blinded to the imaging results until after undergoing TTPM biopsies. We primarily assessed the ability of PHS to rule out clinically significant prostate (negative predictive value [NPV] and sensitivity) for a target histological condition of Gleason ≥4+3 and/or a cancer core length (MCCL) ≥6 mm. We also assessed the role of visually estimated PHS-targeted biopsies.
Results:
Of the 330 men enrolled, 249 underwent both PHS and TTPM biopsy. Mean (SD) age was 62 (7) years, median (IQR) PSA 6.8 (4.98–9.50) ng/ml, median (IQR) number of previous biopsies 1 (1–2) and mean (SD) gland size 37 (15.5) ml. One hundred and forty six (59%) had no clinically significant cancer. PHS classified 174 (70%) as suspicious. Sensitivity was 70.3% (95% CI 59.8–79.5) and NPV 41.3% (95% CI 27.0–56.8). Specificity and positive predictive value (PPV) were 14.7% (95% CI 9.1–22.0) and 36.8% (95% CI 29.6–44.4), respectively. In all, 213/220 had PHS suspicious areas targeted with targeting sensitivity 13.6% (95% CI 7.3–22.6), specificity 97.6% (95% CI 93.1–99.5), NPV 61.6% (95% CI 54.5–68.4) and PPV 80.0% (95% CI 51.9–95.7).
Conclusions:
PHS is not a useful test in men seeking risk stratification following initial prostate biopsy.

Similar content being viewed by others


References
Shaw GL, Thomas BC, Dawson SN, Srivastava G, Vowler SL, Gnanapragasam VJ, et al. Identification of pathologically insignificant prostate cancer is not accurate in unscreened men. Br J Cancer. 2014;110:2405–11.
Valerio M, Willis S, van der Meulen J, Emberton M, Ahmed HU. Methodological considerations in assessing the utility of imaging in early prostate cancer. Curr Opin Urol. 2015;25:536–42.
Valerio M, El-Shater Bosaily A, Emberton M, Ahmed HU. Defining the level of evidence for technology adoption in the localized prostate cancer pathway. Urol Oncol. 2014;32:924–30.
Barzell WE, Melamed MR, Cathcart P, Moore CM, Ahmed HU, Emberton M. Identifying candidates for active surveillance: an evaluation of the repeat biopsy strategy for men with favorable risk prostate cancer. J Urol. 2012;188:762–7.
Simmons LA, Ahmed HU, Moore CM, Punwani S, Freeman A, Hu Y, et al. The PICTURE study -- prostate imaging (multi-parametric MRI and Prostate HistoScanning) compared to transperineal ultrasound guided biopsy for significant prostate cancer risk evaluation. Contemp Clin Trials. 2014;37:69–83.
OCEBM Levels of Evidence Working Group*. “The Oxford Levels of Evidence 2”.Oxford Centre for Evidence-Based Medicine. https://www.cebm.net/index.aspx?o=5653.
Crawford ED, Rove KO, Barqawi AB, Maroni PD, Werahera PN, Baer CA, et al. Clinical-pathologic correlation between transperineal mapping biopsies of the prostate and three-dimensional reconstruction of prostatectomy specimens. Prostate. 2013;73:778–87.
Lecornet E, Ahmed HU, Hu Y, Moore CM, Nevoux P, Barratt D, et al. The accuracy of different biopsy strategies for the detection of clinically important prostate cancer: a computer simulation. J Urol. 2012;188:974–80.
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, et al. Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Ann Intern Med. 2003;138:40–4.
Simmons LA, Ahmed HU, Moore CM, Punwani S, Freeman A, Hu Y, et al. The PICTURE study - Prostate Imaging (multi-parametric MRI and Prostate HistoScanning) Compared to Transperineal Ultrasound guided biopsy for significant prostate cancer Risk Evaluation. Contemp Clin Trials. 2014;37:69–83.
Braeckman J, Autier P, Garbar C, Marichal MP, Soviany C, Nir R, et al. Computer-aided ultrasonography (HistoScanning): a novel technology for locating and characterizing prostate cancer. BJU Int. 2008;101:293–8.
Braeckman J, Autier P, Soviany C, Nir R, Nir D, Michielsen D, et al. The accuracy of transrectal ultrasonography supplemented with computer-aided ultrasonography for detecting small prostate cancers. BJU Int. 2008;102:1560–5.
Wolters T, Roobol MJ, van Leeuwen PJ, van den Bergh RC, Hoedemaeker RF, van Leenders GJ, et al. A critical analysis of the tumor volume threshold for clinically insignificant prostate cancer using a data set of a randomized screening trial. J Urol. 2011;185:121–5.
Stamey TA, Freiha FS, McNeal JE, Redwine EA, Whittemore AS, Schmid HP. Localized prostate cancer. Relationship of tumor volume to clinical significance for treatment of prostate cancer. Cancer . 1993;71(3 Suppl):933–8.
Epstein JI, Allsbrook WC, Amin MB, Egevad LL. The 2005 international society of urological pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am J Surg Pathol. 2005;2:1228–42.
Karram S, Trock BJ, Netto GJ, Epstein JI. Should intervening benign tissue be included in the measurement of discontinuous foci of cancer on prostate needle biopsy? Correlation with radical prostatectomy findings. Am J Surg Pathol. 2011;35:1351–5.
Ahmed HU, Hu Y, Carter T, Arumainayagam N, Lecornet E, Freeman A, et al. Characterizing clinically significant prostate cancer using template prostate mapping biopsy. J Urol. 2011;186:458–64.
Flahault A, Cadilhac M, Thomas G. Sample size calculation should be performed for design accuracy in diagnostic test studies. J Clin Epidemiol. 2005;58:859–62.
Salmi LR, Michel P. Sample size for diagnostic accuracy studies. J Clin Epidemiol. 2004;57:869–70. author reply71-2
Knottnerus JA, Muris JW. Assessment of the accuracy of diagnostic tests: the cross-sectional study. J Clin Epidemiol. 2003;56:1118–28.
Valerio M, Anele C, Bott SR, Charman SC, van der Meulen J, El-Mahallawi H, et al. The prevalence of clinically significant prostate cancer according to commonly used histological thresholds in men undergoing template prostate mapping biopsies. J Urol. 2016;195:1403–8.
Schiffmann J, Manka L, Boehm K, Leyh-Bannurah SR, Karakiewicz PI, Graefen M, et al. Controversial evidence for the use of HistoScanning in the detection of prostate cancer. World J Urol. 2015;33:1993–9.
Simmons LA, Autier P, Zat’ura F, Braeckman J, Peltier A, Romic I, et al. Detection, localisation and characterisation of prostate cancer by prostate HistoScanning. BJU Int. 2012;110:28–35.
Javed S, Chadwick E, Edwards AA, Beveridge S, Laing R, Bott S, et al. Does prostate HistoScanning play a role in detecting prostate cancer in routine clinical practice? Results from three independent studies. BJU Int 2014;114:541–8.
Macek P, Barret E, Sanchez-Salas R, Galiano M, Rozet F, Ahallal Y, et al. Prostate histoscanning in clinically localized biopsy proven prostate cancer: an accuracy study. J Endourol. 2014;28:371–6.
Schiffmann J, Fischer J, Tennstedt P, Beyer B, Bohm K, Michl U, et al. Comparison of prostate cancer volume measured by HistoScanning and final histopathological results. World J Urol. 2014;32:939–44.
Schiffmann J, Tennstedt P, Fischer J, Tian Z, Beyer B, Boehm K, et al. Does HistoScanning predict positive results in prostate biopsy? A retrospective analysis of 1,188 sextants of the prostate. World J Urol. 2014;32:925–30.
Acknowledgements
We would like to thank the men who participated in this study.
Funding
PICTURE received funding from the US National Institute of Health (primary award 1R01CA135089; sub-award via Riverside Research Institute NYO.G00351P.011741.12) and an unrestricted research grant from Advanced Medical Diagnostics SA.
Author contributions
Study concept and initial design: LAMS, CMM, ME, HUA. Study design and statistical analysis: HUA, Moore, ME, SCC, JvdM. Acquisition of data and data analysis and interpretation: MA, HUA, TB, SCC, ME, AF, JG, CJ, AK, NM, CMM, LAMS, JvdM. Guarantor of data: HUA.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
ME’s research is supported by core funding from the NIHR UCH/UCL Biomedical Research Centre. He is an NIHR Senior Investigator. HUA receives funding from the Wellcome Trust, MRC and Prostate Cancer UK. HUA’s research is supported by core funding from the NIHR UCH/UCL Biomedical Research Centre. HUA receives funding from Sonacare Medical, Sophiris and Trod Medical for other trials. Travel allowance was previously provided from Sonacare Inc. He is a paid consultant to Sophiris for trial-related work. ME has stock interest in Nuada Medical Ltd. He is also a consultant to Steba Biotech and GSK. He receives travel funding from Sanofi Aventis, Astellas, GSK and Sonacare. He previously received trial funding or resources from GSK, Steba Biotech and Angiodynamics and currently receives funding for trials from Sonacare Inc, Sophiris Inc and Trod Medical. AF has stock interest in Nuada Medical Ltd. All the other authors declare no conflict of interest.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Simmons, L.A.M., Kanthabalan, A., Arya, M. et al. Prostate Imaging Compared to Transperineal Ultrasound-guided biopsy for significant prostate cancer Risk Evaluation (PICTURE): a prospective cohort validating study assessing Prostate HistoScanning. Prostate Cancer Prostatic Dis 22, 261–267 (2019). https://doi.org/10.1038/s41391-018-0094-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-018-0094-1
- Springer Nature Limited
This article is cited by
-
A systematic review and meta-analysis of Histoscanning™ in prostate cancer diagnostics
World Journal of Urology (2021)
-
Prostatastanzbiopsie 2021: Wo stehen wir?*
InFo Hämatologie + Onkologie (2021)