
Abstract
The pituitary adenylate cyclase-activating polypeptide (PACAP) system is implicated in posttraumatic stress disorder (PTSD) and related amygdala-mediated arousal and threat reactivity. PTSD is characterized by increased amygdala reactivity to threat and, more recently, aberrant intrinsic connectivity of the amygdala with large-scale resting state networks, specifically the default mode network (DMN). While the influence of PACAP on amygdala reactivity has been described, its association with intrinsic amygdala connectivity remains unknown. To fill this gap, we examined functional connectivity of resting-state functional magnetic resonance imaging (fMRI) in eighty-nine trauma-exposed adults (69 female) screened for PTSD symptoms to examine the association between blood-borne (circulating) PACAP levels and amygdala-DMN connectivity. Higher circulating PACAP levels were associated with increased amygdala connectivity with posterior DMN regions, including the posterior cingulate cortex/precuneus (PCC/Precun) and left angular gyrus (lANG). Consistent with prior work, this effect was seen in female, but not male, participants and the centromedial, but not basolateral, subregions of the amygdala. Clinical association analyses linked amygdala-PCC/Precun connectivity to anxious arousal symptoms, specifically exaggerated startle response. Taken together, our findings converge with previously demonstrated effects of PACAP on amygdala activity in PTSD-related processes and offer novel evidence for an association between PACAP and intrinsic amygdala connectivity patterns in PTSD. Moreover, these data provide preliminary evidence to motivate future work ascertaining the sex- and subregion-specificity of these effects. Such findings may enable novel mechanistic insights into neural circuit dysfunction in PTSD and how the PACAP system confers risk through a disruption of intrinsic resting-state network dynamics.
Similar content being viewed by others


Introduction
Posttraumatic stress disorder (PTSD) is a severe psychiatric disorder that is characterized, in part, by sustained states of arousal and threat reactivity following a traumatic experience. PTSD is a leading cause of global disease burden and has systemic influences on emotional, neural, and broader physical health through long-lasting alterations of biological stress and arousal systems [1,2,3]. As such, multilevel systems regulating stress-mediated arousal have been implicated in vulnerability and etiopathology models of PTSD and provide key targets for investigating risk and disease progression factors [4, 5].
The pituitary adenylate cyclase-activating polypeptide (PACAP) system regulates stress responsiveness and physiological arousal and has increasingly gained recognition in PTSD. PACAP is a highly-conserved neuropeptide across species that modulates the stress response through its peripheral and central signaling in the hypothalamic-pituitary-adrenal (HPA) axis and autonomic stress pathways [6,7,8]. Paralleling decades of well-documented dysfunction of the HPA axis in PTSD [9, 10], higher circulating blood levels of long-form PACAP (PACAP38) have been found in individuals with (vs. without) PTSD, especially in participants assigned female at birth [11]. Moreover, blood-borne (circulating) PACAP and allelic variations of the predominant PACAP receptor (PAC1R) gene (ADCYAP1R1) are associated with PTSD symptom severity, specifically hyperarousal symptoms in female patients [11,12,13,14]. As such, PACAP systems may contribute to PTSD through their actions on stress-mediated arousal processes, and this pathway may be sex-dependent.
PACAP and PAC1R are densely expressed within the amygdala complex – the hub of a canonical threat circuit heavily implicated in the neuroanatomy of PTSD and related states of arousal and threat reactivity [15,16,17,18]. Prior work has linked PTSD-related polymorphisms of the PAC1R gene to increased amygdala reactivity to threat in humans [19] and to upregulation of PAC1R gene expression in the amygdala following fear conditioning in rodents [11]. Further evidence suggests this PACAP-PAC1R expression and signaling may be preferential to the central (CeA), versus basolateral (BLA), nucleus of the amygdala, and the adjacent, densely-connected bed nucleus of the stria terminalis (BNST) which together form the central extended amygdala [7, 8, 20, 21]. Consistent with the association between PACAP and symptoms of (hyper)arousal in PTSD, the CeA is integral to the expression of ‘fear’ and ‘panic’ reflexes in response to threat through axonal projections to associated arousal systems [22]. As such, preclinical studies have demonstrated a direct influence of PACAP on CeA activity and CeA-mediated fear responding [20, 23,24,25]. Taken together, these findings emphasize the potential role of PACAP on threat reactivity in stress/trauma-related disorders through the modulation of amygdala activity, which may be specific to the CeA.
While PACAP effects on amygdala signaling and activity have been well-studied in the context of threat reactivity, little is known about how the peptide influences intrinsic amygdala connectivity, especially in humans. Recently, PTSD has been increasingly characterized by a disrupted equilibrium of intrinsic resting-state neural networks [26,27,28]. Specific emphasis has been placed on aberrant coupling between salience network (SN) hubs, responsible for bottom-up arousal and detection of threat, and the default mode network (DMN), responsible for homeostatic coordination of large-scale neural activity at rest. Notably, the amygdala is a central hub of the SN whose exaggerated coupling with the DMN at rest has been implicated in both stress-induced hyperarousal and PTSD [27, 29,30,31,32,33], and this connectivity pattern may also be sex-dependent [34]. Because these intrinsic brain networks are increasingly viewed as viable mechanistic links between lower-order risk markers (i.e., genetics) and higher-order processes (i.e., task-response, behavior) [35,36,37,38,39,40], mechanistic accounts for such aberrant amygdala connectivity profiles may yield critical insights into biologically-based vulnerability and etiopathology models of PTSD.
Expanding upon the extant literature demonstrating PACAP modulation of amygdala activity, we sought to characterize the association between circulating PACAP levels and intrinsic amygdala connectivity in PTSD. Here we utilized resting-state functional connectivity of functional magnetic resonance imaging (fMRI) data in trauma-exposed adults screened for PTSD symptoms to test the hypothesis that elevated serum levels of PACAP would be associated with exaggerated amygdala connectivity with the DMN. Moreover, in keeping with the extant literature suggesting a specificity of PACAP effects to participants assigned female (vs. male) at birth and the CeA (vs. BLA), we tested the sensitivity of these associations to sex and amygdala subregions. Finally, clinical associations of identified PACAP-related connectivity profiles with relevant symptoms of hyperarousal and threat reactivity were assessed.
Materials And methods
Participants
One-hundred and thirty-six (136) trauma-exposed adults were recruited and enrolled via advertisements in the local community. Study procedures were approved by the Mass General Brigham Human Research Committee and all participants provided written informed consent. Participants were included if they met diagnostic criteria for PTSD based on the Clinician Administered PTSD Scale for DSM-5 (CAPS-5) or if they had subthreshold symptoms, defined as meeting diagnostic criteria for at least two symptom clusters [41]. Given our interest in sex differences motivated by prior work [42], participants were required to be the same sex as assigned at birth, female participants were to be premenopausal, and participants with a history of receiving hormonal replacement therapy or undergoing surgery to change biological sex were excluded. Other exclusion criteria are detailed in the Supplemental Methods.
The current sample consisted of 113 participants with resting-state fMRI data, of which 93 had usable data (excluded: excessive motion = 7, incomplete scanning = 3, inadequate structural-functional alignment = 3, significant artifact based on visual inspection = 7). Of these 93 participants, 89 had detectable serum PACAP levels, resulting in the final analyzed sample cohort of n = 89. Demographic and clinical details are provided in Table 1.
Participants completed a fasting blood draw, clinical interview, self-report questionnaires, and a 13-minute eyes-open resting-state fMRI scan.
Interview and self-report measures
Clinician administered PTSD scale for DSM-5 (CAPS-5)
The CAPS-5 [43], the gold-standard diagnostic interview for PTSD, was administered by doctoral-level clinicians. This interview consists of 30 items designed to assess the onset, duration, and impact of PTSD symptoms, yielding a determination of PTSD diagnosis and symptom severity. The hyperarousal symptom cluster (Criterion E) consists of 6 symptoms, of which 2 – hypervigilance and exaggerated startle response –form an “anxious arousal” symptom factor [44].
Life events checklist (LEC-5)
The LEC-5 [45] is a 17-item assessment of potentially traumatic events used to determine which events a participant has experienced, witnessed, or learned about happening to a family member or close friend, reflecting a Criterion A trauma.
PACAP levels
Blood samples were collected at the beginning of each study visit, between approximately 8:00–10:00 AM. Human plasma samples were prepared as described previously [11, 46], and all human PACAP38-specific measurements were performed at the University of Vermont, Larner College of Medicine, using double antibody sandwich ELISA immunoassays (Cat. No. HUFI02692, AssayGenie, Dublin, Ireland). We excluded four samples from our analyses due to undetectable PACAP levels. Outliers with exceedingly high (n = 2) or unreliably low (n = 1) concentrations of PACAP levels were winsorized to the next highest or lowest reliable/non-outlier values [46]. Additional details are reported in the Supplemental Methods.
MRI data acquisition and preprocessing
Imaging was conducted at the McLean Hospital Imaging Center on a 3 T Siemens Prisma scanner with a 64-channel head coil. Structural and functional images were initially acquired using the Human Connectome Project (HCP) Young Adult protocols (n = 15). Early in the study, imaging protocols were transitioned to the HCP Lifespan protocols (n = 78). Protocol details are documented in the Supplement. These protocols were developed to be compatible with each other [47]. As such, no effect of scanner on measures of interest was found (Supplemental Results). Results are therefore reported for the entire sample (Young Adult + Lifespan). Lifespan protocol findings are reported in the Supplemental Results.
MRI data were preprocessed using fMRIPrep version 20.2.7 [48], which is based on Nipype 1.7.0 [49]. Participants were excluded if their mean framewise displacement (FD) exceeded 0.5 mm or greater than 20% of volumes exceeded FD = 0.5 mm (n = 7) [50]. Further preprocessing details are presented in the Supplemental Methods.
Resting-state functional connectivity analyses
Additional preprocessing of resting-state fMRI data was conducted using the CONN toolbox [51], including the regression of physiological noise from white matter and cerebrospinal fluid using the CompCor method [52], scrubbing of motion outliers (FD > 0.5 mm) [50], and high pass (0.01 Hz) filtering.
Cleaned timeseries were extracted from standard left/right (l/r) amygdala (AMYG) regions of interest (ROIs) [53] and DMN ROIs. Pearson correlation analyses were performed between l/r AMYG and DMN ROI timeseries to generate individual pairwise ROI-based AMYG functional connectivity (FC) values. DMN ROIs consisted of medial prefrontal cortex (mPFC), left and right angular gyrus (l/rANG), and combined posterior cingulate cortex-precuneus (PCC-Precun) masks taken from the Brainnetome Atlas, given its superior segregation of cortical subregions based on functional and anatomical connectomics [54]. CeA and BLA AMYG subregion ROIs were generated from the JuBrain Atlas [55, 56] – note that the JuBrain Atlas combines both CeA and medial AMYG nuclei into a single centromedial (CMA) ROI, as segmentation of these adjacent subnuclei has been unreliable in human 3 T fMRI (Supplemental Materials; Fig. S1). Whole-brain seed-based correlations were performed for AMYG seeds to compute whole-brain AMYG FC maps. ROI- and seed-based FC values were Fisher’s z-transformed prior to further statistical analyses.
Statistical analyses
Pearson correlation analyses examined associations between circulating PACAP levels and pairwise ROI-based FC of the l/rAMYG with DMN ROIs. Significant effects were followed by whole-brain analyses to demonstrate the robustness and spatial specificity of the effects. Circulating PACAP levels were regressed onto whole-brain connectivity maps seeded in AMYG ROIs, demonstrating significant effects using SPM12. Whole-brain results were thresholded at p < 0.005 (uncorrected height threshold), p < 0.05 FDR-corrected cluster-size threshold. Whole-brain results not surviving correction are reported in the Supplemental Results.
Based on a priori interest in sex- and AMYG subregion-specific effects, all analyses were additionally performed on male and female participants separately, as well as CMA and BLA ROIs separately. Correlation coefficients between groups (male vs. female) and subregions (CMA vs. BLA) were compared using Fisher’s and Hittner’s r to z procedure, respectively, through the cocor package in R [57], using one-tailed tests given strong a priori hypotheses.
FC effects demonstrating a significant association with PACAP were submitted to Pearson correlation analyses with CAPS-Anxious Arousal symptom severity for clinical association analyses. Sensitivity analyses were performed across CAPS-Hyperarousal symptoms to test the unique association with startle response specifically, given its demonstrated association with the PACAP system.
All analyses were rerun with age, sex, PTSD diagnosis, and total lifetime trauma exposure as covariates, yielding equivalent results (Supplemental Results).
Results
Circulating PACAP levels are associated with increased connectivity between the amygdala and posterior DMN
Across the whole sample, ROI-based functional connectivity analyses revealed a positive association between circulating PACAP levels and rAMYG-PCC/Precun connectivity (Fig. 1A; r = 0.25, p = 0.019, FDR p < 0.05) and rAMYG-lANG connectivity (r = 0.30, p = 0.004, FDR p < 0.05), but not rAMYG-mPFC (r = −0.03, p = 0.756) or rAMYG-rANG (r = 0.15, p = 0.162). No effects were seen with the lAMYG (p’s >0.298).

A Scatterplot of ROI-based rAMYG-DMN connectivity with PACAP levels, demonstrating a unique association with posterior DMN nodes. B Whole-brain regression of PACAP levels on rAMYG seed connectivity, demonstrating the spatial specificity of these effects. Display threshold set at voxel-wise p < 0.005, k = 50. PCC posterior cingulate cortex, l/rANG left/right angular gyrus, mPFC medial prefrontal cortex. *p < 0.05, **p < 0.01.
Whole-brain regression of PACAP levels on rAMYG-seed connectivity confirmed the spatial specificity of these effects. Circulating PACAP levels were associated with greater connectivity between the rAMYG and a cluster spanning the bilateral PCC/Precuneus (Fig. 1B; k = 278, cluster FDR q = 0.006, peak = −4, −68, 26, T = 4.29) and a cluster in the lANG (k = 245, cluster FDR q = 0.006, peak = −38, −82, 26, T = 3.83). No other significant clusters emerged, and no negative associations were seen.
Sex-specific analyses
Planned analyses within each sex revealed that PACAP associations with rAMYG-PCC/Precun and rAMYG-lANG connectivity were statistically significant only in female participants (Fig. 2A; PCC/Precun: r = 0.29, p = 0.016, FDR p < 0.05; lANG: r = 0.34, p = 0.005, FDR p < 0.05). Correlations in the male participants were not significant and corresponded to smaller effect sizes (PCC/Precun: r = −0.18, p = 0.452; lANG: r = 0.06, p = 0.808). Comparison of the correlation coefficients identified a significantly stronger association in females than males for rAMYG-PCC/Precun (z = 1.77, p = 0.039 one-tailed) but not rAMYG-lANG connectivity (z = 1.08, p = 0.140 one-tailed).

A Scatterplot of ROI-based rAMYG-PCC/Precun connectivity with PACAP levels for female vs. male participants, demonstrating effects only in females. B Female whole-brain regression of PACAP on rAMYG seed connectivity demonstrated the spatial specificity of these effects. Display threshold set at voxel-wise p < 0.005 uncorrected, k > 50. Depicted coordinates are those of the main rAMYG effects in the whole sample, rather than those of the female-only participants, to illustrate similarities in cluster location and extent across analyses given the use of cluster-based statistics. *p < 0.05, **p < 0.01.
Whole-brain regression of PACAP levels on rAMYG-seed connectivity in female participants confirmed this effect (Fig. 2B; PCC/Precun: k = 319, cluster FDR q = 0.001, peak = 12, −54, 32, T = 4.09; lANG: k = 296, cluster FDR q = 0.001, peak = −52, −68, 24, T = 4.15). No other significant clusters emerged.
Amygdala subregion analyses
Across the whole sample, PACAP showed a non-significant trend association with CMA-PCC/Precun connectivity (r = 0.20, p = 0.057) but not BLA-PCC/Precun connectivity (r = 0.09, p = 0.363). Comparison of correlation coefficients revealed no significant differences in strength of association with PACAP between the CMA and BLA (p = 0.159 one-tailed). PACAP also was not significantly associated with connectivity of AMYG subregions with the lANG (CMA r = 0.17, p = 0.101; BLA r = 0.18, p = 0.088). Whole-brain analyses revealed similar patterns - the rCMA demonstrated a positive association between circulating PACAP levels and connectivity with the PCC/Precun (k = 193, cluster FDR q = 0.030, peak = 10, −56, 32, T = 4.11) but not with the lANG. No whole-brain effects emerged with the rBLA ROI.
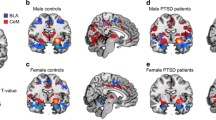
Within the female participants, PACAP was significantly associated with CMA- PCC/Precun connectivity (r = 0.25, p = 0.036; Fig. 3A), but not with BLA-PCC/Precun connectivity (r = 0.15, p = 0.223). There were no significant differences in strength of correlation between the CMA and BLA (p = 0.196 one-tailed). Within males, neither of these associations was statistically significant (CMA: r = −0.06, p = 0.795; BLA: r = −0.34, p = 0.147). Whole-brain analyses confirmed the spatial specificity of this CMA-effect in females to a bilateral PCC/Precun cluster (Fig. 3B, k = 201, cluster FDR q = 0.021, peak = 10, −54, 34, T = 4.06), with no such effects emerging with the BLA.

A Scatterplot of CMA- and BLA-PCC/Precun connectivity with PACAP levels for females vs. males. B Female whole-brain regression of PACAP on rCMA, rBLA seed connectivity. Display threshold set at voxel-wise p < 0.005 uncorrected, k > 50. Depicted coordinates mirror those of the main rAMYG effects, and not CMA-specific peak voxels, to demonstrate similarities in cluster location and extent across analyses given the use of cluster-based statistics. *p < 0.05, **p < 0.01.
Clinical associations
Clinical correlation analyses revealed that rAMYG-PCC/Precun connectivity was significantly associated with CAPS-Anxious Arousal scores (Fig. 4A, r = 0.23, p = 0.025). Sensitivity analyses revealed a specific association of this connectivity with the CAPS – Startle Response (r = 0.23, p = 0.025) and no other hyperarousal symptoms (p’s >0.142). This effect was not sex-specific (females/males r = 0.20/0.36, p = 0.096/0.100). No clinical associations were seen for rAMYG-lANG connectivity (p’s >0.273). Evaluation of AMYG subregions revealed no unique subregion effects (p’s >0.128). No interaction between circulating PACAP levels and rAMYG-PCC/Precun connectivity was found in relation to Anxious Arousal (p = 0.436) or Startle Response (p = 0.655) symptoms.

A Scatterplot of rAMYG-PCC/Precun connectivity with CAPS-Anxious Arousal and Startle Response symptom scores. B Whole-brain regression of CAPS-Anxious Arousal and Startle Response symptom scores on rAMYG seed connectivity. Display threshold set at voxel-wise p < 0.005 uncorrected, k > 50.
Whole-brain regression of CAPS-Anxious Arousal demonstrated a positive association with increased connectivity between rAMYG and a cluster spanning the right PCC/Precuneus (Fig. 4B, k = 158, cluster FDR q = 0.082, peak = 12, −60, 40, T = 3.78) as well as a bilateral cluster in the dorsal PCC (k = 138, cluster FDR q = 0.082, peak = −6, −26, 32, T = 3.93). CAPS-Startle Response was associated with increased connectivity between the rAMYG and a cluster spanning the right PCC/Precuneus; however, this did not survive correction (k = 122, cluster FDR q = 0.166, peak = 6, −62, 22, T = 3.56).
Discussion
Expanding upon the growing literature demonstrating an influence of PACAP on amygdala activity, we demonstrate here that circulating levels of PACAP are associated with increased intrinsic functional connectivity between the amygdala and posterior regions of the DMN. A similar connectivity profile is associated with anxious arousal symptoms, specifically startle response, which is consistent with prior work demonstrating a unique effect of PACAP on arousal and threat reflexes. In keeping with this prior work, our data suggest these PACAP effects on amygdala connectivity may be unique to females and, to a lesser extent, the centromedial amygdala; however, these effects should be interpreted with caution (see below).
These findings emerge in the context of accruing evidence for exaggerated coupling between the intrinsically anti-correlated SN and DMN in PTSD. Exaggerated connectivity between the amygdala (SN) and the PCC/Precuneus (DMN) has been implicated in risk, severity, and maintenance of PTSD [27, 31, 58, 59]. Such connectivity patterns are similarly implicated in transdiagnostic processes of aberrant stress response [29, 33], threat reactivity [32], and trait anxiety [60, 61]. Functionally, this specific circuit, and broader SN-DMN coupling, is suggested to regulate attentional deployment to salient threat cues, with intrinsic anti-correlation between these structures/networks reflecting homeostatic inhibition of threat orientation at rest [26, 28, 62, 63]. Our clinical association analyses support this notion, with increased AMYG-PCC/Precun connectivity demonstrating unique associations with subjective reports of exaggerated startle response. This key translational threat-orienting behavior is known to be affected by the PACAP system [25, 64]. Taken together, these findings align with the proposed role of PACAP signaling within the amygdala to elicit stress responses and behavioral reflexes to threat.
This purported association of PACAP with behavioral threat reflexes is further supported by the specificity of our PACAP findings to the right amygdala and, to a lesser extent, the CMA. Post-hoc analyses revealed a significant effect of hemisphere (left vs. right AMYG) on the association between PACAP and AMYG connectivity (p = 0.013). Although findings regarding laterality of amygdala structure and function are heterogeneous, a recent review of amygdala laterality suggests a right-hemispheric dominance in neuropeptide expression, specifically under stress, and functional specialization in rapid fear/threat processing and responding [65]. However, the authors note lateralization of subnuclei effects remains understudied in humans, due in part to limits to the spatial resolution of human functional imaging. Notably, our analyses utilized a combined centromedial ROI, which may have contributed to the lack of significant contrasts of CMA vs. BLA connectivity, as evidence for PACAP influence on medial amygdala activity is sparse [66]. The lack of significant differences between the association of CMA and BLA connectivity with PACAP precludes any statements of subregion specificity from the current sample. Nonetheless, that the effects emerged in the CMA and not the BLA provides preliminary evidence for potential subregion differences. Therefore, future studies utilizing more refined parcellations of amygdala nuclei, including the adjacent BNST, are needed to ascertain subnuclei specificity of PACAP effects in humans. Keeping these considerations in mind, our findings align with the extant literature suggesting an effect of PACAP on behavioral threat responses via central amygdala signaling [20, 25, 67]. That these effects are present even at rest suggests a “rewiring” of the intrinsic functional architecture of the amygdala by PACAP to prime behavioral responses to threat.
While the cross-sectional nature of our data limits the determination of causal mechanisms linking PACAP with aberrant intrinsic amygdala connectivity, answers may lie in the demonstrated neuroplastic effects of PACAP. Rodent studies have identified robust neurotrophic [68, 69] and neuroplastic [70,71,72] properties of PACAP, especially within the central extended amygdala [73], which are enhanced under stress [21]. Such properties parallel general stress-induced increases in neuroplasticity within the central extended amygdala [74, 75], which has been linked to sustained anxiety-like states through strengthened synaptic transmission between neural structures recruited in threat processing [76, 77]. Notably, acute stress results in activation and increased coupling of central SN and DMN hubs [30]. Sustained effects of stress are further associated with co-activations of the amygdala and posterior midline DMN structures, including the PCC/Precuneus [29, 33], which together demonstrate similar metabolic profiles in response to reactivation of threat memory [78]. As such, the enhanced neuroplastic properties of PACAP under stress may strengthen the synaptic transmission between the co-activated amygdala and PCC/Precuneus, resulting in lasting increases in intrinsic functional connectivity and sustained changes in resting-state network dynamics. Investigating the directionality and causality of PACAP signaling could lead to promising therapeutic avenues for modulating its effects through the right combination of agonism and antagonism of its receptors [79].
Associations between PACAP and amygdala connectivity emerged within the angular gyrus (ANG) as well. Positioned as a lateral node of the DMN, the ANG is a densely connected structure that sits at the junction of multiple functional systems and has thus been implicated as a cross-modal hub [80]. Less frequently implicated in states of stress or threat-mediated arousal, the observed functional coupling between the amygdala and lANG may reflect broader increases in amygdala-DMN coupling. Additionally, as a cross-modal hub linking external sensory processing with internal, self-referential representations and memories [81, 82], this amygdala-lANG coupling may reflect higher-order threat processes, such as threat-associated memory retrieval. This is supported by a lack of association between PACAP and lANG connectivity with the CMA or with the lower-order startle response symptom, suggesting a general coupling with the amygdala that is not specific to threat-reactive reflexes.
Surprisingly, we found no associations between PACAP levels and amygdala-prefrontal cortex connectivity. The amygdala-prefrontal circuit has been at the forefront of neurocircuitry models of PTSD for decades [15, 16, 83,84,85] and has been reliably implicated in the regulation of fear acquisition, expression, and extinction [86,87,88]. Evidence suggests PACAP is markedly expressed within prefrontal (infralimbic in rodents) structures, through which it may play a mechanistic role in fear learning and extinction [89]. However, prior human studies have similarly found no association between the PACAP-PAC1R system and prefrontal activity in relation to PTSD or threat reactivity [19]. Additionally, structures of the medial prefrontal cortex serve as anterior hubs of the DMN which are disrupted in PTSD [90]; however, our findings demonstrate a unique effect with posterior DMN hubs. Notably, the PCC/Precuneus and amygdala are positioned at the apex of the cortical and subcortical functional connectivity hierarchy, respectively [91, 92], and may thus serve as intrinsic connectivity hubs. Therefore, PACAP’s effects on intrinsic connectivity of the amygdala may be unique to these resting-state hubs, whereas its influence on the prefrontal cortex may be task-dependent. Moreover, heterogeneity in prefrontal cortex findings in PTSD [93, 94] mirrors the heterogeneity of prefrontal subregions and their distinct task-dependent functions [86, 95]. More comprehensive investigations into the role of PACAP in the intrinsic connectivity of the human PFC are needed to elucidate these spatial and functional nuances.
Our data suggest that the purported role of PACAP on intrinsic amygdala connectivity may be sex specific. Direct comparisons between sexes in the current sample should be interpreted with caution given significant discrepancies in sample sizes and an insufficient number of male participants to reliably detect group differences. Keeping this limitation in mind, our contrasts of correlation coefficients revealed stronger associations in females. This aligns with initial work demonstrating an association between circulating PACAP levels and PTSD that is unique to female patients [11], as well as preclinical work demonstrating estrogenic modulation of the PACAP-PAC1R system [11, 42, 96]. The observed sex differences in PACAP levels in our sample (Table 1) were robust to other demographic and clinical variables, lending further credence to the potential sexual dimorphism of the PACAP system in PTSD (Supplemental Results). Moreover, the identified PACAP-associated AMYG-PCC/Precun circuit has been previously shown to be sex-dependent and uniquely elevated in female patients with PTSD [34]. Therefore, PACAP-associated alterations of intrinsic amygdala connectivity may yield important insights into our mechanistic understanding of the increased prevalence and risk of PTSD in individuals assigned female at birth. Future studies matching biological sex groups and investigating gonadal hormone levels are needed to delineate the true sex-specificity of PACAP’s effects on intrinsic amygdala connectivity in humans.
Finally, as the current study investigated circulating serum PACAP levels, it is unclear if this association between PACAP and amygdala-DMN connectivity reflects a risk marker for PTSD, and/or physiological sequalae of the condition. Genetic variants associated with an altered PACAP-PAC1R system have been implicated as risk markers for PTSD through changes in neural activity [11, 97]. Moreover, genetic risk for related dysfunction of the HPA axis and stress-sensitive serotonergic systems has been linked to amygdala and PCC/Precuneus activity [98,99,100]. Additionally, recent work in non-PTSD anxious patients also supports a PACAP-related relationship to anxiety- or stress-sensitivity [46]. Taken together, these data position this circuit and its association with PACAP as a potential intermediate phenotype of interest. However, phasic elevations of circulating PACAP also have been found after acute and sustained stress, reflecting a state-like process or prolonged stress-response [25, 101], and mirror the state-like alterations of amygdala-PCC/Precuneus connectivity in response to acute and chronic stress. Therefore, evaluations of PACAP-PAC1R risk genes and pathways are needed to further elucidate the role of PACAP-associated intrinsic amygdala connectivity in risk or pathophysiology models of PTSD.
In addition to the limitations addressed above, the clinical associations in the present sample were noticeably weak. While we restricted our analyses to a priori symptoms of anxious arousal and the connectivity paths demonstrating a significant association with PACAP, the results more broadly did not survive correction for multiple comparisons across all tested brain regions and other symptoms tested in our sensitivity analyses. Moreover, the unique sex- and subregion effects with PACAP were not seen in these clinical associations. The strength of these effects may have been hindered by our lack of “true” controls, as all participants were recruited based on sub-/threshold PTSD symptoms. This was initially chosen to explore mechanistic processes of heterogeneity within the disorder; however, this may have restricted the range and distribution of symptom severity, and subsequently their underlying processes, and precludes statements about PTSD-specific effects. Additionally, we utilized clinician-measured symptom severity from participants’ interview-based self-reports, which may be too distal of a measure of these behavior-centric symptoms (i.e., arousal and startle response). More objective measures of these symptoms that are closer to the biological processes of interest along the units of analysis spectrum may be needed to capture these mechanistic nuances of sex- and subregion-specificity [102]. Given these weaknesses, we limited our discussion of these findings to their contextualization of our main findings within the prior literature. This calls for future studies incorporating physiological markers of anxious arousal, such as startle response, skin conductance, or pupillometry, in both PTSD and trauma-exposed controls to better elucidate the clinical relevance of these results.
The present findings provide initial evidence for an association between PACAP and intrinsic amygdala functional connectivity in PTSD. That the identified network has been reliably implicated in PTSD risk and symptom severity, as well as related transdiagnostic processes, adds to the growing body of evidence implicating the PACAP system in PTSD and stress-related arousal. Moreover, it offers novel mechanistic insights into dysfunctional neural circuitry in PTSD and how the PACAP system may confer risk for PTSD through disruption of intrinsic resting-state network dynamics.
References
McFARLANE AC. The long-term costs of traumatic stress: intertwined physical and psychological consequences. World Psychiatry. 2010;9:3–10.
McEwen BS. Allostasis and allostatic load: implications for neuropsychopharmacology. Neuropsychopharmacology. 2000;22:108–24.
O’Connor DB, Thayer JF, Vedhara K. Stress and health: a review of psychobiological processes. Annu Rev Psychol. 2021;72:663–88.
Jovanovic T, Norrholm SD. Neural mechanisms of impaired fear inhibition in posttraumatic stress disorder. Front Behav Neurosci. 2011;5:44.
Jovanovic T, Ressler KJ. How the neurocircuitry and genetics of fear inhibition may inform our understanding of PTSD. Am J Psychiatry. 2010;167:648–62.
Stroth N, Holighaus Y, Ait-Ali D, Eiden LE. PACAP: a master regulator of neuroendocrine stress circuits and the cellular stress response. Ann N. Y Acad Sci. 2011;1220:49–59.
Hashimoto H, Shintani N, Tanida M, Hayata A, Hashimoto R, Baba A. PACAP is implicated in the stress axes. Curr Pharm Des. 2011;17:985–9.
Hammack SE, May V. Pituitary adenylate cyclase activating polypeptide in stress-related disorders: data convergence from animal and human studies. Biol Psychiatry. 2015;78:167–77.
Yehuda R, LeDoux J. Response variation following trauma: a translational neuroscience approach to understanding PTSD. Neuron 2007;56:19–32.
de Kloet CS, Vermetten E, Geuze E, Kavelaars A, Heijnen CJ, Westenberg HGM. Assessment of HPA-axis function in posttraumatic stress disorder: Pharmacological and non-pharmacological challenge tests, a review. J Psychiatr Res. 2006;40:550–67.
Ressler KJ, Mercer KB, Bradley B, Jovanovic T, Mahan A, Kerley K, et al. Post-traumatic stress disorder is associated with PACAP and the PAC1 receptor. Nature. 2011;470:492–7.
Almli LM, Mercer KB, Kerley K, Feng H, Bradley B, Conneely KN, et al. ADCYAP1R1 genotype associates with post-traumatic stress symptoms in highly traumatized African-American females. Am J Med Genet B Neuropsychiatr Genet. 2013;162B:262–72.
Lind MJ, Marraccini ME, Sheerin CM, Bountress K, Bacanu S-A, Amstadter AB, et al. Association of posttraumatic stress disorder with rs2267735 in the ADCYAP1R1 gene: a meta-analysis. J Trauma Stress. 2017;30:389–98.
Zhang J, Li G, Yang H, Cao C, Fang R, Liu P, et al. The main effect and gene-environment interaction effect of the ADCYAP1R1 polymorphism rs2267735 on the course of posttraumatic stress disorder symptoms-A longitudinal analysis. Front Psychiatry. 2022;13:1032837.
Ressler KJ, Berretta S, Bolshakov VY, Rosso IM, Meloni EG, Rauch SL, et al. Post-traumatic stress disorder: clinical and translational neuroscience from cells to circuits. Nat Rev Neurol. 2022;18:273–88.
Shin LM, Rauch SL, Pitman RK. Amygdala, medial prefrontal cortex, and hippocampal function in PTSD. Ann N. Y Acad Sci. 2006;1071:67–79.
Rauch SL, Shin LM, Phelps EA. Neurocircuitry models of posttraumatic stress disorder and extinction: human neuroimaging research-past, present, and future. Biol Psychiatry. 2006;60:376–82.
Patel R, Spreng RN, Shin LM, Girard TA. Neurocircuitry models of posttraumatic stress disorder and beyond: a meta-analysis of functional neuroimaging studies. Neurosci Biobehav Rev. 2012;36:2130–42.
Stevens JS, Almli LM, Fani N, Gutman DA, Bradley B, Norrholm SD, et al. PACAP receptor gene polymorphism impacts fear responses in the amygdala and hippocampus. Proc Natl Acad Sci USA. 2014;111:3158–63.
Missig G, Roman CW, Vizzard MA, Braas KM, Hammack SE, May V. Parabrachial nucleus (PBn) pituitary adenylate cyclase activating polypeptide (PACAP) signaling in the amygdala: implication for the sensory and behavioral effects of pain. Neuropharmacology. 2014;86:38–48.
Boucher MN, May V, Braas KM, Hammack SE. PACAP orchestration of stress-related responses in neural circuits. Peptides. 2021;142:170554.
Davis M. The role of the amygdala in fear and anxiety. Annu Rev Neurosci. 1992;15:353–75.
Cho J-H, Zushida K, Shumyatsky GP, Carlezon WA, Meloni EG, Bolshakov VY. Pituitary adenylate cyclase-activating polypeptide induces postsynaptically expressed potentiation in the intra-amygdala circuit. J Neurosci. 2012;32:14165–77.
Legradi G, Das M, Giunta B, Hirani K, Mitchell EA, Diamond DM. Microinfusion of pituitary adenylate cyclase-activating polypeptide into the central nucleus of amygdala of the rat produces a shift from an active to passive mode of coping in the shock-probe fear/defensive burying test. Neural Plast. 2007;2007:79102.
Seiglie MP, Huang L, Cottone P, Sabino V. Role of the PACAP system of the extended amygdala in the acoustic startle response in rats. Neuropharmacology. 2019;160:107761.
Sripada RK, King AP, Welsh RC, Garfinkel SN, Wang X, Sripada CS, et al. Neural dysregulation in posttraumatic stress disorder: evidence for disrupted equilibrium between salience and default mode brain networks. Psychosom Med. 2012;74:904–11.
Lanius RA, Bluhm RL, Coupland NJ, Hegadoren KM, Rowe B, Théberge J, et al. Default mode network connectivity as a predictor of post-traumatic stress disorder symptom severity in acutely traumatized subjects. Acta Psychiatr Scand. 2010;121:33–40.
Lanius RA, Frewen PA, Tursich M, Jetly R, McKinnon MC. Restoring large-scale brain networks in PTSD and related disorders: a proposal for neuroscientifically-informed treatment interventions. Eur J Psychotraumatol. 2015;6:27313.
Maron-Katz A, Vaisvaser S, Lin T, Hendler T, Shamir R. A large-scale perspective on stress-induced alterations in resting-state networks. Sci Rep. 2016;6:21503.
Zhang W, Llera A, Hashemi MM, Kaldewaij R, Koch SBJ, Beckmann CF, et al. Discriminating stress from rest based on resting-state connectivity of the human brain: a supervised machine learning study. Hum Brain Mapp. 2020;41:3089–99.
Sheynin J, Duval ER, King AP, Angstadt M, Phan KL, Simon NM, et al. Associations between resting-state functional connectivity and treatment response in a randomized clinical trial for posttraumatic stress disorder. Depress Anxiety. 2020;37:1037–46.
Rabellino D, Tursich M, Frewen PA, Daniels JK, Densmore M, Théberge J, et al. Intrinsic connectivity networks in post-traumatic stress disorder during sub- and supraliminal processing of threat-related stimuli. Acta Psychiatr Scand. 2015;132:365–78.
Veer IM, Oei NYL, Spinhoven P, van Buchem MA, Elzinga BM, Rombouts SARB. Beyond acute social stress: increased functional connectivity between amygdala and cortical midline structures. Neuroimage. 2011;57:1534–41.
Helpman L, Zhu X, Zilcha-Mano S, Suarez-Jimenez B, Lazarov A, Rutherford B, et al. Reversed patterns of resting state functional connectivity for females vs. males in posttraumatic stress disorder. Neurobiol Stress. 2021;15:100389.
Finn ES, Shen X, Scheinost D, Rosenberg MD, Huang J, Chun MM, et al. Functional connectome fingerprinting: identifying individuals using patterns of brain connectivity. Nat Neurosci. 2015;18:1664–71.
Rosenberg MD, Finn ES, Scheinost D, Papademetris X, Shen X, Constable RT, et al. A neuromarker of sustained attention from whole-brain functional connectivity. Nat Neurosci. 2016;19:165–71.
Glahn DC, Winkler AM, Kochunov P, Almasy L, Duggirala R, Carless MA, et al. Genetic control over the resting brain. Proc Natl Acad Sci USA. 2010;107:1223–8.
Elliott ML, Knodt AR, Cooke M, Kim MJ, Melzer TR, Keenan R, et al. General functional connectivity: shared features of resting-state and task fMRI drive reliable and heritable individual differences in functional brain networks. Neuroimage. 2019;189:516–32.
Zhao B, Li T, Smith SM, Xiong D, Wang X, Yang Y, et al. Common variants contribute to intrinsic human brain functional networks. Nat Genet. 2022;54:508–17.
Harnett NG, Lebois LAM. Leveraging resting-state neurophenotypes to identify susceptibility to and heterogeneity of posttraumatic stress disorder. Neuropsychopharmacology. 2022;47:403–4.
McLaughlin KA, Koenen KC, Friedman MJ, Ruscio AM, Karam EG, Shahly V, et al. Sub-threshold post traumatic stress disorder in the WHO world mental health surveys. Biol Psychiatry. 2015;77:375–84.
King SB, Toufexis DJ, Hammack SE. Pituitary adenylate cyclase activating polypeptide (PACAP), stress, and sex hormones. Stress. 2017;20:465–75.
Weathers FW, Bovin MJ, Lee DJ, Sloan DM, Schnurr PP, Kaloupek DG, et al. The clinician-administered PTSD scale for DSM-5 (CAPS-5): development and initial psychometric evaluation in military veterans. Psychol Assess. 2018;30:383–95.
Elhai JD, Palmieri PA. The factor structure of posttraumatic stress disorder: a literature update, critique of methodology, and agenda for future research. J Anxiety Disord. 2011;25:849–54.
Gray MJ, Litz BT, Hsu JL, Lombardo TW. Psychometric properties of the life events checklist. Assessment. 2004;11:330–41.
Ross RA, Hoeppner SS, Hellberg SN, O’Day EB, Rosencrans PL, Ressler KJ, et al. Circulating PACAP peptide and PAC1R genotype as possible transdiagnostic biomarkers for anxiety disorders in women: a preliminary study. Neuropsychopharmacology. 2020;45:1125–33.
Harms MP, Somerville LH, Ances BM, Andersson J, Barch DM, Bastiani M, et al. Extending the human connectome project across ages: imaging protocols for the lifespan development and aging projects. Neuroimage. 2018;183:972–84.
Esteban O, Markiewicz CJ, Blair RW, Moodie CA, Isik AI, Erramuzpe A, et al. fMRIPrep: a robust preprocessing pipeline for functional MRI. Nat Methods. 2019;16:111–6.
Gorgolewski K, Burns CD, Madison C, Clark D, Halchenko YO, Waskom ML, et al. Nipype: a flexible, lightweight and extensible neuroimaging data processing framework in python. Front Neuroinform. 2011;5:13.
Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage. 2012;59:2142–54.
Whitfield-Gabrieli S, Nieto-Castanon A. Conn: a functional connectivity toolbox for correlated and anticorrelated brain networks. Brain Connect. 2012;2:125–41.
Behzadi Y, Restom K, Liau J, Liu TT. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage. 2007;37:90–101.
Frazier JA, Chiu S, Breeze JL, Makris N, Lange N, Kennedy DN, et al. Structural brain magnetic resonance imaging of limbic and thalamic volumes in pediatric bipolar disorder. AJP. 2005;162:1256–65.
Fan L, Li H, Zhuo J, Zhang Y, Wang J, Chen L, et al. The human brainnetome atlas: a new brain atlas based on connectional architecture. Cereb Cortex. 2016;26:3508–26.
Eickhoff S, Walters NB, Schleicher A, Kril J, Egan GF, Zilles K, et al. High-resolution MRI reflects myeloarchitecture and cytoarchitecture of human cerebral cortex. Hum Brain Mapp. 2005;24:206–15.
Amunts K, Kedo O, Kindler M, Pieperhoff P, Mohlberg H, Shah NJ, et al. Cytoarchitectonic mapping of the human amygdala, hippocampal region and entorhinal cortex: intersubject variability and probability maps. Anat Embryol (Berl). 2005;210:343–52.
Diedenhofen B, Musch J. Cocor: a comprehensive solution for the statistical comparison of correlations. PLOS ONE. 2015;10:e0121945.
Bluhm RL, Williamson PC, Osuch EA, Frewen PA, Stevens TK, Boksman K, et al. Alterations in default network connectivity in posttraumatic stress disorder related to early-life trauma. J Psychiatry Neurosci. 2009;34:187–94.
Lieberman JM, Rabellino D, Densmore M, Frewen PA, Steyrl D, Scharnowski F, et al. Posterior cingulate cortex targeted real-time fMRI neurofeedback recalibrates functional connectivity with the amygdala, posterior insula, and default-mode network in PTSD. Brain and Behavior. 2023;13:e2883.
Geng H, Wang Y, Gu R, Luo Y-J, Xu P, Huang Y, et al. Altered brain activation and connectivity during anticipation of uncertain threat in trait anxiety. Hum Brain Mapp. 2018;39:3898–914.
Toazza R, Franco AR, Buchweitz A, Molle RD, Rodrigues DM, Reis RS, et al. Amygdala-based intrinsic functional connectivity and anxiety disorders in adolescents and young adults. Psychiatry Res Neuroimaging. 2016;257:11–6.
Ferri J, Schmidt J, Hajcak G, Canli T. Emotion regulation and amygdala-precuneus connectivity: Focusing on attentional deployment. Cogn Affect Behav Neurosci. 2016;16:991–1002.
van Oort J, Tendolkar I, Hermans EJ, Mulders PC, Beckmann CF, Schene AH, et al. How the brain connects in response to acute stress: a review at the human brain systems level. Neurosci Biobehav Rev. 2017;83:281–97.
Jovanovic T, Norrholm SD, Davis J, Mercer KB, Almli L, Nelson A, et al. PAC1 receptor (ADCYAP1R1) genotype is associated with dark-enhanced startle in children. Mol Psychiatry. 2013;18:742–3.
Ocklenburg S, Peterburs J, Mundorf A. Hemispheric asymmetries in the amygdala: a comparative primer. Prog Neurobiol. 2022;214:102283.
Velasco ER, Florido A, Flores Á, Senabre E, Gomez-Gomez A, Torres A, et al. PACAP-PAC1R modulates fear extinction via the ventromedial hypothalamus. Nat Commun. 2022;13:4374.
Iemolo A, Seiglie M, Blasio A, Cottone P, Sabino V. Pituitary adenylate cyclase-activating polypeptide (PACAP) in the central nucleus of the amygdala induces anxiety via melanocortin receptors. Psychopharmacology. 2016;233:3269–77.
May V, Lutz E, MacKenzie C, Schutz KC, Dozark K, Braas KM. Pituitary adenylate cyclase-activating polypeptide (PACAP)/PAC1HOP1 receptor activation coordinates multiple neurotrophic signaling pathways: Akt activation through phosphatidylinositol 3-kinase gamma and vesicle endocytosis for neuronal survival. J Biol Chem. 2010;285:9749–61.
Mercer A, Rönnholm H, Holmberg J, Lundh H, Heidrich J, Zachrisson O, et al. PACAP promotes neural stem cell proliferation in adult mouse brain. J Neurosci Res. 2004;76:205–15.
Johnson GC, May V, Parsons RL, Hammack SE. Parallel signaling pathways of pituitary adenylate cyclase activating polypeptide (PACAP) regulate several intrinsic ion channels. Ann N. Y Acad Sci. 2019;1455:105–12.
Miles OW, May V, Hammack SE. Pituitary Adenylate Cyclase-Activating Peptide (PACAP) Signaling and the Dark Side of Addiction. J Mol Neurosci. 2019;68:453–64.
Yang K, Lei G, Jackson MF, Macdonald JF. The involvement of PACAP/VIP system in the synaptic transmission in the hippocampus. J Mol Neurosci. 2010;42:319–26.
Meloni EG, Kaye KT, Venkataraman A, Carlezon WA. PACAP increases Arc/Arg 3.1 expression within the extended amygdala after fear conditioning in rats. Neurobiol Learn Mem. 2019;157:24–34.
Zhang X, Ge TT, Yin G, Cui R, Zhao G, Yang W. Stress-induced functional alterations in Amygdala: implications for neuropsychiatric diseases. Front Neurosci. 2018;12:367.
Pêgo JM, Morgado P, Pinto LG, Cerqueira JJ, Almeida OFX, Sousa N. Dissociation of the morphological correlates of stress-induced anxiety and fear. Eur J Neurosci. 2008;27:1503–16.
Pittenger C, Duman RS. Stress, depression, and neuroplasticity: a convergence of mechanisms. Neuropsychopharmacology. 2008;33:88–109.
McEwen BS, Gianaros PJ. Stress- and allostasis-induced brain plasticity. Annu Rev Med. 2011;62:431–45.
Jeon Y, Lim Y, Yeom J, Kim E-K. Comparative metabolic profiling of posterior parietal cortex, amygdala, and hippocampus in conditioned fear memory. Mol Brain. 2021;14:153.
Tasma Z, Siow A, Harris PWR, Brimble MA, Hay DL, Walker CS. Characterisation of agonist signalling profiles and agonist-dependent antagonism at PACAP-responsive receptors: Implications for drug discovery. Br J Pharmacol. 2022;179:435–53.
Seghier ML. The angular gyrus: multiple functions and multiple subdivisions. Neuroscientist. 2013;19:43–61.
Tibon R, Fuhrmann D, Levy DA, Simons JS, Henson RN. Multimodal integration and vividness in the angular gyrus during episodic encoding and retrieval. J Neurosci. 2019;39:4365–74.
Bonnici HM, Richter FR, Yazar Y, Simons JS. Multimodal feature integration in the angular gyrus during episodic and semantic retrieval. J Neurosci. 2016;36:5462–71.
Fenster RJ, Lebois LAM, Ressler KJ, Suh J. Brain circuit dysfunction in post-traumatic stress disorder: from mouse to man. Nat Rev Neurosci. 2018;19:535–51.
Koenigs M, Grafman J. Posttraumatic stress disorder: the role of medial prefrontal cortex and amygdala. Neuroscientist. 2009;15:540–8.
Rauch SL, Shin LM. Functional neuroimaging studies in posttraumatic stress disorder. Ann N. Y Acad Sci. 1997;821:83–98.
Hiser J, Koenigs M. The multifaceted role of the ventromedial prefrontal cortex in emotion, decision making, social cognition, and psychopathology. Biol Psychiatry. 2018;83:638–47.
Phelps EA, Delgado MR, Nearing KI, LeDoux JE. Extinction learning in humans: role of the amygdala and vmPFC. Neuron. 2004;43:897–905.
Giustino TF, Maren S. The role of the medial prefrontal cortex in the conditioning and extinction of fear. Front Behav Neurosci. 2015;9:298.
Martelle SE, Cotella EM, Nawreen N, Chen C, Packard BA, Fitzgerald M, et al. Prefrontal cortex PACAP signaling: organization and role in stress regulation. Stress. 2021;24:196–205.
Akiki TJ, Averill CL, Wrocklage KM, Scott JC, Averill LA, Schweinsburg B, et al. Default mode network abnormalities in posttraumatic stress disorder: A novel network-restricted topology approach. Neuroimage. 2018;176:489–98.
Cole MW, Pathak S, Schneider W. Identifying the brain’s most globally connected regions. Neuroimage. 2010;49:3132–48.
Tomasi D, Volkow ND. Functional connectivity hubs in the human brain. Neuroimage. 2011;57:908–17.
Olson EA, Kaiser RH, Pizzagalli DA, Rauch SL, Rosso IM. Regional prefrontal resting-state functional connectivity in posttraumatic stress disorder. Biol Psychiatry Cogn Neurosci Neuroimaging. 2019;4:390–8.
Neria Y. Functional neuroimaging in PTSD: from discovery of underlying mechanisms to addressing diagnostic heterogeneity. Am J Psychiatry. 2021;178:128–35.
Pizzagalli DA, Roberts AC. Prefrontal cortex and depression. Neuropsychopharmacology. 2022;47:225–46.
Mercer KB, Dias B, Shafer D, Maddox SA, Mulle JG, Hu P, et al. Functional evaluation of a PTSD-associated genetic variant: estradiol regulation and ADCYAP1R1. Transl Psychiatry. 2016;6:e978.
Pohlack ST, Nees F, Ruttorf M, Cacciaglia R, Winkelmann T, Schad LR, et al. Neural mechanism of a sex-specific risk variant for posttraumatic stress disorder in the Type I receptor of the pituitary adenylate cyclase activating polypeptide. Biol Psychiatry. 2015;78:840–7.
Madsen MK, Mc Mahon B, Andersen SB, Siebner HR, Knudsen GM, Fisher PM. Threat-related amygdala functional connectivity is associated with 5-HTTLPR genotype and neuroticism. Soc Cogn Affect Neurosci. 2016;11:140–9.
Vai B, Serretti A, Poletti S, Mascia M, Lorenzi C, Colombo C, et al. Cortico-limbic functional connectivity mediates the effect of early life stress on suicidality in bipolar depressed 5-HTTLPR*s carriers. J Affect Disord. 2020;263:420–7.
Rogers J, Raveendran M, Fawcett GL, Fox AS, Shelton SE, Oler JA, et al. CRHR1 genotypes, neural circuits and the diathesis for anxiety and depression. Mol Psychiatry. 2013;18:700–7.
Seiglie MP, Lepeak L, Velázquez-Sanchez C, Ferragud A, Le T, Cottone P, et al. The pituitary adenylate cyclase-activating polypeptide (PACAP) system of the central amygdala mediates the detrimental effects of chronic social defeat stress in rats. ENeuro. 2022;9:ENEURO.0260–22.2022.
Patrick CJ, Hajcak G. RDoC: translating promise into progress: RDoC: translating promise into progress. Psychophysiology. 2016;53:415–24.
Funding
This work was supported by NIH awards P50-MH115874 (to WAC, KJR; Project 4: IMR, SLR), R01-MH120400 (IMR), and R01-MH97988 (SEH and VM).
Author information
Authors and Affiliations
Contributions
KJC performed data processing, statistical analyses, and wrote the initial draft of the manuscript. QD and PK assisted in collection, processing, and analysis of fMRI data. VM and SEH performed analysis of PACAP data. CDP and NPD assisted in the collection and processing of PACAP samples. EA, EJC, and SAJ contributed to all data collection, management, and processing. MWL processed self-report and clinical interview data. WAC, KJR, SLR, and IMR obtained funding and contributed to study design and conceptualization. SLR and IMR conceived the study. All authors provided critical input to the manuscript, contributed to revised drafts, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
For completeness of disclosure: SLR has been employed by Mass General Brigham/McLean Hospital; paid as secretary of Society of Biological Psychiatry, and for Board service to Mindpath Health/Community Psychiatry and National Association of Behavioral Healthcare; served as volunteer member of the Board for Anxiety & Depression Association of America, and The National Network of Depression Centers; received royalties from Oxford University Press, American Psychiatric Publishing Inc, and Springer Publishing; received research funding from NIMH. WAC is a member of the NPP Editorial Board. Within the past 3 years, WAC has served as a consultant for Psy Therapeutics and has had sponsored research agreements with Cerevel Therapeutics and Delix Therapeutics. NPD has served as a paid consultant for Sunovion Pharmaceuticals and is on the scientific advisory board for Sentio Solutions, Inc. and Circular Genomics, Inc. for unrelated work. KJR has performed scientific consultation for Bioxcel, Bionomics, Acer, and Jazz Pharma; serves on Scientific Advisory Boards for Sage, Boehringer Ingelheim, Senseye, and the Brain Research Foundation. He has received sponsored research support from Alto Neuroscience. None of these relationships are related to the current manuscript. The remaining authors have no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Clancy, K.J., Devignes, Q., Kumar, P. et al. Circulating PACAP levels are associated with increased amygdala-default mode network resting-state connectivity in posttraumatic stress disorder. Neuropsychopharmacol. 48, 1245–1254 (2023). https://doi.org/10.1038/s41386-023-01593-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41386-023-01593-5
- Springer Nature Switzerland AG