
Abstract
Blunted and exaggerated neuronal response to rewards are hypothesized to be core features of schizophrenia spectrum disorders (SZ) and bipolar disorder (BD), respectively. Nonetheless, direct tests of this hypothesis, in which response between SZ and BD is compared in the same study, are lacking. Here we examined the functional correlates of reward processing during the Incentivized Control Engagement Task (ICE-T) using 3T fMRI. Reward-associated activation was examined in 49 healthy controls (HCs), 52 recent-onset individuals with SZ, and 22 recent-onset individuals with Type I BD using anterior cingulate (ACC), anterior insula, and ventral striatal regions of interest. Significant group X reward condition (neutral vs. reward) interactions were observed during reward anticipation in the dorsal ACC (F(2,120) = 4.21, P = 0.017) and right insula (F(2,120) = 4.77, P = 0.010). The ACC interaction was driven by relatively higher activation in the BD group vs. HCs (P = 0.007) and vs. individuals with SZ (P = 0.010). The insula interaction was driven by reduced activation in the SZ group relative to HCs (P = 0.018) and vs. people with BD (P = 0.008). A composite of reward anticipation-associated response across all associated ROIs also differed significantly by diagnosis (F(1,120) = 5.59, P = 0.02), BD > HC > SZ. No effects of group or group X reward interactions were observed during reward feedback. These results suggest that people with SZ and BD have opposite patterns of activation associated with reward anticipation but not reward receipt. Implications of these findings in regard to Research Domain Criteria-based classification of illness and the neurobiology of reward in psychosis are discussed.
Similar content being viewed by others

Introduction
In recent years, interest has been growing in performing cross-diagnostic studies, in which a neuronal circuit associated with a key neurocognitive domain is examined across more than one psychiatric disorder. The goal of these studies is to determine which domains show deficits across multiple disorders, the pattern(s) in which these differences occur, and ultimately if shared behavioral deficits can be explained by common neuronal mechanisms that would be amendable to cross-diagnostic intervention. Previous research using this framework to evaluate individuals with bipolar disorder (BD) and schizophrenia spectrum disorders (SZ) suggest a dimensional pattern across various domains (e.g., cognitive control), with intermediate deficits in BD and more severe deficits in SZ [1,2,3].
This graded dimensional pattern of deficits, however, may not be true of all pathophysiological mechanisms. Studies examining reward responsiveness, for example, have frequently observed elevations in BD (reviewed by [4,5,6,7]) while studies in SZ (reviewed by Whitton et al. and Robinson et al. [6, 8]) suggest reductions in associated neuronal activity. Indeed, mania in BD and negative symptoms in SZ in some respects appear to be diametrically opposed clinical phenomena that have been hypothesized to be a consequence of opposite abnormalities in brain reward-associated processing [6]. Hence, manic symptoms in BD are theorized to be the consequence of a hyperactive reward system, whereas negative symptoms in SZ may be the result of a hypoactive reward system [6]. Nonetheless, to our knowledge, only one study has directly compared reward processing between BD and SZ on a functional level using fMRI [9]. In that study, Schwarz et al. found reduced ventral striatal (VS) activation during reward anticipation in both SZ and BD using the monetary incentive delay (MID) task. Reduced executive network activation during anticipation was also observed in BD in the study.
The MID task used by Schwarz et al., however, is a non-demanding task in which the same button is pressed in response to a light stimulus. Due of its low difficulty, the task may not provide a sensitive measure of psychosis-related impairments, as differences in reward-associated activation may be amplified in tasks that require more effort [10]. Indeed, previous research in individuals with BD suggests that difficult tasks are more sensitive to reward-associated differences in brain activation in BD (vs. healthy people) than easy tasks [11]. Furthermore, the previous study examined chronic individuals with BD or SZ, and consequently, it is unclear if the differences observed were the direct result of illness or a secondary consequence of chronic disease or medication. Here, we used a more engaging, demanding reward task, the Incentivized Control Engagement Task (ICE-T) [12, 13], to further examine the neuronal correlates of reward anticipation and receipt in recent (<2 years) onset BD vs. SZ. Unlike the MID, the ICE-T incorporates a variable cognitive control condition in addition to a variable reward condition, thereby requiring more effortful engagement [12]. We focused our analysis on dorsal anterior cingulate (ACC), anterior insula, VS, and ventromedial prefrontal cortex (vmPFC) regions of interest (ROIs) as they are core components of the corticostriatal reward network [8, 14, 15] and have been previously identified in an fMRI meta-analysis of reward [16]. We also examined activation during the cognitive control-associated component of the ICE-T using a dorsolateral prefrontal cortex (DLPFC) ROI. Relative to healthy controls (HCs), we hypothesized increased reward-associated activation in BD and reduced activation in SZ, consistent with previous observations [4,5,6,7,8] along with the view that BD may be distinguishable from SZ based on neuronal activation associated with reward. We also speculated these differences would be more apparent during reward anticipation in SZ based on prior research suggesting that SZ patients show normal “in the moment” processing of reward (i.e., unaltered hedonic response) while displaying blunted anticipatory processing [17]. Finally, we hypothesized that activation would be negatively associated with scores on the SANS Anhedonia and Avolition/Apathy subscales based on their transdiagnostic links to the neuronal reward system [18], and positively associated with mania symptoms as measured by the Young Mania Rating Scale (YMRS) [19].
Methods
Participants
Sixty-three individuals (48 male, 15 female) with recent-onset non-affective psychosis (including schizophrenia, schizoaffective disorder, schizophreniform disorder, and psychosis-not-otherwise-specified, comprising a “schizophrenia spectrum disorder” (“SZ”) group), 25 individuals (16 male, 9 female) with recent-onset Type I BD with psychotic features, and 51 demographically matched HCs (34 male, 17 female) were recruited from the UC Davis Early Psychosis Programs (EDAPT and SacEDAPT Clinics). Notably, Type I BD is a more severe illness than Type II, as Type I patients must have had a full-blown manic episode to meet the criteria for diagnosis, whereas Type II patients present with hypomania. All individuals were between 14 and 35 years of age. SZ and BD participants were within two years of their first psychotic episode. The University of California, Davis Institutional Review Board approved the study. Participants gave written informed consent and were paid for their participation.
Please see the Supplementary file for clinical rating information, exclusion criteria, and details on demographic and clinical group comparisons.
Task description
The ICE-T is a delayed match-to-sample task (Fig. 1) that dissociates reward motivation and top-down cognitive control [12, 13]. The task differs from the MID in that there are two cognitive control conditions (opposite vs. same) in addition to the two reward conditions (reward vs. neutral) used in the MID. Briefly, the task was composed of blocks of “same” trials requiring low cognitive control and blocks of “opposite” trials requiring high cognitive control. Participants were alerted to the type of block by the words “same” or “opposite” that appeared on the screen before each block. These blocks were further composed of “neutral” or “rewarded” trials. Individuals were alerted via a prestimulus cue if a trial was to be “neutral” or “rewarded.” Participants were given response buttons for each hand.

In “same” trials, participants were instructed to press the button in the same hand as the matching star (e.g., left hand if the matching probe was on the left side of the screen). In “opposite” trials, participants were instructed to press the button in the opposite hand as the matching star (e.g., left hand if the matching probe was on the right side of the screen). Neutral vs. rewarded trials were color-coded, with the color code (red or green) counterbalanced between individuals.
Task parameters are provided in Supplementary Table 1. Specifically, in ICE-T trials, a cue stimulus first appeared on the screen for 0.5 s. The color of the stimulus alerted the participant if the trial will be neutral or rewarded. Stimulus color mapping (i.e., if red or green corresponded to neutral or rewarded trials) and block order (same or opposite) were counterbalanced across participants. Following a 2- or 4-s interstimulus interval, two side-by-side probe stimuli were then presented for 1 s. One of the probe stimuli matched the previous stimulus and the other did not. In “same” (low cognitive control) blocks, the participant was instructed to press the button on the ipsilateral side of the matching stimulus, e.g., the left-hand button if the matching stimulus was on the left side. In “opposite” (high cognitive control) blocks, the participant was instructed to press the button on the contralateral side of the matching stimulus, e.g., the left-hand button if the matching stimulus was on the right side. Visual feedback (0.5 s duration) was then provided. Specifically, in neutral trials, “OK” was displayed if the participant answered accurately within the time limit, and “X” was displayed otherwise. In rewarded trials, “$$“ was displayed if the participant answered accurately within the time limit (earning $0.50), and “X” was displayed otherwise. Each trial was followed by a jittered intertrial interval of 4 s on average, with a minimum 2 s and a maximum 16 s. Incentive condition (neutral or rewarded) and target location (left or right) was pseudorandomized and consequently counterbalanced within blocks. Each participant was presented with six runs of 6 m 4 s each, with each run consisting of one opposite block of 20 trials and one same block of 20 trials. The task, therefore, included 60 trials of each condition (Same Neutral, Same Reward, Opposite Neutral, Opposite Reward). The total task length was 36 m 48 s.
The initial response time limit of 1 s was shortened by 10% after streaks of five correct and fast responses to rewarded trials. Conversely, two consecutive errors, late responses, or null responses in rewarded trials increased the response time limit by 10%. This adjustment was performed was to reduce changes in the reward expectation of each trial as the task went on [12, 13]. In addition, the adjustment may help minimize performance differences that might change the value of opposite vs. same trials independent of the reward status of the trial, because trials more likely to be answered correctly may induce more rewards for answering correctly [12, 13].
Accuracy scores were calculated as the mean percent correct in response to the probe over all blocks of trials for each condition (Same Neutral, Same Reward, Opposite Neutral, Opposite Reward). Reaction time was calculated as the mean reaction time in response to the probe over all blocks of trials for each condition.
fMRI image acquisition and preprocessing
Images were acquired on a Siemens TimTrio 3T scanner with an eight-channel head coil using gradient T2*-weighted echo-planar imaging (EPI) sequence (32 interleaved axial-oblique slices; 3.8 × 3.8 × 3.5 mm voxels; 75° flip angle; 2000 ms TR; 29 ms TE; 240 × 240 mm field of view). BOLD images were aligned to the anterior commissure–posterior commissure + 10°. These scanning parameters (including alignment angle) were chosen based on recommendations from MR physicist collaborators at the UC Davis Imaging Research Center in order to provide optimal cerebral coverage while limiting the number of slices that include air-tissue interfaces that lead to susceptibility-related signal loss. The alignment angle results in scans aligned at an angle of approximately 10° to the tangential intercommissural reference line [20, 21]. High-resolution anatomical images were also acquired for each participant using a three-dimensional T1-weighted magnetization-prepared rapid acquisition of gradient-echo (MPRAGE) sequence (176 contiguous anterior commissure–posterior commissure slices; acceleration factor of 2; 1 × 1 × 1 mm voxels; 7° flip angle; 2530 ms TR; 3.5 ms TE; 256 × 256 mm field of view). Head movement was minimized using foam padding and participants wore earplugs to muffle scanner noise.
Images were preprocessed with Statistical Parametric Mapping-8 (SPM8) software (http://www.fil.ion.ucl.ac.uk/SPM8). Functional data were reoriented, slice-time corrected, and realigned. Structural images were brain-extracted using FSL’s BET toolbox [22] and then segmented and co-registered to the mean functional image. Images were spatially normalized to the Montreal Neurological Institute (MNI) template using a nonlinear 12-parameter affine transformation and then smoothed with an 8-mm kernel. Data were screened for image artifacts, structural abnormalities, and normalization errors to ensure data quality. Individual participant’s data were excluded if >0.45 mm frame-wise displacement was observed on four or more task blocks.
First-level analysis
First-level blood oxygen level-dependent (BOLD) effects were modeled using a double-gamma function without temporal derivatives in a mixed event-related design using the general linear model function in SPM8. A 75 s high-pass filter was employed. Images were motion-corrected using rigid-body motion parameters as single-subject regressors. All trial types were modeled (Same Neutral, Same Reward, Opposite Neutral, Opposite Reward) and only correct responses were used to create first-level images of cue and feedback-associated BOLD response. Contrasts of interest were Reward > Neutral (corresponding to reward-associated BOLD activation) and Opposite > Same (corresponding to cognitive control-associated BOLD activation).
Regions of interest (ROIs)
Reward anticipation (cue)-associated activation was extracted from 4-mm radius spherical ROIs from a 2012 meta-analysis of high reward >no reward anticipation fMRI contrasts [16] using the Marsbar toolbox [23]. Of the ROIs in this meta-analysis, we focused on the ACC, insula, and ventral striatum as these regions are frequently associated with reward processing [14, 15]. Montreal Neurological Institute (MNI) ROI coordinates were centered at x = 2, y = 30, z = 32 for dorsal ACC, x = 38, y = 20, z = −8 for the right anterior rostral insula, x = −10, y = 10, z = −2 for left VS, and x = 12, y = 12, z = −4 for the right VS.
Reward receipt (feedback)-associated activation was similarly extracted from 4 mm radius spherical ROIs taken from a meta-analysis of high reward > no reward fMRI contrasts during reward receipt [16]. ROI coordinates were centered at x = 0, y = 38, z = 8 for the ventromedial prefrontal cortex (vmPFC) and x = 14, y = 12, z = −12 for the right VS. Although the 2012 meta-analysis also found clusters in the medial orbitofrontal lobe, we did not analyze data from this region due to the high probability of 3T signal loss [24].
As the ICE-T was also designed to examine cognitive control, it incorporates a low control condition and high control condition. To examine this component of the task, we used dorsolateral prefrontal cortex (DLPFC) ROIs. The DLPFC was chosen for analysis because it is the primary brain region associated with cognitive control and context-appropriate responding [25]. These ROIs were centered on coordinates x = −42, y = 26, z = 37 (left) and x = 42, y = 26, z = 37 (right) based on a previous cognitive control study in an independent dataset [26].
Group analysis
Following single-subject BOLD signal extraction from contrasts of interest within the ROIs, group analysis was performed by factorial ANOVA (SPSS26, IBM) with reward (neutral vs. rewarded) as a within-subjects factor, level of cognitive control (same vs. opposite) as a within-subjects factor, and group diagnosis (HC vs. SZ. vs. BD) as a between-subjects factor. Accuracy and reaction time were analyzed by ANOVA in the same manner. Reward-associated activations within the reward > neutral contrast-generated, “reward network” ROIs for cue and feedback (see “Regions of interest“) were each analyzed by one-way ANOVA with the group as a between-subjects factor. The hypothesis that SZ and BD would show opposite patterns of reward-associated activation also was tested by extracting the first principal component of reward-associated BOLD response across all ROIs (as performed in [27]), using the resulting factor scores as dependent variables in an ANOVA, and testing the linear contrast BD > HC > SZ. This process was performed separately for reward anticipation and receipt. Only individuals who showed at least 60% accuracy during all four task conditions were included in analyses. Significant (P < 0.05) group effects were followed-up by post hoc tests to describe which group comparisons were responsible for driving the effects. Exploratory whole-brain analyses were also conducted in SPM8 with a threshold of voxelwise P < 0.001, k > 20 voxels.
Correlations between clinical and experimental variables
Please refer to the Supplementary file for methodological details on clinical correlations.
Results
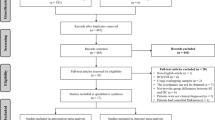
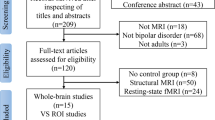
Excluded data
Please refer to the Supplementary file for counts of excluded individuals and reasons for exclusion. 49 HCs, 52 individuals with SZ, and 22 participants with BD were included in the final sample.
Demographics
Demographic and clinical information for participants in the final sample is shown in Table 1. Groups differed significantly on education and WASI scores, but not on age, biological sex, or handedness. BD individuals had significantly lower SANS and SAPS total scores than those with SZ, driven by lower Affective Flattening score on the SANS and lower Hallucinations and Delusions scores on the SAPS. Results from other demographic and clinical between-group comparisons are provided in Table 1.
Behavioral results
Performance metrics for the ICE-T for each group are presented in Fig. 2 and Supplementary Tables 2a and 2b. For accuracy, significant main effects of reward (F(1,120) = 26.88, P < 0.001), level of cognitive control (F(1,120) = 169.81, P < 0.001), and group (F(2,120) = 4.99, P < 0.001) were observed, but no significant interactions. Group effects were driven by significantly lower accuracy across conditions in the SZ group vs. HC (P = 0.003). The between-group difference in mean accuracy between the BD and HC groups trended toward significance (P = 0.064).

Thick black lines represent group means.
For reaction time, significant main effects of reward (F(1,120) = 25.63, P < 0.001) and level of cognitive control (F(1,120) = 498.29, P < 0.001) were observed, driven by higher reaction times during neutral trials and high control trials, respectively.
fMRI results: reward anticipation
No significant group differences were observed in any of the six rigid-body motion parameters in the final sample (Supplementary Table 3).
Across the whole brain, the contrast reward cues > neutral cues activated a broad network of regions, including the dorsal ACC, insula, VS, precuneus, and visual cortex across all participants (Supplementary Table 4 and Supplementary Fig. 1).
Group mean + /− SD reward anticipation-associated ROI BOLD response, effect sizes (Cohen’s d), and statistical parametric maps for the reward × group interaction are provided in Table 2 and/or Fig. 3. Significant main effects of reward anticipation were observed in the dorsal ACC ROI (F(1,120) = 41.90, P < 0.001), right insula ROI (F(1,120) = 45.10, P < 0.001), left VS ROI (F(1,120) = 41.68, P < 0.001), and right VS ROI (F(1,120) = 61.13, P < 0.001) due to increased activity during reward cues vs. non-reward cues (P < 0.001 for all ROIs). Group × reward interactions were also observed in the dorsal ACC (F(2,120) = 4.21, P = 0.017) and right insula (F(2,120) = 4.77, P = 0.010) but not left VS (F(2,120) = 1.73, P = 0.183) or right VS (F(2,120) = 1.23, P = 0.297). The dorsal ACC interaction effect was driven by increased reward-associated activation in the BD group vs. HCs (P = 0.007) and vs. individuals with SZ (P = 0.010). The right insula interaction effect was driven by decreased reward-associated activation in the SZ group vs. HCs (P = 0.018) and vs. people with BD (P = 0.008). Examining the entire reward network by extracting the first principal component of BOLD response across all four ROIs, the a priori contrast BD > HC > SZ was also significant (F(1,120) = 5.59, P = 0.02) (Fig. 4).

Image thresholded at P < 0.001, k > 20 voxels for visualization. Coronal section displayed in the neurologic convention (right on right). Bottom: Individual reward anticipation-associated activations for the dorsal ACC and right anterior insula ROIs sorted by group. *P < 0.05 vs. healthy controls (HC) and individuals with schizophrenia spectrum disorders (SZ). **P < 0.05 vs. HC and individuals with bipolar disorder (BD). Thick black lines represent group means.

The a priori linear contrast BD > HC > SZ was significant (F(1,120) = 5.59, P = 0.02). Factor scores represent the first principle component of BOLD response across all reward anticipation ROIs (dorsal ACC, right anterior insula, left ventral striatum, right ventral striatum). Thick black lines represent group means.
fMRI results: reward receipt
Across the whole brain, the contrast reward cues > neutral activated a network of regions including the vmPFC/subgenual ACC, superior parietal cortex, insula, and posterior cingulate cues across all participants (Supplementary Table 5 and Supplementary Fig. 2).
Group mean + /− SD reward receipt-associated ROI BOLD response and effect sizes (Cohen’s d) are provided in Table 2. A significant main effect of reward receipt was observed in the vmPFC ROI (F(1,120) = 11.72, P = 0.001) due to increased activity during reward feedback vs. neutral feedback (P = 0.001). The main effect of reward in the right VS ROI was not significant (F(1,120) = 1.87, P = 0.17). No significant group × reward interactions or main effects of the group were observed. Examining the first principal component of BOLD response across both ROIs, the a priori contrast BD > HC > SZ was also nonsignificant (F(1,120) = 0.27, P = 0.60).
fMRI results: ROI analysis of cognitive control-associated effects
Cognitive control-associated effects were examined using the opposite (high control) > same (low control) contrast. No main effects of level of cognitive control were observed in either the left DLPFC ROI (F(1,120) = 0.61, P = 0.438) or right DLPFC ROI (F(1,120) = 1.13, P = 0.290). Furthermore, consistent with the lack of behavioral effects, no significant voxels in any prefrontal area were observed using the contrast opposite > same. Significant interactions with the group were also not observed.
Medication effects
After excluding unmedicated participants (four with BD, five with SZ), reward X group interaction effects in both ROIs remained significant for reward anticipation (dorsal ACC: F(2,111) = 4.05, P = 0.020; right insula: F(2,111) = 3.83, P = 0.025). No difference in magnitude of the reward anticipation-associated principle component was observed between BD individuals taking mood stabilizers and not taking stabilizers (t = 0.34, P = 0.74). The antipsychotic dose was not associated with reward anticipation-associated component magnitude in either the SZ (r = −0.12, P = 0.43) or BD (r = 0.07, P = 0.77) groups.
Correlations between clinical and experimental variables
A negative correlation was observed between SANS Avolition/Apathy score and reward-associated activation in the dorsal ACC ROI among people with BD (ρ = −0.51, P = 0.017) (Supplementary Fig. 3). Correlations with YMRS score were nonsignificant.
Discussion
In agreement with our hypothesis, individuals with BD and SZ showed opposite patterns of activation during reward anticipation during the performance of the ICE-T. Specifically, during reward anticipation, significant hyperactivation was observed in people with BD relative to HC and SZ in the dorsal ACC, and significant hypoactivation was observed in people with SZ relative to BD and HC in the anterior insula. No group differences, however, were observed in reward receipt, suggesting that this aspect of reward processing is not significantly altered in these illnesses and consistent with previous findings that have examined this distinction in psychosis [17]. As hypothesized, a negative association was also observed between SANS Avolition/Apathy score and reward anticipation-associated BOLD response in the dorsal ACC in participants with BD. These results suggest that BD and SZ may be distinguishable based on their patterns of brain activity specifically during reward anticipation. Indeed, the differential brain response observed in this study between BD and SZ is in stark contrast to previous findings of a graded pattern in other neurocognitive domains (e.g., cognitive control [2]), where levels of activation in BD are lower than in HC but higher than in SZ. Our observation that this pattern occurs in recent-onset individuals further suggests that differences in reward response are not a secondary consequence of chronic disease or long-term treatment with antipsychotic medications.
The neurotransmitter system most commonly implicated in reward processing is dopamine. In a well-established model of reinforcement learning, the brain uses fast, phasic modulation of dopamine signaling to compute the difference between expected and actual reward [28]. Based on the magnitude of this dopamine-coded “prediction error,” the brain is able to dynamically learn associations between stimuli and outcomes in order to maximize the utility of its actions. Elevated reward-associated signaling in BD and blunted signaling in SZ may thus be the result of opposing forms of disruption in the magnitude, timing, or duration of this dopaminergic-based signal [29]. Indeed, some studies suggest reduced mesocortical (as opposed to the well-documented increased nigrostriatal [30]) dopamine release capacity in SZ [31] and increased D2/D3 receptor availability in BD [29], although the nature of dopamine signaling in the cortex remains poorly understood (particularly in BD). Thus, if dopamine is a common pharmacologic mechanism linking atypical reward processing in these disorders, it suggests that normalization would require distinct regionally and temporally targeted reduction and enhancement of dopaminergic signaling in BD and SZ, respectively. Indeed, hyperdopaminergia is hypothesized to contribute to symptoms of BD [32] and frontal hypodopaminergia is thought to contribute to negative and cognitive symptoms of SZ [31, 33]. Furthermore, the mood stabilizer lithium reverses dopamine-dependent hyperactivity in dopamine transporter knockout mice [34], illustrating a potential monoaminergic mechanism by which lithium can downregulate mania. Clozapine, on the other hand, may increase mesocortical dopamine release via serotonin receptor blockade [33, 35] and is currently the most efficacious antipsychotic for ameliorating negative symptoms in SZ [36]. As a large majority of patients in the present study were taking antipsychotic medications, our study was not designed to compare unmedicated vs. medicated individuals. The effects of dopaminergic drugs on activation during this task is consequently an important area for future investigation.
As opposed to a primary effect of dopamine, an alternative interpretation of these results is that they may reflect functional differences in ACC and insula function in BD and SZ [37,38,39,40], which in turn drive dopaminergic changes (e.g., hyperdopaminergia in SZ) as an adaptive response to not receiving high-quality estimates of future reward and cost-related outcomes. Indeed, the ACC and insula are also part of interconnected dopaminergic midbrain–striatal–cortical feedback loops [14], making these regions functionally sensitive to dopaminergic tone and enabling them to potentially compute action value to support motivated behavior. Furthermore, the ACC and insula are widely regarded as important for integrating reward and effort/cost signals to guide behavior in a goal-directed manner [41,42,43,44]. Deficits in the online subjective value estimation process have also been identified in SZ [45, 46]. Finally, although our study focused on reward processing, it is important to acknowledge that the ACC and insula are involved in other functions, including pain [47] and sensory processing [48]. The ACC and insula are also hubs of the salience network, an intrinsic network [49]. Future studies in our clinic may determine the extent to which the observed reward anticipation-associated differences in ACC/insula function in recent-onset BD vs. SZ extend to other tasks that involve these regions.
Interestingly, group differences in reward processing during this task occurred during the anticipation phase but not the feedback phase. This pattern of normal “in the moment” processing of rewarding stimuli but the abnormal perception of future or past reward is consistent with clinical findings in SZ, in which individuals display typical experiences of positive emotion when presented with evocative stimuli [17]. In addition, people with SZ report positive emotion at HC levels with assessing current feelings, but lower than HCs when assessing past or future feelings [50, 51].
It is notable that three previous studies using the MID have observed hypoactivation in BD relative to HCs [9, 52, 53]. Although the reasons for this discrepancy are unclear, one possibility is the relative lack of effort engaged by the MID relative to the ICE-T, making action value computation less relevant for a trial-to-trial performance on this task. In the MID, after participants are cued as to whether a trial will be rewarded, they are asked to press a button as soon as possible after a stimulus appears. Only one button is used, and the stimulus target is typically the same (e.g., a light flash). In contrast, the ICE-T requires pressing buttons on opposite hands depending on the location of the target. The ICE-T is therefore a more engaging, demanding task that may be more sensitive to eliciting group differences in action valuation. A second possibility is that these previous studies recruited individuals with chronic illness who were likely taking medications for several years and accumulating a range of comorbidities, pharmacological treatments, and other consequences of chronicity, whereas our study examined people with a recent-onset illness. Related to this point, the long-term effects of treatments such as mood stabilizers on brain function are poorly understood, although a 2019 study found normalization of intrinsic network architecture associated with mania after 8 weeks of lithium treatment [54].
Examining clinical correlations in an exploratory fashion, we found a negative association between reward anticipation-associated hyperactivation in the dorsal ACC and SANS Avolition/Apathy score in BD, potentially linking a functional neuronal signature with a symptomatic presentation in the illness. The observed inverse correlation with SANS Avolition/Apathy is consistent with the view that activation of the ACC is a measure of the ability to select and maintain goal-directedness [55]. Loss of activation may thus be reflected in high SANS Avolition scores, which measure grooming/hygiene, persistence at work/school and/or ability to stay employed, and physical anergia. Depressive symptoms may also blunt neuronal activation during reward anticipation in BD [56,57,58]. As we used an uncorrected statistical threshold for detecting significant clinical correlations and our BD sample was small; however, this finding requires replication in a larger sample before strong conclusions can be drawn. It was also somewhat surprising that we did not observe a significant correlation with mania as scored by the YMRS. This lack of an observed relationship may have been due to the fact that BD participants in our sample had relatively mild mania symptoms, resulting in a limited dynamic range with which to observe associations.
In contrast to our fMRI results, in the behavioral data, we found generalized deficits in accuracy and increases in reaction time across conditions in both SZ and BD (Fig. 1). One possible explanation for the discrepancy between behavioral and fMRI results was the nature of the task. Specifically, the high control condition might not have been sufficiently challenging relative to the low control condition, making the task insensitive to detect behavioral differences in cognitive control. Supporting this view, the frontoparietal cortex was not recruited under the high control condition, and individuals also performed the task well across all conditions. The SZ and BD groups also had relatively high WASI scores (BD mean = 105.1, SZ mean = 103.8), potentially limiting the sensitivity of the cognitive control-dependent aspect of the task. The low cash reward ($0.50) per correct trial may also not have been high enough to substantially alter behavior. Interestingly, however, the observed ACC hyperactivation in BD during reward trials was not associated with improved performance during these trials, suggesting an inefficient mechanism by which individuals with BD may require higher than normal levels of ACC activation to maintain close to normal performance [59]. Given the psychometric limitations of the task, additional manipulations to increase the differences in cognitive control demands between conditions should be considered in future studies.
Our study had additional limitations. The sample size was smaller in the BD than in the other two groups. This reflects the lower percentage of BD patients with psychotic features presenting to our Early Psychosis Coordinated Specialty Care Clinic compared to those with SZ. It was also surprising that, contrary to our hypothesis, no group effects were observed in the VS, despite the main effect of reward being observed in the region. Previous findings using reward tasks, however, have not yielded consistent patterns of activation of the striatum during reward anticipation in BD, with some studies showing increased activation (e.g., [60, 61]) and others decreased activation (e.g., [9, 62, 63]) (reviewed by Johnson et al. [53]). We must also acknowledge that although ROIs were selected a priori from a meta-analysis based on their previous activations in fMRI contrasts designed to measure reward anticipation and receipt, that does not necessarily imply that activation in these regions is entirely specific to these processes (for example, activation during reward anticipation may also represent heightened attention or arousal). A further limitation was that our vmPFC analysis may have been influenced by magnetic susceptibility artifacts that occur due to the region being near the orbital sinus. This possibility may be mitigated in future studies using EPI sequences optimized to reduce artifacts near this region (e.g., [64, 65]). Finally, our study only examined individuals with Type I BD, and it is unclear if our results would generalize to Type II.
In conclusion, our study suggests that BD and SZ are associated with dissociable functional patterns in reward processing and that these differences are specific to reward anticipation as opposed to reward receipt. Indeed, these results suggest that some biological aspects of these disorders may translate in concordance with clinical diagnoses, providing support for categorical diagnostic distinction for some dimensions of psychopathology and in contrast to “DSM diagnosis-independent” conceptualizations (such as the Research Domain Criteria (RDoC) [66]). As our study is the first to directly compare the functional correlates of reward anticipation in BD vs. SZ, our results require replication in larger sample size and with additional behavioral measures of reward processing in order to enable direct tests of the RDoC hypothesis as it relates to reward. As diagnosis-related differences in regional dopaminergic tone may underlie the opposite pattern in the two illnesses, future imaging studies may seek to examine this relationship using dopamine-targeting drugs and/or dopaminergic radioligands.
Funding and disclosure
This study was supported by NIH grants MH059883 (Dr. Carter), MH114325 (Dr. Smucny) and HD051958 (Dr. Tully). TAN and LMT are cofounders and shareholders in Safari Health, Inc. The remaining authors have nothing to disclose.
References
Smucny J, Iosif AM, Eaton NR, Lesh TA, Ragland JD, Barch DM, et al. Latent profiles of cognitive control, episodic memory, and visual perception across psychiatric disorders reveal a dimensional structure. Schizophr Bull. 2020;46:154–62.
Smucny J, Lesh TA, Newton K, Niendam TA, Ragland JD, Carter CS. Levels of cognitive control: a functional magnetic resonance imaging-based test of an RDoC domain across bipolar disorder and schizophrenia. Neuropsychopharmacology. 2018;43:598–606.
Hill SK, Reilly JL, Keefe RS, Gold JM, Bishop JR, Gershon ES, et al. Neuropsychological impairments in schizophrenia and psychotic bipolar disorder: findings from the Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP) study. Am J Psychiatry. 2013;170:1275–84.
Nusslock R, Young CB, Damme KS. Elevated reward-related neural activation as a unique biological marker of bipolar disorder: assessment and treatment implications. Behav Res Ther. 2014;62:74–87.
Nusslock R, Alloy LB. Reward processing and mood-related symptoms: an RDoC and translational neuroscience perspective. J Affect Disord. 2017;216:3–16.
Whitton AE, Treadway MT, Pizzagalli DA. Reward processing dysfunction in major depression, bipolar disorder and schizophrenia. Curr Opin Psychiatry. 2015;28:7–12.
Johnson SL, Edge MD, Holmes MK, Carver CS. The behavioral activation system and mania. Annu Rev Clin Psychol. 2012;8:243–67.
Robison AJ, Thakkar KN, Diwadkar VA. Cognition and reward circuits in schizophrenia: synergistic, not separate. Biol Psychiatry. 2020;87:204–14.
Schwarz K, Moessnang C, Schweiger JI, Baumeister S, Plichta MM, Brandeis D, et al. Transdiagnostic prediction of affective, cognitive, and social function through brain reward anticipation in schizophrenia, bipolar disorder, major depression, and autism spectrum diagnoses. Schizophr Bull. 2020;46:592–602.
Gold JM, Strauss GP, Waltz JA, Robinson BM, Brown JK, Frank MJ. Negative symptoms of schizophrenia are associated with abnormal effort-cost computations. Biol Psychiatry. 2013;74:130–6.
Harmon-Jones E, Abramson LY, Nusslock R, Sigelman JD, Urosevic S, Turonie LD, et al. Effect of bipolar disorder on left frontal cortical responses to goals differing in valence and task difficulty. Biol Psychiatry. 2008;63:693–8.
Ursu S, Clark KA, Stenger VA, Carter CS. Distinguishing expected negative outcomes from preparatory control in the human orbitofrontal cortex. Brain Res. 2008;1227:110–9.
Ursu S, Carter CS. Outcome representations, counterfactual comparisons and the human orbitofrontal cortex: implications for neuroimaging studies of decision-making. Brain Res Cogn Brain Res. 2005;23:51–60.
Haber SN. Corticostriatal circuitry. Dialogues Clin Neurosci. 2016;18:7–21.
Haber SN. Neuroanatomy of reward: a view from the ventral striatum. In: Gottfried JA, editor. Neurobiology of sensation and reward. Boca Raton, FL: CRC Press/Taylor and Francis; 2011.
Diekhof EK, Kaps L, Falkai P, Gruber O. The role of the human ventral striatum and the medial orbitofrontal cortex in the representation of reward magnitude—an activation likelihood estimation meta-analysis of neuroimaging studies of passive reward expectancy and outcome processing. Neuropsychologia. 2012;50:1252–66.
Gold JM, Waltz JA, Prentice KJ, Morris SE, Heerey EA. Reward processing in schizophrenia: a deficit in the representation of value. Schizophr Bull. 2008;34:835–47.
Strauss GP, Cohen AS. A transdiagnostic review of negative symptom phenomenology and etiology. Schizophr Bull. 2017;43:712–9.
Young RC, Biggs JT, Ziegler VE, Meyer DA. Young mania rating scale. Handbook of psychiatric measures. Washington, D.C.: American Psychiatric Association; 2000. p. 540–42.
Choi SH, Chi JG, Kim YB, Cho ZH. Anterior commissure–posterior commissure revisited. Korean J Radiol. 2013;14:653–61.
Otake S, Taoka T, Maeda M, Yuh WT. A guide to identification and selection of axial planes in magnetic resonance imaging of the brain. Neuroradiol J. 2018;31:336–44.
Smith SM. Fast robust automated brain extraction. Hum Brain Mapp. 2002;17:143–55.
Andreasen NC. Scale for the assessment of negative symptoms (SANS). Iowa City, IA: Department of Psychiatry, College of Medicine, The University of Iowa; 1984.
Domsch S, Linke J, Heiler PM, Kroll A, Flor H, Wessa M, et al. Increased BOLD sensitivity in the orbitofrontal cortex using slice-dependent echo times at 3 T. Magn Reson Imaging. 2013;31:201–11.
Lesh TA, Niendam TA, Minzenberg MJ, Carter CS. Cognitive control deficits in schizophrenia: mechanisms and meaning. Neuropsychopharmacology. 2011;36:316–38.
MacDonald AW III, Cohen JD, Stenger VA, Carter CS. Dissociating the role of the dorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science. 2000;288:1835–8.
Smucny J, Lesh TA, Carter CS. Baseline frontoparietal task-related BOLD activity as a predictor of improvement in clinical symptoms at 1-year follow-up in recent-onset psychosis. Am J Psychiatry. 2019;176:839–45.
Schultz W. Dopamine reward prediction-error signalling: a two-component response. Nat Rev Neurosci. 2016;17:183–95.
Ashok AH, Marques TR, Jauhar S, Nour MM, Goodwin GM, Young AH, et al. The dopamine hypothesis of bipolar affective disorder: the state of the art and implications for treatment. Mol Psychiatry. 2017;22:666–79.
McCutcheon RA, Abi-Dargham A, Howes OD. Schizophrenia, dopamine and the striatum: from biology to symptoms. Trends Neurosci. 2019;42:205–20.
Weinstein JJ, Chohan MO, Slifstein M, Kegeles LS, Moore H, Abi-Dargham A. Pathway-specific dopamine abnormalities in schizophrenia. Biol Psychiatry. 2017;81:31–42.
Berk M, Dodd S, Kauer-Sant’anna M, Malhi GS, Bourin M, Kapczinski F, et al. Dopamine dysregulation syndrome: implications for a dopamine hypothesis of bipolar disorder. Acta Psychiatr Scand Suppl. 2007;116:41–9.
Brisch R, Saniotis A, Wolf R, Bielau H, Bernstein HG, Steiner J, et al. The role of dopamine in schizophrenia from a neurobiological and evolutionary perspective: old fashioned, but still in vogue. Front Psychiatry. 2014;5:47.
Beaulieu JM, Sotnikova TD, Yao WD, Kockeritz L, Woodgett JR, Gainetdinov RR, et al. Lithium antagonizes dopamine-dependent behaviors mediated by an AKT/glycogen synthase kinase 3 signaling cascade. Proc Natl Acad Sci USA. 2004;101:5099–104.
Ichikawa J, Ishii H, Bonaccorso S, Fowler WL, O’Laughlin IA, Meltzer HY. 5-HT(2 A) and D(2) receptor blockade increases cortical DA release via 5-HT(1 A) receptor activation: a possible mechanism of atypical antipsychotic-induced cortical dopamine release. J Neurochem. 2001;76:1521–31.
Huhn M, Nikolakopoulou A, Schneider-Thoma J, Krause M, Samara M, Peter N, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394:939–51.
Carter CS, Mintun M, Nichols T, Cohen JD. Anterior cingulate gyrus dysfunction and selective attention deficits in schizophrenia: [15 O]H2O PET study during single-trial Stroop task performance. Am J Psychiatry. 1997;154:1670–5.
Fassbender C, Scangos K, Lesh TA, Carter CS. RT distributional analysis of cognitive-control-related brain activity in first-episode schizophrenia. Cogn Affect Behav Neurosci. 2014;14:175–88.
Kerns JG, Cohen JD, MacDonald AW III, Johnson MK, Stenger VA, Aizenstein H, et al. Decreased conflict- and error-related activity in the anterior cingulate cortex in subjects with schizophrenia. Am J Psychiatry. 2005;162:1833–9.
Snitz BE, MacDonald A III, Cohen JD, Cho RY, Becker T, Carter CS. Lateral and medial hypofrontality in first-episode schizophrenia: functional activity in a medication-naive state and effects of short-term atypical antipsychotic treatment. Am J Psychiatry. 2005;162:2322–9.
Alexander WH, Brown JW. Medial prefrontal cortex as an action-outcome predictor. Nat Neurosci. 2011;14:1338–44.
Shenhav A, Botvinick MM, Cohen JD. The expected value of control: an integrative theory of anterior cingulate cortex function. Neuron. 2013;79:217–40.
Hunt LT, Hayden BY. A distributed, hierarchical and recurrent framework for reward-based choice. Nat Rev Neurosci. 2017;18:172–82.
Rushworth MF, Behrens TE, Rudebeck PH, Walton ME. Contrasting roles for cingulate and orbitofrontal cortex in decisions and social behaviour. Trends Cogn Sci. 2007;11:168–76.
Cooper JA, Barch DM, Reddy LF, Horan WP, Green MF, Treadway MT. Effortful goal-directed behavior in schizophrenia: Computational subtypes and associations with cognition. J Abnorm Psychol. 2019;128:710–22.
Gold JM, Waltz JA, Frank MJ. Effort cost computation in schizophrenia: a commentary on the recent literature. Biol Psychiatry. 2015;78:747–53.
Fuchs PN, Peng YB, Boyette-Davis JA, Uhelski ML. The anterior cingulate cortex and pain processing. Front Integr Neurosci. 2014;8:35.
Uddin LQ, Nomi JS, Hebert-Seropian B, Ghaziri J, Boucher O. Structure and function of the human insula. J Clin Neurophysiol. 2017;34:300–06.
Menon V, Uddin LQ. Saliency, switching, attention and control: a network model of insula function. Brain Struct Funct. 2010;214:655–67.
Strauss GP, Gold JM. A new perspective on anhedonia in schizophrenia. Am J Psychiatry. 2012;169:364–73.
Barch DM, Pagliaccio D, Luking K. Mechanisms underlying motivational deficits in psychopathology: similarities and differences in depression and schizophrenia. Curr Top Behav Neurosci. 2016;27:411–49.
Schreiter S, Spengler S, Willert A, Mohnke S, Herold D, Erk S, et al. Neural alterations of fronto-striatal circuitry during reward anticipation in euthymic bipolar disorder. Psychol Med. 2016;46:3187–98.
Johnson SL, Mehta H, Ketter TA, Gotlib IH, Knutson B. Neural responses to monetary incentives in bipolar disorder. Neuroimage Clin. 2019;24:102018.
Spielberg JM, Matyi MA, Karne H, Anand A. Lithium monotherapy associated longitudinal effects on resting state brain networks in clinical treatment of bipolar disorder. Bipolar Disord. 2019;21:361–71.
Holroyd CB, Yeung N. Motivation of extended behaviors by anterior cingulate cortex. Trends Cogn Sci. 2012;16:122–8.
Urosevic S, Luciana M, Jensen JB, Youngstrom EA, Thomas KM. Age associations with neural processing of reward anticipation in adolescents with bipolar disorders. Neuroimage Clin. 2016;11:476–85.
Satterthwaite TD, Kable JW, Vandekar L, Katchmar N, Bassett DS, Baldassano CF, et al. Common and dissociable dysfunction of the reward system in bipolar and unipolar depression. Neuropsychopharmacology. 2015;40:2258–68.
Sharma A, Wolf DH, Ciric R, Kable JW, Moore TM, Vandekar SN, et al. Common dimensional reward deficits across mood and psychotic disorders: a connectome-wide association study. Am J Psychiatry. 2017;174:657–66.
Green MF, Horan WP, Sugar CA. Has the generalized deficit become the generalized criticism? Schizophr Bull. 2013;39:257–62.
Nusslock R, Almeida JR, Forbes EE, Versace A, Frank E, Labarbara EJ, et al. Waiting to win: elevated striatal and orbitofrontal cortical activity during reward anticipation in euthymic bipolar disorder adults. Bipolar Disord. 2012;14:249–60.
Dutra SJ, Cunningham WA, Kober H, Gruber J. Elevated striatal reactivity across monetary and social rewards in bipolar I disorder. J Abnorm Psychol. 2015;124:890–904.
Caseras X, Lawrence NS, Murphy K, Wise RG, Phillips ML. Ventral striatum activity in response to reward: differences between bipolar I and II disorders. Am J Psychiatry. 2013;170:533–41.
Yip SW, Worhunsky PD, Rogers RD, Goodwin GM. Hypoactivation of the ventral and dorsal striatum during reward and loss anticipation in antipsychotic and mood stabilizer-naive bipolar disorder. Neuropsychopharmacology. 2015;40:658–66.
Deichmann R, Gottfried JA, Hutton C, Turner R. Optimized EPI for fMRI studies of the orbitofrontal cortex. Neuroimage. 2003;19(2 Pt 1):430–41.
Weiskopf N, Hutton C, Josephs O, Deichmann R. Optimal EPI parameters for reduction of susceptibility-induced BOLD sensitivity losses: a whole-brain analysis at 3 T and 1.5 T. Neuroimage. 2006;33:493–504.
Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry. 2010;167:748–51.
Acknowledgements
We thank Benjamin Geib, Madison Titone, Taylor Salo, Estera (Neli) Mihov, Erika Steinbauer, Markie Benavidez, and Huan Wang for their assistance with data collection and processing. We also thank the study participants and their families.
Author information
Authors and Affiliations
Contributions
Conceived and designed the analysis: JS and LT. Collected the data: AH. Performed the analysis: JS. Designed the task: SU. Funded the study: CC. Drafted the paper: JS. Reviewed the paper, gave conceptual advice, and provided suggested revisions: JS, LT, AH, TL, SJ, RO, MM, SU, JY, TN, JDR, and CC.
Corresponding author
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Smucny, J., Tully, L.M., Howell, A.M. et al. Schizophrenia and bipolar disorder are associated with opposite brain reward anticipation-associated response. Neuropsychopharmacol. 46, 1152–1160 (2021). https://doi.org/10.1038/s41386-020-00940-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41386-020-00940-0
- Springer Nature Switzerland AG