
Abstract
Objective
To quantify initial tidal volume (VT) during neonatal volume-targeted ventilation (VTV) and to characterize the agreement of initial VT with the limited-evidence available.
Study design
We performed a multi-center retrospective observational cohort study in two Neonatal Intensive Care Units evaluating 313 infants who received VTV as the initial ventilation modality prior to postnatal day 14. We generated descriptive statistics and performed multivariable logistic regression analysis to determine factors associated with initial VT use that agreed with available literature.
Results
154 (49%) infants received an initial VT of 5.0 mL/kg (median 5.0 mL/kg, IQR 5.0–5.1). 45 (14%) infants received an initial VT that was congruent with available literature. A birth weight of 700 –<1250 g was significantly associated with an initial VT in agreement with VT literature (aOR 9.4, 95% CI 1.7–50.4).
Conclusions
Most infants receive an initial VT of 5.0 mL/kg.
Similar content being viewed by others

Introduction
Mechanical ventilation (MV) in the Neonatal Intensive Care Unit (NICU) is a life-saving therapy. However, MV in preterm infants is associated with increased mortality [1], neurodevelopmental impairment [2], structural changes in the central nervous system [3], and bronchopulmonary dysplasia (BPD) [4]. Despite improvements in neonatal care, BPD occurs in 40% of very low birth weight infants in the United States (US) [5].
In neonates receiving MV, volume-targeted ventilation (VTV) [6] results in improved clinical outcomes compared to pressure-limited ventilation (PLV). Compared to PLV modes, VTV is associated with lower rates of death or BPD, pneumothorax, intraventricular hemorrhage, and fewer days of MV [6]. However, only 42% of NICUs in the US and Canada report VTV as their primary ventilation modality [7].
One of the most important decisions neonatal clinicians must make when using VTV is to choose an initial tidal volume (VT) that is appropriate for each infant’s respiratory pathology and size. Several small studies have evaluated short-term physiologic outcomes with different tidal volumes [8,9,10,11,12]. Based on the results of those studies, one manuscript provided recommendations for initial VT based on weight and respiratory physiology [13]. A previous survey showed that the initially chosen VT often does not agree with these recommendations [7]. However, no studies have described initial VTs in clinical practice. The objectives of our study were to quantify initial VT used during neonatal VTV and to characterize the frequency with which initial VT agreed with the limited-evidence available [8, 9, 13, 14] for neonatal VTV use.
Materials/Subjects And Methods
Study design, setting, and population
We performed a retrospective observational cohort study using prospectively collected data in the 98-bed, level IV Vanderbilt University Medical Center (VUMC) NICU and the 30-bed, level III Jackson-Madison County General Hospital NICU from October 2018 to September 2020. We collected data from October 8, 2018 to February 23, 2020 at the VUMC NICU and from March 15, 2019 to September 23, 2020 in the Jackson-Madison NICU with differences in study periods due to local infrastructure for data collection and restrictions on clinical research during the COVID-19 pandemic. We included all infants who received VTV as the initial ventilation modality prior to postnatal day 14. We excluded infants who received PLV or high frequency ventilation prior to receiving VTV and infants with congenital pulmonary airway malformations. The VUMC institutional review board approved the study with a waiver of consent.
Unit practices
In both NICUs, non-invasive ventilation is the primary mode of respiratory support for all infants born at less than 32 weeks’ gestational age (GA). For infants who receive endotracheal intubation, conventional VTV modes are the most common ventilator modalities used. During the study, both NICUs primarily used either flow-cycled or time-cycled modes with the volume guarantee feature and leak compensation on the Dräger Evita Infinity V500 ventilator (Drägerwerk AG and Co, Lübeck, Germany) activated. Both study units utilized flow sensors placed at the proximal end of the endotracheal tube. High frequency jet ventilation is generally used as the first ventilation modality for all non-vigorous infants less than 25 weeks GA. At VUMC, existing unit guidelines were based on the limited-evidence available for choosing initial VT settings [8, 9, 13,14,15]. These guidelines were not present at the Jackson-Madison County General Hospital NICU during the study period.
Study outcomes
The primary outcome for each infant was the initial VT used during the first MV course in mL per kg of birth weight (BW). We defined the initial VT as the first VT that was used for 15 or more consecutive minutes after initiating MV. Each initial VT was then classified as congruent or not with the available literature [8, 9, 13, 14] according to the birth weight of the infant: <700 g (g) (5.5–6 mL/kg), 700 – <1250 g (4.5–5 mL/kg), and ≥1250 g (4–4.5 mL/kg).
Data sources and additional variables
We determined the initial VT and FiO2 by downloading data directly from the mechanical ventilators. Patients with missing ventilator data, defined as those for whom ventilator data at the beginning of the ventilation course were not downloaded, were excluded from the study. The initial FiO2 was defined as the recorded value on each ventilator at the same time as the initial VT. We determined the demographic and clinical characteristics of study infants including sex, race, inborn status, antenatal steroid use, postnatal day at NICU admission, BW, GA, and Clinical Risk Index for Babies (CRIB) score [16] by querying local NICU research databases manually curated by trained research nurses in each unit and electronic health records using Epic’s Clarity database (Epic Systems Corporation, Verona, WI). When applicable, one study investigator (LAK) performed manual chart review to confirm outliers and capture missing data elements.
Statistical analysis
We generated descriptive statistics to define the baseline characteristics of study infants using median and interquartile range (IQR) for continuous variables and percentages for nominal variables. Initial VT was described using median and IQR and agreement with the limited published VT data as compounded by a single review article [13] was reported using counts and percentages. The number of patients who received an initial VT of exactly 5.0 mL/kg was reported using counts and percentages. For initial VT, we reported the total cohort and values stratified by BW. Because this was a retrospective cohort analysis, no sample size calculations were performed.
To evaluate which factors were associated with an initial VT consistent with the limited published literature, we fit a multivariable logistic regression model to the data with the congruence of initial TV with recommendations by a single review article [13] as the dependent variable and the following a priori identified independent variables: BW, sex, inborn status, CRIB score, and initial FiO2.
Finally, we performed a pre-specified sensitivity analysis to account for potential rounding errors by clinicians in either VT or estimated BW. For this, we classified the initial VT for each ventilation course as congruent with published literature if it was within 0.3 mL/kg above or below the literature recommended initial VT range. This adjustment accounts for the BW specific rounding of the initial VT to a whole number that commonly occurs in practice. We then repeated our multivariable logistic regression analysis with the expanded cohort of infants with VT in agreement with recommended initial VT. All statistical analyses were performed using Stata/BE 17.0 (StataCorp, College Station, TX).
Results
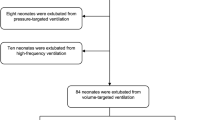
During the study period, 558 infants received MV in the study NICUs. Of these, 313/558 (56%) met study inclusion criteria (Fig. 1). The most common reasons for exclusion from the study were missing ventilator data files, MV after 14 days post menstrual age, and high frequency ventilation prior to conventional MV. There were more infants in our cohort who were not in agreement with the published literature for initial tidal volume. The majority of study infants were inborn with median BW and GA of 2300 g and 35 weeks, respectively (Table 1).

#Total may be greater than total number excluded due to patients being in multiple categories; PMA (post menstrual age), HFV (high frequency ventilation), CMV (conventional mechanical ventilation), CPAM (congenital pulmonary airway malformation).
The most common initial VT used was 5.0 mL/kg (median 5.0 mL/kg, IQR 5.0–5.1), with 154/313 (49%) of infants receiving an initial VT of exactly 5.0 mL/kg. This was the most common VT across the two study NICUs (50% and 37%). When stratified by BW, 5.0 mL/kg was most commonly used in larger infants: <700 g: 5/25 (20%), 700–<1250 g: 26/50 (52%), and ≥1250: 123/238 (52%). Infants with a BW < 700 g had the greatest variability in the initial VT used, though the initial VT clustered around 5.0 mL/kg in all three BW strata (Table 2). All initial VTs for infants in our cohort are shown in Fig. 2. The most common initial tidal volumes clustered around 5.0 mL/kg with 49% of infants receiving exactly 5.0 mL/kg. 1/313 (0.3%) infants received an initial VT less than 3.0 mL/kg with the actual initial VT recorded at 2.9 mL/kg. The highest initial VT was 8.0 mL/kg and 10/313 (3.2%) received an initial VT greater than 6.0 mL/kg (Fig. 2).

Initial tidal volume and literature-informed range based on birth weight.
45/313 (14%) infants received an initial VT that was congruent with the limited-evidence [8, 9, 13, 14] available. The percentage of infants who received an initial VT in agreement was highest in infants with a BW of 700–<1250 g (Table 1), which was also the only BW category that included 5.0 mL/kg in the recommendation. This accounts for the clinical characteristic differences seen between those in agreement with literature-informed initial VT and those with non-agreement with literature-informed initial VT (Table 1). Infants within the BW category of 700–<1250 g were more likely to have a lower GA, receive antenatal steroids, and be inborn. In multivariable logistic regression analysis, having a BW 700–<1250 g was the single factor significantly associated with an initial VT in agreement with initial VT literature (aOR 9.4, 95% CI 1.7–50.4) (Table 2).
In our sensitivity analysis using an expanded range for initial VT, the number of infants who had an initial VT congruent with the published data increased to 76/313 (24%, Table 3). Consistent with our main analyses, the single factor associated with an initial VT in agreement with the published literature was having a BW of 700–<1250 g (aOR 4.8, 95% CI 1.2–19.7).
Discussion
We provide the first observational data regarding the use of initial VT in a large multicenter cohort of critically ill infants on VTV. Nearly half of infants in our cohort received an initial VT of exactly 5.0 mL/kg and most infants had an initial VT clustered near 5.0 mL/kg. Though most infants received an initial VT near 5.0 mL/kg, several infants received a VT well outside recommended ranges for initial neonatal VTs. 14% of infants had initial VTs that were congruent with the limited-evidence available to inform choice of VT [8, 9, 13, 14]. Having a BW 700–<1250 g was the single factor significantly associated with having an initial VT in agreement with published literature likely because this BW category included 5.0 mL/kg in the recommended range.
While we report the first clinical data regarding the use of initial VT during neonatal VTV, the related finding that clinicians are more likely to opt for an initial VT of 5.0 mL/kg, regardless of the patient size or respiratory pathology, has been reported previously. In a survey of neonatologists in the United States and Canada, Gupta and Keszler presented survey respondents with five clinical vignettes and asked clinicians to choose the VT they would use during VTV. Similar to observations in our study, the majority of survey respondents (41–84% depending on the vignette) chose 5.0 mL/kg as the initial VT [7], despite studies which have suggested that set VT should be individualized based on the patient size, instrumental dead space, and respiratory pathology [8, 9, 11, 12, 14, 17,18,19,20]. However, these studies are mainly retrospective and include small sample sizes. Our study also observed this preference in two NICUs with nearly exclusive use of VTV [15]. At the time of our study, the VUMC NICU had unit guidelines in place for VT based on BW and respiratory pathology while the Jackson-Madison NICU did not. Despite these differences, infants in both units received similar initial VT.
While we did not survey clinicians and respiratory therapists in our study about their reason for using 5.0 mL/kg as the initial VT in nearly all cases, multiple reasons for these findings are possible. First, the use of 5.0 mL/kg may be due to the cognitive ease of remembering this value as a starting place for VTV. Second, it is possible that clinicians may be unaware of the literature recommending an individualized approach to choosing the initial VT. Finally, it is possible that clinicians do not perceive the evidence-base for choosing appropriate initial VT for VTV as robust. Unlike in adult medicine [21], no randomized trials comparing specific VTs and evaluating long-term outcomes such as BPD or neurodevelopmental outcomes have been performed in neonates. Therefore, clinicians may feel that optimal initial VTs are still unknown and that choosing a consistent and reliable VT, such as 5.0 ml/kg, is an appropriate starting place in most scenarios. Thus, future research in neonatal VTV should focus on both evaluating the optimal VT to enhance long-term outcomes as well as interventions, such as clinical decision support tools, to implement the optimal VT into clinical practice.
Though the effect of different VT on long-term outcomes is not known, several short-term studies are available to guide current practice [8, 9]. Nassabeh-Montazami et al showed that smaller infants require higher initial VT to achieve normal carbon dioxide levels due to increased instrumental dead space [9]. Conversely, excessive VTs must be avoided to minimize volutrauma [22]. Small initial VTs (3 mL/kg) have also been shown to increase inflammatory cytokines likely due to ineffective alveolar recruitment [23]. In our study, we found that a small minority of infants received initial VTs of >6 mL/kg (3.2%) and of <3 mL/kg (0.3%). Though we do not know the exact reason, it is possible that these outliers were due to incorrect VT calculations because of inaccurate BW estimations or erroneous calculations at the bedside. Many ventilators require BW to be entered upon initiation of MV, opening up the future possibility of ventilator based clinical decision support or safety warnings when inappropriate VT are entered.
Our study had several limitations. First, our study was observational in nature and did not allow us to determine how much effect the choice of initial VT had on long-term clinical outcomes such as BPD and neurodevelopmental impairment. Second though we captured a large cohort of infants, we excluded infants with diagnoses such as congenital diaphragmatic hernia or BPD. In our centers during the study period, most of the infants with congenital diaphragmatic hernia were ventilated with either PLV or high-frequency ventilation. Further, all infants with established BPD were excluded by limiting the study to infants who were ventilated within the first two postnatal weeks. Third, we did not include the initial VT per kilogram that clinicians intended to use, only the VT that each infant received. We attempted to adjust for errors in rounding of VT or BW during our sensitivity analysis and found that even with these adjustments, most initial VT clustered around 5.0 mL/kg. Finally, our study may have limited generalizability as it was conducted in two units which primarily use VTV. While our findings likely represent the prevailing practices in most NICUs given prior survey results [7], more studies are needed in NICUs with different clinical practices.
In two NICUs that primarily use VTV, clinicians widely favored using an initial VT of 5.0 mL/kg for infants. Future work is needed to better define the optimal initial VTs for VTV and to develop tools, such as clinical decision support, to assist clinicians in using evidence-based strategies during neonatal VTV.
Data availability
A deidentified dataset and the Stata and R code used to clean the dataset may be shared with interested researchers upon request.
References
Vendettuoli V, Bellu R, Zanini R, Mosca F, Gagliardi L.Italian Neonatal Network Changes in ventilator strategies and outcomes in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2014;99:F321–324.
Laptook AR, O’Shea TM, Shankaran S, Bhaskar B, Network NN. Adverse neurodevelopmental outcomes among extremely low birth weight infants with a normal head ultrasound: prevalence and antecedents. Pediatrics. 2005;115:673–80.
Guillot M, Guo T, Ufkes S, Schneider J, Synnes A, Chau V, et al. Mechanical ventilation duration, brainstem development, and neurodevelopment in children born preterm: a prospective cohort study. J Pediatr. 2020;226:87–95.e83.
Jensen EA, DeMauro SB, Kornhauser M, Aghai ZH, Greenspan JS, Dysart KC. Effects of multiple ventilation courses and duration of mechanical ventilation on respiratory outcomes in extremely low-birth-weight infants. JAMA Pediatr. 2015;169:1011–7.
Islam JY, Keller RL, Aschner JL, Hartert TV, Moore PE. Understanding the short- and long-term respiratory outcomes of prematurity and Bronchopulmonary Dysplasia. Am J Respir Crit Care Med. 2015;192:134–56.
Klingenberg C, Wheeler KI, McCallion N, Morley CJ, Davis PG. Volume-targeted versus pressure-limited ventilation in neonates. Cochrane Database Syst Rev. 2017;10:CD003666.
Gupta A, Keszler M. Survey of ventilation practices in the neonatal intensive care units of the United States and Canada: use of volume-targeted ventilation and barriers to its use. Am J Perinatol. 2018;36:484–9.
Dawson C, Davies MW. Volume-targeted ventilation and arterial carbon dioxide in neonates. J Paediatr Child Health. 2005;41:518–21.
Nassabeh-Montazami S, Abubakar KM, Keszler M. The impact of instrumental dead-space in volume-targeted ventilation of the extremely low birth weight (ELBW) infant. Pediatr Pulmonol. 2009;44:128–33.
Keszler M, Nassabeh-Montazami S, Abubakar K. Evolution of tidal volume requirement during the first 3 weeks of life in infants <800 g ventilated with Volume Guarantee. Arch Dis Child Fetal Neonatal Ed. 2009;94:F279–282.
Sharma S, Abubakar KM, Keszler M. Tidal volume in infants with congenital diaphragmatic hernia supported with conventional mechanical ventilation. Am J Perinatol. 2015;32:577–82.
Sharma S, Clark S, Abubakar K, Keszler M. Tidal volume requirement in mechanically ventilated infants with meconium aspiration syndrome. Am J Perinatol. 2015;32:916–9.
Keszler M. Volume-targeted ventilation: one size does not fit all. Evidence-based recommendations for successful use. Arch Dis Child Fetal Neonatal Ed. 2019;104:F108–F112.
Dassios T, Dixon P, Hickey A, Fouzas S, Greenough A. Physiological and anatomical dead space in mechanically ventilated newborn infants. Pediatr Pulmonol. 2018;53:57–63.
Hatch LD, Sala C, Araya W, Rivard M, Bolton J, Rivard A, et al. Increasing volume-targeted ventilation use in the NICU. Pediatrics. 2021;147:e20201500.
Tarnow-Mordi W, Parry G. The CRIB score. Lancet. 1993;342:1365.
te Pas AB, Kamlin CO, Dawson JA, O’Donnell C, Sokol J, Stewart M, et al. Ventilation and spontaneous breathing at birth of infants with congenital diaphragmatic hernia. J Pediatr. 2009;154:369–73.
Henderson-Smart DJ, De Paoli AG, Clark RH, Bhuta T. High frequency oscillatory ventilation versus conventional ventilation for infants with severe pulmonary dysfunction born at or near term. Cochrane Database Syst Rev. 2009;2009:CD002974.
Hunt K, Dassios T, Ali K, Greenough A. Volume targeting levels and work of breathing in infants with evolving or established bronchopulmonary dysplasia. Arch Dis Child Fetal Neonatal Ed. 2019;104:F46–f49.
Abman SH, Collaco JM, Shepherd EG, Keszler M, Cuevas-Guaman M, Welty SE, et al. Interdisciplinary care of children with severe Bronchopulmonary Dysplasia. J Pediatr. 2017;181:12–28.e11.
Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl J Med. 2000;342:1301–8.
Clark RH, Slutsky AS, Gerstmann DR. Lung protective strategies of ventilation in the neonate: what are they? Pediatrics. 2000;105:112–4. 1 Pt 1
Lista G, Castoldi F, Fontana P, Reali R, Reggiani A, Bianchi S, et al. Lung inflammation in preterm infants with respiratory distress syndrome: effects of ventilation with different tidal volumes. Pediatr Pulmonol. 2006;41:357–63.
Acknowledgements
We express our deepest gratitude to Steven Steele, Theresa Rogers, and Eva Dye, DNP who helped with research data collection for this study.
Funding
LAK received funding by the National Library of Medicine T15 LM007450 to perform this study. LDH was supported by the Vanderbilt Department of Pediatrics Turner-Hazinski Faculty Scholars Award and the Gerber Foundation. Use of the Research Electronic Data Capture program was supported by UL1 TR000445 from NCATS/NIH.
Author information
Authors and Affiliations
Contributions
LAK, MWA, CUL, and LDH conceived this project and outlined the primary objectives for this manuscript. LAK and LDH extracted and reviewed the ventilator data and performed the data analyses. SOG implemented and extracted data from the Jackson-Madison NICU location. LAK, MWA, ABM, and AW assisted with data extraction and transformation of data extracted from the electronic health record. LAK, MWA, and LDH produced the first draft of the manuscript for publication. All authors critically appraised and approved the final submitted version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Knake, L.A., Alrifai, M.W., McCoy, A.B. et al. Factors associated with initial tidal volume selection during neonatal volume-targeted ventilation in two NICUs: a retrospective cohort study. J Perinatol 42, 756–760 (2022). https://doi.org/10.1038/s41372-022-01362-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-022-01362-0
- Springer Nature America, Inc.