
Abstract
Introduction
Patients with low socioeconomic status have been reported to have poorer outcome than those with a high socioeconomic status after several types of surgery. The influence of socioeconomic factors on weight loss after bariatric surgery remains unclear. The aim of the present study was to evaluate the association between socioeconomic factors and postoperative weight loss.
Materials and methods
This was a retrospective, nationwide cohort study with 5-year follow-up data for 13,275 patients operated with primary gastric bypass in Sweden between January 2007 and December 2012 (n = 13,275), linking data from the Scandinavian Obesity Surgery Registry, Statistics Sweden, the Swedish National Patient Register, and the Swedish Prescribed Drugs Register. The assessed socioeconomic variables were education, profession, disposable income, place of residence, marital status, financial aid and heritage. The main outcome was weight loss 5 years after surgery, measured as total weight loss (TWL). Linear regression models, adjusted for age, preoperative body mass index (BMI), sex and comorbid diseases were constructed.
Results
The mean TWL 5 years after surgery was 28.3 ± 9.86%. In the adjusted model, first-generation immigrants (%TWL, B −2.4 [95% CI −2.9 to −1.9], p < 0.0001) lost significantly less weight than the mean, while residents in medium-sized (B 0.8 [95% CI 0.4–1.2], p = 0.0001) or small towns (B 0.8 [95% CI 0.4–1.2], p < 0.0001) lost significantly more weight.
Conclusions
All socioeconomic groups experienced improvements in weight after bariatric surgery. However, as first-generation immigrants and patients residing in larger towns (>200,000 inhabitants) tend to have inferior weight loss compared to other groups, increased support in the pre- and postoperative setting for these two groups could be of value. The remaining socioeconomic factors appear to have a weaker association with postoperative weight loss.
Similar content being viewed by others


Introduction
Gastric bypass surgery is a safe and effective treatment for morbid obesity [1, 2]. Mean weight loss remains high even after long-term follow-up [3]. There are groups of patients, however, that experience a lesser degree of long-term weight loss [4]. While age, sex and obesity-related comorbidities, such as diabetes, have been reported to influence postoperative weight loss [5,6,7,8,9,10], the influence of socioeconomic factors remains unclear [11, 12]. A low socioeconomic status has been reported to be associated with higher complication rates and poorer outcomes after surgical procedures [13,14,15]. Recent studies have shown the same applies to gastric bypass surgery, with an increased risk for postoperative complications and less improvement in quality of life [16, 17]. The recognition of risk factors for inadequate postoperative weight loss that can be identified preoperatively may help in identifying certain groups of patients who require increased support in the pre- and postoperative setting.
The aim of the present study was to identify socioeconomic factors associated with suboptimal postoperative weight loss 5 years after surgery.
Methods
The Scandinavian Obesity Surgery Register (SOReg) is a nationwide register for metabolic surgery, containing virtually all patients operated with metabolic surgery in Sweden since 2007 [18]. From the SOReg, all primary gastric bypass procedures from June 1, 2007 until December 31, 2012, were identified and assessed for inclusion in the study. Pre-established exclusion criteria were age <18 years; missing information on weight 5 years after surgery; and operation at a centre not routinely performing a 5-year follow-up. Based on personal identification numbers (unique to all Swedish citizens), data from SOReg were cross-linked to the Swedish National Patient Register, the Swedish Prescribed Drug Register, and Statistics Sweden. The Swedish National Patient Register covers inpatient and outpatient care with high validity for the variables included in the present study [19]. The Prescribed Drug Register covers all prescribed drugs in Sweden, based on ATC-codes [20].
Baseline characteristics, perioperative data, and follow-up data were obtained from the SOReg, the Swedish National Patient Register and the Swedish Prescribed Drug Register.
Patient-specific data on socioeconomic factors (education, profession, disposable income, residence, marital status, financial aid, and heritage) were obtained from Statistics Sweden, reporting quality assured and validated personal data on socioeconomic factors (https://www.scb.se/en/About-us/main-activity/quality-work/statistics-sweden-has-quality-certification/). Educational level was divided into four groups based on the highest completed education at the time of surgery: primary education (≤9 years of schooling), secondary education (completed 11–12 years of schooling), higher education ≤3 years (completed college or university degree with ≤3 years of education), and higher education >3 years. Profession was reported in accordance with the International Standard Classification of Occupations from 1988 (ISCO-88) and further classified into the following subgroups (based on the respective ISCO-88 groups): Senior officials and management (group 1), Professionals and technicians (groups 2 and 3), Clerical support workers (group 4), Service and sales workers (group 5), Manual labour (groups 6–8), and Elementary occupation (group 9). The place of residence was divided into three categories: Large city (>200,000 inhabitants) and municipality near a large city, medium-sized town (≥50,000 inhabitants) and municipality near a medium-sized town, and smaller town or urban area (<50,000 inhabitants) and rural municipality disposable income, in accordance with the definition of the Swedish Association of Local Authorities and Regions. Disposable income (total taxable income minus taxes and other negative transfers) was divided into percentiles (lowest 20th, 20th to median, median to 80th, and highest 80th) based on the disposable income of all adults in Sweden during the year of surgery. Marital status, financial aid, and heritage were all based on accepted standards as described previously [16].
Comorbidity at baseline was defined as continuous treatment (pharmacological or with positive airway pressure) for sleep apnoea, hypertension, dyslipidaemia, dyspepsia/GERD, and depression. Diabetes was defined according to the American Diabetes Association [21]. Cardiovascular comorbidity was defined as a diagnosis of ischaemic heart disease, angina pectoris, arrhythmia, or heart failure at any time prior to surgery.
Procedure
The surgical technique for laparoscopic gastric bypass is highly standardized in Sweden, with the majority being antecolic, antegastric, Roux-en-Y gastric bypass with a small (<25 mL) gastric pouch, an alimentary limb of 100 cm and a biliopancreatic limb of 50 cm [22]. In open cases, the gastric pouch and small bowel are handled similarly.
Outcome
The main outcome was weight loss 5 years after surgery defined as the percentage of total weight loss (%TWL). Secondary outcomes were percentage excess BMI loss (%EBMIL = 100 × [preoperative BMI – BMI 5 years after surgery]/[preoperative BMI – 25]), and the proportion of patients achieving satisfactory weight loss (defined as EBMIL ≥ 50%).
Sensitivity analysis
Risk factors for loss to follow-up were analyzed as a sensitivity analysis. A further analysis was performed including only patients operated on at centres with >75% follow-up rates for the same year of surgery.
Statistics
Categorical values were presented as numbers and percentages, continuous values as mean ± standard deviation for values with normal distribution, and median with interquartile range (IQR) for values without normal distribution. The association between patient-specific risk factors and weight loss was evaluated using linear regression analyses with the regression coefficient (B) and 95% confidence interval as measures of association. The socioeconomic factors were further evaluated in a linear regression model adjusted for preoperative factors (age, BMI, sex, and comorbidity) known to influence weight loss.
The association between patient-specific risk factors and the chance of achieving an EBMIL ≥ 50% was evaluated with logistic regression. All factors evaluated were also entered into a multivariable logistic regression model. The model was also tested for multicollinearity using linear regression. A variance inflation factor (VIF) >5 was considered to indicate an issue with multicollinearity.
Due to the multiplicity of variables analyzed, the Bonferroni–Holm method was used to compensate for multiple calculations [23].
IBM SPSS version 25 (IBM Corporation, Armonk, New York, USA) was used for all statistical analyses.
Results
During the inclusion period, 29,524 patients operated with a primary gastric bypass procedure were identified. After exclusion of patients who died before the 5-year follow-up (n = 336), patients operated on at a centre not routinely performing a 5-year follow-up (n = 4326), and patients without weight registered at the 5-year follow-up (n = 11,587), 13,275 patients remained within the study group (53.4% of patients with potential 5-year follow-up).
Operative data and weight results
The mean age at surgery was 42.3 ± 11.1 years, the mean preoperative BMI was 42.5 ± 5.3 kg/m2, 77.6% were women and 49.8% suffered an obesity-related comorbid condition.
In all, 94.6% of the operations were managed with a laparoscopic approach (n = 12,561), 1.3% were converted to open surgery (n = 167), and 4.1% were primarily open procedures (n = 547). The mean operation time was 84 ± 38.9 min, with a median postoperative hospital stay of 2 days (IQR 2–3 days).
At 1, 2, and 5 years after surgery, the mean BMI was reduced to 29.2 ± 4.6 kg/m2, 28.8 ± 4.8 kg/m2, and 30.4 ± 5.3 kg/m2, respectively (p < 0.0001 for all, compared to baseline). At 5 years, the average reduction in BMI was 12.1 ± 4.8 BMI units, corresponding to an average percentage %TWL of 28.3 ± 9.9%, and a %EBMIL of 71.6 ± 26.1%. At that time point, satisfactory excess weight loss (≥50% EBMIL) was achieved in 10,572 patients (79.6%).
Factors affecting postoperative weight loss at 5 years
Lower %TWL was associated with an occupation other than service and sales work, higher disposable income, living in larger cities, receiving financial aid other than social benefits, and being a first-generation immigrant, as well as older age, male gender, and obesity-related comorbidities. Higher %TWL was seen in higher BMI and single status (Table 1).
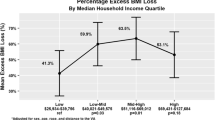
An occupation other than service and sales work, clerical support work or management, receiving financial aid, being a 1st generation immigrant, and disposable incomes in the lowest 20th, and highest 80th percentiles, older age, male gender, higher BMI, and obesity-related comorbidity (other than dyspepsia/GERD) were associated with a lower %EBMIL. After correction for multiple calculations, disposable income and receiving social benefits no longer remained significant factors (Table 2).
After adjustment for factors previously known to affect weight loss after bariatric surgery (age, BMI, sex, and obesity-related comorbidities), higher education, living in larger cities and being a first-generation immigrant were independently associated with a lower %TWL and %EBMIL. An occupation as a professional or technician and receiving social benefits were independently associated with a lower %TWL, but not independently associated with a lower %EBMIL. After correction for multiple calculations, place of residence and being a first-generation immigrant remained significant risk factors (Table 3).
Receiving disability pension/early retirement, social benefits, and being a first-generation immigrant, were all independently associated with a lower chance of achieving a postoperative EBMIL ≥ 50%, while employment as a senior official or manager, higher income, and residence in small towns were associated with a higher chance (Table 4).
Amongst first-generation immigrants, all non-Nordic subgroups had less weight loss, in terms of both %TWL and %EBMIL. Patients born outside Europe also had a lower chance of achieving a postoperative EBMIL ≥ 50% (Table 5).
No multicollinearity issue was detected in either of the multivariable models.
Sensitivity analysis
Loss to follow-up was more common in patients with a low disposable income, those receiving social benefits, citizens of medium-sized towns, patients who were unmarried, patients with a higher BMI and younger ages, males, and those with absence of comorbidities (except for depression) (Supplementary Table 1). However, when entering only patients from centres with a >75% follow-up rate, very similar results to those of the main analyses were seen (Supplementary Table 2).
Discussion
Among the socioeconomic variables studied, being a first-generation immigrant and living in a larger city were independently associated with less weight loss (measured by %TWL and %EBMIL).
With these exceptions, socioeconomic factors had less impact on weight loss than other patient-specific factors, which is consistent with previous smaller studies reporting a lack of association [11, 12].
First-generation immigrants experienced significantly less weight loss at 5 years than other groups of patients, and fewer patients in this group achieved satisfactory weight loss. After adjustment for other potential risk factors, the risk for less weight loss among patients born outside of the Nordic countries, and in particular outside of Europe, was equivalent to the effect of strong patient-demographic factors such as age, sex, and metabolic comorbidities. This group of patients may also experience higher complication rates [16] as well as less improvement in HRQoL [17]. Although there may be a difference in the response to bariatric surgery between ethnic groups [11, 24], the inferior weight loss among first-generation immigrants could be related to difficulties in their ability to understand and apply preoperative information (health literacy), failure to appreciate the importance of patient involvement, lack of a supportive network, and simple misunderstandings due to language or cultural mismatch between care providers and patients [25]. Furthermore, inherited eating habits and a different food culture could be of importance. Finally, the motivation of the patient to undergo bariatric surgery is known to differ [26, 27]. Although immigrants from countries outside of Europe had a tendency towards less weight loss, first-generation immigrants from other parts of Europe also achieved less weight loss than patients born in Sweden. This finding suggests a psychosocial rather than a strictly biological explanation for these differences in outcome.
Patients residing in larger cities had lost less weight 5 years after surgery than patients residing in small towns or municipalities. This group of patients has also been reported to be lost to follow-up more often and report less improvement in health-related quality of life after bariatric surgery [17, 28]. The explanation for this is likely to be multifactorial, including behavioural and sociopsychological factors not considered in the present study. Part of the explanation may lie in the chronic stress and higher cortisol levels associated with urban life [29], less time for exercise due to congestion, increased travelling times, as well as a higher availability of energy dense food, often called “junk food”.
In the unadjusted analyses, receiving social benefits were associated with less weight loss, and patients receiving social benefits or disability pension/early retirement were less likely to achieve satisfactory weight loss. Both groups are composed of individuals who often have a difficult economic situation and a higher proportion of physical or mental disabilities that influence their ability to follow diet and exercise recommendations postoperatively. Furthermore, these socioeconomically challenged patients often have a weaker social network and lower health literacy [30]. In fact, lower health literacy may contribute to poor outcome from non-communicable disease among socioeconomically weaker groups [31]. Moreover, a weak association was seen between education, profession and weight loss. Although this could be related to longer working hours and poor work–life balance, the slightly lower weight loss among patients with higher education and professionals/technicians contradicts previous reports and is likely to be due to inequality of access to bariatric surgery rather than a direct association [32].
In a previous American study on US veterans, the average income in the neighbourhood of the patient was reported to influence outcome after bariatric surgery [33]. In our study, higher personal income was associated with a slightly greater EBMIL but lower TWL, thus signalling a potential confounding effect of BMI. Indeed, after correction for other relevant factors, including BMI, no correlation was seen. The association between average neighbourhood income and bariatric surgery outcome is more likely to be explained by other factors associated with residence in poorer neighbourhoods, such as health literacy, lack of a supportive network, and poor access to healthcare. Indeed, it is known that patients with higher incomes have better access to bariatric surgery [34].
In addition to socioeconomic factors, several patient-specific factors also influenced 5-year weight loss. Older age, male gender, and obesity-related comorbidities other than dyspepsia/GERD were all associated with lower postoperative weight loss as well as a reduced chance of achieving satisfactory weight loss (EBMIL > 50%). Preoperative BMI had a strong impact on weight loss, but the impact of BMI was highly dependent on the outcome measured. When weight loss was measured as EBMIL, patients with a higher BMI at the time of surgery had less weight loss, which is in accordance with the results of several previous studies addressing EMBIL as an outcome measure [5, 7, 8, 35]. On the other hand, patients with a higher preoperative BMI lost a greater proportion of their total weight, supporting the results of studies using total weight loss as an outcome measure [6]. Given the link between TWL and other outcomes after bariatric surgery [36], both differences in total weight as well as excess BMI need to be considered when evaluating weight loss after bariatric surgery.
The greater weight loss among younger patients and those without obesity-related comorbidities is in-line with previous studies [5, 7, 9] and may be related to other factors, such as mobility, covariation with other risk factors (such as comorbid disease and age), and established insulin resistance with higher circulating insulin levels, as well as to the effects of medication on weight gain. Clinical depression has also been reported to be associated with poorer follow-up attendance, which in turn is known to be associated with poorer long-term weight results [28, 37].
Women had significantly greater weight loss and more often experienced satisfactory weight loss after surgery than men. Although this result contradicts the result of a recent Swiss study including 444 patients [6], it is supported by older studies [11]. Women also attend follow-up visits more often than men [28] and experience better improvement in health-related quality of life [17]. The better compliance and results among women may well be the result of different motivations for surgery. Furthermore, preoperative information, perioperative care, and long-term follow-up programmes are likely to be more adapted to suit the needs of women, since more women than men undergo bariatric surgery.
Although several groups with postoperative weight loss less than the mean were identified in this study, it is important to point out that all subgroups showed good weight loss results, confirming the benefits of bariatric surgery. The relatively poor weight loss results among certain subgroups warrant further research to gain more information about specific reasons. Meanwhile, since several of the groups experiencing a poorer weight-related outcome also tended to miss follow-up visits [28], bariatric surgical centres should concentrate on improving follow-up attendance rates, motivating and supporting these patients, and adapting follow-up programmes to meet the requirements of individual patients. The results of the present study suggest that certain socioeconomic groups, in particular first-generation immigrants, are at particular risk for poorer outcome and are a group likely to benefit from more intense perioperative support, as well as directed information adapted to cultural aspects and native language.
Strengths and limitations
The major strengths of this study lie in the large number of patients included and the high quality of data. Furthermore, most previous studies have only measured weight loss as either TWL or EBMIL, but as evident in the present study, both measures are highly dependent on preoperative BMI, though in different ways. EBMIL allows comparisons of patients with varying initial and excess weights, but has the disadvantage of underestimating successful weight loss in patients with very high BMIs. TWL may be a better option under these circumstances, but it may not always provide sufficient clinically relevant information to reflect weight loss success or failure [38]. The inclusion of both measures in this study is thus a strength. There are, however, limitations that must be acknowledged. There were many patients whose weight at the 5-year follow-up was not registered. Maintaining a high follow-up rate over a long period after bariatric surgery is a great challenge [39]. For the purposes of research and patient well-being, however, follow-up is important since patients lost to follow-up are often those with inferior weight loss [28]. Even though a second analysis including only centres with high follow-up rates showed very similar results, the high loss to follow-up may still constitute a potential source of bias. The present study was also limited to socioeconomic and demographic definitions that were decided prior to starting the study. For this reason, cognitive and behavioural factors known to influence weight loss could not be evaluated [40, 41].
Conclusion
All socioeconomic groups experienced improvements in weight after bariatric surgery. However, as first-generation immigrants and residents of larger cities tend to have inferior weight loss, increased support in the pre- and postoperative setting for these two groups could be of value. The remaining socioeconomic factors appear to have a weaker association with postoperative weight loss.
References
Stenberg E, Szabo E, Ågren G, Näslund E, Boman L, Bylund A, et al. Early complications after laparoscopic gastric bypass surgery: results from the scandinavian obesity surgery registry. Ann Surg. 2014;260:1040–7.
Sundbom M, Hedberg J, Marsk R, Boman L, Bylund A, Hedenbro J, et al. Substantial decrease in comorbidity 5 years after gastric bypass: a population-based Study From the Scandinavian Obesity Surgery Registry. Ann Surg. 2017;265:1166–71.
Sjostrom L, Peltonen M, Jacobson P, Ahlin S, Andersson-Assarsson J, Anveden A, et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA. 2014;311:2297–304.
Courcoulas AP, King WC, Belle SH, Berk P, Flum DR, Garcia L, et al. Seven-year weight trajectories and health outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) Study. JAMA Surg. 2018;153:427–34.
Ortega E, Morinigo R, Flores L, Moize V, Rios M, Lacy AM, et al. Predictive factors of excess body weight loss 1 year after laparoscopic bariatric surgery. Surg Endosc. 2012;26:1744–50.
Seyssel K, Suter M, Pattou F, Caiazzo R, Verkindt H, Raverdy V, et al. A predictive model of weight loss after Roux-en-Y gastric bypass up to 5 years after surgery: a useful tool to select and manage candidates to bariatric surgery. Obes Surg. 2018;28:3393–9.
Al-Khyatt W, Ryall R, Leeder P, Ahmed J, Awad S. Predictors of inadequate weight loss after laparoscopic gastric bypass for morbid obesity. Obes Surg. 2017;27:1446–52.
Wood GC, Benotti PN, Lee CJ, Mirshahi T, Still CD, Gerhard GS, et al. Evaluation of the association between preoperative clinical factors and long-term weight loss after Roux-en-Y gastric bypass. JAMA Surg. 2016;151:1056–62.
Chang WW, Hawkins DN, Brockmeyer JR, Faler BJ, Hoppe SW, Prasad BM. Factors influencing long-term weight loss after bariatric surgery. Surg Obes Relat Dis. 2019;15:456–61.
Sillen L, Andersson E. Patient factors predicting weight loss after Roux-en-Y gastric bypass. J Obes. 2017;2017:3278751.
Adams ST, Salhab M, Hussain ZI, Miller GV, Leveson SH. Roux-en-Y gastric bypass for morbid obesity: what are the preoperative predictors of weight loss? Postgrad Med J. 2013;89:411–6.
Alfa Wali M, Ashrafian H, Schofield KL, Harling L, Alkandari A, Darzi A, et al. Is social deprivation associated with weight loss outcomes following bariatric surgery? A 10-year single institutional experience. Obes Surg. 2014;24:2126–32.
Courtney PM, Huddleston JI, Iorio R, Markel DC. Socioeconomic risk adjustment models for reimbursement are necessary in primary total joint arthroplasty. J Arthroplasty. 2017;32:1–5.
Mahal BA, Inverso G, Aizer AA, Ziehr DR, Hyatt AS, Chouteiri TK, et al. Incidence and determinants of 1-month mortality after cancer-directed surgery. Ann Oncol. 2015;26:399–406.
Goljo E, Parasher AK, Iloreta AM, Shrivastava R, Govindaraj S. Racial, ethnic, and socioeconomic disparities in pituitary surgery outcomes. Laryngoscope. 2016;126:808–14.
Stenberg E, Persson C, Näslund E, Ottosson J, Sundbom M, Szabo E, et al. The impact of socioeconomic factors on the early postoperative complication rate after laparoscopic gastric bypass surgery. Surg Obes Relat Dis. 2019;15:575–81.
Gryth K, Persson C, Naslund I, Sundbom M, Naslund E, Stenberg E. The influence of socioeconomic factors on quality-of-life after laparoscopic gastric bypass surgery. Obes Surg. 2019;29:3569–76.
Hedenbro JL, Naslund E, Boman L, Lundegårdh G, Bylund A, Ekelund M, et al. Formation of the Scandinavian Obesity Surgery Registry, SOReg. Obes Surg. 2015;25:1893–1900.
Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450.
Wallerstedt SM, Wettermark B, Hoffmann M. The first decade with the swedish prescribed drug register—a systematic review of the output in the scientific literature. Basic Clin Pharmacol Toxicol. 2016;119(5):464–9.
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81–90.
Olbers T, Lonroth H, Fagevik-Olsen M, Lundell L. Laparoscopic gastric bypass: development of technique, respiratory function, and long-term outcome. Obes Surg. 2003;13:364–70.
Holm S. A simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6:65–70.
Anderson WA, Greene GW, Forse RA, Apovian CM, Istfan NW. Weight loss and health outcomes in African Americans and whites after gastric bypass surgery. Obesity. 2007;15:1455–63.
Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Powe NR, Nelson C, et al. Race, gender, and partnership in the patient-physician relationship. JAMA. 1999;282:583–9.
LaRose JG, Leahey TM, Hill JO, Wing RR. Differences in motivations and weight loss behaviors in young adults and older adults in the National Weight Control Registry. Obesity. 2013;21:449–53.
Trainer S, Benjamin T. Elective surgery to save my life: rethinking the “choice” in bariatric surgery. J Adv Nurs. 2017;73:894–904.
Kedestig J, Stenberg E. Loss to follow-up after laparoscopic gastric bypass surgery—a post hoc analysis of a randomized clinical trial. Surg Obes Relat Dis. 2019;15:880–6.
Zarzycka D, Slusarska B, Marcinowicz L, Wronska I, Kozka M. Assessment of differences in psychosocial resources and state of health of rural and urban residents–based on studies carried out on students during examination stress. Ann Agric Environ Med. 2014;21:882–7.
Sorensen K, Pelikan JM, Rothlin F, Ganahl K, Slonska Z, Doyle G, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25:1053–8.
Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97–107.
Santry HP, Lauderdale DS, Cagney KA, Rathouz PJ, Alverdy JC, Chin MH. Predictors of patient selection in bariatric surgery. Ann Surg. 2007;245(1):59–67.
Carden A, Blum K, Arbaugh CJ, Trickey A, Eisenberg D. Low socioeconomic status is associated with lower weight-loss outcomes 10-years after Roux-en-Y gastric bypass. Surg Endosc. 2019;33:454–9.
Martin M, Beekley A, Kjorstad R, Sebesta J. Socioeconomic disparities in eligibility and access to bariatric surgery: a national population-based analysis. Surg Obes Relat Dis. 2010;6:8–15.
Palmisano S, Silvestri M, Giuricin M, Baldini E, Albertario S, Capelli P, et al. Preoperative predictive factors of successful weight loss and glycaemic control 1 year after gastric bypass for morbid obesity. Obes Surg. 2015;25:2040–6.
King WC, Hinerman AS, Belle SH, Wahed AS, Courcoulas AP. Comparison of the performance of common measures of weight regain after bariatric surgery for association with clinical outcomes. JAMA. 2018;320(15):1560–9.
Keren D, Matter I, Rainis T, Lavy A. Getting the most from the sleeve: the importance of post-operative follow-up. Obes Surg. 2011;21:1887–93.
Brethauer SA, Kim J, El Chaar M, et al. Standardized outcomes reporting in metabolic and bariatric surgery. Surg Obes Relat Dis. 2015;11:489–506.
Higa K, Ho T, Tercero F, Yunus T, Boone KB. Laparoscopic Roux-en-Y gastric bypass: 10-year follow-up. Surg Obes Relat Dis. 2011;7:516–25.
Spitznagel MB, Alosco M, Galioto R, Strain G, Devlin M, Sysko R, et al. The role of cognitive function in postoperative weight loss outcomes: 36-month follow-up. Obes Surg. 2014;24:1078–84.
Sawamoto R, Nozaki T, Nishihara T, Furukawa T, Hata T, Komaki G, et al. Predictors of successful long-term weight loss maintenance: a two-year follow-up. Biopsychosoc Med. 2017;11:14.
Acknowledgements
The study was supported by grants from Region Örebro County Council, the Bengt Ihre Foundation, Stockholm County Council, SRP Diabetes and the NovoNordisk Foundation. None of the supporting bodies influenced the contents of this article.
Funding
This work was supported by grants from Region Örebro County, the Bengt Ihre Foundation, Stockholm County Council, SRP Diabetes, and the NovoNordisk Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
IN has received consultant fees from Baricol Bariatrics AB, Sweden and Ethicon Endosurgery, Johnson & Johnson for work unrelated to the context of the present study. JO has received consultant fees from Vifor Pharma AB, and Ethicon Endosurgery, Johnson & Johnson for work unrelated to the context of the present study. None of the remaining authors declares any conflict of interest.
Ethics
The study was approved by the Regional Ethics Committee in Stockholm and followed the standards of the 1964 Helsinki Declaration and its later amendments.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Stenberg, E., Näslund, I., Persson, C. et al. The association between socioeconomic factors and weight loss 5 years after gastric bypass surgery. Int J Obes 44, 2279–2290 (2020). https://doi.org/10.1038/s41366-020-0637-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-020-0637-0
- Springer Nature Limited
This article is cited by
-
Optimizing Hospital Performance Evaluation in Total Weight Loss Outcomes After Bariatric Surgery: A Retrospective Analysis to Guide Further Improvement in Dutch Hospitals
Obesity Surgery (2024)
-
Major adverse cardiovascular events among patients with type-2 diabetes, a nationwide cohort study comparing primary metabolic and bariatric surgery to GLP-1 receptor agonist treatment
International Journal of Obesity (2023)
-
Mapping the obesity problems scale to the SF-6D: results based on the Scandinavian Obesity Surgery Registry (SOReg)
The European Journal of Health Economics (2023)
-
Towards precision medicine in bariatric surgery prescription
Reviews in Endocrine and Metabolic Disorders (2023)
-
The long weight: association between distressed communities index and long-term weight outcomes following bariatric surgery
Surgical Endoscopy (2023)