
Abstract
Background/Objectives:
Only a few papers have treated of the relationship between Barrett’s esophagus (BE) or erosive esophagitis (E) and coffee or tea intake. We evaluated the role of these beverages in BE and E occurrence.
Subjects/Methods:
Patients with BE (339), E (462) and controls (619) were recruited. Data on coffee and tea and other individual characteristics were collected using a structured questionnaire.
Results:
BE risk was higher in former coffee drinkers, irrespective of levels of exposure (cup per day; ⩽1: OR=3.76, 95% CI 1.33–10.6; >1: OR=3.79, 95% CI 1.31–11.0; test for linear trend (TLT) P=0.006) and was higher with duration (>30 years: OR=4.18, 95% CI 1.43–12.3; TLT P=0.004) and for late quitters, respectively (⩽3 years from cessation: OR=5.95, 95% CI 2.19–16.2; TLT P<0.001). The risk of BE was also higher in subjects who started drinking coffee later (age >18 years: OR=6.10, 95% CI 2.15–17.3). No association was found in current drinkers, but for an increased risk of E in light drinkers (<1 cup per day OR =1.85, 95% CI 1.00–3.43).
A discernible risk reduction of E (about 20%, not significant) and BE (about 30%, P<0.05) was observed in tea drinkers.
Conclusions:
Our data were suggestive of a reduced risk of BE and E with tea intake. An adverse effect of coffee was found among BE patients who had stopped drinking coffee. Coffee or tea intakes could be indicative of other lifestyle habits with protective or adverse impact on esophageal mucosa.
Similar content being viewed by others

Introduction
Barrett's esophagus (BE) is a condition in which the normal esophageal squamous mucosa is replaced by a metaplastic columnar mucosa, conferring a predisposition to esophageal adenocarcinoma. In Western areas, the prevalence of BE is estimated to be between 0.5 and 6.8%, to arrive at 15% in symptomatic patients.1 In Italy it has been estimated to be around 1.5%.2, 3
Chronic gastroesophageal reflux disease (GERD), a spectrum of hiatal hernia, gastroesophageal reflux, heartburn and regurgitation is a risk factor for both BE and erosive esophagitis (E). It is worth noting that GERD is not always present in all patients with endoscopic diagnosis of BE or E and they may also share other modifiable risk factors such as smoking and overweight.1, 4, 5
So far, epidemiologic data regarding coffee and tea consumption and risk of BE and E in Western areas are scarce and inconclusive. Only a few papers examined the relationship between coffee or tea intake and BE or E, while more data exist on the association with some types of cancer.
Coffee consumption did not seem to be associated with risk of BE, nor with GERD.6, 7, 8
A recent study did not also support a correlation between tea intake and the risk of BE,6 while there was a reduced risk of esophageal and other digestive cancers in Asian areas, at higher consumption of green tea.9 On the other side, no association with cancers of the esophagus was found integrating a series of case–control studies conducted in Italy.10
About 90% of adults drink espresso coffee in Italy, while consumption of tea, in particular black tea, is still low.
In this multicenter case–control study we sought to assess the relationship between coffee, tea and herbal tea consumption and risk of BE and E.
Materials and methods
Between March 2009 and October 2012, 339 BE patients, 462 E patients and 619 C with no BE or E undergoing upper gastrointestinal endoscopy for other digestive disorders were consecutively enrolled in 12 Endoscopic Units in the North (n=5), Center (n=2) and South (n=5) of Italy.
BE cases were enrolled among those with an endoscopic 15 mm upward displacement of the squamocolumnar junction (Z-line) from the gastroesophageal junction at endoscopy, and with specialized intestinal metaplasia with ‘goblet’ cells on histology.11 BE length at endoscopy was defined according to the Prague C & M criteria.12
The E group was identified among patients with Los Angeles grade A or B reflux esophagitis with mucosal breaks proven by endoscopy.13 E and C patients were identified in the same centers and in the same period as BE patients.
Multiple biopsies were taken for BE, according to the Seattle protocol, while four biopsies were taken in E patients (two at the Z-line and two at 2 cm above it).14 Biopsies were interpreted in every center by experienced gastrointestinal pathologists.
Controls were recruited from subjects undergoing endoscopy for any reason both in the presence or absence of GERD. We defined as GERD positive those patients reporting at least weekly heartburn or pyrosis (i.e. burning retrosternal sensation, rising from the epigastric region and radiating to the neck, throat or angle of the jaw) and/or acid regurgitation (a sour or bitter taste in the mouth) 1 year before diagnosis.15
Overall, we elected subjects aged 18 years or older, with no serious chronic diseases and prepared to undergo a questionnaire. Only patients with a new diagnosis of BE or E were recruited. The study was approved by the Ethics Committee in each Center and all participants signed an informed consent.
A questionnaire on symptoms or lifestyle habits preceding the diagnosis of BE and E, or endoscopy for controls, was administered by centrally trained interviewers. The questionnaire covered individual characteristics (weight, height, education, occupation), smoking, alcohol consumption, diet, medical history and presence and duration of GERD symptoms. Each subject was asked to report about lifetime consumption of both alcoholic and non-alcoholic beverages, in particular coffee, decaffeinated coffee, tea and herbal tea.
For coffee and tea, subjects' entire drinking histories were recalled according to his/her drinking status, namely non-drinker, current drinker and former drinker (who had stopped drinking at least 1 year before enrollment). Subjects were considered ‘drinkers’ if they consumed beverages at least monthly for 6 months or longer. Questions were asked about the frequency of consumption and the number of units consumed on each drinking occasion, age at initiation, duration and, for former drinkers, years since cessation. One unit was equivalent to 1 cup of coffee or tea (about 30 ml and 170 ml, respectively).
Statistical methods
Data were explored through the analysis of contingency tables and χ2 test was used to assess the independence between each individual characteristic and the three-category health outcome (i.e., BE, E and C). For this reason, continuous variables (e.g., age at interview, BMI) were categorized according to percentiles.
The association between coffee/tea drinking characteristics and health outcome was evaluated using the multinomial logistic regression (MLR) modeling.16 MLR is a particular logistic modeling in that it allows to carry out simultaneously two binary comparisons, namely E vs C and BE vs C. Within each comparison, odds ratio (OR), along with the corresponding and 95% confidence interval (95% CI), was computed and considered as an index of association between each binary health outcome and each putative risk factor.
Coffee/tea drinking habit can be represented through some quantitative characteristics (frequency of consumption, number of units consumed, years of duration, age at initiation and years since cessation), each of which should be properly addressed and analyzed in order to evaluate their distinct effect on individual health status. Such characteristics are generally well correlated and this occurrence (collinearity) can seriously impede to assess their joint role on health outcomes estimated through a regression analysis, and therefore prevent from controlling for the reciprocal confounding effect.17 In an attempt to reduce this statistical drawback, data were stratified according to drinking status (former and current drinkers) and in each stratum an MLR analysis was performed using non-drinkers as a reference category. Only one quantitative drinking variable (main predictor) at a time entered the regression equation after categorization based on specific thresholds (percentiles) a priori defined on the distribution of the C group. The remaining quantitative characteristics, appropriately transformed (centered), entered the equation as continuous variables (covariates).17 In addition to quantitative drinking variables, all MLRs also included, as confounding variables, gender, age at interview, years of schooling, body mass index, smoking habit, alcohol drinking, duration of GERD and categorical terms for collaborative centers.
The statistical significance (two-tailed P-value <0.05) was assessed using the likelihood-based chi-square test for linear trend (TLT).16 All statistical analyses were performed using STATA software.18
Results
Characteristics of BE patients (n=339), E patients (n=462) and C subjects (n=619) are reported in Table 1. Mean age was 56.2±15.2 for BE, 52.6±14.7 for E and 53.7±14.1 for C. Controls had a higher percentage of females (59.3% vs 32.4% BE and 38.3% E) and a lower BMI (49.3% had BMI<24.23 vs 36.9% of BE and 32.5 of E). C had also a lower percentage of smokers (46.7% vs 60.2% of BE and 52.8% of E). Controls underwent endoscopy because of epigastric pain (38%), regurgitation (25%), dyspepsia (24%), pyrosis or dysphagia (9%), gastric or duodenal ulcer (3%) and anemia (1%). GERD symptoms were reported by 78.5% of BE, 80.3% of E and in 54.8% of C. Among GERD-positive subjects, 80.8% of BE patients had suffered from symptoms for more than 3 years vs 50.4% of E and 40.7% of C.
No differences were observed with regard to percentage of subjects consuming coffee (BE 90.9%, E 87.4% and C 88.9%), but BE were more likely to be former drinkers (BE 16.5% vs C and E 6.9%, P-value <0.001). When compared with C, BE patients reported a slightly higher frequency (⩾3 cups/day: 37.2% vs 31.3% C, P-value=0.069) and drank for more time (⩾30 years: 58.7% vs 50.1%, P-value=0.011). In addition, BE started drinking at earlier age (age at initiation ⩽15 years: 19.2% vs 14.4%, P-value=0.056) and quitted drinking coffee later than C (time since cessation ⩽3 years: 10.0% vs 3.4% C, P-value<0.001). In comparison with C subjects, E patients were more likely to be younger when starting drinking (age at initiation ⩽15 years: 19.0%, P-value=0.041), while no differences were observed as for frequency (⩾3 cups/day: 32.1%), duration (⩾30 years: 48.1%) and time since cessation (⩽3 years: 3%).
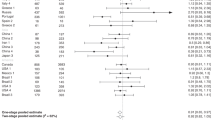
Tables 2 and 3 show the results of MLR modeling reporting the risk of BE and E in former and current coffee drinkers, respectively, using non-drinkers as a reference category. Adjusting for confounding, MLR analysis pointed out a noteworthy risk of BE in former drinkers for all coffee-related predictors (Table 2). In particular, BE risk was high (about fourfold), irrespective of levels of exposure (Table 2, model 1; TLT P-value=0.006) and was four to six times more with duration (Table 2, model 2, >30 years: OR=4.18, 95% CI=1.43–12.3; TLT P-value=0.004) and for late quitters (Table 2, model 3; ⩽3 years: OR=5.95, 95% CI=2.19–16.2; TLT P-value <0.001), respectively. The risk of BE was very high also in subjects who started drinking coffee later (Table 2, model 4; >18 years: OR=6.10, 95% CI=2.15–17.3).
No correlation was found in current drinkers, except an increased risk of E in light drinkers (Table 3, model 1; <1 cup/day: OR=1.85, 95% CI=1.00–3.43).
Unfortunately, we were unable to apply to decaffeinated coffee, tea and herbal tea data the same regression strategy used for coffee intake given the poorness and sparseness of information on several quantitative characteristics. In this context, Table 4 shows the results of contingency tables and MLR analyses. Only few subjects consumed decaffeinated coffee (BE: 23.0%, E: 18.2% and C: 24.1%), and no remarkable differences in frequency of consumption between the study groups were observed.
Controls were more likely to drink tea, and with a higher frequency, compared with both BE (67.8% vs 55.5%, P-value <0.001; cups ⩾1 week: 39.2% vs 32.3%, P-value=0.039) and E (48.9%, P-value <0.001; cups ⩾1 week: 31.6%, P-value=0.017). Tea consumption seemed to decrease the risk of both E and BE, but the observed descending trend is neither monotonic nor statistically significant. However, it is worth noting a discernible risk reduction of E (OR=0.80, 95% CI=0.59–1.07, P-value=0.128) and BE (OR=0.71, 95% CI=0.51–0.97, P-value=0.033) in ever-drinkers when compared with non-drinkers.
No evidence of association between BE or E and herbal tea consumption was found.
Discussion
In this study we investigated coffee and tea consumption in relation to the risk of BE or E. Results were suggestive of a protective effect of tea on BE occurrence, while a remarkable risk of BE for all coffee-related predictors was evidenced.
Coffee intake has been related to a lower risk of a number of cancers at different sites such as liver, prostate, breast and colorectum,19, 20, 21, 22, 23 while it seemed to increase the risk of laryngeal cancer.24
The studies on the role of coffee on the occurrence of esophageal diseases did not exclude a weak inverse relationship between coffee intake and esophageal cancers,25 while a meta-analysis of some Italian observational studies provided evidence of an inverse association with cancers of the oral cavity or pharynx, but not with laryngeal and esophageal cancers.26 Furthermore, other data from a pool of Italian case–control studies revealed no association with tea consumption.10
Data regarding the relationship between tea and cancer are inconsistent. Tea consumption has been inversely associated with all cancers and all-cause mortality;27 nevertheless, meta-analyses suggested an inverse association of high tea consumption (mainly green tea) only with oral, bladder cancer, leukemia and myeloid malignancies, while less clear data were found for other cancers.24, 28, 29, 30 Correlation with esophageal cancer remains unclear, too, with data on a protective effect of green tea, especially in studies conducted among Chinese population,25 or a risk reduction only for subgroups of patients such as females.31, 32
Among the few studies on non-neoplastic esophageal diseases, a meta-analysis showed that overall coffee did not seem to be a causal factor for GERD, while a significantly higher odds ratio was found for E.8 No association was found between coffee intake and the presence of BE in an our previous study;33 furthermore, results from a US survey did not support an association between consumption of coffee or tea and the risk of BE.6 No other data exist on the relationship between BE and tea consumption, but for a suggestion of green tea as an a potential chemopreventive agent for esophageal adenocarcinoma and BE because of the presence of polyphenols able to inhibit the growth of human Barrett's and aerodigestive adenocarcinoma cells.34 Some authors, nevertheless, reported of an amount of heartburn due to tea intake when compared with water.35
Despite the uncertainty on the role of coffee on esophageal tissue, there are some mechanisms supporting the hypothesis of a beneficial or harmful effect. Overall, coffee, including the decaffeinated type, may cause lower-esophageal-sphincter dysfunction and GERD in susceptible subjects.36, 37 In addition, it contains potentially carcinogenic compounds, including acrylamide.23
On the other side, coffee contains polyphenols that inhibit harmful oxidation processes in the body.38 Unfortunately, we were not able to evaluate the different types of coffee, as well as coffee processing and the method used for roasting. The issue is controversial, but these characteristics might explain some of the variability in esophageal tissue response to coffee consumption.39, 40, 41
The poorness of information did not allow us to better analyze some quantitative characteristics of tea consumption or to distinguish between green and black tea type. Anyway, it might be difficult to compare our results with other studies since the majority of Italian people consume black tea, and at low levels, while most reports on this topic are from Asian areas where green tea consumption is largely prevalent. As already said, green tea contains high concentrations of polyphenols that have shown inhibitory effects against the development and growth of carcinogen-induced tumors in animal models at different organs, including the esophagus. In humans, green tea polyphenols may suppress cell proliferation and induce apoptosis.42 This favorable biological activity is nevertheless reduced with the process of black tea production.43
The consumption of beverages at high temperature may be a risk factor for esophageal diseases,44, 45 but coffee and tea temperature did not seem to influence the risk of BE among a western population.6
Comparisons among the studies on the role of beverages on esophageal diseases may be hampered by different characteristics of the studies. A determinant of esophageal disorders is often the presence of GERD, so the lack of information on the presence of GERD may have led authors to underestimate the role of studied beverages.46 Moreover, population controls might have an undiagnosed BE or GERD, even though BE is rarely diagnosed among healthy volunteers and is found in less than 10% of subjects with severe reflux.47, 48 Contrasting results may be also obtained with adjustment for different confounders or when considering different temporalities of the associations. With this regard, it is possible that the cases or GERD controls have changed their drinking habits in the years because of symptoms or diagnosis of esophageal abnormality.
In addition, an underestimation of the observed effects may be present, due to the fact that controls underwent endoscopy because of dyspeptic symptoms. There is also the possibility of a recall bias and some confounders, such as diet, were not taken into account. Few data exist on the association between diet and BE: an inverse relationship between fruits, vegetables and antioxidants intake and the risk of developing BE has been reported, while a diet rich in meat and fast food moderately increased the risk in subjects without GERD.49
To the best of our knowledge, this is the first study analyzing the association between coffee and tea and BE or E in Italian regions. In Italy consumption of these beverages is presumably different from that in other studies and controls did not seem to differ from the Italian population with regard to coffee consumption. Furthermore, all study subjects had an endoscopic diagnosis, BE and E were incident cases and we could control for intensity of GERD symptoms.
In conclusion, our data are suggestive of a reduced risk of BE and E with tea intake, while an adverse effect of coffee was found among BE patients who had stopped drinking coffee, probably due to the development of symptoms or diagnosis. These results are interesting; nevertheless, there is the possibility that coffee or tea intakes be indicative of other lifestyle or food habits with protective or adverse impact on esophageal mucosa.
References
Runge TM, Abrams JA, Shaheen NJ . Epidemiology of Barrett's esophagus and esophageal adenocarcinoma. Gastroenterol Clin North Am 2015; 44: 203–231.
Zagari RM, Law GR, Fuccio L, Pozzato P, Forman D, Bazzoli F . Dyspeptic symptoms and endoscopic findings in the community: The Loiano–Monghidoro Study. Am J Gastroenterol 2010; 105: 565–571.
Zullo A, Esposito G, Ridola L, Hassan C, Lahner E, Perri F et al. Prevalence of lesions detected at upper endoscopy: an Italian survey. Eur J Intern Med 2014; 25: 772–776.
Koek GH, Sifrim D, Lerut T, Janssens J, Tack J . Multivariate analysis of the association of acid and duodeno-gastro-oesophageal reflux exposure with the presence of oesophagitis, the severity of oesophagitis and Barrett’s oesophagus. Gut 2008; 57: 1056–1064.
Ronkainen J, Aro P, Storskrubb T, Johansson SE, Lind T, Bolling-Sternevald E et al. High prevalence of gastroesophageal reflux symptoms and esophagitis with or without symptoms in the general adult Swedish population: a Kalixanda study report. Scand J Gastroenterol 2005; 40: 275–285.
Sajja KC, El-Serag HB, Thrift AP . Coffee or tea, hot or cold, are not associated with risk of Barrett's esophagus. Clin Gastroenterol Hepatol 2016; 14: 769–772.
Pandeya N, Green AC, Whiteman DC, Australian Cancer Study. Prevalence and determinants of frequent gastroesophageal reflux symptoms in the Australian community. Dis Esophagus 2012; 25: 573–583.
Kim J, Oh SW, Myung SK, Kwon H, Lee C, Yun JM et al. Association between coffee intake and gastroesophageal reflux disease: a meta-analysis. Dis Esophagus 2014; 27: 311–317.
Nechuta S, Shu XO, Li HL, Yang G, Ji BT, Xiang YB et al. Prospective cohort study of tea consumption and risk of digestive system cancers: results from the Shanghai Women's Health Study. Am J Clin Nutr 2012; 96: 1056–1063.
La Vecchia C, Negri E, Franceschi S, D'Avanzo B, Boyle P . Tea consumption and cancer risk. Nutr Cancer 1992; 17: 27–31.
Wang KK, Sampliner RE . Practice Parameters Committee of the American College of Gastroenterology. Updated guidelines 2008 for the diagnosis, surveillance and therapy of Barrett's esophagus. Am J Gastroenterol 2008; 103: 788–797.
Sharma P, Dent J, Armstrong D, Bergman JJ, Gossner L, Hoshihara Y et al. The development and validation of an endoscopic grading system for Barrett’s esophagus: the Prague C & M criteria. Gastroenterology 2006; 131: 1392–1399.
Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut 1999; 45: 172–180.
Reid BJ, Blount PL, Feng Z, Levine DS . Optimizing endoscopic biopsy detection of early cancers in Barrett’s high-grade dysplasia. Am J Gastroenterol 2000; 95: 3089–3096.
Edelstein ZR, Bronner MP, Rosen SN, Vaughan TL . Risk factors for Barrett’s esophagus among patients with gastroesophageal reflux disease: a community clinic-based case-control study. Am J Gastroenterol 2009; 104: 834–842.
Hosmer DW, Lemeshow S . Applied Logistic Regression, 2nd edn. Wiley & Sons: NY, USA, 2000.
Leffondré K, Abrahamowicz M, Siemiatycki J, Rachet B . Modeling smoking history: a comparison of different approaches. Am J Epidemiol 2002; 156: 813–823.
StataCorp Stata: Release 14. Statistical Software. StataCorp LP: College Station, TX, 2016.
Bravi F, Bosetti C, Tavani A, Gallus S, La Vecchia C . Coffee reduces risk for hepatocellular carcinoma: an updated meta-analysis. Clin Gastroenterol Hepatol 2013; 11: 1413–1421.
Lu Y, Zhai L, Zeng J, Peng Q, Wang J, Deng Y et al. Coffee consumption and prostate cancer risk: an updated meta-analysis. Cancer Causes Control 2014; 25: 591–604.
Li G, Ma D, Zhang Y, Zheng W, Wang P . Coffee consumption and risk of colorectal cancer: a meta-analysis of observational studies. Public Health Nutr 2013; 16: 346–357.
Jiang W, Wu Y, Jiang X . Coffee and caffeine intake and breast cancer risk: an updated dose-response meta-analysis of 37 published studies. Gynecol Oncol 2013; 129: 620–629.
Wierzejska R . Coffee consumption vs. cancer risk—a review of scientific data. Rocz Panstw Zakl Hig 2015; 66: 293–298.
Chen J, Long S . Tea and coffee consumption and risk of laryngeal cancer: a systematic review meta-analysis. PLoS ONE 2014; 9: e112006.
Zheng JS, Yang J, Fu YQ, Huang T, Huang YJ, Li D . Effects of green tea, black tea, and coffee consumption on the risk of esophageal cancer: a systematic review and meta-analysis of observational studies. Nutr Cancer 2013; 65: 1–16.
Turati F, Galeone C, La Vecchia C, Garavello W, Tavani A . Coffee and cancers of the upper digestive and respiratory tracts: meta-analyses of observational studies. Ann Oncol 2011; 22: 536–544.
Tang J, Zheng JS, Fang L, Jin Y, Cai W, Li D . Tea consumption and mortality of all cancers, CVD and all causes: a meta-analysis of eighteen prospective cohort studies. Br J Nutr 2015; 114: 673–683.
Parodi S, Santi I, Marani E, Casella C, Puppo A, Garrone E et al. Lifestyle factors and risk of leukemia and non-Hodgkin's lymphoma: a case-control study. Cancer Causes Control 2016; 27: 367–375.
Yu F, Jin Z, Jiang H, Xiang C, Tang J, Li T et al. Tea consumption and the risk of five major cancers: a dose-response meta-analysis of prospective studies. BMC Cancer 2014; 14: 197.
Zhang YF, Xu Q, Lu J, Wang P, Zhang HW, Zhou L et al. Tea consumption and the incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Eur J Cancer Prev 2015; 24: 353–362.
Sang LX, Chang B, Li XH, Jiang M . Green tea consumption and risk of esophageal cancer: a meta-analysis of published epidemiological studies. Nutr Cancer 2013; 65: 802–812.
Zheng P, Zheng HM, Deng XM, Zhang YD . Green tea consumption and risk of esophageal cancer: a meta-analysis of epidemiologic studies. BMC Gastroenterol 2012; 12: 165.
Conio M, Filiberti R, Blanchi S, Ferraris R, Marchi S, Ravelli P et al. Risk factors for Barrett's esophagus: a case-control study. Int J Cancer 2002; 97: 225–229.
Gordon V, Jankowski J . Chemoprevention in Barrett's oesophagus. Best Pract Res Clin Gastroenterol 2011; 25: 569–579.
Feldman M, Barnett C . Relationships between the acidity and osmolality of popular beverages and reported postprandial heartburn. Gastroenterology 1995; 108: 125–131.
Cohen S . Pathogenesis of coffee-induced gastrointestinal symptoms. N Engl J Med 1980; 303: 122–124.
Pehl C, Pfeiffer A, Wendl B, Kaess H . The effect of decaffeination of coffee on gastro-oesophageal reflux in patients with reflux disease. Aliment Pharmacol Ther 1997; 11: 483–486.
Cavin C, Holzhaeuser D, Scharf G, Constable A, Huber WW, Schilter B . Cafestol and kahweol, two coffee specific diterpenes with anticarcinogenic activity. Food Chem Toxicol 2002; 40: 1155–1163.
Brazer SR, Onken JE, Dalton CB, Smith JW, Schiffman SS . Effect of different coffees on esophageal acid contact time and symptoms in coffee-sensitive subjects. Physiol Behav 1995; 57: 563–567.
Van Deventer G, Kamemoto E, Kudznicki JT, Heckert DC, Schulte MC . Lower esophageal sphincter pressure, acid secretion, and blood gastrin after coffee consumption. Dig Dis Sci 1992; 37: 558–569.
DiBaise JK . A randomized, double-blind comparison of two different coffee-roasting processes on development of heartburn and dyspepsia in coffee-sensitive individuals. Dig Dis Sci 2003; 48: 652–656.
Yuan JM . Green tea and prevention of esophageal and lung cancers. Mol Nutr Food Res 2011; 55: 886–904.
Graham HN . Green tea composition, consumption, and polyphenol chemistry. Prev Med 1992; 21: 334–350.
Chung CS, Lee YC, Wu MS . Prevention strategies for esophageal cancer: perspectives of the East vs. West. Best Pract Res Clin Gastroenterol 2015; 29: 869–883.
Roshandel G, Khoshnia M, Sotoudeh M, Merat S, Etemadi A, Nickmanesh A et al. Endoscopic screening for precancerous lesions of the esophagus in a high risk area in Northern Iran. Arch Iran Med 2014; 17: 246–252.
Johansson J, Hakansson HO, Mellblom L, Kempas A, Johansson KE, Granath F et al. Risk factors for Barrett’s oesophagus: a population-based approach. Scand J Gastroenterol 2007; 42: 148–156.
El-Serag HB, Petersen NJ, Carter J, Graham DY, Richardson P, Genta RM et al. Gastroesophageal reflux among different racial groups in the United States. Gastroenterology 2004; 126: 1692–1699.
Nandurkar S, Locke GR III, Murray JA, Melton LJ 3rd, Zinsmeister AR, Dierkhising R et al. Rates of endoscopy and endoscopic findings among people with frequent symptoms of gastroesophageal reflux in the community. Am J Gastroenterol 2005; 100: 1459–1465.
De Ceglie A, Fisher DA, Filiberti R, Blanchi S, Conio M . Barrett's esophagus, esophageal and esophagogastric junction adenocarcinomas: the role of diet. Clin Res Hepatol Gastroenterol 2011; 35: 7–16.
Acknowledgements
We are grateful to Bracco for the financial support of the study. We thank the study participants for their confidence and collaboration.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Filiberti, R., Fontana, V., De Ceglie, A. et al. Association between coffee or tea drinking and Barrett’s esophagus or esophagitis: an Italian study. Eur J Clin Nutr 71, 980–986 (2017). https://doi.org/10.1038/ejcn.2017.64
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2017.64
- Springer Nature Limited