
Abstract
Study Design
Literature review with supplementary case examples.
Objectives
The objective of this article was to review neurofibromatosis type 1 (NF1) and the associated spinal pathology with a focus on the disorder’s manifestations in the immature cervical spine.
Summary of Background Data
NF1 is one of the most common inheritable genetic disorders. The disorder is associated with spinal deformities, long bone dysplasia, and osteoporosis. The manifestations of NF1 in the cervical spine commonly include instability secondary to kyphosis, neurofibromas, and dural ectasia.
Methods
Literature relevant to the evaluation and management of NF1 in the cervical spine was reviewed using the PubMed/NCBI database with a focus on recent clinical studies. The review was supplemented with a historical perspective and patient cases.
Results
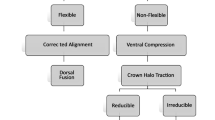
The prevalence of NF1 cervical spine lesions is difficult to define because many patients may be asymptomatic. Symptoms of cervical kyphosis can include pain or nerve deficits but some have a surprisingly high tolerance for deformity and may have frank dislocation of one vertebral body over another (spondyloptosis) with few associated symptoms. Cervical radiographs should be obtained in patients requiring traction, surgery, or intubation, and those with neck pain or symptoms that suggest spinal neurofibromas. Patients with progressive symptoms should be offered surgery. Careful planning is required because many patients will have small, dysplastic vertebral bodies, thin posterior elements, plexiform neurofibromas, or dural ectasia. The decision to use preoperative traction will vary from patient to patient. Combined anterior-posterior fusion is recommended for most cases of severe symptomatic kyphosis, and the fusion should extend from parallel to parallel vertebrae (or six or more levels). Anterior or posterior fusion alone may be an alternative for skeletally mature patients with smaller, flexible curves.
Conclusions
Spinal deformity is the most common musculoskeletal manifestation of NF1. Cervical lesions are frequently asymptomatic, but patients with thoracolumbar scoliosis, dystrophic features, or a history of laminectomy should have the cervical spine carefully evaluated. For severe and progressive kyphotic deformities, most authors recommend a period of traction followed by a combined anterior-posterior fusion that is instrumented from parallel to parallel vertebra (or six or more levels). Close follow-up is very important because complications and progression are frequent.
Similar content being viewed by others


Change history
30 December 2019
The corresponding authors regret that his professional degree was inadvertently included as co-author “Hono Caus Gr” in the article.
References
Crawford AH, Schorry EK. Neurofibromatosis in children: the role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217–30.
Goldberg NS, Collins FS. The hunt for the neurofibromatosis gene. Arch Dermatol 1991;127:1705–7.
Crawford AH, Lykissas MG, Schorry EK, et al. Neurofibromatosis: etiology, commonly encountered spinal deformities, common complications and pitfalls of surgical treatment. Spine Deform 2012:85–94.
Crawford AH, Herrera-Soto J. Scoliosis associated with neurofibromatosis. Orthop Clin North Am 2007;38:553–62. vii.
Durrani AA, Crawford AH, Chouhdry SN, et al. Modulation of spinal deformities in patients with neurofibromatosis type 1. Spine 2000;25:69–75.
Crawford AH. Pitfalls of spinal deformities associated with neurofibromatosis in children. Clin Orthop 1989;245:29–42.
Takeshita K, Peterson ETK, Bylski-Austrow D, et al. The nuchal ligament restrains cervical spine flexion. Spine 2004;29:E388–93.
Nathan ST, Mangano FT, Crawford AH. Spondyloptosis of the cervical spine in a patient with neurofibromatosis type 1: a case report and review of the literature. JBJS Case Connect 2013;3:e5.
Messiaen LM, Callens T, Mortier G, et al. Exhaustive mutation analysis of the NF1 gene allows identification of 95% of mutations and reveals a high frequency of unusual splicing defects. Hum Mutat 2000;15:541–55.
National Institutes of Health Consensus Development Conference Statement: neurofibromatosis. Bethesda, Md., USA, July 13–15, 1987. Neurofibromatosis 1988;1:172–8.
Pride NA, North KN. The cognitive profile of NF1 children: therapeutic implications. In: Neurofibromatosis Type 1. Berlin: Springer;2012. p. 55–69.
Mautner VF, Friedrich RE, von Deimling A, et al. Malignant peripheral nerve sheath tumours in neurofibromatosis type 1: MRI supports the diagnosis of malignant plexiform neurofibroma. Neuroradiology 2003;45:618–25.
Funasaki H, Winter RB, Lonstein JB, Denis F. Pathophysiology of spinal deformities in neurofibromatosis. An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692–700.
Tsirikos AI, Saifuddin A, Noordeen MH. Spinal deformity in neurofibromatosis type-1: diagnosis and treatment. Eur Spine J 2005;14:427–39.
Nguyen R, Dombi E, Akshintala S, et al. Characterization of spinal findings in children and adults with neurofibromatosis type 1 enrolled in a natural history study using magnetic resonance imaging. J Neurooncol 2015;121:209–15.
Khong P-L, Goh WHS, Wong VCN, et al. MR imaging of spinal tumors in children with neurofibromatosis 1. AJR Am J Roentgenol 2003;180:413–7.
Thakkar SD, Feigen U, Mautner VF Spinal tumours in neurofibromatosis type 1: an MRI study of frequency, multiplicity and variety. Neuroradiology 1999;41:625–9.
Yong-Hing K, Kalamchi A, MacEwen GD. Cervical spine abnormalities in neurofibromatosis. J Bone Joint Surg Am 1979;61:695–9.
Bell DF, Walker JL, O’Connor G, Tibshirani R. Spinal deformity after multiple-level cervical laminectomy in children. Spine 1994;19:406–11.
de Jonge T, Slullitel H, Dubousset J, et al. Late-onset spinal deformities in children treated by laminectomy and radiation therapy for malignant tumours. Eur Spine J 2005;14:765–71.
Fraser RD, Paterson DC, Simpson DA. Orthopaedic aspects of spinal tumors in children. J Bone Joint Surg Br 1977;59:143–51.
Katsumi Y, Honma T, Nakamura T. Analysis of cervical instability resulting from laminectomies for removal of spinal cord tumor. Spine 1989;14:1171–6.
Yasuoka S, Peterson HA, MacCarty CS. Incidence of spinal column deformity after multilevel laminectomy in children and adults. J Neurosurg 1982;57:441–5.
Helenius IJ, Sponseller PD, Mackenzie W, et al. Outcomes of spinal fusion for cervical kyphosis in children with neurofibromatosis. J Bone Joint Surg Am 2016;98:e95.
Albert TJ, Vacarro A. Postlaminectomy kyphosis. Spine 1998;23:2738–45.
Pal GP, Sherk HH. The vertical stability of the cervical spine. Spine 1988;13:447–9.
Saito T, Yamamuro T, Shikata J, et al. Analysis and prevention of spinal column deformity following cervical laminectomy. I. Pathogenetic analysis of postlaminectomy deformities. Spine 1991;16:494–502.
Cusick JF, Yoganandan N, Pintar F, et al. Biomechanics of cervical spine facetectomy and fixation techniques. Spine 1988;13:808–12.
Zdeblick TA, Zou D, Warden KE, et al. Cervical stability after foraminotomy. A biomechanical in vitro analysis. J Bone Joint Surg Am 1992;74:22–7.
Sim FH, Svien HJ, Bickel WH, Janes JM. Swan-neck deformity following extensive cervical laminectomy. A review of twenty-one cases. J Bone Joint Surg Am 1974;56:564–80.
Cattell HS, Clark GL. Cervical kyphosis and instability following multiple laminectomies in children. J Bone Joint Surg Am 1967;49:713–20.
Connolly ES, Seymour RJ, Adams JE. Clinical evaluation of anterior cervical fusion for degenerative cervical disc disease. J Neurosurg 1965;23:431–7.
Lonstein JE. Post-laminectomy kyphosis. Clin Orthop 1977;128:93–100.
Yasuoka S, Peterson HA, Laws ER, MacCarty CS. Pathogenesis and prophylaxis of postlaminectomy deformity of the spine after multiple level laminectomy: difference between children and adults. Neurosurgery 1981;9:145–52.
Ma J, Wu Z, Yang X, Xiao J. Surgical treatment of severe cervical dystrophic kyphosis due to neurofibromatosis type 1: a review of 8 cases. J Neurosurg Spine 2011;14:93–8.
Kokubun S, Ozawa H, Sakurai M, Ishii Y. One-stage anterior and posterior correction of severe kyphosis of the cervical spine in neurofibromatosis. A case report. Spine 1993;18:2332–5.
Craig JB, Govender S. Neurofibromatosis of the cervical spine. A report of eight cases. J Bone Joint Surg Br 1992;74:575–8.
Curtis BH, Fisher RL, Butterfield WL, Saunders FP Neurofibromatosis with paraplegia. Report of eight cases. J Bone Joint Surg Am 1969;51:843–61.
Taleb FS, Guha A, Arnold PM, et al. Surgical management of cervical spine manifestations of neurofibromatosis type 1: long-term clinical and radiological follow-up in 22 cases. J Neurosurg Spine 2011;14:356–66.
Goffin J, Grob D. Spondyloptosis of the cervical spine in neurofibromatosis. A case report. Spine 1999;24:587–90.
Haddad FS, Williams RL, Bentley G. The cervical spine in neurofibromatosis. Br J Hosp Med 1995;53:318–9.
Horsley M, Taylor TK, Sorby WA. Traction-induced rupture of an extracranial vertebral artery aneurysm associated with neurofibromatosis. A case report. Spine 1997;22:225–7.
Kawabata S, Watanabe K, Hosogane N, et al. Surgical correction of severe cervical kyphosis in patients with neurofibromatosis type 1. J Neurosurg Spine 2013;18:274–9.
Wu F, Zhang L, Liu Z, et al. Cervical neurofibromatosis with tetraplegia: management by cervical suspensory traction. Spine 2012;37:E858–62.
Laohacharoensombat W, Wajanavisit W, Woratanarat P. Cervical neurofibromatosis with quadriparesis: management by fibular strut graft. Indian J Orthop 2010;44:95–7.
Winter RB, Moe JH, Bradford DS, et al. Spine deformity in neurofibromatosis. A review of one hundred and two patients. J Bone Joint Surg Am 1979;61:677–94.
Yonezawa I, Arai Y, Tsuji T, et al. Anterior fusion and posterior correction of severe cervical kyphosis using pedicle screw fixation in a patient with neurofibromatosis: a case report. J Spinal Disord Tech 2003;16:493–6.
Asazuma T, Yamagishi M, Nemoto K, et al. Spinal fusion using a vascularized fibular bone graft for a patient with cervical kyphosis due to neurofibromatosis. J Spinal Disord 1997;10:537–40.
Rodgers WB, Coran DL, Kharrazi FD, et al. Increasing lordosis of the occipitocervical junction after arthrodesis in young children: the occipitocervical crankshaft phenomenon. J Pediatr Orthop 1997;17:762–5.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author disclosures: AHC (none), APS (none), FTM (none).
This study was approved by the University of Cincinnati Institutional Review Board (no. 2013-7134).
Rights and permissions
About this article

Cite this article
Crawford, A.H., Gr, H., Schumaier, A.P. et al. Management of Cervical Instability as a Complication of Neurofibromatosis Type 1 in Children: A Historical Perspective With a 40-Year Experience. Spine Deform 6, 719–729 (2018). https://doi.org/10.1016/j.jspd.2018.04.002
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/j.jspd.2018.04.002